


Abstract
Integrins are upregulated on both tumor cells and associated vasculature, where they play an important role in angiogenesis and metastasis. Fluciclatide is an arginine-glycine-aspartic acid peptide with high affinity for αvβ3/αvβ5 integrin, which can be radiolabeled for PET imaging of angiogenesis. Thus, 18F-fluciclatide is a potential biomarker of therapeutic response to antiangiogenic inhibitors. The aim of this study was to evaluate the reproducibility of 18F-fluciclatide in multiple solid-tumor types. Methods: Thirty-nine patients underwent PET/CT scanning at 40, 65, and 90 min after injection of 18F-fluciclatide (maximum, 370 MBq) on 2 separate days (2–9 d apart). Patients did not receive any therapy between PET/CT scans. 18F-fluciclatide images were reported and quantitative measures of uptake were extracted using the PERCIST methodology. Intrasubject reproducibility of PET uptake in all measurable lesions was evaluated by calculating relative differences in SUV between PET scans for each lesion during the 2 imaging sessions. Results: Thirty-nine measurable lesions were detected in 26 patients. Lesion uptake correlated strongly across imaging sessions (r = 0.92, P < 0.05, at 40 min; r = 0.94, P < 0.05, at 65 min; r = 0.94, P < 0.05, at 90 min) with a mean relative difference and SD of the relative difference of 0.006 ± 0.18 at 40 min, 0.003 ± 0.19 at 65 min, and 0.025 ± 0.20 at 90 min. This reflects 95% limits of repeatability of 35%–39% for the difference between the 2 SUV measurements or a variability of 18%–20% in agreement from that observed in well-calibrated multicenter 18F-FDG studies. Conclusion: The test–retest reproducibility of 18F-fluciclatide across multiple tumor types has been measured and shown to be acceptable. This is an important step in the development of this in vivo biomarker to identify and quantify response to antiangiogenic therapy in cancer patients.
Tumor angiogenesis, the formation of tumor-associated vasculature, is an essential event in tumor growth and metastasis and has been the focus of therapeutic target development for decades (1). Several antiangiogenic therapies are routinely used for the management of solid tumors, including bevacizumab for management of colorectal and ovarian cancer (2–5), sunitinib and pazopanib for metastatic renal cell cancer (6,7), and sorafenib for hepatocellular cancer (8). Using conventional imaging assessment, these agents predominantly result in a cytostatic response, with changes in tumor size taking months to evolve. Furthermore, these agents are associated with significant toxicity profiles, including hypertension, gastrointestinal perforation, and hemorrhage. Therefore, there is a real need for a validated biomarker of therapeutic response to differentiate those patients benefiting from these targeted agents and those being exposed to potential life-threatening toxicities without clinical effect.
As new vessels form, integrins, a family of cell adhesion molecules, facilitate the interaction between tumor vasculature and the extracellular matrix (9,10). αvβ3/5 integrins are of particular interest as these are expressed at low levels on mature vessels and nonneoplastic epithelium but are highly expressed on activated tumor-related endothelial cells, as well as cancers such as breast and lung cancer, melanoma, and osteosarcoma (9,11). αvβ3/5 integrins interact with components of the extracellular matrix such as fibronectin, laminin, and collagen via the tripeptide sequence arginine-glycine-aspartic acid (RGD) (12). Peptide ligands have high affinity for the RGD sequence, and several radiolabeled probes, have been developed to image integrin expression either with PET or with SPECT (13–17). Given the pivotal role that these integrins hold in tumor angiogenesis and cancer progression, the ability to visualize and quantify αvβ3/αvβ5 integrin presents an opportunity to develop a response biomarker.
18F-fluciclatide is a cyclic tripeptide that contains the RGD sequence and binds with high affinity to integrins αvβ3 and αvβ5, both of which are upregulated in tumor-associated vasculature (18). 18F-fluciclatide is currently being developed as a radiotracer for the imaging of angiogenesis in tumors and consequently as a biomarker of response to antiangiogenic therapies (14,19).
Imaging biomarkers used in any prognostic or treatment response studies should exhibit a high degree of reproducibility such that a significant change in imaging parameters between 2 studies can be considered relevant and not attributable to noise variance. Quantification of intrinsic variability in the absence of treatment is important to provide a robust objective response criterion such as PERCIST for 18F-FDG PET (20). Therefore, test–retest measurements are an essential step in the clinical development of any new PET tracers. The Quantitative Imaging Biomarker Alliance has listed repeatability metrics commonly found in the literature (21). Although mean absolute percentage difference in SUV appears to be the most common measure assessed, mean relative difference and the SD of the relative differences provides information on both systematic and random error. Additionally, this approach allows calculation of a measure of reproducibility reflecting the 95% confidence limits for identification of a true difference between the 2 measurements, such that measured changes in tumor uptake that fall outside this 95% coefficient of repeatability can be attributed to biologic response (22). An appreciation of test variability is also a requirement for correct powering of single and multicenter controlled trials. The sample size depends on both the effect size (expected treatment group difference) and the response variance. Consequently, studies using a test with high test–retest variability will require a larger subject cohort than one with lower variability to demonstrate the same effect (23). Therefore, the primary objective of this study was to assess the test–retest reproducibility of 18F-fluciclatide uptake in solid tumors within a multicenter setting.
MATERIALS AND METHODS
Patients
Ethical approval was obtained before the study commenced, and all procedures were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Thirty-nine patients were enrolled into this multicenter study. All had at least one solid primary or metastatic tumor 2.0 cm or larger in diameter, including but not limited to non–small cell lung cancer, renal cell cancer, glioblastoma, melanoma, sarcoma, head and neck cancer, and breast cancer. Only patients not undergoing curative treatment and who had undergone routine clinical imaging within 8 wk of study entry were eligible. Patients who had undergone biopsy, radiotherapy, surgery, or any other treatment within 4 wk before the first imaging session (within 2 wk of chemotherapy) or were scheduled to undergo such procedures between the first and second 18F-fluciclatide PET sessions were ineligible. Patients who were pregnant, lactating, or not practicing adequate contraception were also excluded. All subjects were required to give signed and dated informed consent to take part in the study.
Study Design
The aim of the study was to determine the reproducibility of serial 18F-fluciclatide PET scans and to define objective 18F-fluciclatide response parameters. To this end, patients underwent 2 18F-fluciclatide sessions within 10 d of each other before commencement of therapy.
PET Imaging
Radiolabeled active 18F-fluciclatide was formulated in phosphate-buffered saline containing up to 7% w/v ethanol and a 2 mg/mL concentration of sodium p-aminobenzoate as a ready-to-use sterile solution (18) at a qualified, good-manufacturing-practice–validated facility. Before administration, the suitability of each preparation was assessed by radioactivity, high-performance liquid chromatography, and pH measurement, according to the approved standard operating procedures of the facility. A maximum of 20 μg of fluciclatide peptide was administered in a single intravenous bolus at each 18F-fluciclatide imaging session. The pH of the solution was 6–8. The radiochemical purity of 18F-fluciclatide injection was not less than 90% during the shelf life of the product. The maximum dose for radioactivity was 370 MBq for each scan. 18F-fluciclatide was administered as a bolus dose over 10 s, followed by a 10-mL saline flush. Thirty-five minutes after injection, a short CT scan was performed followed by a low-dose, whole-body CT scan for attenuation correction and anatomic localization. Three-dimensional whole-body PET acquisitions were obtained at 3 time points with nominal start times at 40, 65, and 90 min after injection. Emission data were reconstructed using iterative ordered-subset expectation maximization and filtered backprojection. Reconstruction was performed with 8 iterations and 21 subsets; the voxel size ranged between 1.277 and 1.788 mm3 and was consistent across centers.
Site Qualification and Quality Control
All subjects were imaged on a dedicated, full-ring PET/CT scanner (Discovery models STE x4, ST x2, VCT, Rx, 690, and 600 [GE Healthcare]; Gemini TF [Philips]). Participating sites were required to submit recently acquired test data to the sponsor for review before the commencement of scanning. Using these data, image reconstruction parameters were adjusted when necessary to minimize intersite variability to allow the pooling of data. 18F-fluciclatide image quality and protocol adherence was monitored throughout the study. Standard-of-care images did not undergo formal quality control.
Image Acquisition and Analysis
Uptake Characteristics
Tumor uptake characteristics were determined from the 40-min acquisition scan of the first PET session. PERCIST-type analysis was undertaken by a single interpreter who was masked to scan timing and clinical history (20). For each lesion, volume of interest was used to determine tracer uptake, denoted as SUVpeak, and was normalized to body weight. When a suitable region of tissue could be identified, a 3-cm-diameter region of interest, as described by the PERCIST methodology, was placed over healthy liver to determine the intersubject variability of liver SUVmean normalized to body weight (SUVliver) across the 3 time points as a further validation of acquired PET images. SUVliver was not used as a reference in the final analysis.
Lesions were included in the final analysis if they were interpretable and measurable on standard-of-care imaging (24), if they were larger than 2 cm in diameter, and if they were identified on both PET session 1 and PET session 2, with both PET studies having been acquired at the same time after injection. In subjects with more than 5 visible lesions on PET session 1, the 5 lesions with the highest SUVpeak were used. In all cases, the maximum number of selected lesions per organ was two.
Temporal Segmentation
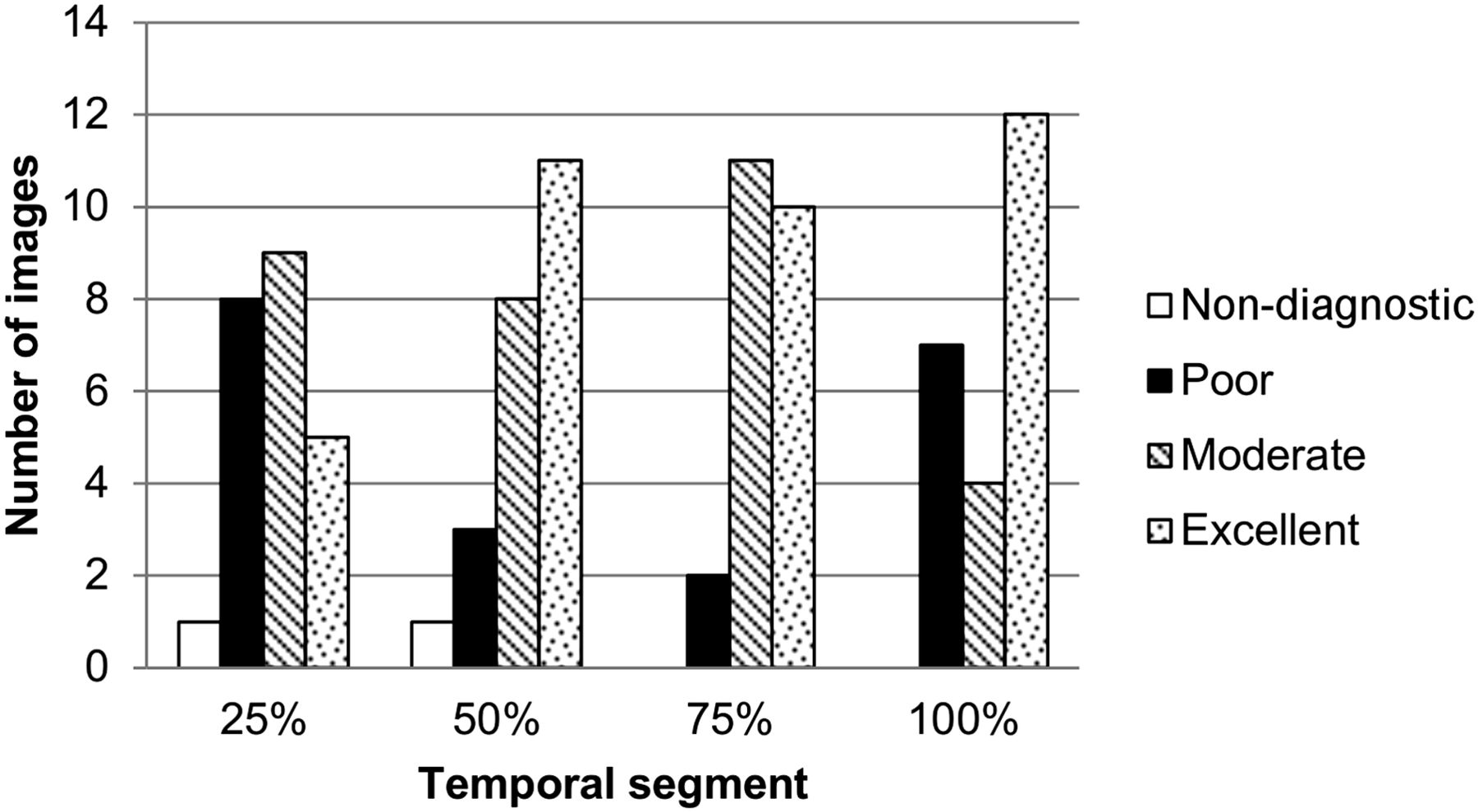
In addition, list-mode data were temporally segmented after acquisition to characterize the efficacy of 18F-fluciclatide as a function of administered activity (25). Injected activities of 25%, 50%, 75%, and 100% of the actual dose were simulated, and a masked image evaluation was performed to assess the fraction of the administered activity required to produce a diagnostic-quality image. Images were graded as excellent, moderate, poor, or nondiagnostic by 3 independent interpreters. The Cohen κ statistic was used to measure agreement between ratings of overall image quality (26). Additionally, SUVliver and the coefficient of variation within the liver region of interest were measured across temporal fractions.
Determination of Sample Size and Statistical Analysis
The primary objective was to assess the reproducibility of 18F-fluciclatide. Previous single-center reproducibility studies with 18F-FDG reported a 10% variation in 18F-FDG uptake between repeated PET scans (27). Moreover, in evaluations of treatment response with 18F-FDG, a 20%–30% decrease in tumor uptake suggests tumor response (28–30). Therefore, we assumed that, on the basis of 18F-FDG data, intratumoral variation exceeding 15% was unlikely to be clinically useful (27). A sample size of 35 was chosen to give a 95% confidence interval of the mean relative difference with an SD of 0.15. A second group of 10 subjects, following the same protocol, was recruited to meet a secondary objective comparing SUV and immunohistochemical analysis of biopsied tissue. Concern that a biopsy would affect uptake meant these subjects were scheduled for a separate reproducibility analysis from the main group. Therefore, the total number of subjects to be enrolled was 45.
The reproducibility of SUVpeak was analyzed on a lesion-by-lesion basis. For reproducibility measures, the individual SUVpeak for each scanning visit was plotted for each acquisition time. High reproducibility was represented by all data being distributed along a line of unity. Correlation analysis and Wilcoxon signed-rank testing were used to assess reproducibility. The distribution of SUV for all lesions was assessed for normality using the Shapiro–Wilk test and the quantile–quantile plot and described as SUVmean ± SD. The relative difference in uptake at each time point was defined as 2 × (SUV2 − SUV1)/(SUV1 + SUV2), where SUV1 is the SUVpeak in the first scanning session and SUV2 is that in the second session. Box-and-whisker plots were generated to illustrate the distribution of the acquired data and mean relative differences. The 95% reference range from spontaneous fluctuations in SUVpeak was calculated as 1.96 × SD of the relative difference between both PET scans. To provide further examination predicated on tumor type, additional analyses were performed for tumor types found in at least 3 subjects. Bland–Altman plots of the paired differences in SUVs were also examined. A P value of less than 0.05 was considered significant, and statistical analysis was performed using R for Windows (Microsoft), version 3.0.1 (27).
RESULTS
Patient Population
Of the subgroup scheduled for immunochemical analysis, no biopsies were performed within the time window allowed by the protocol. The 4 subjects scanned within this group were therefore included in the main study group, to give a total of 39 patients (24 women and 15 men) recruited from 11 sites. The median age was 58.7 y (range, 29–86 y), and the most common tumor types were breast (21%) and colorectal (15%) (Table 1). The interval between PET sessions 1 and 2 ranged from 2 to 9 d (median, 5 d). The mean (±SD) start times of each acquisition during the first imaging session were 44 ± 11.8, 71 ± 11.9, and 98 ± 12.1 min. During the second imaging session, these were 44 ± 12.1, 71 ± 12.2, and 97 ± 12.4 min after injection. The mean administered activity was 327.2 MBq for PET session 1 (range, 262.9–374.8 MBq) and 326.6 MBq for PET session 2 (range, 271.8–363.8 MBq)
Patient and Lesion Characteristics of Evaluable Tumors
Tumor and Normal-Tissue Uptake of 18F-Fluciclatide
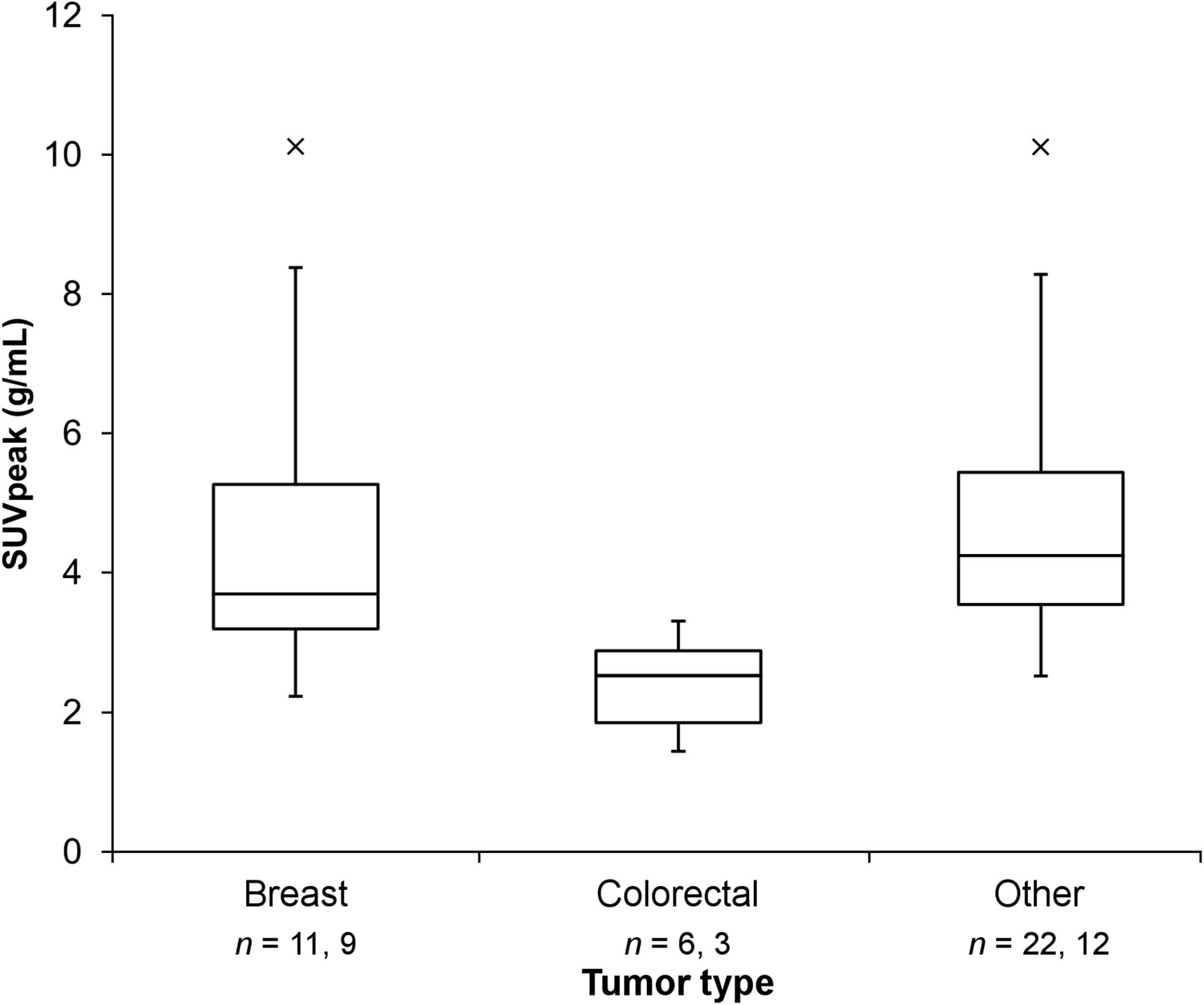
Approximately half the lesions identified in the standard-of-care images exhibited measurable 18F-fluciclatide uptake (Fig. 1). Mean SUVpeak at each time point in session 1 was 4.54 (±2.21) at 40 min, 4.63 (±2.34) at 65 min, and 4.39 (±2.25) at 90 min. The SUV data were not normally distributed (P < 0.05), but normality was restored by a logarithmic transform. Figure 2 illustrates the distribution of SUVpeak within tumor types. Regions of healthy liver tissue were identified in 20 subjects; mean SUVliver was 3.94 ± 0.75 at 40 min after injection.
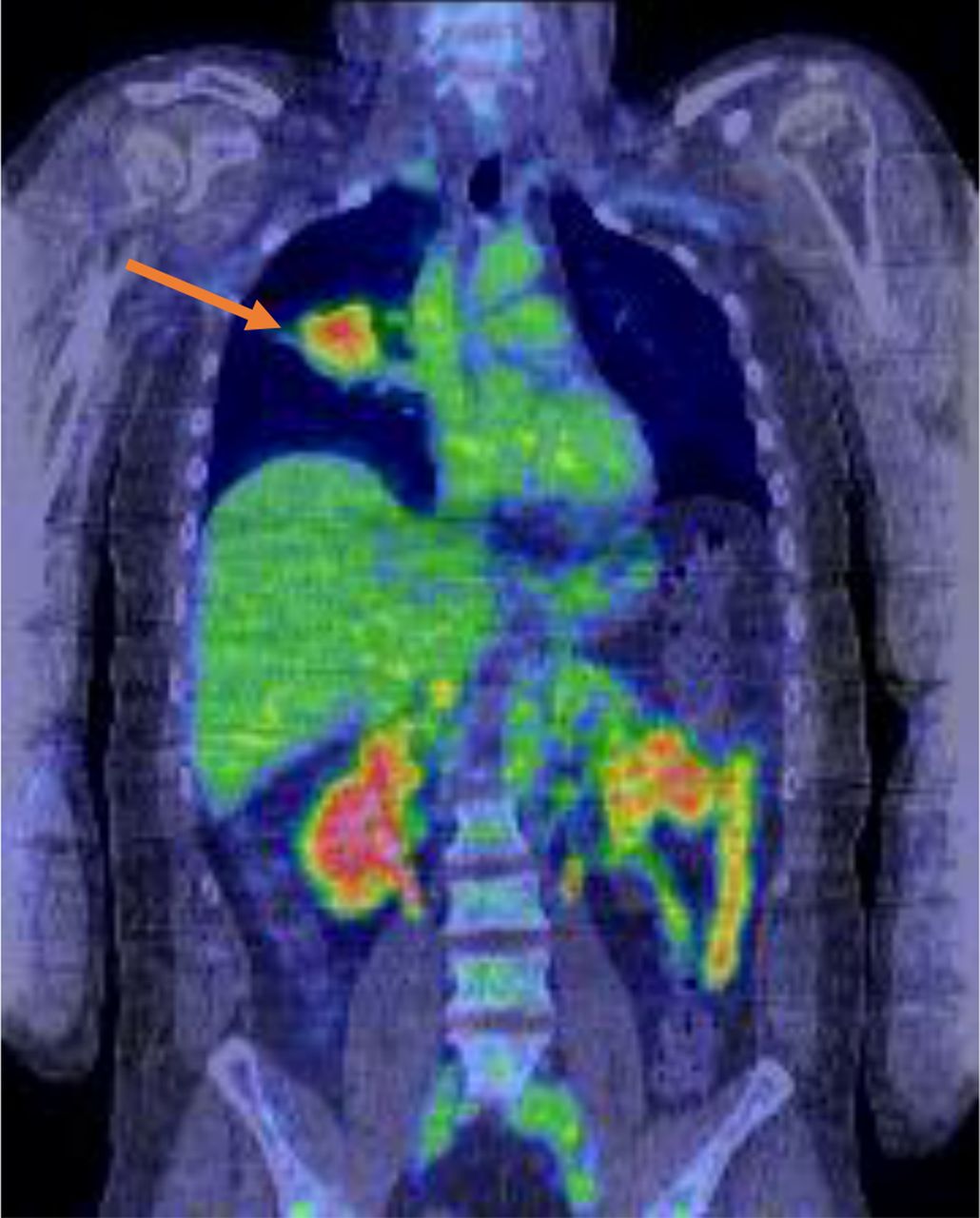
18F-fluciclatide PET scan of 39-y-old man with diagnosis of melanoma. In rainbow-color-map image taken 65 min after injection, 18F-fluciclatide uptake is seen within lung metastasis (arrow).
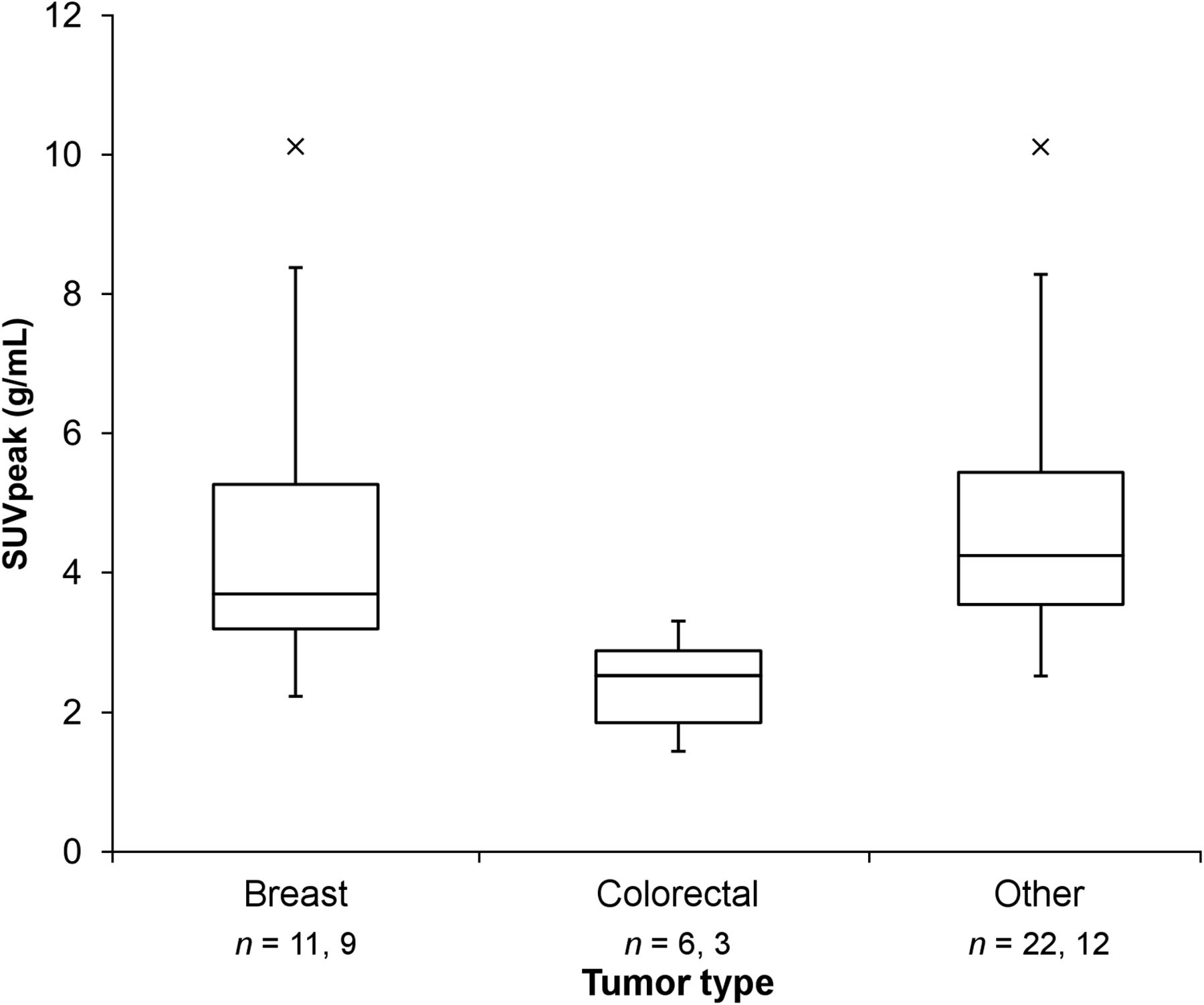
Box-and-whisker plot illustrating median and distribution of SUVpeak within lesions for each tumor subtype. Sample sizes (n) indicate both number of lesions measured and second number of subjects in each group. × = outliers.
Reproducibility of 18F-Fluciclatide SUV
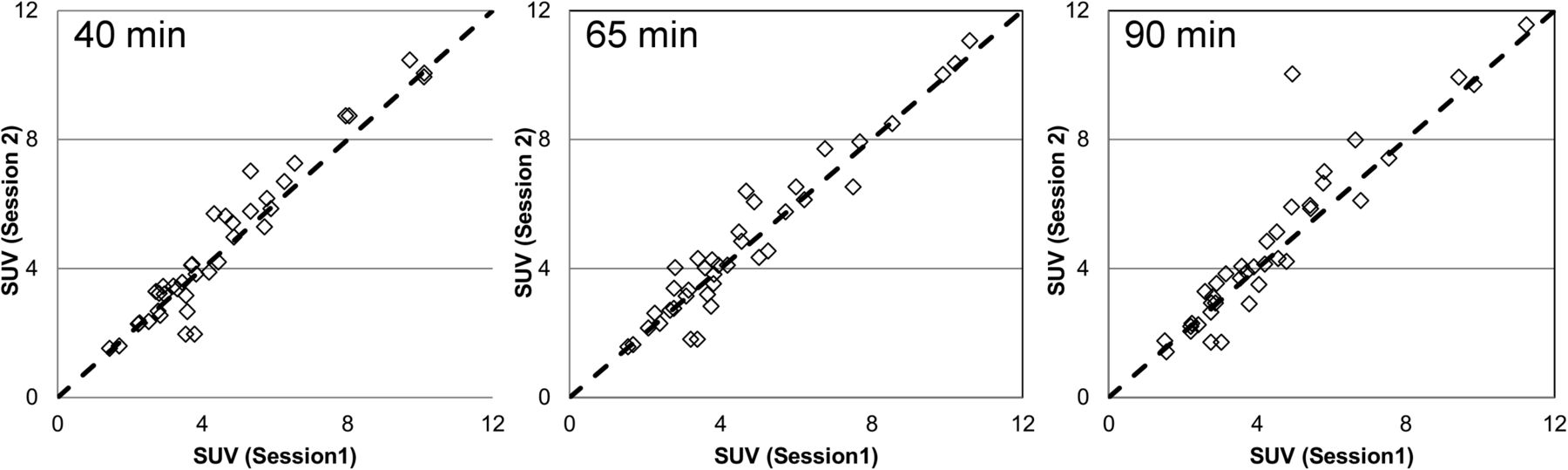
Thirty-nine discrete lesions from 26 patients were evaluated for reproducibility of repeated measures of 18F-fluciclatide retention; the other lesions did not fulfil the predefined criteria for lesion selection (Table 1). Figure 3 shows plots of SUVpeak for the 2 PET sessions at the 3 acquisition times. No significant difference in SUVpeak between the 2 sessions was observed across the 3 acquisition points. Regression analysis of the line of unity indicated good test–retest correlation for the 3 acquisition times (Spearman r = 0.92, 0.94, and 0.94 at 40, 65, and 90 min, respectively). Figure 4 illustrates the variability of the relative difference. The mean relative differences were 0.01, 0.00, and 0.02 at 40, 65, and 90 min, respectively, with none being significantly different from zero. The SDs of the mean relative difference were 18%, 19%, and 20% for the 40-, 65-, and 90-min acquisition times, respectively. Intraclass correlation coefficients were, respectively, 0.96, 0.96, and 0.91 at the 3 acquisition times. These results indicate that SUVpeak obtained from 18F-fluciclatide PET can be used repeatedly in serial scans. The 95% normal values for spontaneous fluctuations were 35%–39% (i.e., 1.96 × SD of relative difference).
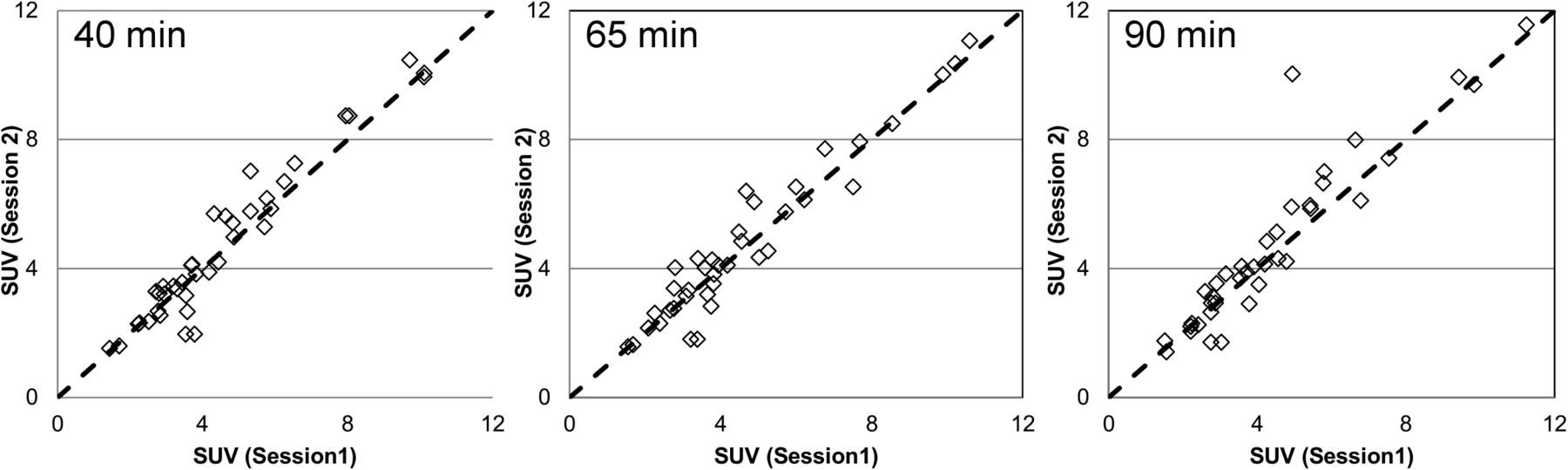
Test–retest scatterplots of SUV in session 2 (y-axis) against SUV in session 1 (x-axis) at 40, 65, and 90 min. Dotted line is line of unity.
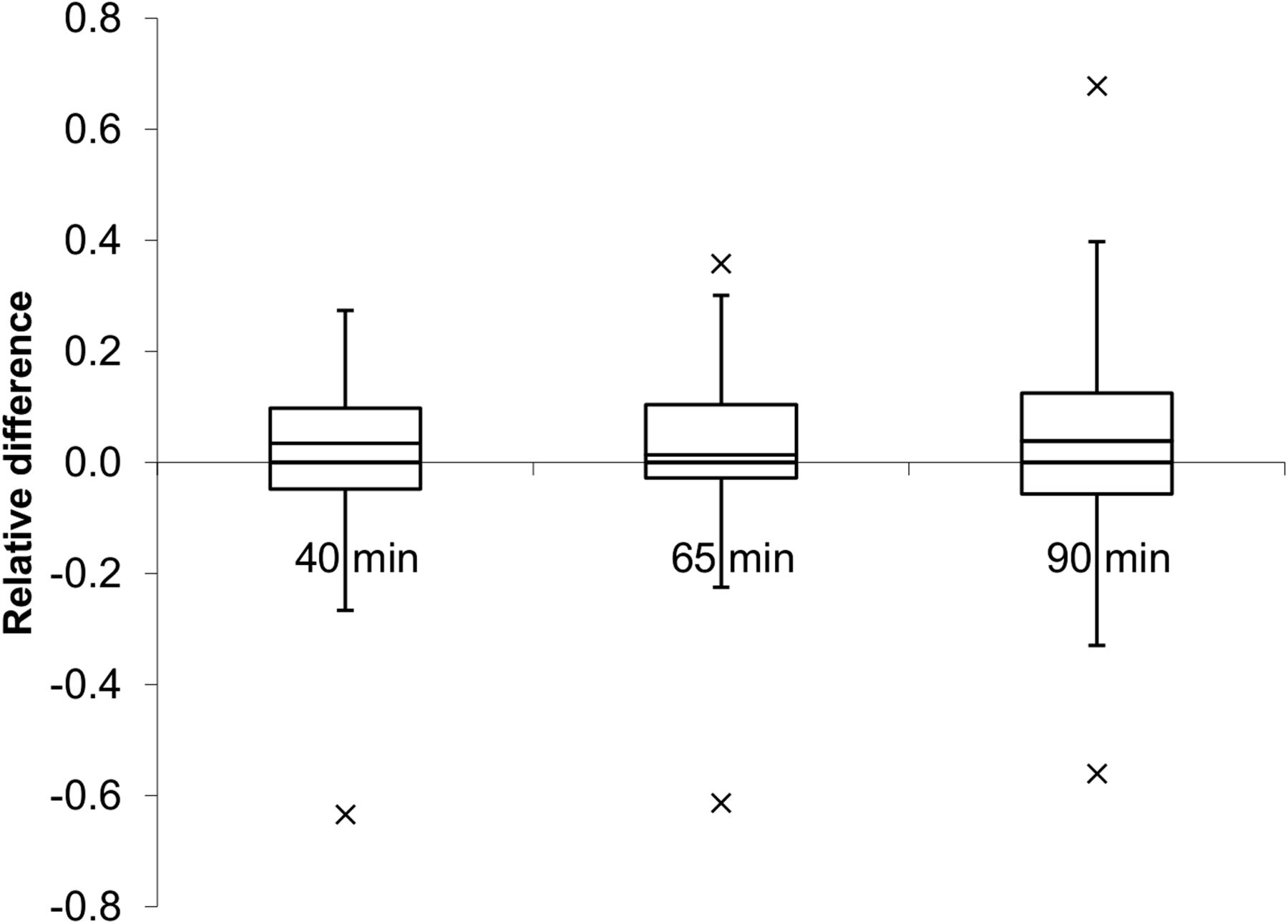
Box plot illustrating relative difference in SUVpeak at 40, 65, and 90 min after injection. Plot shows median relative difference. × = outliers.
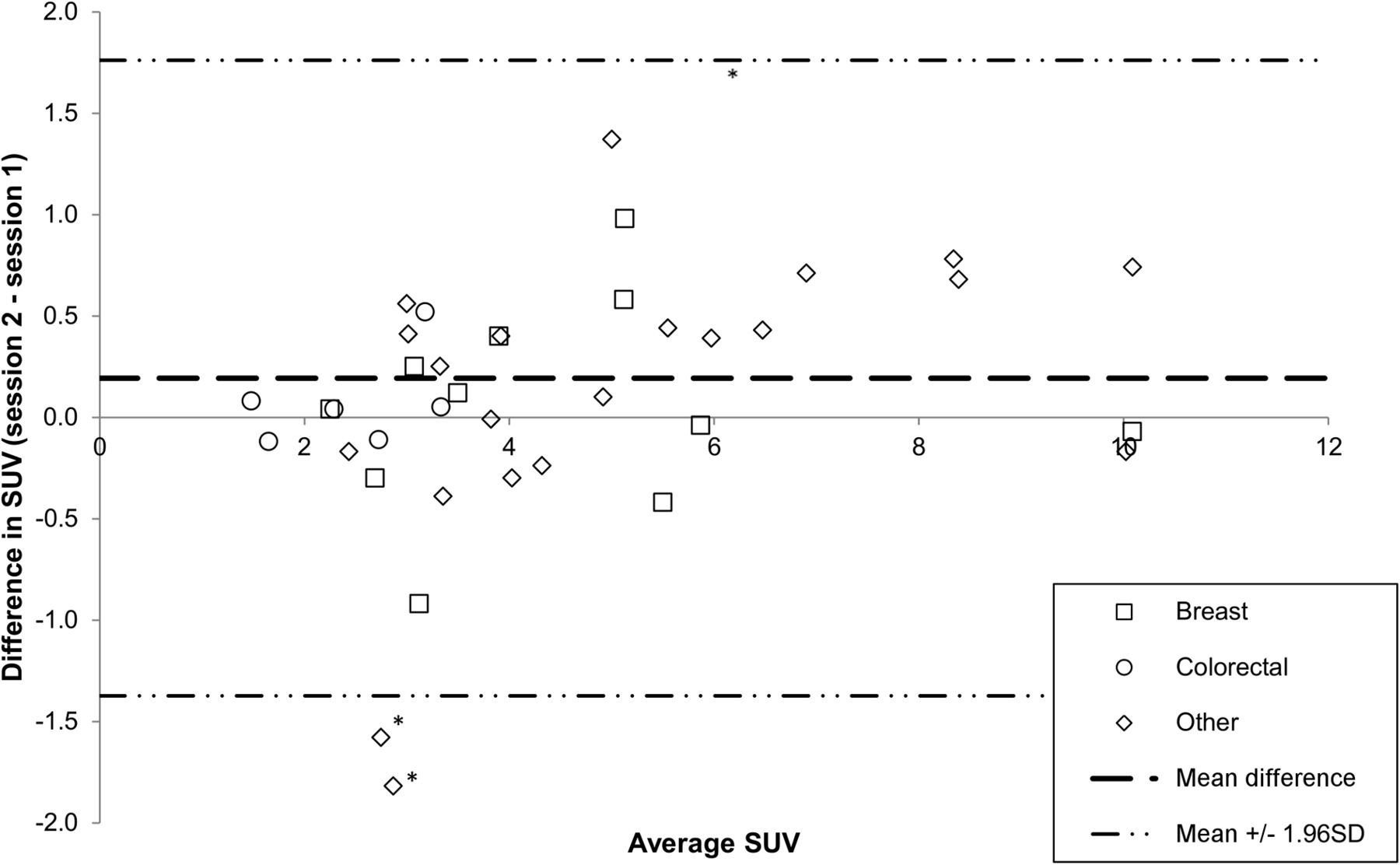
The Bland–Altman plot of the differences between the 2 PET sessions at 40 min highlighting tumor types that occurred in more than 3 patients per group is shown in Figure 5. Overall, the mean difference in SUVpeak between the 2 sessions was 0.19, with 95% of the differences lying between the limits of agreement of 1.76 and −1.37. In breast cancer (11 lesions in 9 subjects), the mean relative difference was 0.00 ± 0.13, and in colorectal cancer it was 0.02 ± 0.08 (6 lesions in 3 subjects).

Bland–Altman plot of difference in SUV at 40 min against SUVmean. Outliers are from subject with NSCLC. *Lung lesions.
Temporal Segmentation
For uniformity, temporal segmentation was done using liver data. The κ statistics showed that the 2 interpreters’ ratings of the 75%-activity images agreed substantially better with full-activity (100%) images than did 25%- or 50%-activity images, which were rated similarly in their degree of agreement with the full acquisition dataset (Fig. 6). Quantitatively, there was a reduction in SUVliver with each successively smaller fraction (100%: 3.94 ± 0.36; 75%: 3.76 ± 0.40; 50%: 3.68 ± 0.47; 25%: 3.49 ± 0.59). The coefficient of variation for SUVliver progressively increased as the fractional administered activity of 18F-fluciclatide injection was reduced, indicating a progressively decreasing signal-to-noise ratio.
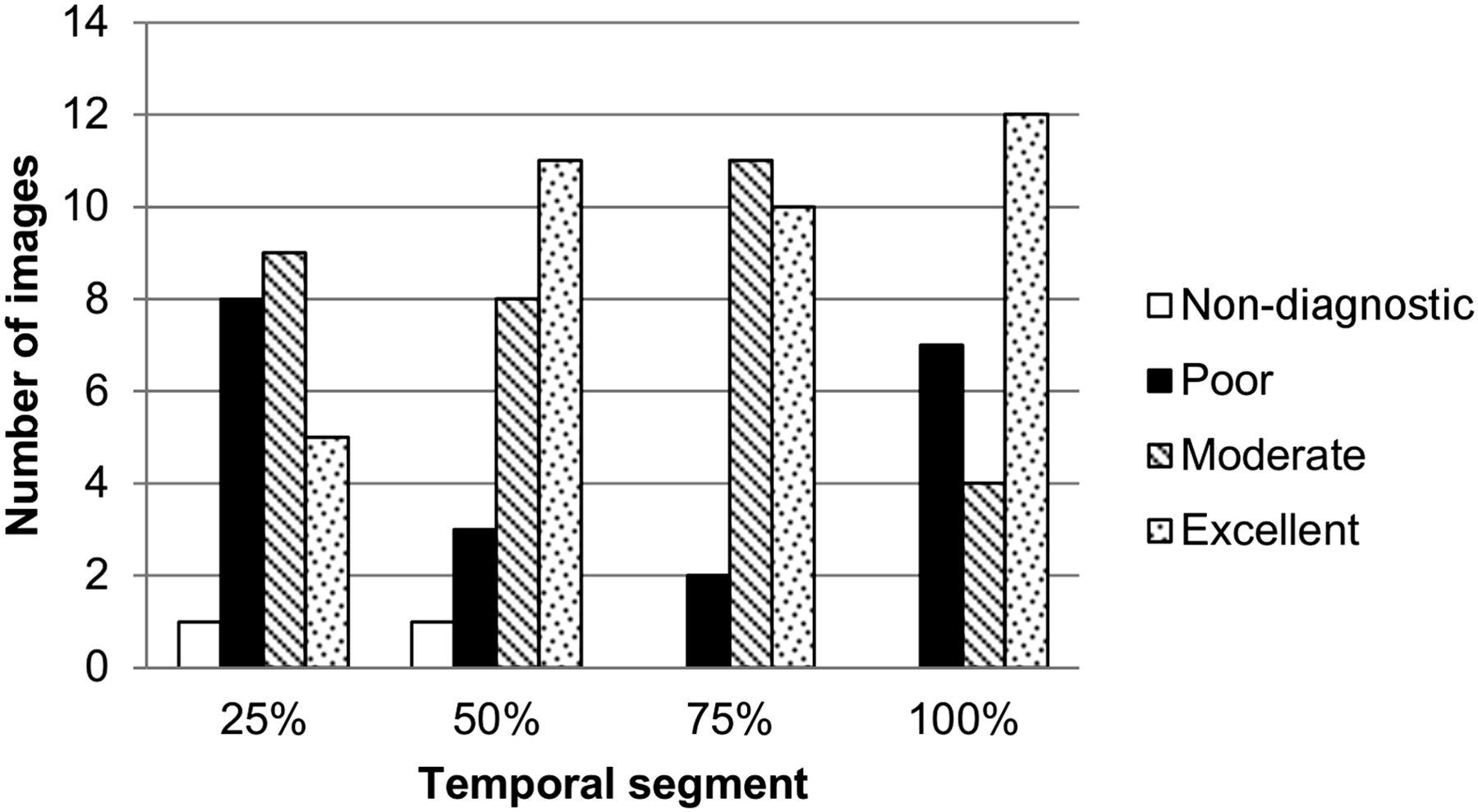
Assessment of image quality of temporally segmented image data.
DISCUSSION
The primary aim of this study was to establish the serial reproducibility of 18F-fluciclatide in a multicenter study to allow further investigation of this novel tracer as a biomarker of response to antiangiogenic and antiintegrin therapies. We have shown that 18F-fluciclatide has good reproducibility in several tumor types at all 3 time points after administration, with mean relative SUV differences of 0%–2% between the 2 imaging sessions and an SD range of 18%–20% for the mean. This reproducibility is consistent with reproducibility data obtained in large, multicenter studies assessing 18F-FDG and is acceptable for evaluation of tumor response to therapy (27).
Despite the widespread use of antiangiogenic drugs in the therapeutic setting, there are no validated biomarkers of response to therapy. Measurement of microvessel density by immunohistochemistry is the gold standard by which tumor angiogenesis is assessed. However, serial tumor biopsies are generally not acceptable in the clinical setting, and heterogeneity of microvessel density within the tumor limits the utility of this procedure further (31). A noninvasive method of assessing changes to tumor vasculature in response to treatment is therefore needed. There is expanding literature on the notion that tumor uptake of radiolabeled RGD peptides can reflect the angiogenesis phenotype. For example, tumor uptake of the RGD peptide 18F-galacto-RGD correlates with microvessel density (32,33). Moreover, Battle et al. demonstrated a serial reduction in 18F-fluciclatide uptake in tumors after treatment with the antiangiogenic agent sunitinib; a corresponding reduction in microvessel density was also observed (34). These findings are in keeping with the high affinity of RGD sequences for integrins expressed on tumor endothelial cells as reported by Pasqualini et al. (35). The ability of 18F-fluciclatide and other RGD probes to detect angiogenesis phenotype may be less dependent on tumor cell expression of the receptor. Melanoma, for example, has a higher expression of αvβ3 integrin in tumor cells than in the associated vasculature. However, work by our group, considering the uptake of 68Ga-DOTA-[c(RGDfK)]2 in melanoma and breast cancer models with varying αvβ3 expression, indicates that although the binding kinetics of RGD probes are influenced by αvβ3 expression on cells in vivo, the vessel fraction of αvβ3 integrin contributes maximally to the uptake of RGD probe, supporting its role as a biomarker of angiogenesis (36).
Several other tracers based on the cyclic RGD structure have been developed, with 18F-galacto-RGD being the only other probe to have undergone clinical studies, which showed SUV to correlate with αvβ3 expression in tumors (32). Other imaging modalities consider functional parameters such as blood flow, vessel permeability, and blood volume as surrogates of angiogenesis. Clinically, dynamic contrast-enhanced CT and MRI are widely used (37). However, clinical trials have demonstrated marked heterogeneity in the results obtained, with no correlation with response to antiangiogenic therapies being observed (38). Therefore, probes that directly image αvβ3 on tumor vasculature hold promise.
Knowledge of the precision of repeated imaging parameters is a prerequisite for serial response measurements and, therefore, response to treatment. Our study found no significant change in SUVpeak between the 2 scans; the 95% reference range of spontaneous fluctuations was 35%–39%. Thus, with the current protocol, a reduction in SUVpeak of at least 39% within any given lesion can be classified as an 18F-fluciclatide response. A similar level of reproducibility has been reported for 18F-FDG in a diverse range of tumor types and for 18F-fluorothymidine in breast cancer (27,39). Furthermore, our findings agree with those of Doot et al., who suggested that an SD of 20% in relative SUV change is typical of a multicenter trial with good calibration (23).
Not all tumors were visualized on 18F-fluciclatide PET scans compared with standard-of-care imaging. Because 18F-fluciclatide binds with high affinity to αvβ3/αvβ5 integrin, uptake of the tracer may be linked to differential expression of αvβ3/αvβ5 integrin within tumors. Beer et al. reported an 80% uptake of 18F-galacto-RGD in patients with malignancy and reported a correlation between SUV and expression of αvβ3 both within the tumor and within its associated microvasculature (17). Variability in uptake of both 18F-fluciclatide and 18F-galacto-RGD may reflect differential growth of tumors, with the expression of αvβ3 playing an important role during the initial phases of tumor growth, whereas an alternative angiogenic signaling mechanism may be more involved in metastases. Furthermore, tumor size may affect tracer uptake, with large tumors generally demonstrating areas of neoangiogenesis around the tumor periphery and the central area being relatively hypoxic, containing areas of necrosis.
In individual tumor types, Bland–Altman plotting indicated poor reproducibility for lung lesions and a case of renal cell cancer. Low reproducibility may be attributed to physiologic motion, particularly in patients with pleural lesions. Application of respiratory motion techniques may improve reliability in future studies. Pelvic lesions also showed reduced reproducibility, because physiologic uptake of 18F-fluciclatide within the bladder made their assessment difficult, a common limitation with 18F-FDG. Urinary excretion may have also contributed to the adverse reproducibility of the renal tumor. Although most lesions observed on standard-of-care imaging were observed on PET imaging, several lesions were not observed. Some lesions were based within the liver, where physiologic accumulation of 18F-fluciclatide occurs as a result of both metabolism and the dense vasculature of the liver, hampering visualization of hepatic tumors. Therefore, the clinical application of 18F-fluciclatide may be limited in those patients with predominantly pelvic and hepatic disease. However, a key issue directly affecting uptake of 18F-fluciclatide will be the expression level of αvβ3/αvβ5 integrin within the tumor and associated vasculature. Future studies would benefit from correlation of 18F-fluciclatide uptake characteristics with αvβ3/αvβ5 integrin expression within the tumor.
Temporal segmentation visual analysis did not identify large differences in image quality between 25% and 50% data despite the decreasing signal-to-noise ratio observed in the quantitative study of liver SUV. The mean SUVpeak decreased with increasing frame times. This is a slightly unusual result because increased image noise (e.g., in short dynamic image frames with low counts) usually results in a positive bias in SUV due to the nonnegativity constraint of ordered-subset expectation maximization reconstruction. However, because the SUV reported is far from zero, this effect should be small. One possible explanation is that the corrections (e.g., dead time and scatter) applied to the emission data are always based on the full acquisition and errors are introduced as the temporal segment is reduced.
CONCLUSION
We have shown in a multicenter study that 18F-fluciclatide PET imaging can be conducted with high reproducibility in several tumor types including breast and colorectal cancer and warrants further investigation as a response biomarker to antiangiogenic therapies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This paper presents independent research funded by GE Healthcare. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 17, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 27, 2015.
- Accepted for publication June 18, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}