


Abstract
This study was designed to assess the diagnostic value of 68Ga-NOTA-PRGD2 (NOTA-PRGD2 is NOTA-PEG4-E[c(RGDfK)]2) PET/CT in lung cancer. Methods: Ninety-one patients (48 men and 43 women; age, 22–82 y) with suspected lung lesions on CT were enrolled with informed consent. Immediately after intravenous injection of 117.7 ± 37.7 MBq of 68Ga-NOTA-PRGD2, 15 patients underwent dynamic whole-body PET/CT scans for 1–2 h, and the remaining 76 patients underwent whole-body PET/CT scans at 30 ± 10 min after bolus injection. Each patient also underwent standard 18F-FDG PET/CT for comparison. Results: No side effect was found after 68Ga-NOTA-PRGD2 injection. 68Ga-NOTA-PRGD2 was rapidly cleared from the blood pool and primarily excreted through the urinary system. The standardized uptake values of proven malignancies were significantly higher than those of the benign ones. With an average standardized uptake value of greater than 1.3 being considered malignant, the sensitivity, specificity, and accuracy of 68Ga-NOTA-PRGD2 PET/CT in diagnosing lung cancer were 83.8% (57/68), 91.3% (21/23), and 85.7% (78/91), respectively. The diagnostic value of 68Ga-NOTA-PRGD2 for lung cancer is comparable to that of 18F-FDG PET/CT. However, 68Ga-NOTA-PRGD2 PET/CT is more specific than 18F-FDG PET/CT in assessing lymph node metastasis, with positive and negative predictive values of 90.0% (27/30) and 93.8% (121/129), respectively, whereas those of 18F-FDG PET/CT were 30.2% (29/96) and 90.5% (57/63), respectively. Conclusion: This study indicates the efficacy of 68Ga-NOTA-PRGD2 PET/CT in lung cancer diagnosis. 68Ga-NOTA-PRGD2 PET/CT shows significant advantage over 18F-FDG PET/CT in judging metastatic lymph nodes with higher specificity.
The integrin family consists of 24 different heterodimerized transmembrane receptors, which play important roles in many physiologic and pathologic processes including cell survival, growth, differentiation, migration, inflammatory responses, platelet aggregation, tissue repair, and tumor invasion (1). Among them, integrin receptor αvβ3 is one of the key molecules participating in tumor angiogenesis, invasion, and metastasis (2–4). On the basis of the key role it plays in oncology and its easy accessibility as a cell surface receptor, integrin αvβ3 has been intensively investigated as a target for both therapeutic and diagnostic uses in various malignancies (5–8).
Several extracellular matrix proteins interact with integrin αvβ3 through the arginine-glycine-aspartic acid (RGD) tripeptide sequence, and thus cyclic RGD peptides with various modifications have been labeled with 99mTc (9) and 111In (10) for SPECT imaging and with 18F (11), 64Cu (12), 68Ga (13,14), and 89Zr (15) for PET imaging. The peptide modifications have included dimerization and polymerization of up to 8 cyclic RGD peptide units to increase binding affinity and the attachment of polar functional groups, such as sugar and polyethylene glycol (PEG), to increase renal excretion (16,17).
One clinical study reported the use of 68Ga-labeled RGD monomer in pediatric patients with moyamoya disease (18). Compared with the monomer, the dimeric RGD peptide binds the receptor in a divalent manner and is thus more preferable in targeting integrin-expressing cells both in vitro and in mouse models. Therefore, dimeric RGD is expected to have more intense uptake and more prolonged retention than the monomeric counterpart in integrin-expressing tumors (19,20).
Lung cancer is one of the leading causes of cancer mortality worldwide. PET imaging using 18F-FDG has become the standard of care in the initial management of patients with lung cancer, especially non–small cell lung cancer (21). However, false-positive 18F-FDG PET/CT results in nodal staging have been shown in patients with coexistent inflammatory or infectious diseases (22). Therefore, alternative imaging probes for accurate staging studies are necessary to assess the extent of disease and to determine appropriate treatment. In this study, we investigated the diagnostic value of a 68Ga-labeled RGD dimer, 68Ga-NOTA-PRGD2 (NOTA-PRGD2 is NOTA-PEG4-E[c(RGDfK)]2), for lung cancer using PET/CT.
MATERIALS AND METHODS
This clinical study was approved by the Institutional Review Board (IRB) of the Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College (IRB protocol S-417). All subjects signed a written informed consent form. This study was registered at the National Institutes of Health ClinicalTrials.gov (NCT01737112).
Volunteers and Patients
To validate the safety of 68Ga-NOTA-PRGD2 PET/CT, 7 healthy volunteers (3 men and 4 women; age, 38–65 y; mean age ± SD, 48 ± 9 y) were enrolled (the supplemental data provides more details; supplemental materials are available at http://jnm.snmjournals.org). To study the diagnostic value of 68Ga-NOTA-PRGD2 PET/CT, 91 patients (48 men and 43 women; age, 22–82 y; 56.5 ± 14.9 y) with suspected lung lesions according to CT were enrolled. The inclusion criteria were age 18 y or older, identified with lung lesion by CT in suspicion of primary lung cancer, and ability to provide basic information and sign the written informed consent form. The exclusion criteria included claustrophobia, possible pregnancy, lactation, kidney or liver failure, and inability to fulfill the study. Of the 91 patients recruited, 68 patients (36 men and 32 women; age, 30–82 y; 58.7 ± 12.9 y) were diagnosed as having lung cancer, based on the pathologic result of surgical removal or biopsy. Twenty-three benign diagnoses (12 men and 11 women; age, 22–76 y; 50.1 ± 18.6 y) were made on both pathologic results (n = 19) and follow-up (n = 4). The follow-up CT or PET/CT reexaminations in the 4 patients were obviously diminished after antiinflammatory treatment and disappeared after 6 mo to 1 y. The detailed diagnostic information of all patients is listed in Table 1.
Patient Information and Diagnosis
68Ga-NOTA-PRGD2 Preparation
68Ga-NOTA-PRGD2 was synthesized in a sterile hot cell. The precursor NOTA-PRGD2 (14) was dissolved in deionized water to 1 μg/μL and stored at 4°C before use. Fresh 68Ga was eluted into 3 tubes (∼1.3 mL each) from the 68Ge/68Ga generator (ITG Co.) using 4 mL of 0.05 M HCL (J.T. Baker). A pipette (Thermo Co., USA) was used to draw 1,000 μL of 68GaCl3 eluent from the middle tube, and the radioactivity was measured. The solution was then mixed with 50 μL of 1.25 M NaOAc and 40 μL of stored precursor. After shaking, the mixture was kept in a 100°C metal heater (Gingko) for 10 min. After the product was cooled down to room temperature, a 0.22-μm aseptic filtration membrane was used for purification. Radio–thin-layer chromatography (Bioscan) was used to test the radiochemical purity with CH3OH:NH4OAc (v/v 1:1) as the developing solution. The radiochemical purity of the product 68Ga-NOTA-PRGD2 exceeded 97%.
Examination Procedures
A Siemens Biograph 128 mCT X scanner was used for 68Ga-NOTA-PRGD2 PET/CT. Volunteers and patients were asked to urinate right before examination. For 15 patients, after the whole-body low-dose CT scan (140 kV; 35 mA; pitch, 1:1; layer, 5 mm; layer spacing, 3 mm; matrix, 512 × 512; field of view, 70 cm), approximately 111 MBq (3 mCi) of 68Ga-NOTA-PRGD2 were injected intravenously, followed by immediate serial whole-body dynamic PET acquisitions. The duration was 3 s/bed position for the 1–8 phases, 6 s/bed position for the 9–14 phases, 60 s/bed position for the 15–17 phases, 120 s/bed position for the next several phases, and the last phase lasted for 240 s/bed position. The whole-body images were obtained in sequence, and the total scanning lasted for 1–2 h based on the patient’s height and number of phases. The other 76 patients underwent 68Ga-NOTA-PRGD2 PET/CT scans at 30 ± 10 min after injection.
Except for 1 patient with a benign lesion, all the other 90 patients underwent standard routine 18F-FDG PET/CT within 1 wk. Patients were asked to fast for at least 4 h before the examination, and the blood glucose levels were below 6.4 mM. After injection of approximately 7.4 MBq of 18F-FDG per kilogram, the patients were asked to rest quietly in a warm and dark room for about 1 h. Then, the patients underwent low-dose CT and PET scans from the pelvic bottom to the skull base. A scan usually included 5 or 6 bed positions according to the patient’s height, and each bed position lasted for 2 min.
Integrin Immunohistochemical Staining
Representative tumor and lymph node samples were fixed with 10% neutral-buffered formalin and embedded in paraffin. Five-micrometer-thick tissue sections were blocked with endogenous peroxidase using 3% H2O2 for 20 min. Sections were then washed 3 times with phosphate-buffered saline briefly in a buffer containing 1% polymerized bovine serum albumin and incubated with mouse antihuman monoclonal antibody against human integrin αvβ3 (1:200; SC-7312 [Santa Cruz Biotechnology]) at 37°C for 2 h. After being washed with phosphate-buffered saline, each section was incubated with horseradish peroxidase–conjugated antigoat IgG for 60 min at room temperature. Diaminobenzidine was used as the chromogen, and hematoxylin and eosin counterstaining was performed. Six fields were randomly selected from each section and observed using a light microscope (BX41; Olympus).
Data Analysis
The same physician measured all images with the same standard in the final analysis. A Siemens workstation (MultiModality Workplace) was used for postprocessing. The volume of interest of 15 normal organs/tissues and concerned lesions were drawn on the last set of the serial images, and the software automatically obtained the radioactivity concentration and standardized uptake value (SUV) in the volumes of interest. Prism 5.0 software (GraphPad Software, Inc.) was used for statistical analysis. The same physician compared and measured the 68Ga-NOTA-PRGD2 and 18F-FDG uptake in the lesions side by side. A receiver-operating-characteristic curve was used to set the threshold for diagnosis of lung cancer. The Student t test was used to compare the SUVs of different groups. The Z test was used to compare the performance of 68Ga-NOTA-PRGD2 and 18F-FDG PET/CT in evaluating lung cancer. A P value of less than 0.05 was considered statistically significant.
RESULTS
Lung Cancer Evaluation
The biodistribution and dosimetry studies in healthy volunteers showed predominant renal clearance of 68Ga-NOTA-PRGD2 and comparable total-body effective dose to that from routine 18F-FDG (more details are provided in the supplemental materials). The low background in the lung region allows the detection of lung lesions with high target-to-background ratio. Moreover, the activity in the heart and mediastinum vasculature faded away quickly, which facilitates easy recognition of abnormal lymph nodes. All positive lesions, including primary tumors, lymphatic and bone metastases, and benign foci could be clearly observed at 30–45 min after intravenous injection of 68Ga-NOTA-PRGD2 (Fig. 1). The lesions with prominent 68Ga-NOTA-PRGD2 uptake appeared to be integrin αvβ3–positive.
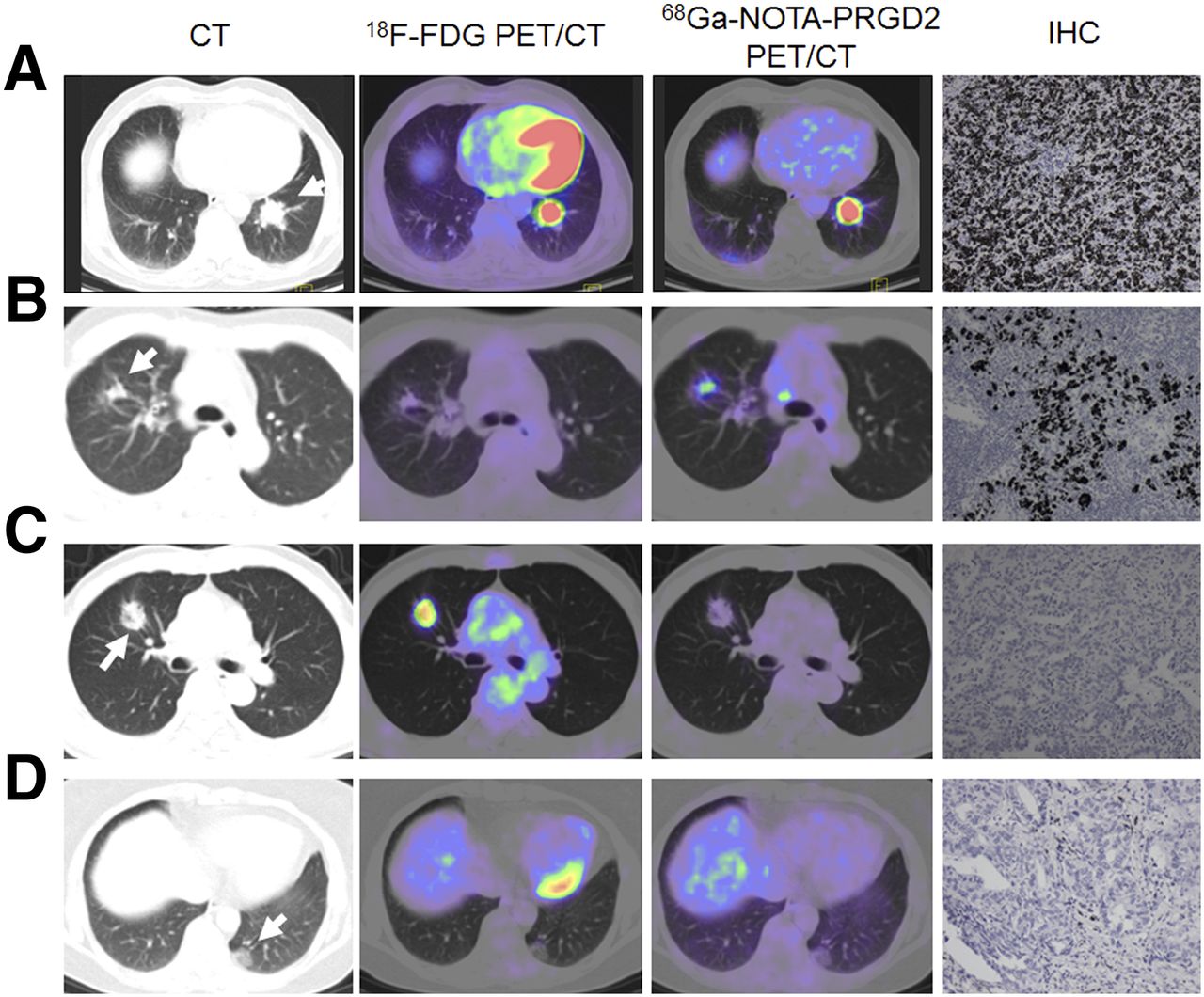
CT, 18F-FDG PET/CT, and 68Ga-NOTA-PRGD2 PET/CT images and immunohistochemical (IHC) staining of primary lung cancer. Arrows point to tumor. (A) A 76-y-old man with moderately differentiated adenocarcinoma in inferior lobe of left lung. Lesion is visualized by both 18F-FDG and 68Ga-NOTA-PRGD2 PET, with SUVavg/SUVmax of 8.9/14.5 and 4.3/6.1, respectively. Tumor sections show positive integrin αvβ3 staining. (B) A 37-y-old woman with highly differentiated adenocarcinoma in superior lobe of right lung. Lesion is visualized only on 68Ga-NOTA-PRGD2 PET with SUVavg/SUVmax of 1.7/2.3. Tumor sections show positive integrin αvβ3 staining. (C) A 61-y-old woman with highly differentiated adenocarcinoma in superior lobe of right lung. SUVavg/SUVmax of 18F-FDG and 68Ga-NOTA-PRGD2 PET were 2.8/4.7 and 0.8/1.3, respectively. Tumor sections show negative integrin αvβ3 staining. (D) A 61-y-old woman with highly differentiated adenocarcinoma. CT shows lesion with ground-glass opacity in inferior lobe of left lung. Both 18F-FDG and 68Ga-NOTA-PRGD2 PET show low tracer uptake within lesion with SUVavg/SUVmax of 0.7/0.9 and 0.1/0.2, respectively. Tumor sections show sparsely positive integrin αvβ3 staining.
In the 68Ga-NOTA-PRGD2 PET/CT images of the patients, the average SUV (SUVavg) and maximum SUV (SUVmax) of malignances at 30 min after injection were 2.12 ± 1.30 and 3.66 ± 2.87, respectively, which were significantly higher than those of the benign ones (SUVavg = 0.94 ± 0.43 and SUVmax = 1.57 ± 0.71, P < 0.05). The mean SUV of normal lung tissue was 0.31 ± 0.19, and the mean SUV of normal aortic arch was 0.85 ± 0.44. Using the receiver-operating-characteristic curve and area under the curve of SUV data of 68Ga-NOTA-PRGD2 PET/CT, we determined a threshold of 1.3 for SUVavg and 2.0 for SUVmax. The sensitivity, specificity, and accuracy of 68Ga-NOTA-PRGD2 PET/CT in the diagnosis of lung cancer were 83.8% (57/68), 91.3% (21/23), and 85.7% (78/91), respectively, using a cutoff value of 1.3 for SUVavg. The minimal size of detected tumor was 7.5 mm as measured on the CT images using a cutoff value of 1.3 for SUVavg. When SUVmax with a cutoff value of 2.0 was used, the sensitivity, specificity, and accuracy of 68Ga-NOTA-PRGD2 PET/CT in the diagnosis of lung cancer were 80.9% (55/68), 82.6% (19/23), and 81.3% (74/91), respectively. For 18F-FDG PET/CT, with a cutoff SUVavg value of 2.0, the sensitivity, specificity, and accuracy were 86.8% (59/68), 69.6% (16/23), and 82.4% (75/91), respectively. With an SUVmax cutoff value of 3.0, the sensitivity, specificity, and accuracy of 18F-FDG PET/CT in the diagnosis of lung cancer were 85.3% (58/68), 69.6% (16/23), and 81.3% (74/91), respectively. The critical ratio z for comparing 68Ga-NOTA-PRGD2 and 18F-FDG PET/CT in evaluating lung cancer was 1.033 for SUVavg (P = 0.30) and 0.077 for SUVmax (P = 0.94).
Both SUVavg and SUVmax of 18F-FDG were significantly higher than those of 68Ga-NOTA-PRGD2 (P < 0.0001). There was no significant correlation between the 18F-FDG uptake and the 68Ga-NOTA-PRGD2 accumulation. There was no significant difference in 68Ga-NOTA-PRGD2 accumulation and 18F-FDG uptake in primary lung lesions with or without metastatic lymphonodus (P = 0.87 and 0.86, respectively). The SUVavg and SUVmax of adenocarcinoma (n = 43) at 30 min after injection of 68Ga-NOTA-PRGD2 were 1.78 ± 1.81 and 3.36 ± 3.42, respectively, and those of squamous cell carcinoma (n = 15) were 2.12 ± 1.05 and 4.43 ± 2.31, respectively. There was no significant difference between the 2 types of tumors (P = 0.63 for SUVavg and P = 0.49 for SUVmax). When all the tumors were graded as high, moderate, or low differentiation, no significant correlation was found between SUVs and grade of tumor (correlation coefficient r = 0.208, P > 0.05).
Lymph Node Evaluation
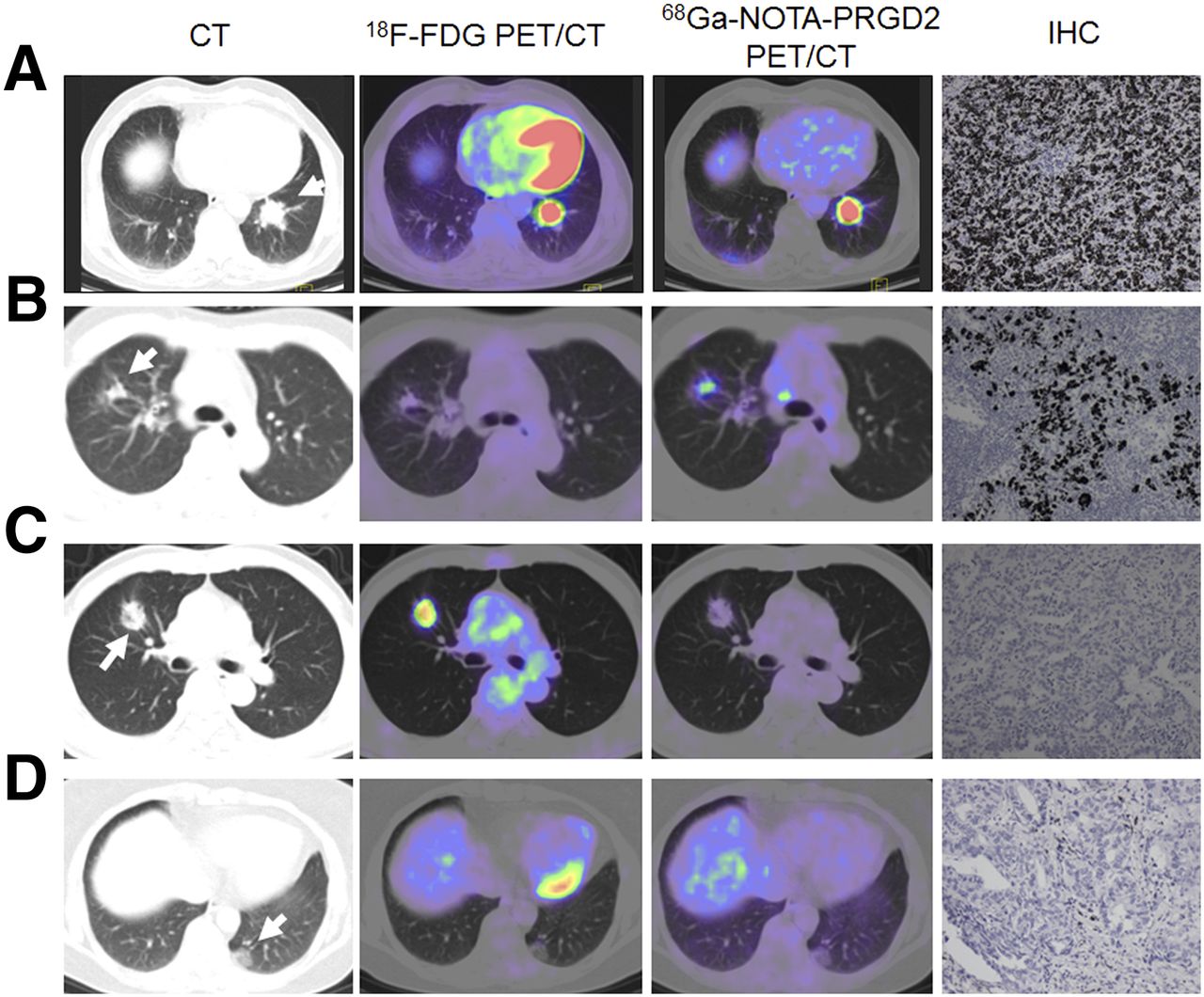
For lymph node staging, 38 patients, including 3 cases of chronic inflammation and 35 cases of lung cancer, went through surgery and had confirmed multiregion lymphonodus results. Two hundred nine regions of lymphonodi were recognized from surgery with varied sizes from 0.1 to 2.0 cm. Among them, 50 were too small (<0.5 cm as measured by histopathology) to be identified with the images. In the remaining 159 regions, 35 were metastatic and 124 were normal. As summarized in Table 2, we graded the 18F-FDG uptake and RGD accumulation in 3°: high, moderate, and low. The representative PET images and immunohistochemical staining of lymph nodes are shown in Figure 2. Among the 124 negative lymph nodes, only 3 had low-to-moderate RGD accumulation, but for 18F-FDG, 29 had moderate and 38 had high uptake. In 35 malignant lymph nodes, 8 had very low RGD accumulation, 6 had low-to-moderate accumulation, and 21 had moderate-to-high uptake. If the latter 2 are defined as a sign for metastasis, the positive and negative predictive values of RGD for the assessment of lymph node metastasis were 90.0% (27/30) and 93.8% (121/129), whereas those of 18F-FDG were 30.2% (29/96) and 90.5% (57/63). Quantitative analysis showed the RGD SUVmax of nonmetastatic and metastatic lymphonodi were 0.75 ± 0.75 and 1.93 ± 1.03, respectively (P < 0.05), whereas the 18F-FDG SUVmax of nonmetastatic and metastatic lymphonodi were 2.30 ± 2.31 and 3.91 ± 2.37, respectively (P = 0.48). No apparent correlation between the 18F-FDG uptake or 68Ga-NOTA-PRGD2 accumulation in lymph nodes (Table 2) and the final staging of the 38 patients was found.
18F-FDG Uptake and 68Ga-NOTA-PRGD2 Accumulation in Lymph Nodes

18F-FDG PET/CT and 68Ga-NOTA-PRGD2 PET/CT images and immunohistochemiscal (IHC) staining of lymph nodes within lung region. Arrows point to lymph nodes. (A) A 69-y-old woman with moderately differentiated adenocarcinoma with lymph node metastasis. Both 18F-FDG and 68Ga-NOTA-PRGD2 PET show positive lymph nodes with positive integrin αvβ3 staining. (B) A 44-y-old woman with highly differentiated adenocarcinoma with lymph node metastasis. Lymph node is negative on 18F-FDG PET and positive on 68Ga-NOTA-PRGD2 PET with positive integrin αvβ3 staining. (C) A 58-y-old woman with adenocarcinoma with no lymph node metastasis. However, 18F-FDG PET shows positive lymph nodes whereas 68Ga-NOTA-PRGD2 PET shows negative result with negative integrin αvβ3 staining. (D) A 62-y-old woman with highly differentiated adenocarcinoma with no lymph node metastasis. Both 18F-FDG and 68Ga-NOTA-PRGD2 PET show negative lymph nodes with negative integrin αvβ3 staining.
DISCUSSION
As a diagnostic study, only a trace amount of NOTA-PRGD2 was used to target the integrin receptor αvβ3, so no biologic effect was expected. Indeed, no side effect was found according to the safety data. The results are in accordance with other RGD peptide–based PET tracers such as 18F-galacto-RGD, 18F-AH111585, 18F-RGD-K5, 68Ga-NOTA-RGD, 18F-alfatide, and 18F-FPPRGD2 (23–29).
18F-FDG PET has been intensively applied for diagnosis and staging of lung cancer. However, large variations in sensitivity, specificity, and accuracy in lung cancer diagnosis have been reported (30,31). The accuracy of 18F-FDG PET for diagnosing lung nodules was extremely heterogeneous (32). In this study, the sensitivity of 18F-FDG PET was 86.8%, which is within the range of literature reports. Compared with 18F-FGD PET, 68Ga-NOTA-PRGD2 PET showed lower sensitivity but higher specificity. However, there is no significant difference between the diagnostic values of these 2 tracers. Whether the combination of 68Ga-NOTA-PRGD2 and 18F-FDG will have added value to increase the specificity will need further investigation with a larger patient population.
68Ga-NOTA-PRGD2 PET appears to merit lymph node metastasis assessment, which is important for clinical decision making and surgical planning for lung cancer patients. Although 18F-FDG PET/CT improves the accuracy of N staging, it still cannot replace invasive staging methods, such as mediastinoscopy, mainly because of its relatively low specificity and high uptake in the inflammatory lymph nodes (33). In this study, a remarkable improvement of positive predictive value was demonstrated from 30.2% (29/96) in 18F-FDG PET/CT to 90% (27/30) in 68Ga-NOTA-PRGD2 PET/CT. Thirty-five regions of malignant lymphonodi, including the 1 as small as 0.6 cm, were detected by 68Ga-NOTA-PRGD2 PET/CT. Active inflammatory lymphonodi are the main reasons of the false-positive results in 18F-FDG PET/CT (31). Most 18F-FDG–avid lymph nodes in acute or chronic inflammation are characterized by lymphoid follicular hyperplasia that cause high 18F-FDG uptake but not necessarily express integrin αvβ3. 68Ga-NOTA-PRGD2 PET/CT shows advantages over 18F-FDG PET/CT in the differentiation of malignant and inflammatory lymphonodi. It is also of note that we performed both visual analysis and semiquantitative SUV analysis, and visual analysis is preferred and SUV would be a secondary aid (34).
Because RGD peptide tracers bind specifically with integrin αvβ3, there have been numerous reports of positive correlation of tracer uptake with the receptor density (35,36). We also observed a similar correlation between 68Ga-NOTA-PRGD2 SUVs with immunohistochemical staining results. Because we did not have access to all the tumor tissues, it is thus not possible for us to perform a systematic analysis to answer the question of whether a metastatic lymph node is always integrin-positive. There is also concern about the lymph node lesion size. In this study, 50 of 209 regions of lymphonodi that were smaller than 0.5 cm were directly excluded from the analysis, which may have caused a negative diagnosis in both 18F-FDG and 68Ga-NOTA-PRGD2 scans.
CONCLUSION
68Ga-NOTA-PRGD2 is a safe PET agent that offers good human tolerance and clear images. 68Ga-NOTA-PRGD2 PET/CT has a sensitivity similar to and specificity higher than 18F-FDG PET/CT in the detection and differentiation of lung lesions. Moreover, 68Ga-NOTA-PRGD2 PET/CT shows significant advantage over 18F-FDG PET/CT for N staging of lung cancer, with a remarkable improvement of positive predictive value in the assessment of lymph node metastasis.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by the Capital Special Project for Featured Clinical Application (Z121107001012119), the National Natural Science Foundation of China projects (81171369, 81171370, 81371596, and 81271614), the Ministry of Education of China (311037), Young Scientist Research Funding of Peking Union Medical College Hospital (PUMCH2013), and the Intramural Research Program (IRP) of the National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institutes of Health (NIH). No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 1, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication September 16, 2015.
- Accepted for publication September 21, 2015.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Targeted Radionuclide Therapy in Patient-Derived Xenografts Using 177Lu-EB-RGD
- Primary Preclinical and Clinical Evaluation of 68Ga-DOTA-TMVP1 as a Novel VEGFR-3 PET Imaging Radiotracer in Gynecological Cancer
- In Vivo Characterization of 4 68Ga-Labeled Multimeric RGD Peptides to Image {alpha}v{beta}3 Integrin Expression in 2 Human Tumor Xenograft Mouse Models
- PET response assessment in apatinib-treated radioactive iodine-refractory thyroid cancer