


Abstract
Despite the favorable prognosis of stage IA non–small cell lung cancer (NSCLC), the disease recurs after complete surgical resection in 20%–30% of patients. This study determined the prognostic value of various metabolic parameters of 18F-FDG PET/CT in surgically resected stage IA NSCLC. Methods: We retrospectively reviewed 248 patients with stage IA NSCLC who underwent lobectomy and complete lymph node dissection after PET/CT. A region of interest was drawn on the primary lesion, and metabolic indices such as metabolic tumor volume, maximum standardized uptake value (SUVmax), and total lesion glycolysis (TLG) were measured using an SUV cutoff of 2.5. Results: The patients included 134 men and 114 women, and the mean age was 63.03 ± 10.01 y; 129 were stage T1a (≤2 cm) and 119 were T1b (>2 cm). The median follow-up period was 36.6 mo. Recurrence took place in 15 patients. The mean (±SD) SUVmax, metabolic tumor volume, and TLG were 4.55 ± 3.75, 5.92 ± 5.57, and 14.42 ± 17.35, respectively. The cutoffs of SUVmax and TLG were 3.7 and 13.76, respectively. The 5-y overall survival (OS) was 95.1% in low-SUVmax patients and 82.2% in high-SUVmax patients (P = 0.02). The 5-y OS was 93.7% in low-TLG patients and 78.3% in high-TLG patients (P = 0.01). On multivariate analysis, TLG was a risk factor for OS (hazard ratio, 3.159; P = 0.040), but SUVmax showed marginal significance (P = 0.064). The concordance index of the TLG model was 0.676 (95% CI, 0.541–0.812). Conclusion: TLG was a significant prognostic factor for OS in patients with stage IA NSCLC.
Lung cancer is the second most common cancer in both men and women and the most common cause of cancer death in the world (1). Non–small cell lung cancer (NSCLC) accounts for 80%–85% of all lung cancer cases. Oncologic treatment options for NSCLC typically include surgery, radiation, and chemotherapy, either alone or in combination. TNM stage has been considered the primary prognostic factor in NSCLC. However, tumor- and patient-specific factors vary even within the same disease stage, creating a heterogeneous population of patients, each with an individual prognosis that requires consideration of patient- and tumor-specific factors for best estimation (2,3). Recently, the incidence of early-stage NSCLC has increased as a result of the use of low-dose CT for screening. However, despite having early-stage disease, up to 20%–30% of patients with stage IA NSCLC relapse after surgical treatment. Therefore, other prognostic factors besides TNM stages are needed to identify patients at high risk for recurrence, predict prognosis, and recommend individualized adjuvant therapy (4).
18F-FDG PET relies on the fact that most neoplasms are highly metabolically active and therefore can be detected on a background of relatively less active normal tissues. When performed in addition to qualitative evaluation by visual inspection, 18F-FDG PET can provide several semiquantitative measurements of radioactivity concentration in each tissue compartment, such as standardized uptake value (SUV) (5). Maximum SUV (SUVmax) has been reported as a prognostic factor in surgically treated NSCLC. However, a single highly metabolic focus may not accurately reflect the metabolic activity of the whole tumor. To compensate for this factor, volume-based parameters such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG) have been explored as measures of the metabolic burden of the whole tumor. MTV indicates the volume of metabolically active tumor, and TLG is the product of mean SUV and MTV (6). Studies have shown that TLG is a better index of patient prognosis than SUVmax in advanced NSCLC (7–12). However, the prognostic role of volume-dependent parameters in stage IA NSCLC has not been reported.
This study was conducted to document the prognostic role of volume-based parameters in patients with stage IA NSCLC who underwent lobectomy and mediastinal lymph node dissection. Furthermore, the importance of volume-based parameters as a prognostic factor was compared with that of the conventional PET parameter, SUVmax.
MATERIALS AND METHODS
Materials
The institutional review board approved this retrospective study (4-2014-590), and the requirement to obtain informed consent was waived. A total of 248 patients who were confirmed to have pathologic stage IA NSCLC after lobectomy and complete lymph node dissection in the Yonsei University College of Medicine between January 2006 and November 2011 were enrolled. We retrospectively reviewed the medical records, PET data, and pathologic data. Chest CT, PET/CT, bronchoscopy, and pulmonary function testing were performed preoperatively. Pure ground glass opacity lesions were excluded from this analysis. Postoperatively, chest CT scans were obtained at 3-mo intervals and PET/CT scans were obtained annually to detect recurrence. Local recurrence was defined as that occurring on resection margins, such as bronchial stumps or stapler lines. Regional recurrence was defined as that occurring in the hilar or mediastinal lymph nodes, pleural cavity, or ipsilateral lung. Distant recurrence was defined as that occurring in the contralateral lung, brain, liver, adrenal glands, bone, or other locations.
18F-FDG PET/CT Protocol
All patients underwent routine 18F-FDG PET/CT on either a Discovery 600 PET/CT scanner (GE Healthcare) or a Biograph TruePoint 40 PET/CT scanner (Siemens Medical Systems, CTI). The patients fasted for at least 6 h, and glucose levels in the peripheral blood in all patients were confirmed to be no more than 140 mg/dL before 18F-FDG injection. Approximately 5.5 MBq of 18F-FDG per kilogram of body weight were administered intravenously 1 h before image acquisition. After the initial low-dose CT (Discovery 600: 30 mA, 130 kVp; Biograph TruePoint 40: 36 mA, 120 kVp), standard PET imaging from the neck to the proximal thighs with an acquisition time of 3 min/bed position in 3-dimensional mode was performed. Images were reconstructed using ordered-subset expectation maximization (2 iterations, 20 subsets).
Images were reviewed by an experienced nuclear medicine specialist using an AW 4.0 workstation (GE Healthcare). A volume of interest was drawn on the primary lesion. The SUVmax of the primary lesion was obtained and recorded. TLG of the primary lesion was also obtained using an SUV cutoff of 2.5; if the volume of interest was out of proportion to the lesion seen on CT, an isocontour with variable threshold levels was used to best fit the contour of the lesion on CT. TLG was calculated by multiplication of MTV (volume, cm3) by mean SUV within the volume of interest. A representative example of measuring and calculating TLG is shown in Figure 1. In Figure 1A, a 2.2-cm adenocarcinoma in the right middle lung (T1b, stage IA) showed mild uptake (SUVmax, 2.0; MTV, 7.3 cm3; TLG, 8.8). In Figure 1B, a 2.7-cm adenocarcinoma in the right lower lung showed intense uptake (SUVmax, 17.8; MTV, 7.4 cm3; TLG, 47.6).

Representative examples of relationship between 18F-FDG uptake and recurrence. (A) A 70-y-old woman was diagnosed with adenocarcinoma (2.2 cm) in right middle lung (T1b, stage IA). Lesion showed mild uptake (SUVmax, 2.0; MTV, 7.3 cm3; TLG, 8.8). Patient survived follow-up period of 4.4 y without recurrence. (B) A 62-y-old man was diagnosed with adenocarcinoma (2.7 cm) in right lower lung (T1b, stage IA). Lesion showed intense uptake (SUVmax, 17.8; MTV, 7.4 cm3; TLG, 47.6). Patient experienced recurrence 2.3 y after operation.
Statistical Analysis
Statistical analysis was performed using the open-source statistical software R (http://www.R-project.org). Clinical and pathologic parameters were described as mean ± SD for continuous variables and frequency followed by percentage for categoric variables. The correlation between SUVmax and TLG was calculated by the Pearson correlation test. The primary endpoint was overall survival (OS), which was measured from the date of operation to the date of death from any cause or last clinical follow-up. The Kaplan–Meier method and log-rank test were used to perform univariate survival analysis, and the Cox proportional hazards model was used to identify independent prognostic factors. A parameter was included in the Cox proportional hazards model if the P value was less than 0.2 on the log-rank test or if it was a previously proven risk factor. The maxstat package for maximally selected rank statistics was used to detect the optimal cutoff of each volume-dependent parameter. The survcomp packages for performance assessment, calculation of concordance index, and comparison of several Cox proportional hazards models were used for analyses (12,13). All tests were 2-sided, and the criterion for significance was a P level of less than 0.05.
RESULTS
General Characteristics of Patients
The 248 patients included 134 men (54%) and 114 women (46%), with a mean age of 63.03 ± 10.01 y. The median follow-up period was 36.6 mo (range, 1.2–87.5 mo). Regarding tumor stage, 129 (52%) were reported as T1a (≤2 cm) and 119 (48%) as T1b (>2 cm to ≤3 cm). The mean number of dissected lymph nodes was 21.50 ± 9.38. The general characteristics of the patients are shown in Table 1.
General Characteristics of Patients
Among the 248 patients, the mean SUVmax was 4.55 ± 3.75, the mean MTV was 5.92 ± 5.57, and the mean TLG was 14.42 ± 17.35. SUVmax and TLG showed a positive correlation, with a Pearson correlation coefficient of 0.522 (P < 0.001). On the basis of maximally selected rank statistics, the optimal cutoffs for SUVmax and TLG were 3.7 and 13.76, respectively; 121 patients (48.8%) showed an SUVmax above 3.7, and 83 (33.5%) showed TLG above 13.76. The patients were divided into 2 groups based on the results of maximally selected rank statistics: high SUVmax (>3.7, n = 121, 48.8%) versus low SUVmax (≤3.7, n = 127, 51.2%) and high TLG (>13.76, n = 83, 33.5%) versus low TLG (≤13.76, n = 165, 66.5%).
Patterns of Recurrence and Survival Analysis
Recurrence was reported in 15 patients (6.05%) as follows: 1 case of local recurrence (bronchial stump), 4 cases of regional recurrence (1 pleural seeding, 1 mediastinal lymph node, and 2 ipsilateral lung), and 10 cases of distant recurrence (3 contralateral lung, 2 brain, 2 bone, 2 neck node, and 1 spine).
According to the Kaplan survival model, the 5-y OS was 88.4% and 5-y disease-free survival was 83.2% in all patients (Fig. 2). The 5-y OS was 95.1% in low-SUVmax patients compared with 82.2% in high-SUVmax patients (P = 0.02; Fig. 3A) and was 93.7% in low-TLG patients compared with 78.3% in high-TLG patients (P = 0.01; Fig. 3B).
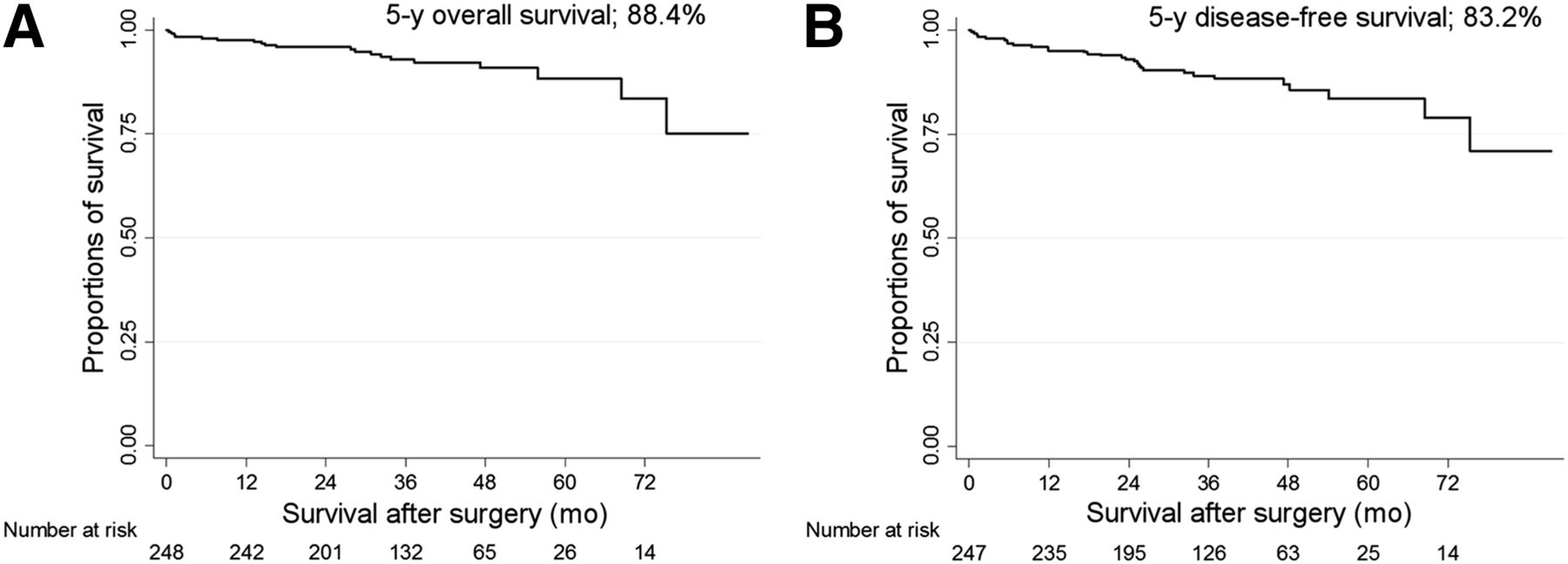
(A) OS in all patients. (B) Disease-free survival in all patients.

(A) OS curves according to SUVmax. (B) OS curves according to TLG.
Risk Factors for OS and Comparison of Concordance Index
In univariate analysis, old age, the male sex, larger tumor size, the presence of adenocarcinoma, high SUVmax, and high TLG were risk factors for OS (Table 2). On the basis of the univariate analysis results, 3 different multivariate Cox proportional hazards models were established to compare the predictive power of each PET parameter. For model 1, which excluded the PET parameters, age (hazard ratio [HR], 1.085) and adenocarcinoma (HR, 0.370) were risk factors for OS. For model 2, which included SUVmax and tumor size in the analysis, age (HR, 1.083) was the only risk factor for OS, although SUVmax showed marginal significance. For model 3, which included TLG and MTV instead of SUVmax and tumor size because TLG included information on tumor size, age (HR, 1.079) and TLG (HR, 3.159) were risk factors for OS.
Cox Proportional Hazards Models for Predicting Risk Factors of OS in Stage IA NSCLC
The concordance index was calculated for each Cox proportional hazards model. The concordance indices of models 1, 2, and 3 were 0.663 (95% CI, 0.525–0.801), 0.668 (95% CI, 0.528–0.807), and 0.676 (95% CI, 0.541–0.812), respectively (Table 2). The concordance indices of the TLG model (model 3) and the SUVmax model (model 2) were superior to that of the tumor size model (model 1 vs. model 2, P = 0.006; model 1 vs. model 3, P = 0.005). Although the TLG model showed a higher concordance index than the SUVmax model, the difference was not statistically significant (P = 0.306).
DISCUSSION
This study demonstrated that high TLG was related to poor OS in our patients with surgically resected stage IA NSCLC. As far as we know, this study was the first to analyze the influence of volume-dependent parameters of PET/CT as risk factors for OS in stage IA NSCLC.
Although SUV is recognized as a PET parameter related to survival in surgically treated NSCLC, SUV has several important limitations. First, the SUV depends largely on many biologic factors (body weight, serum glucose level) and technologic factors (interscanner variability, image reconstruction method). Second, SUVmax does not take the volume of the tumor lesion into account, and this limitation may be significant because tumor volume is a well-known prognostic determinant (11). Third, SUV measures a single highly metabolic focus that may not accurately reflect the metabolic activity of the whole tumor. To overcome these limitations of SUV, MTV and TLG have been studied as prognostic factors for NSCLC (7,8,10,14,15). Another advantage of TLG and MTV over SUV is that multiple lesions can be summed to determine the metabolic tumor burden in multiple sites. These lesions can also be categorized according to TNM stage, detemining metabolic tumor burden according to stage. A recent paper by Liao et al. has shown that MTV and TLG grouped according to TNM stage were prognostic of patient survival independent of clinical stage (10). Other studies have confirmed that TLG and MTV are better indices of patient survival than SUVmax or mean SUV (7,8,10,14,15). Previous studies focused primarily on advanced-stage disease, and few studies have reported the role of volume-based parameters in early-stage NSCLC. Hyun et al. evaluated preoperative MTV and TLG in 529 patients with early-stage (stages I and II) NSCLC that was treated surgically (9). In multivariate analyses, MTV and TLG were significantly associated with an increased risk of recurrence and death, independent of histology, tumor stage, and type of surgery. SUVmax was not a significant prognostic factor in their report. They also analyzed the outcomes of 299 patients with stage I NSCLC as a subset analysis and showed that MTV and TLG were additional significant risk factors in stage I NSCLC. Melloni et al. analyzed 99 patients with surgically treated stage I NSCLC and reported that TLG seemed to be an accurate prognostic factor for recurrence (11).
In this study, we analyzed only stage IA NSCLC to evaluate the prognostic influence of volume-dependent parameters. Our data indicated that TLG was the only significant risk factor for OS, although SUVmax showed marginal significance as a prognostic factor. Among the volume-dependent parameters, TLG was a prognostic factor but MTV was not. These results are consistent with the previous report by Melloni et al. (11). The advantage of this study over previous studies lies in the use of the concordance index of several Cox proportional hazards models to compare the importance of PET parameters as a prognostic factor. Concordance in survival analysis is defined as the probability of agreement for any 2 randomly chosen patients such that the patient with the shorter survival time has the larger risk score and a value of 1 indicates perfect agreement (16,17). The concordance index of the TLG model was higher than that of other models, implying that the TLG model may predict survival most precisely.
Our analysis of stage IA NSCLC has important implications in clinical situations. First, it may enable risk stratification among patients with stage IA NSCLC. Despite the early stage of disease, approximately 20%–30% of these patients experience recurrence during the follow-up, and this recurrence is related to poor OS. It may be beneficial to further postoperatively treat patients who have stage IA NSCLC and high TLG because high TLG is related to poor OS after surgical treatment. Therefore, it may be possible to tailor individualized therapy for stage IA lung cancer, although a large-scale prospective study is needed to confirm our results. Another application of TLG in stage IA NSCLC lies in the extent of surgery. Generally, anatomic resection such as lobectomy and mediastinal lymph node dissection is standard surgical treatment in lung cancer surgery, even in early-stage disease. Recently, sublobar resection such as segmentectomy or wedge resection has been applied in cases of early-stage lung cancer (<2 cm in size or with ground glass opacity) as a clinical trial. Patients with stage IA NSCLC with high TLG may have a higher risk of recurrence than patients with low TLG; therefore, the application of sublobar resection should be avoided. The level of TLG may therefore be an indication of sublobar resection in clinical situations.
This study has the limitation that we initially hypothesized that TLG may show better predictive performance than SUVmax. Even though the concordance index of the TLG model was slightly higher than that of SUVmax, the difference was not statistically significant. This may be because the small size of the stage IA NSCLC lesions means that they are influenced by partial-volume effects to a greater extent than larger lesions (18). On the other hand, our analysis may be considered a more reliable correlation study between the metabolic activity of small tumors and prognosis because we reduced size variability by selecting only stage IA patients. Analysis of a larger number of patients is needed to confirm whether TLG shows better predictive power. Despite these limitations, to our knowledge this study is the first analysis of surgically resected stage IA NSCLC.
CONCLUSION
High TLG was shown to be a risk factor for OS in patients with surgically treated stage IA NSCLC. Patients with high TLG should be closely observed for recurrence and may benefit from adjuvant therapy. Additionally, high TLG in stage IA NSCLC may be a relative contraindication for sublobar resection in early lung cancer.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Dec. 18, 2014.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 22, 2014.
- Accepted for publication November 25, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.