


Abstract
This work was performed to evaluate the performance of 18F-fluorodihydroxyphenylalanine (18F-FDOPA) PET/CT in detecting primary neuroendocrine tumors (NETs) occult on morphologic and functional imaging, in relation to tumor origin and differentiation. Methods: A retrospective study of NET patients who were investigated with 18F-FDOPA PET/CT imaging in 2 academic endocrine tumor centers was conducted. Only patients with negative conventional and somatostatin receptor scintigraphy (SRS) results were studied. Results: Twenty-seven patients were evaluated with 18F-FDOPA PET/CT, 23 at their initial staging and 4 during their follow-up. The primary occult NET was localized by 18F-FDOPA PET/CT in 12 patients (overall sensitivity, 44%; 52% in patients evaluated at initial diagnosis), leading to tumor resection in all cases. The primary tumors were distributed and graded as follows: 1 duodenum G2 lesion, 7 ileum G2 lesions, 2 terminal ileum G1 lesions, 1 pancreas G2 lesion, and 1 gallbladder G3 lesion. Patients with positive 18F-FDOPA PET/CT results had higher values of serum chromogranin A (100% vs. 20%, P = 0.0003), serotonin, or urinary 5-hydroxyindolacetic acid (83% vs. 20%, P = 0.003). Two false-negative results were related to poorly differentiated duodenal and prostatic NETs (G3). 18F-FDOPA PET/CT showed more metastatic anatomic regions than SRS in 17 patients. Conclusion: 18F-FDOPA PET appears to be a sensitive functional imaging tool for the detection of primary NETs occult on SRS, especially tumors with a well-differentiated pattern and serotonin secretion.
Neuroendocrine tumors (NETs) are epithelial neoplasms derived from cells of the diffuse neuroendocrine system. Their incidence is usually reported as 40–50 cases per million individuals, accounting for about 0.5% of all cancers in the adult population (1). NETs can be classified as functioning or nonfunctioning according to the presence or absence of tumoral secretion of peptides or hormones. In about 20%–50%, the primary tumor is of unknown origin, accounting for 2%–4% of all carcinomas of unknown primary origin (2–6). The identification of the primary tumor is crucial in treatment planning since resection of the primary tumor is associated with improvement of symptom-free survival, overall survival, and quality of life even at later stages of the disease with presence of distant metastases (7–10). Furthermore, the detection of a primary tumor of pancreatic origin enables the use of new, highly efficient molecular targeted therapies such as everolimus (an inhibitor of mammalian target of rapamycin) and sunitinib (an antiangiogenic agent) (11,12).
A multimodality imaging approach is usually needed to fully evaluate the extent of disease and to localize the primary tumor. Nevertheless, the primary tumor frequently remains occult on the recommended morphologic and functional imaging studies based on the use of multiphasic CT, MR imaging, endoscopic sonography, and somatostatin receptor scintigraphy (SRS) (2,13,14).
In recent years, dihydroxyphenylalanine radiolabeled with 18F (18F-FDOPA) has been developed to image NETs originating in different areas (15,16). The uptake and retention of 18F-FDOPA is dependent on the expression of the large neutral amino acid transporter system and the activity of amino acid decarboxylase (17). It is widely recognized that the sensitivity of 18F-FDOPA is influenced by the embryologic origin of the NETs, with a higher sensitivity for midgut NETs than for others (18,19).
Analysis of the relevant literature is hampered by the frequent mixing of different clinical situations. Moreover, patients with NETs of unknown origin are rarely investigated in a specific manner. Reported sensitivities for 18F-FDOPA PET and PET/CT in the detection of primary NETs have ranged from 29%–100% (19–23), and sensitivity for SRS-negative lesions has scarcely been investigated. It is therefore important to specifically evaluate the diagnostic performance of 18F-FDOPA PET in the detection of primary NETs.
The aim of the present retrospective study was to evaluate the performance of 18F-FDOPA PET/CT in the detection of neuroendocrine primary tumors in a cohort of patients with negative findings on conventional imaging and SRS.
MATERIALS AND METHODS
Patient Population
Among all the patients evaluated by 18F-FDOPA PET/CT between January 2009 and December 2012 in the Nuclear Medicine Department of the university hospitals of Strasbourg and Marseille, only patients with histologically proved metastatic disease of neuroendocrine origin were evaluated. Tumors were classified for differentiation and grade according to the criteria of the World Health Organization and the European Neuroendocrine Tumour Society (24,25). Imaging work-up included at least liver sonography, triphasic thoracoabdominal CT, abdominal MR imaging, and SRS performed less than 3 mo before the 18F-FDOPA PET/CT. Follow-up data were obtained for at least 12 mo after 18F-FDOPA PET/CT in surviving patients.
All selected subjects underwent a standard physical examination investigating the presence of symptoms related to tumoral secretion, particularly flushing and diarrhea. Serum chromogranin A, serum serotonin, and urinary 5-hydroxyindolacetic acid were measured in all patients. Serum gastrin, insulin, glucagon, and ACTH were measured only in selected patients. In addition to the conventional imaging work-up, endoscopic sonography combined with fine-needle aspiration cytology or large-bowel colonoscopy, video capsule endoscopy, or 18F-FDG PET/CT were available in a limited number of patients. 18F-FDG PET/CT was added to the work-up for selected patients with occult primary NETs on 18F-FDOPA PET/CT, poorly differentiated NETs, or a Ki-67 of at least 15%.
18F-FDOPA was used in the setting of marketing authorization. The Institutional Review Board approved this retrospective study, and the requirement to obtain written informed consent was waived.
Technical Features and Interpretation Criteria for SRS and PET/CT
SRS included anterior and posterior whole-body planar images (matrix, 256 × 1,024; speed, 8–10 cm/min), and abdominopelvic SPECT/CT (21 patients) or abdominopelvic SPECT (6 patients) was performed 4 and 24 h after intravenous injection of 148–259 MBq (4–7 mCi) of 111In-pentetreotide using a 2-head γ camera (ECAM or Symbia T6; Siemens) equipped with medium-energy parallel-hole collimators. Twenty percent energy windows were centered at 172 and 245 keV. Using a 360° arch and step-and-shoot acquisition, 64 projections lasting 45 s each were acquired with a 64 × 64 matrix. Images were reconstructed from projection data using a common iterative algorithm. For SPECT/CT, a CT scan (110 kV, 80 mAs, 2.5-mm slice thickness) was obtained for attenuation correction and localization of scintigraphic abnormalities.
A combined PET/CT scanner was used for all patients (Discovery ST; GE Healthcare). Patients fasted 4 h before tracer injection. They were administered a 4 MBq/kg dose of 18F-FDOPA without carbidopa premedication. 18F-FDOPA PET/CT images were acquired in the early phase (centered over the abdomen) and the delayed phase (whole-body acquisition) at 10 and 30–45 min after injection, respectively. PET/CT images were acquired from head to mid thigh. Unenhanced CT was performed using 140 kV, 80 mAs, and 0.8 s/rotation. Three-dimensional PET was performed using 7 fields of view, 15 cm/field, 3–4 min/field, and a 3.27-mm slice thickness. PET data were reconstructed with and without CT-based attenuation correction using ordered subsets expectation maximization (2 iterations, 21 subsets, 128 × 128 matrix). CT data were reconstructed using an approximately 1-mm section thickness, a 15-cm field of view, and a high-resolution kernel. The same PET/CT scanner was used for 18F-FDG imaging, with CT at the same setting being acquired first, followed by PET (4 min per bed position) 45–60 min after 18F-FDG injection. For 18F-FDG PET/CT, the patients fasted 6 h before the intravenous injection of a 4.5 MBq/kg dose of 18F-FDG. CT, PET (after attenuation correction), and PET/CT fusion images were displayed on a Xeleris workstation (GE Healthcare) for analysis.
Two experienced nuclear medicine physicians who were aware of the clinical and pathologic background of each patient interpreted the SRS and 18F-FDOPA PET/CT images as positive or negative for primary NET localization. A focal extraphysiologic increase of tracer uptake was considered to be tumoral. In cases of conflicting results between the 2 reviewers, a third physician was required for reaching a consensus. Pathologic analysis was used as the gold standard for the diagnosis of primary NETs.
For comparison with SRS, all affected regions were detailed as follows: liver, bone, lung, lymph nodes, brain, and other. Multiple foci of pathologic tracer uptake in the same region were considered to be a single localization. 18F-DOPA PET/CT and SRS results were considered concordant when both tracers detected the same involved organ and discordant when pathologic uptake was present in a single functional imaging modality. In this situation, the final diagnosis was based on the conventional imaging, histology, or follow-up data.
Statistical Analysis
Results are expressed as mean, range, and percentage. 18F-FDOPA PET/CT sensitivity for the localization of the primary tumor was calculated. Between-group comparisons were performed using the χ2 test for qualitative variables. P values of less than 0.05 were considered statistically significant. All statistical analyses were performed using SPSS software, version 17.0 (IBM).
RESULTS
Patients and Tumors
Twenty-seven patients were eligible for final analysis. There were 16 men (59%) and 11 women, with a mean age of 60 y (range, 25–76 y). Twenty-three patients underwent 18F-FDOPA PET/CT for initial staging and the remaining 4 patients for follow-up during therapy, which consisted of chemotherapy in 3 patients and peptide-receptor radiotherapy in 1 patient. NET was diagnosed from pathologic analysis of liver metastases in 19 patients (70%), retroperitoneal or mesenteric lymph node metastases in 6 patients (22%), upper-clavicular lymph node metastases in 2 patients (7%), peritoneal carcinomatosis in 2 patients (7%), adrenal metastasis in 1 patient (4%), and lung metastasis in 1 patient (4%). NETs were classified as well differentiated and poorly differentiated in, respectively, 23 patients (85%) and 4 patients (15%), and tumor stages were G1, G2, and G3 in 5 patients (18%), 18 patients (67%), and 4 patients (15%), respectively (24,25). Most patients (20/27 [74%]) had clinical symptoms consisting of a variable association of diarrhea (55%), flushing (40%), abdominal pain (15%), anorexia (15%), and weight loss (40%). Serum chromogranin A was elevated in 17 patients (63%). Moreover, both serum serotonin and urinary 5-hydroxyindolacetic acid values were elevated in 13 patients (48%).
18F-FDOPA PET/CT Findings for Localization of Primary Tumor
Among the 27 selected patients with negative SRS results, 18F-FDOPA PET/CT successfully detected the primary tumor with subsequent histologic confirmation in 12 patients (overall sensitivity, 44%; 52% in patients evaluated at initial diagnosis). According to tumor differentiation, the sensitivity of 18F-FDOPA PET/CT for detection of the primary tumor was 48% (11/23 patients) and 25% (1/4 patients) in patients with well differentiated and poorly differentiated NET metastases, respectively.
More patients with positive 18F-FDOPA PET/CT results than patients with negative results were symptomatic (100% vs. 53%, P = 0.01) and had higher values of serum chromogranin A (100% vs. 20%, P = 0.0003), serotonin, or urinary 5-hydroxyindolacetic acid (83% vs. 20%, P = 0.003).
The primary tumors detected by 18F-FDOPA PET/CT were distributed and graded as follows: 1 duodenum G2 lesion, 7 ileum G2 lesions, 2 terminal ileum G1 lesions, 1 pancreas G2 lesion, and 1 gallbladder G3 lesion. The Ki-67 index ranged from 1% to 60% and was always equal to or higher than its metastatic counterpart.
All primary tumors were detected on whole-body images (Fig. 1). The single primary pancreatic NET (patient 6) was visible despite a faint and homogeneous 18F-FDOPA uptake in the whole pancreas. In 2 patients, 18F-FDOPA PET/CT showed prostatic uptake, which was considered unrelated to the NET disease. Histologic analysis was available for 1 patient and showed nonspecific inflammation. Two false-negative results were related to duodenal and prostatic poorly differentiated NETs (G3) (patients 8 and 3). In 13 patients, the primary tumor was not detected within a mean follow-up of 21 mo (range, 12–32 mo) after PET imaging. In the latter case, the patient died 2 mo after PET imaging from his poorly differentiated NET without identification of the primary NET.

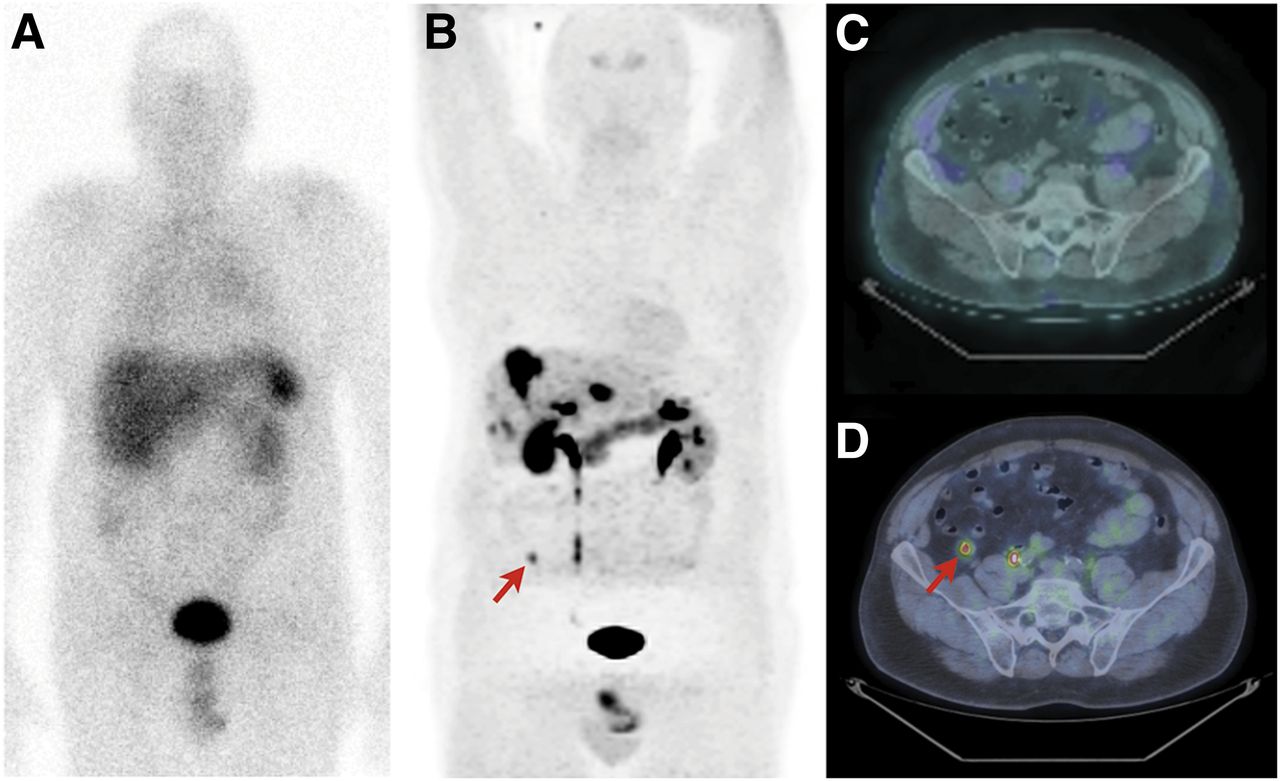
SRS anterior whole-body planar imaging (A), 18F-FDOPA PET/CT (anterior maximum-intensity projection) (B), axial SRS SPECT/CT (C), and axial 18F-FDOPA PET/CT (D) performed on a 56-y-old patient (patient 17) with metastatic NET of unknown origin. 18F-FDOPA PET/CT confirmed presence of liver metastases and identified primary tumor in ileum (arrow), occult on both conventional imaging and SRS.
18F-FDG PET/CT was performed on 10 patients and was positive in only 1 patient with a poorly differentiated biliary NET (patient 12).
Patient and tumor characteristics and PET/CT findings are detailed in Table 1
Patient and Tumor Characteristics and PET/CT Findings
18F-FDOPA PET/CT Metastatic Disease Assessment and Clinical Impact
The comparison between 18F-FDOPA PET/CT and SRS showed a concordant pattern in 8 patients (30%) and discordant results in the remaining 19 (70%). 18F-FDOPA PET/CT showed more localizations than did SRS in 17 patients. Additional lesions were localized as follows: upper diaphragmatic lymph nodes in 12 patients (71%), lower diaphragmatic lymph nodes in 12 patients (71%), liver in 5 patients (29%), bone in 3 patients (18%), and peritoneal carcinomatosis in 1 patient (6%). In the additional discordant situations, SRS showed liver metastases that were occult on 18F-FDOPA PET/CT in 2 patients. Serotonin immunoexpression analysis performed on liver tissue samples was negative in these 2 patients. The primary NET remained occult on both functional imaging modalities in the subsequent follow-up.
If resection of the primary tumor based on 18F-FDOPA PET/CT findings is considered to be a major clinical impact, 18F-FDOPA PET/CT induced a major modification in the therapeutic strategy in 12 (44%) of the 27 patients included. None of the patients who underwent surgery for their primary NET had a false-positive lesion.
DISCUSSION
The present study determined the sensitivity of 18F-FDOPA PET/CT in the detection of primary NETs in a large cohort of patients with negative morphologic and functional imaging results. In our series, the sensitivity of 18F-FDOPA PET/CT was 44% overall and increased to 52% in patients evaluated at initial diagnosis. Furthermore, 18F-FDOPA PET/CT detected more of the involved anatomic regions than did SRS in 17 patients.
Localization of the primary NET remains a diagnostic challenge in different clinical situations such as gastroenteropancreatic tumors, hyperinsulinism, and paraneoplastic Cushing syndrome (2,13,14). To date, only a few studies have evaluated the clinical value of 18F-FDOPA PET/CT in NETs (20–23), probably because 18F-FDOPA is not routinely available at most imaging centers worldwide. The overall reported sensitivity of 18F-FDOPA PET/CT ranged from 29% to 100% (19–23), but results on the detection of the primary tumor have only rarely been specifically addressed (26,27). Hoegerle et al. (20) were the first to uniquely demonstrate the utility of 18F-FDOPA PET to localize gastroenteropancreatic tumors. They found 88% sensitivity for 18F-FDOPA PET in a series of 8 patients with NETs of unknown origin, with a higher detection rate than SRS (50%) and 18F-FDG (25%). In 2006, Montravers et al. compared SRS and 18F-FDOPA PET/CT in 30 patients with metastatic NETs (21). 18F-FDOPA PET/CT detected the unknown primary lesion in only 2 of 7 patients (29%). In another study by the same group, the primary NET was detected by 18F-FDOPA PET/CT in 6 of 16 patients (22). In these 2 studies, 18F-FDOPA PET/CT was more sensitive than SRS in patients with secreting carcinoid tumors. In contrast, SRS was superior to 18F-FDOPA PET/CT in noncarcinoid tumors. In our series, as in others, the sensitivity of 18F-FDOPA was clearly influenced by the embryologic origin of the NETs and their tumor differentiation. The detection rate of the primary tumor by 18F-FDOPA PET/CT was higher in well-differentiated NETs of the mid gut. This higher value of 18F-FDOPA PET/CT over SRS is probably related to an increased sensitivity of PET/CT cameras over SPECT/CT cameras and to specific features such as overexpression or increased activity of the amino acid decarboxylase involved in the biosynthesis of serotonin. Fiebrich et al. showed that the whole-body metabolic tumor burden correlates with the amount of serotonin secretion (28).
Accurately localizing NETs plays a critical role in the management of patients with these tumors, especially in determining surgery of the primary tumors (20–23). In our series, 12 patients underwent surgery based on 18F-FDOPA PET/CT findings.
Several hypotheses may explain the decrease of 18F-FDOPA PET/CT in noncarcinoid tumors. One hypothesis is that there is a specific imaging phenotype related to the absence of activation of the large neutral amino acid transporter and CD98 transporter systems. It is well established that these tumors exhibit specific responses to targeted therapies, and this molecular singularity may also extend to functional imaging. However, this possibility remains speculative and requires evaluation in further basic science research.
Another explanation may be related to the imaging protocol itself, which may be inappropriate for optimal detection of these tumors. It has been reported that the high physiologic 18F-FDOPA uptake by the whole pancreas potentially reduces the detection rate of pancreatic tumors (29). The use of carbidopa before 18F-FDOPA injection for inhibiting amino acid decarboxylase increases the signal-to-background ratio (30,31), but negativization of 18F-FDOPA focal pancreatic hot spots has been reported after carbidopa in patients with hyperinsulinemic hypoglycemia.
At present, no recommendation exists concerning the use of carbidopa premedication, but this approach should be further evaluated in this clinical setting as well as the optimal timing for image acquisition.
We acknowledge several limitations to our study: its retrospective design, the limited number of patients, and the short duration of follow-up. However, to our knowledge it is the largest study showing extensive data related to primary tumors.
On the basis of the currently available imaging techniques for diagnosis and staging of NETs, we propose that 18F-FDOPA PET/CT be performed as the first-line functional imaging technique for NETs of unknown origin, especially those with a well-differentiated tumor and serotonin secretion. SRS should be reserved for other situations or when 18F-FDOPA PET/CT findings are negative for a primary tumor or targeted radiotherapy is planned.
The current leading role of 18F-FDOPA PET/CT in the evaluation of NETs will need to be further compared with newly introduced and promising agents for PET imaging such as somatostatin analogs labeled with 68Ga (32). High sensitivity has been reported for PET/CT with 68Ga-labeled peptides in patients with clinically, biochemically, or radiologically suspected NET (33–35). Recently, some authors prospectively compared 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT in the same patients with gastroenteropancreatic tumor NETs and highlighted the high diagnostic sensitivity of 68Ga-DOTANOC to assess the extent of metastatic disease (36). Moreover, 68Ga-DOTANOC PET/CT seems to be a promising diagnostic modality for detecting primary tumor in patients with neuroendocrine carcinoma of unknown origin (37). At present, only few clinical investigations involving a limited number of patients with NET have compared the diagnostic role of PET/CT with 18F-FDOPA or 68Ga-labeled somatostatin analogs (38,39). 68Ga-DOTANOC PET/CT was found to be more accurate than 18F-FDOPA PET/CT in the detection of primary tumor and metastatic disease. Unfortunately, the heterogeneity of the studied population still represents a major bias for a reliable head-to head comparison of the imaging approaches.
CONCLUSION
18F-FDOPA PET appears to be a sensitive functional imaging tool for the detection of primary NETs occult on SRS. Some unanswered questions arise from lesions missed by 18F-FDOPA PET, including specific genetic or molecular features and the possibility of inappropriate acquisition protocols.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 16, 2013.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 29, 2013.
- Accepted for publication September 24, 2013.





{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-DOPA PET/CT at the Forefront of Initial or Presurgical Evaluation of Small-Intestine Neuroendocrine Tumors
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- Use of Video Goggles to Distract Patients During PET/CT Studies of School-Aged Children
- 18F-DOPA and Other Radiopharmaceuticals for Imaging Unknown Primary Neuroendocrine Tumors