


Abstract
The purpose of this study was to assess the safety of repeated 90Y radioembolization with resin microspheres in patients with extensive primary and secondary liver tumors after failure of first radioembolization. Methods: Between 2007 and 2011, 21 patients (12 women, 9 men; mean age, 61.0 y) with nonresectable advanced liver tumors (breast cancer liver metastases, n = 7; colorectal liver metastases, n = 5; hepatocellular carcinoma, n = 8; cholangiocellular carcinoma, n = 1) were repeatedly treated by radioembolization. Safety was the primary endpoint. Whole-liver treatment was achieved with sequential treatment sessions in most patients, with selective embolization of the left and right liver lobes within 6 wk. Toxicity was documented prospectively and according to Common Terminology Criteria for Adverse Events 4.0 criteria based on laboratory parameters; magnetic-resonance tomography; and clinical examinations 3 d, 6 wk, and every 3 mo after selective internal radiotherapy (SIRT). Metric variables were evaluated using the Student t test. Overall survival was assessed by Kaplan–Meier statistics. Results: Patients received an average of 1.6 whole-liver treatments performed in 3.0 unilobar radioembolizations (liver lobes sequentially). The mean total activity administered was 2.57 GBq. No radioembolization-induced liver disease was observed in any of the patients. Three patients showed reversible grade III to IV toxicities according to laboratory values, which returned to pretreatment levels after 6 wk. In 1 patient, a treatment-related duodenal ulcer occurred. Median overall survival was 18 mo after first radioembolization. Conclusion: In advanced liver tumors, repeated whole-liver treatments with 90Y radioembolization can be performed with an acceptable toxicity profile.
The liver is a common site of metastasis in various tumors, for example, colorectal cancer or breast cancer (1,2). Unfortunately, most patients with liver metastasis will face advanced-stage disease, lacking curative options. Furthermore, malignancies with the liver as the primary site, such as hepatocellular carcinoma (HCC) or cholangiocellular carcinomas, are—despite advances throughout surveillance programs in risk groups—not likely to be diagnosed until there is extended disease (3,4). In this palliative situation, and given the incidence of extrahepatic tumor spread, effective treatment and control of the hepatic tumor load may be, especially in colorectal liver metastases, of the utmost importance for survival (5). Radioembolization using 90Y microspheres is a relatively new modality applicable even in patients with extensive primary and secondary liver neoplasms. Recent experience indicates the efficacy of radioembolizations in these patients (6–11), but there is still a lack of evidence from randomized controlled trials such as have been published on systemic chemotherapies (especially colorectal liver metastases) or transarterial chemoembolization (HCC) (12,13).
Radioembolization is, therefore, frequently placed at the end of therapeutic management, and as of today radioembolization is conducted predominantly after failure of conventional therapies. In that regard, radioembolization is seen as an exceptional salvage treatment usually conducted at just 1 time point per patient. The absence of alternative treatment options after an initial radioembolization raises the question of whether repeated radioembolization would be safe and effective. In individual patients, the indication for repeated radioembolizations may vary, with indication for repeated whole-liver or lobar radioembolization. Safety is of considerable interest in patients with restricted liver function after previous radioembolization, possibly in combination with hepatotoxic chemotherapies or liver cirrhosis.
In this study, we retrospectively reviewed 21 patients who had undergone repeated radioembolizations of one or both liver lobes. The primary endpoint was safety of the repeated radioembolization, with specific emphasis on liver function during follow-up. Survival analysis was also performed.
MATERIALS AND METHODS
Patients
Between 2007 and 2011, 21 patients (12 women, 9 men; mean age, 61.0 y [range, 34–75 y]) with nonresectable advanced liver tumors (breast cancer, n = 7; colorectal cancer, n = 5; HCC, n = 8; cholangiocellular carcinoma, n = 1) were repeatedly treated by radioembolization (at least 3 lobar procedures).
The indications for the initial radioembolization were disease relapse after various pretreatments, including liver resection in most patients. Prior treatments included surgical procedures in 6 patients and local ablations in 4 patients. Fifteen patients had previously been treated systemically with an average of 2 lines of chemotherapy. Furthermore, we recorded all concomitant treatments for method (e.g., radiofrequency ablation) and location. Details of patient characteristics are shown in Table 1.
Patient Characteristics
Patients presenting with liver cirrhosis and Child–Pugh category C were not offered radioembolization. Among the patients with HCC, 6 presented with Child–Pugh stage A (5–6 points) and 2 with stage B (7 points). Inclusion criteria for all patients at initial or repeated radioembolizations comprised an East Coast Oncology Group (ECOG) performance status of 0–2, a Karnofsky index above 70%, a platelet count above 50,000, a prothrombin time of at least 50%, and bilirubin below 30 μmol/L. Controlled ascites and partial portal-vein occlusion were not exclusion criteria.
Extrahepatic metastases were found in 9 of 18 patients at the time of intervention. In these patients, a dominant hepatic tumor load to the liver was considered the most relevant prognostic factor for survival and therefore patients were offered radioembolizations if systemic options were not available or were refused by the patient. The decision for a repetitive radioembolization cycle was based on the response after the initial radioembolization. As a consequence, patients with early progression, observed 6 wk after the first radioembolization, were excluded from repeated treatment. Sixteen patients received 3 lobar radioembolizations, 4 patients were treated with 4, and 1 patient was treated with 5. Patients were exclusively treated 1 lobe at a time. If for a single radioembolization cycle both liver lobes were scheduled for radioembolization, the interval between radioembolizations of both lobes was 4–6 wk.
Expressed as a cumulative exposure, patients received 1.6 whole-liver treatments applied on average in 3 unilobar sessions.
Measurements of tumor and uninvolved liver parenchyma were performed on the basis of pretherapeutic MR imaging scans with a hepatocyte-specific contrast agent. The median pretherapeutic volume of uninvolved liver parenchyma was 1,580 mL (range, 1,032–2,410 mL), and the median tumor volume was 201 mL (100–695 mL). The tumor volume as a fraction of the total liver volume (median, 1,755 mL [1,287–2,972 mL]) ranged between 4% and 29% (median, 12%).
All patients underwent the standard evaluation procedure at our institution including a physical examination, liver function tests, and extensive tumor staging.
The local ethics committee approved this retrospective study, and the requirement to obtain an informed consent was waived.
Radioembolization Technique
Radioembolization comprises the injection of radioactive 90Y-labeled resin microspheres (SIR-Spheres; Sirtex Medical) into the arterial hepatic circulation. Resin microspheres accumulate specifically in tumor tissue because tumors almost exclusively receive their blood supply from the hepatic artery. Antitumor efficacy is linked to the β radiation from 90Y, which decays with a physical half-life of 64 h (∼2.7 d).
Before radioembolization, angiography of the celiac trunk was performed; this usually included coil embolization of the gastroduodenal artery, right gastric artery, and cystic artery to avoid extrahepatic accumulation of microspheres in the therapy session. After coil embolization, 99mTc-MAA (99mTc bound to macroaggregated albumin) was injected into the right and left hepatic artery to rule out a relevant shunt volume to the lung and extrahepatic accumulation (e.g., in the stomach). A shunt fraction exceeding 20% of the total was considered a contraindication for radioembolization, whereas 10%–20% resulted in a dose reduction as recommended in the specification of product characteristics for the microspheres. With a typical delay of 2–3 wk after the diagnostic scan, therapy (treatment cycle) with 90Y-labeled resin microspheres was conducted in 2 separate sessions (procedures) with selective injection of 90Y-labeled microspheres into the right and left hepatic artery and separated by an interval of 4–6 wk. The intrahepatic distribution of 90Y-labeled resin microspheres was assessed using Bremsstrahlung and SPECT imaging, and the distribution of 99mTc-MAA was assessed using SPECT imaging.
Before initiation of another therapy cycle after progression, angiography and 99mTc-MAA scintigraphy were repeated to exclude extrahepatic accumulations caused by collaterals or by shunts to the lung that have increased in the meantime.
Activity Calculation
The body surface area (BSA) method was used to calculate the required dose (14,15).
Following the recommendations of Kennedy et al., BSA was calculated as follows:
BSA (m2) = 0.20247 × height (m)0.725 × weight (kg)0.425. The activity administered was calculated as follows: activity (GBq) = (BSA – 0.2) + tumor volume/total liver volume.
The prescribed dose was not reduced because of a repeated radioembolization; it was, however, reduced in cases of an increased shunt volume. Activity calculation for the first and second radioembolizations followed the same algorithm.
As mentioned above, the dose was administered sequentially to each liver lobe separately, with an interval of 4–6 wk between the sessions.
Endpoints, Assessments, and Statistical Methods
Primary endpoints were toxicities (acute and subacute), and the secondary endpoint was overall survival (OS). Before therapy, a physical examination; MR and CT imaging; and laboratory tests including total bilirubin, alanine transaminase, aspartate transaminase, alkaline phosphatase, γ glutamyl transpeptidase, and albumin were performed. All these were repeated 6 wk and 3 mo after radioembolization and thereafter every 3 mo.
MR imaging scans were obtained in a 1.5-T system, before radioembolization and 6 wk and 3 mo after the completion of therapy and then every 3 mo thereafter to monitor tumor response and time to progression (TTP). The hepatocyte-specific contrast agent Gd-EOB-DTPA (Primovist; Bayer) was used. Common side effects of radioembolization (e.g., ascites, pleural effusion) were graded in conjunction with imaging findings. Furthermore, patients were examined for clinical signs of radioembolization-induced liver disease (REILD) according to Sangro et al. (16).
Toxicities were graded by the Common Terminology Criteria for Adverse Events (CTCAE), version 4.02, on the basis of laboratory values, MR imaging, and clinical examinations. Grading was performed 3 d and 6 wk after SIRT and then every 3 mo.
TTP was assessed according to the modified Response Evaluation Criteria In Solid Tumors (17) and defined as the time from the first procedure to the first assessment showing intrahepatic progression. OS was defined as the time from the first procedure to the patient’s death.
The program suite PASW Statistics 18.0.0 (Polar Engineering and Consulting) was used for statistical analysis. Metric variables were calculated by the Student t test and nonmetric by the Wilcoxon test. Frequencies were assessed by the Fisher exact test. Survival was estimated by the Kaplan–Meier method. P values below 0.05 were considered to be significant at the descriptive level of this study.
RESULTS
The mean total whole-liver activity administered (cumulative activity applied; the cumulative sum of the activities administered in all single sessions) was 2.57 GBq (range, 1.55–4.15 GBq; SD, 0.63 GBq).
Before the first treatment, the mean pulmonary shunt of all patients was 5.4% (2.0%–14.4%; SD, 3.0). Reevaluation before the second treatment cycle did not show a significant increase in the shunt volume. Nevertheless, the calculated dose had to be reduced in 5 patients because of the increasing shunt volume. The mean dose administered to the same lobe decreased from 0.97 GBq in the first session to 0.88 GBq in the second session (P > 0.05).
Between radioembolization cycles, 4 patients were treated with local ablation for small focal lesions. Four patients with HCC were treated with sorafenib (Nexavar; Bayer). Two patients with liver metastases received a systemic treatment during the observation period. Table 2 provides a summary of treatment characteristics.
Previous Systemic Treatments
Safety and Complications
No REILD was observed in any of the patients. In patients with liver cirrhosis (n = 8), no significant worsening of the Child–Pugh class was observed. Two patients showed an increase (5–6 points and 6–7 points, respectively) and another 2 patients a decrease in Child–Pugh score by 1 point. Between patients with and without cirrhosis, no statistically significant differences were seen with respect to liver function toxicities at any time point.
Furthermore, when bilirubin level was investigated as a surrogate of liver function, no significant correlation was found between cumulative activity and the increase of bilirubin level during the observation.
Total numbers of adverse events in treatment cycle 1 were 22 events for patients with HCC (n = 8) and 35 for all other patients (n = 13). Total numbers of adverse events in treatment cycle 2 were 27 events for patients with HCC (n = 8) and 44 for all other patients (n = 13). No grade IV or grade V events were recorded after initial or repeated radioembolization procedures. In treatment cycle 1, adverse events of CTCAE grade I, II, and III were reported for 75%, 50%, and 13% (respectively) of the patients with HCC and for 92%, 38%, and 8% of all other patients. In treatment cycle 2, the respective numbers of patients were 100%, 25%, and 0% for the patients with HCC and 92%, 54%, and 8% of all other patients (Table 3).
Most frequent adverse events were ascites, elevation of bilirubin or liver enzymes, and decrease of serum albumin levels (Table 4). Grade II laboratory events were seen in 8 cases, of which 4 had resolved by the time of the next radioembolization procedure. Three patients showed reversible grade III toxicities in laboratory values that returned to pretreatment levels after 6 wk (Tables 4 and 5). In 1 patient, a treatment-related duodenal ulcer (grade II) occurred after 3 mo.
Frequency of Adverse Events
Treatment Characteristics
Severity and Type of Adverse Events
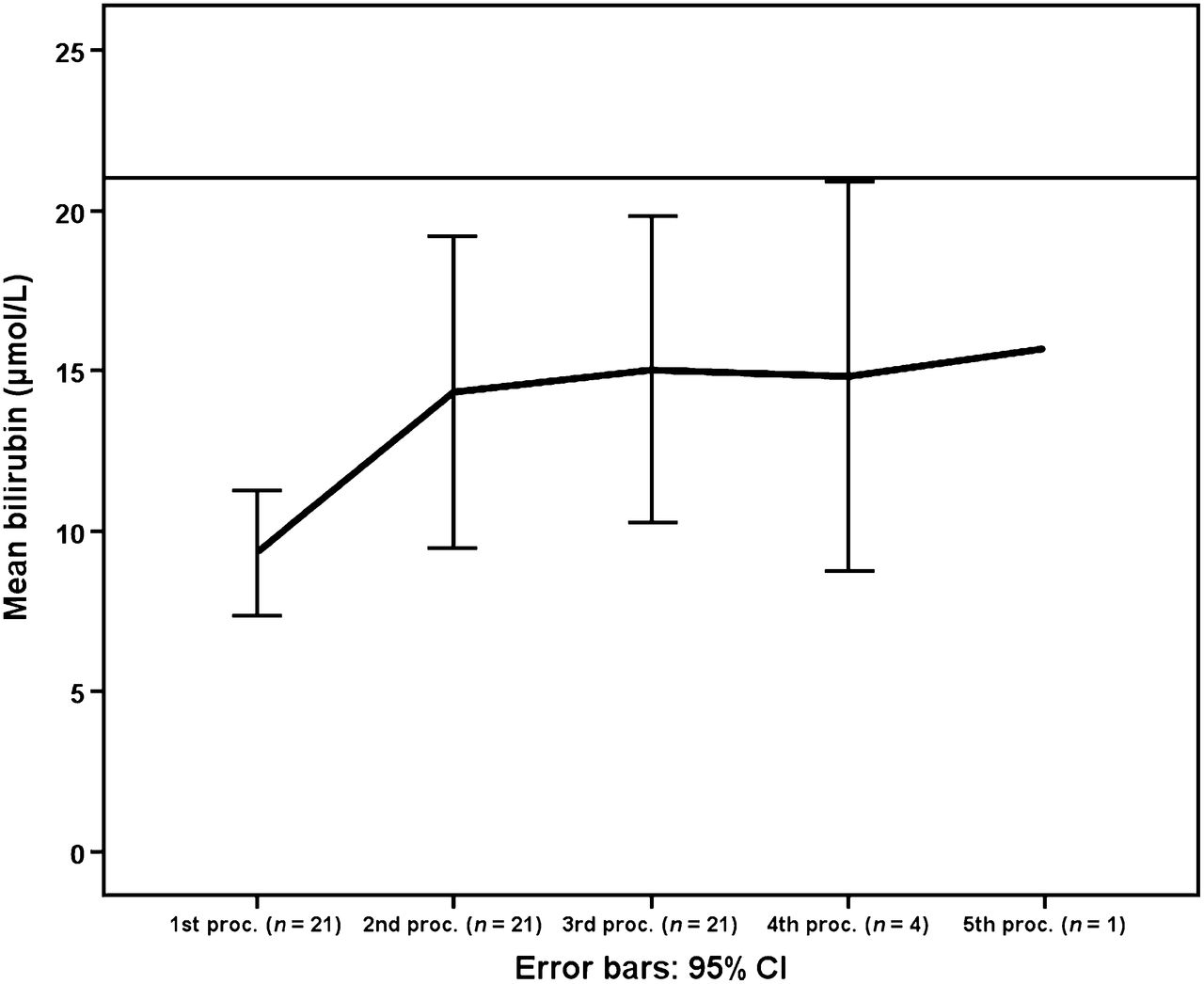
A significant increase in mean total bilirubin level (up to 1.6 times the pretreatment level) was seen during the observation period. However, despite that increase, all bilirubin values remained within normal limits (Fig. 1).
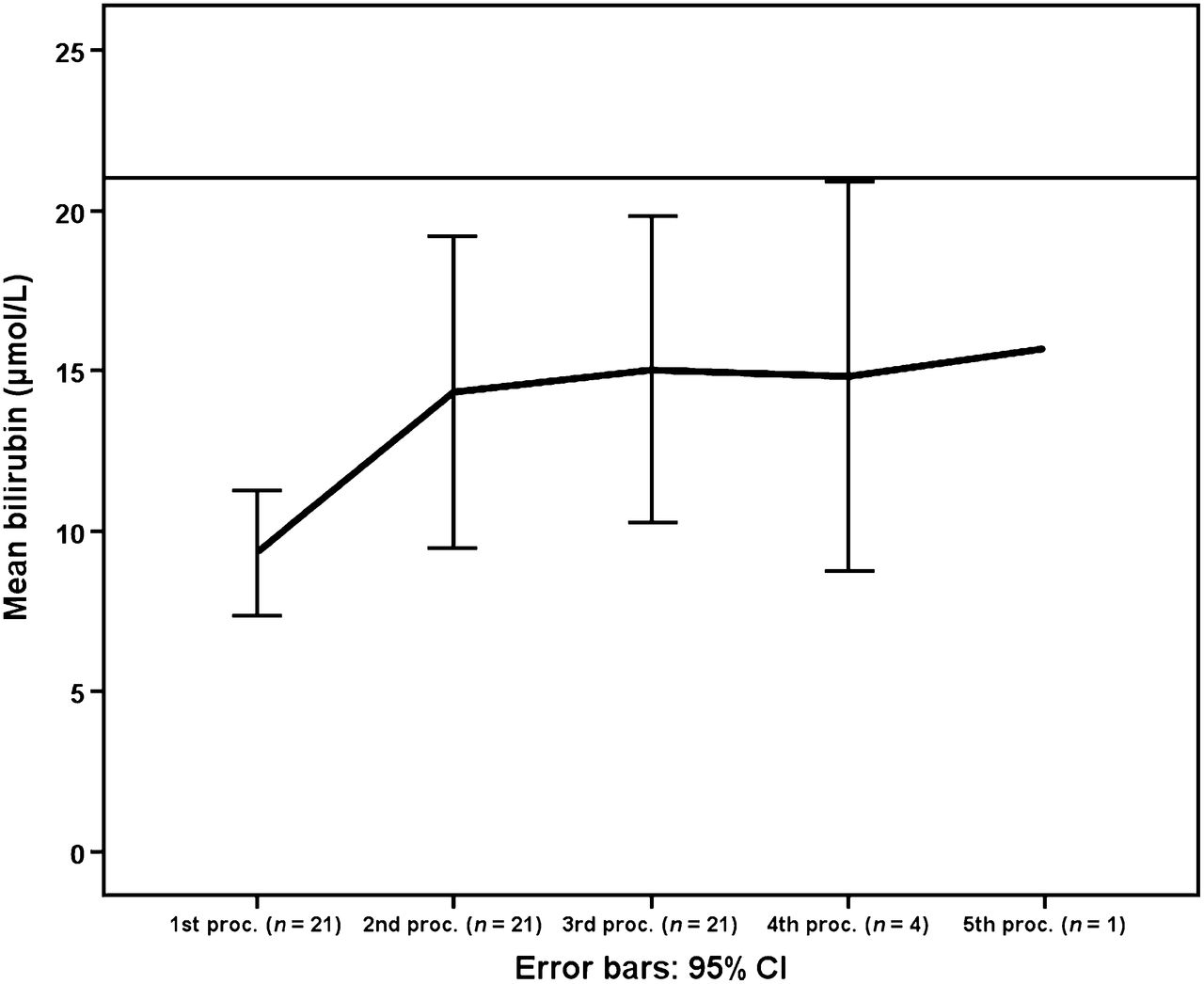
Bilirubin trend during observation period. CI = confidence interval; proc. = procedure.
Four patients developed ascites or increase of bilirubin that was due to intrahepatic tumor progression within the 3 mo after the last radioembolization. No radiation-induced pneumonitis was observed.
TTP and OS
The median duration of follow-up (including MR imaging to assess TTP) was 10 mo (range, 5–38 mo). The median TTP after the first radioembolization was 3.0 mo after the start of the first treatment session. At the time of this analysis, 13 patients had died; the median OS was 18 mo (Fig. 2).
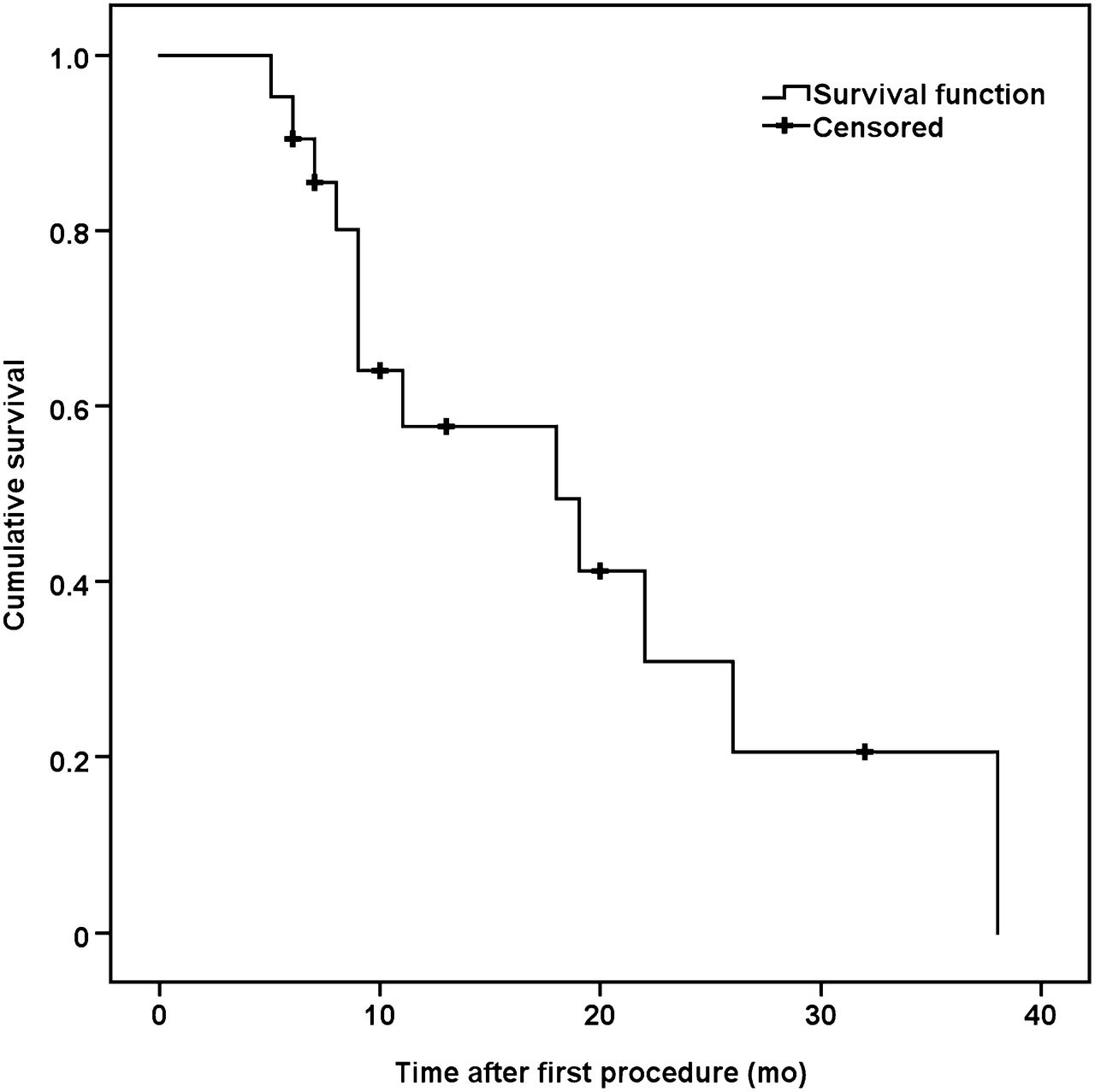
OS (mo).
DISCUSSION
In patients with advanced primary or secondary liver neoplasms confined to the liver with or without minor extrahepatic spread of the disease, there is debate as to what constitutes optimum therapeutic management. Whereas a lack of alternatives after failure of an established chemotherapy regimen eases the decision for radioembolization of the liver, the question of to where radioembolization needs to be placed in the therapeutic algorithm is still open and simple answers are unlikely to be forthcoming in the near future because of the lack of randomized controlled trials. In HCC, results from recent single-arm phase II trials have led the debate in the direction of the competition with transarterial chemoembolization (TACE). However, currently available data suggest that radioembolization is best placed after the failure of TACE in early intermediate-stage HCC (European Association for the Study of the Liver/European Organisation for Research and Treatment of Cancer guidelines) or in patients with diffuse disease (>4 tumors) or large tumors (>5 cm) (18). The clearest difference between radioembolization and TACE is, however, the fact that TACE has evolved as a repetitive procedure, which is not the case for radioembolization (13). Despite the fact that its effect vanishes over time, radioembolization has been adopted as a single-application therapeutic approach. In HCC, the only current prospective randomized study considering repetitive treatments in intermediate- and advanced-stage HCC is SORAMIC (19), which is expected to continue recruitment until 2014.
Besides HCC, the next most common indications for radioembolization are colorectal cancer, breast cancer, and others including neuroendocrine liver metastases. In all these tumors, radioembolization has demonstrated high tumor response rates in phase II studies, but despite the fact that a reasonable response rate could probably be expected by second or third radioembolization procedures, data on such an approach are scarce.
The reason for the lack of data on repetitive radioembolization is probably that the risk of toxic liver function deterioration—such as through REILD—is significant, specifically in salvage patients. In a study by Sangro et al., 30% of patients with liver metastases developed clinical symptoms of REILD after total liver irradiation (16). Risk factors were young age, previous chemotherapies containing 5-fluorouracil, and low tumor volume in small livers. A recent publication by the group of Seidensticker et al. (20) describes a significant risk reduction for liver function deterioration or REILD. In that study, patients received either total liver radioembolization in a single treatment or sequential lobar treatments at intervals of 4–6 wk. In the latter group, bilirubin increase and portal hypertension including ascites were displayed significantly less frequently.
The present study is the first report, to our knowledge, on repetitive liver treatment by radioembolization in cases with disease progression after the first intervention in a larger patient cohort. In our patient group, treated exclusively with a sequential lobar approach, repeated radioembolization had a high safety profile. No REILD was observed. No significant differences in toxicity profile between patients with and without cirrhosis were evident. In no patient was a significant worsening of liver function noted.
Radioembolization was performed repeatedly in one or both liver lobes with predominantly minor toxicities, maintaining the ECOG performance stage and the liver function with respect to the Child–Pugh score. Overall, up to 5 procedures could safely be performed in individual patients. The frequency and severity of toxicity were not different from, or even lower than, those reported in other radioembolization trials (21–24). The reason for that is indubitably a strong patient selection in terms of liver function, especially bilirubin level, and the sequential approach chosen (20). At our institution, a bilirubin level exceeding 30 μmol/L disqualifies a patient for radioembolization.
Despite a significant increase in the mean total bilirubin level during follow-up, bilirubin values always remained within reference ranges during the observation period.
Recently, Lam et al. (25) reported an interesting case series of 8 patients undergoing repeated radioembolization out of 247 patients treated with radioembolization. The cumulative dose of these 8 patients ranged between 2.41 and 3.88 GBq. Two patients developed symptoms of REILD. Both had received whole-liver treatments with a cumulative dose of 3.08 and 2.66 GBq, and at least one radioembolization was performed in a single-session whole-liver treatment approach, with the resin microspheres administered into the proper or common hepatic artery. This was not the case in our patient cohort, in which a strictly sequential approach in a lobar manner with an interval of 4–6 wk between the sessions was performed.
Both our study and that of Lem et al. failed to detect a significant correlation between activity administered and development of REILD.
Despite the fact that Lem et al. did not find the treatment approach to be a statistically significant factor for REILD, nevertheless 9 of 10 patients in their trial developed REILD after a whole-liver treatment (162 patients, 5.5% REILD), compared with 1 after lobar–segmental radioembolization (75 patients, 1.3% REILD). Therefore, the risk of developing REILD was more than 4 times greater in patients receiving single-session whole-liver treatments.
In addition, and as mentioned earlier in this section, the work of Seidensticker et al. revealed a significant difference in terms of toxicities, with significantly better tolerance to radioembolization in the patient group with sequential lobar treatments than in patients receiving single-session whole-liver treatments (20). These results are supported by the data of Ricke, Ruehl, and Seidensticker (26–28), whose research findings in MR imaging examinations with a hepatocyte-specific contrast agent (Primovist; Bayer) documented repair mechanisms over time after high-dose-rate brachytherapy of liver metastases after a transient hepatocyte function loss following exposure to a specific radiation dose.
All of our patients received the sequential approach. Therefore, and besides other safety constraints (see above), the probability of the development of REILD induction was lower in our patient cohort.
OS was promising, with a median of 18 mo, when compared with published outcomes after radioembolization or second- to third-line chemotherapy.
For colorectal liver metastases, an OS of 14.5 mo (29), 10.5 mo (30), and 10 mo (31) have been reported. Seidensticker et al. showed the superiority of radioembolization over best supportive care for colorectal liver metastases (32).
Salem et al. reported an OS of 17.2 and 7.7 mo for 291 patients with HCC, depending on the Child–Pugh stage (A or B) (33).
There is broad evidence for the efficacy of second- to third-line chemotherapy. In a second-line situation, a FOLFIRI regimen in 213 patients resulted in a progression-free survival of 5.1 mo (34). In a third-line situation, bevacizumab plus FOLFIRI (folinic acid, fluorouracil, irinotecan) or FOLFOX (folinic acid, fluorouracil, oxaliplatin) resulted in a progression-free survival and OS of 5.3 and 9.5 mo, respectively (35). Adverse events in the aforementioned trial included grade III to IV neutropenia in approximately 43%, fatigue in 22%, neuropathy in 22%, and mucositis in 22% of all patients.
Taking into account the heterogeneity with 12 secondary liver neoplasms and 9 primary liver tumors in our study, the OS of 18 mo in our patient cohort indicates a possible benefit also in terms of effectiveness. Nevertheless, this is a safety study, and prospective trials with a larger cohort are needed to prove a benefit with respect to OS after repeated radioembolizations.
CONCLUSION
Repetitive radioembolization was demonstrated to be safe in our patients with preserved liver function. Our results encourage one to consider radioembolization in patients with tumor recurrences after failed initial radioembolization and without alternative treatment options. Future studies should evaluate the effectiveness of repeated radioembolizations, specifically with regard to response rates as compared with the initial radioembolization.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was funded exclusively by the University of Magdeburg. Maciej Pech, Jens Ricke, and Holger Amthauer have received consultant's fees or research grants from SIRTEX Medical. The study was conducted in accordance with the protocol, the ethical principles that have their origin in the Declaration of Helsinki and ICH-GCP. The study protocol and all study-related documentation were approved by all relevant authorities. No other potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Feb. 10, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 4, 2013.
- Accepted for publication October 10, 2013.





{kind=link}
{kind=link}