


Abstract
Outcome analyses for patients with gastroenteropancreatic neuroendocrine tumors (GEP NET) after peptide receptor radionuclide therapy (PRRT) are still limited, especially with regard to the impact of the Ki-67 index. Using a single-center analysis, we aimed to establish predictors of survival. Methods: We retrospectively analyzed a consecutive cohort of 74 patients who had metastatic GEP NET and underwent PRRT with 177Lu-octreotate (mean activity of 7.9 GBq per cycle, aimed at 4 treatment cycles at standard intervals of 3 mo). Patients (33 with pancreatic NET and 41 with nonpancreatic GEP NET) had unresectable metastatic disease graded as G1 or G2 (G1/G2) and documented morphologic or clinical progression within less than 12 mo or uncontrolled disease under somatostatin analog treatment. Responses were evaluated according to modified Southwest Oncology Group criteria. Potential predictors of survival were analyzed with the Kaplan–Meier curve method (log-rank test) and multivariate analysis (P < 0.05). Results: The response rates were 36.5% partial response, 17.6% minor response, 35.1% stable disease, and 10.8% progressive disease for the entire cohort; 54.5% partial response, 18.2% minor response, 18.2% stable disease, and 9.1% progressive disease for pancreatic NET; and 22.0% partial response, 17.1% minor response, 48.8% stable disease, and 12.2% progressive disease for nonpancreatic GEP NET. The median progression-free survival and overall survival were 26 mo (95% confidence interval, 18.3–33.7) and 55 mo (95% confidence interval, 48.8–61.2), respectively. Besides the Ki-67 index, a Karnofsky performance score of less than or equal to 70%, a hepatic tumor burden of greater than or equal to 25%, and a baseline plasma level of neuron-specific enolase of greater than 15 ng/mL independently predicted shorter overall survival (hazard ratio, 2.1–3.1). Patients with a Ki-67 index of greater than 10% still had median progression-free survival and overall survival of 19 and 34 mo, respectively. Conclusion: The results of this study demonstrated the favorable response and long-term outcome of patients with G1/G2 GEP NET after PRRT. Independent predictors of survival were the Ki-67 index, the patient’s performance status (Karnofsky performance scale score), the tumor burden, and the baseline neuron-specific enolase level. Even patients with a Ki-67 index of greater than 10% seemed to benefit from PRRT, with a good response and a notable long-term outcome. We present the first evidence, to our knowledge, that even in patients with metastatic disease the distinction between G1 and G2—in particular, between G1 (Ki-67 index of 1%–2%) and low-range G2 (Ki-67 index of 3%–10%)—provides prognostic stratification.
- gastroenteropancreatic tumors
- neuroendocrine tumors
- peptide receptor radionuclide therapy
- 177Lu-octreotate
- tumor grading
Peptide receptor radionuclide therapy (PRRT) is a highly efficient modality for the systemic treatment of gastroenteropancreatic neuroendocrine tumors (GEP NET) (1–4). The compound [177Lu-DOTA0,Tyr3]octreotate (177Lu-octreotate) is frequently used for this purpose. Outstanding response and survival data are available (1), and with the growing importance of this treatment modality, the relevance of outcome predictors (2) is becoming increasingly meaningful for multidisciplinary management of tumors.
The first analysis of the impact of the Ki-67 index on the efficacy of PRRT has been reported (5). Interestingly, it was demonstrated that indices of up to 20% had no discernible influence on tumor response. However, analyses of the impact of the proliferation parameter on survival in the context of PRRT were not yet available. We aimed to assess the impacts of various baseline variables, including the Ki-67 index, on outcome in the well-characterized population of patients in whom the previously reported factor analysis was performed.
MATERIALS AND METHODS
We retrospectively analyzed a consecutive cohort of patients who had well-differentiated GEP NET and a known Ki-67 index (≤20%) and underwent PRRT at our institution. In addition to giving written informed consent for their treatment, patients also gave written informed consent for the scientific analysis of their data; the local ethics committee approved the study. All 74 patients were part of a previously published study (5), and 23 of the patients were included in a more recent analysis of bone metastatic GEP NET (4). None of the patients was included in a therapy trial.
Patients
The patient cohort consisted of 74 consecutive patients (mean age, 62.5 y; range, 34–83 y; 42 men and 32 women) who had well-differentiated GEP NET graded as G1 or G2 (G1/G2) according to the current World Health Organization classification; who were treated with PRRT at the University Hospital of Bonn; and who had complete restaging and follow-up (Table 1). Thirty-three patients had pancreatic NET, and 41 patients had nonpancreatic GEP NET; of the latter, 4 had foregut, 19 had midgut, and 2 had hindgut GEP NET, and 16 had GEP NET with an unknown primary tumor. Metastatic sites included the liver in 58 patients (78.4%), bone in 28 patients (37.8%), and other organs in 12 patients (16.2%). Previous treatments comprised surgery (n = 38; 51.4%), biotherapy (n = 28; 37.8%), chemotherapy (n = 18; 24.3%), and locoregional treatment (n = 13; 17.6%). PRRT was the first-line systemic therapy in 25 patients (33.8%). At baseline, before the initiation of PRRT, there was documented clinical progression (n = 16; 21.6%) or morphologic progression (n = 56; 75.7%) within less than 12 mo or uncontrolled disease under somatostatin analog treatment (n = 8; 10.8%). For the purpose of the present study, hepatic tumor burden at baseline was retrospectively assessed according to pretreatment CT or MR imaging, and patients were categorized into 4 groups of liver involvement: none, less than 25%, 25%–50%, and greater than 50% of the liver volume. The cutoff value of 25% was then identified as the best predictive separator and consequently used for all survival analyses. Tumor uptake was classified according to the 177Lu-octreotate therapy scan of the first PRRT cycle (grade 3, greater than that of the kidney or spleen; grade 2, greater than that of the liver; and grade 1, approximately that of the liver). This was done to standardize the uptake score for the entire cohort because some patients had scintigraphic scans (e.g., OctreoScan; Covidien) and others had PET-based pretherapeutic somatostatin receptor imaging.
Patient Characteristics and Proportions Receiving PRRT as First-Line Treatment
Histopathology
Tumors were classified according to the current TNM staging and grading system for NET (6–8). All tumors were well-differentiated endocrine tumors, according to histopathology, with the presence of distant metastases (TNM stage IV). Histologic and immunohistochemical analyses, including determination of the Ki-67 proliferation index, were performed on resection specimens (n = 35; 47.3%) or biopsy material (n = 39; 52.7%). The Ki-67 index was expressed as the percentage of MIB1 antibody–stained tumor cells in areas in which the highest level of nuclear labeling was observed (6,7). The median time interval between the Ki-67 index assessment and the initiation of PRRT (first treatment cycle) was 14.5 mo; in 38 patients (51.4%), the interval was greater than 12 mo. The time interval was insignificantly shorter for pancreatic tumors (median, 9 mo) than for nonpancreatic tumors (median, 16 mo) (P = 0.313). Categorization of the proliferation of tumors as G1 (Ki-67 index of <3%), low-range G2 (Ki-67 index of 3%–10%), and high-range G2 (Ki-67 index of 15%–20%) was done retrospectively to analyze the potential impact on survival. There were no Ki-67 indices between 10% and 15%, in accordance with current standard practice for reporting the immunostaining of NET.
PRRT
The inclusion criteria for treatment with PRRT were histologically confirmed, unresectable, metastatic GEP NET; sufficient tracer uptake (greater than or equal to that of normal liver) on baseline somatostatin receptor imaging; a glomerular filtration rate of greater than 30 mL/min/1.73 m2; a white blood cell count of greater than or equal to 2 × 109/L; and a platelet count of greater than 70 × 109/L. PRRT was performed by the administration of a mean activity of 7.9 GBq of 177Lu-octreotate per treatment cycle, aimed at 4 courses at standard intervals of 3 mo (10–14 wk). At the time of administration, 177Lu (IDB Holland) had a specific activity of approximately 100–160 GBq/μmol. Peptide labeling (9,10) was performed to obtain an apparent specific activity of about 54 GBq/μmol (ratio of activity to the total amount of peptide). Nephroprotection was implemented with standard amino acid coinfusion according to the Rotterdam protocol (11,12) (2.5% lysine and 2.5% arginine in 1 L of 0.9% NaCl; infusion of 250 mL/h). Short-acting somatostatin analogs were required to be paused 1 d before the administration of 177Lu-octreotate, and long-acting analogs were required to be paused a minimum of 6 wk before PRRT. Informed consent was obtained from all patients before the initiation of therapy and before the administration of each treatment cycle.
Response Assessment
Restaging was performed 3 mo after the termination of PRRT. Imaging consisted of CT or MR imaging according to the baseline imaging modality. Follow-up imaging was performed at 6-mo intervals after the first restaging. Responses were evaluated according to modified Southwest Oncology Group solid tumor response criteria as described previously (5,13) and were classified as partial response, minor response (25%–49% decrease in the sum of perpendicular diameters), stable disease, and progressive disease. Documented tumor progression at any time before the end of treatment led to the termination of PRRT and the classification of the patient as having progressive disease. Because complete remission was not observed in the present study, this term does not appear in the analyses. The results of standard functional imaging (pre- and posttreatment somatostatin receptor imaging) were not incorporated into the response characterization in the present study.
Outcome and Statistical Analyses
The baseline characteristics of the study population were analyzed with regard to the tumor response. For this purpose, the Fisher exact test was applied after dichotomization for each factor and the resulting response: regression (partial response or minor response) versus nonregression (stable disease or progressive disease). Overall survival (OS) and progression-free survival (PFS) were analyzed with the Kaplan–Meier curve method (log-rank test) (P < 0.05). Patients were censored at the start of another antiproliferative treatment, such as chemotherapy or salvage PRRT. Univariate analysis with the log-rank test was performed for each baseline factor. Multivariate analysis (Cox proportional hazards model) by use of the stepwise model with backward elimination was performed with significant variables from the log-rank test. The Fisher exact test was used for comparing proportions of regression in patient groups dichotomized for baseline characteristics. For all tests, a 2-sided P value of less than 0.05 was considered significant. The statistical software package SPSS (version 18.0; SPSS Inc.) was used to analyze the data.
RESULTS
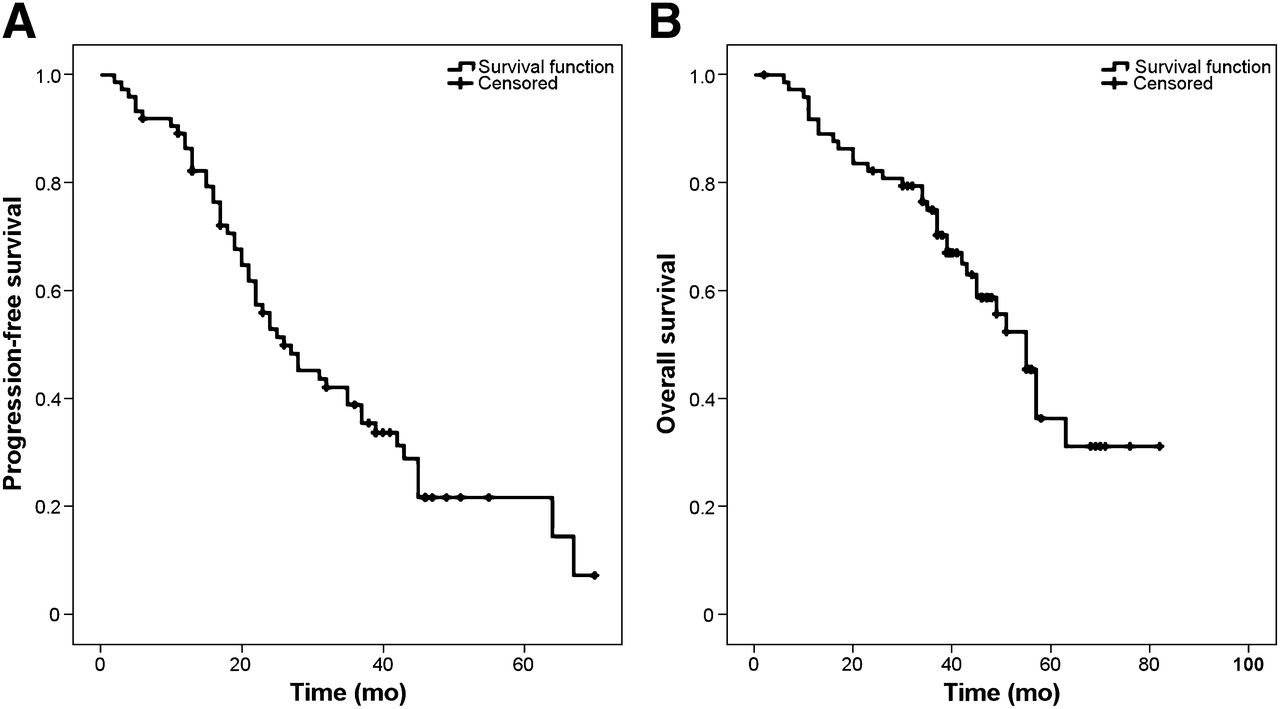
The median follow-up period was 47 mo (95% confidence interval [CI], 44.5–49.5), and the median OS of the entire cohort (n = 74) (Fig. 1) was 55 mo (95% CI, 48.8–61.2). Thirty-four patients (45.9%) had died by the end of the study. No treatment-related deaths were observed. Relevant transient myelosuppression (grade 3 or 4; Common Terminology Criteria for Adverse Events, version 3.0) occurred in less than 10% of treatments. No irreversible toxicity, including renal toxicity (grade 3 or 4), was noted.

Kaplan–Meier curves for PFS (A) and OS (B) of entire study cohort. Median PFS from start of treatment was 26 mo (95% CI, 18.3–33.7), and median OS was 55 mo (95% CI, 48.8–61.2).
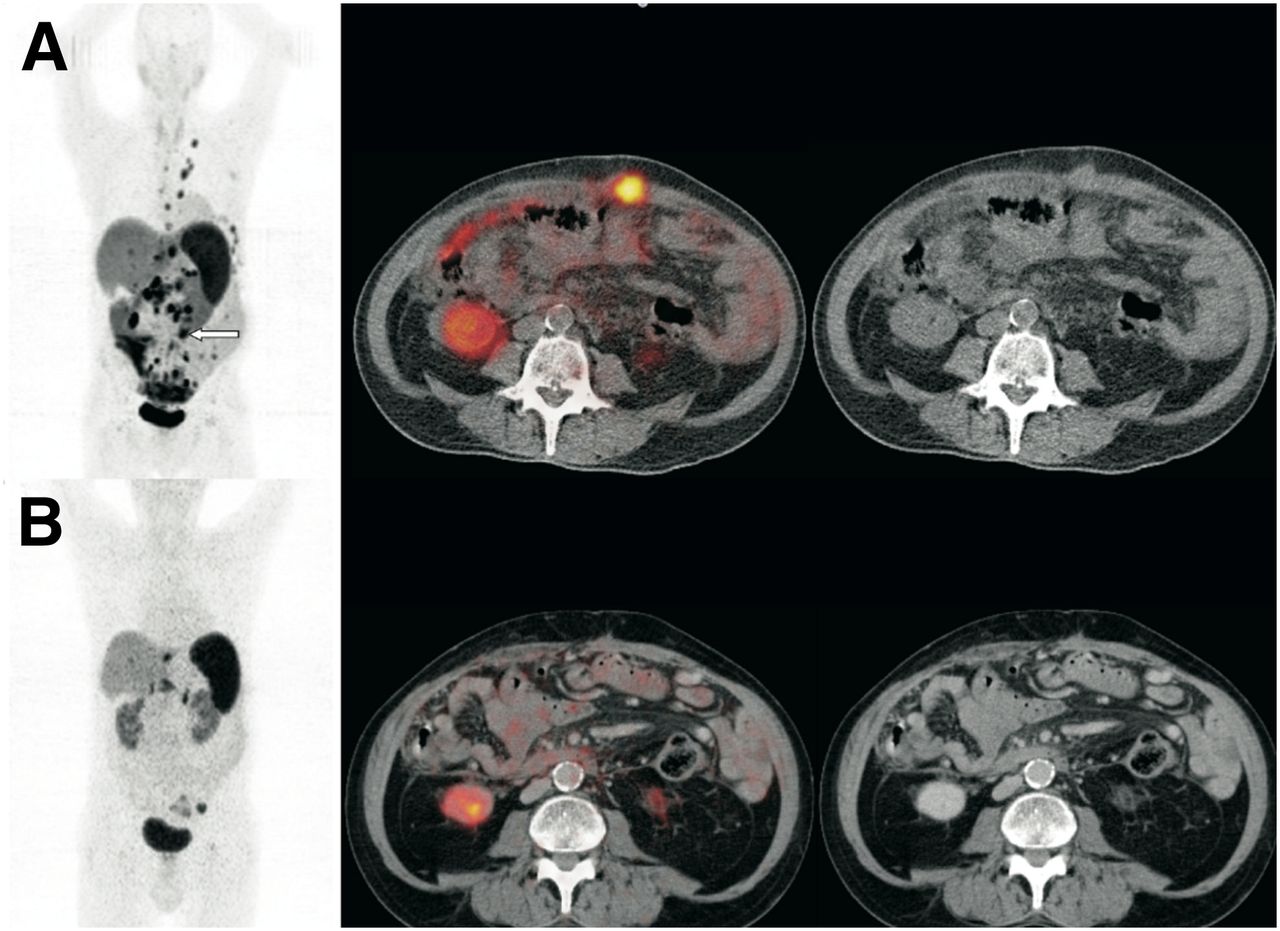
The observed response rates were 36.5% partial response, 17.6% minor response, 35.1% stable disease, and 10.8% progressive disease for the entire cohort; 54.5% partial response, 18.2% minor response, 18.2% stable disease, and 9.1% progressive disease for the pancreatic NET cohort; and 22.0% partial response, 17.1% minor response, 48.8% stable disease, and 12.2% progressive disease for the nonpancreatic GEP NET cohort. Figure 2 shows a partial response to PRRT in a patient with a pancreatic NET; the Ki-67 index was 20%. The analysis of various baseline factors for potential contributions to responses is shown in Table 2.
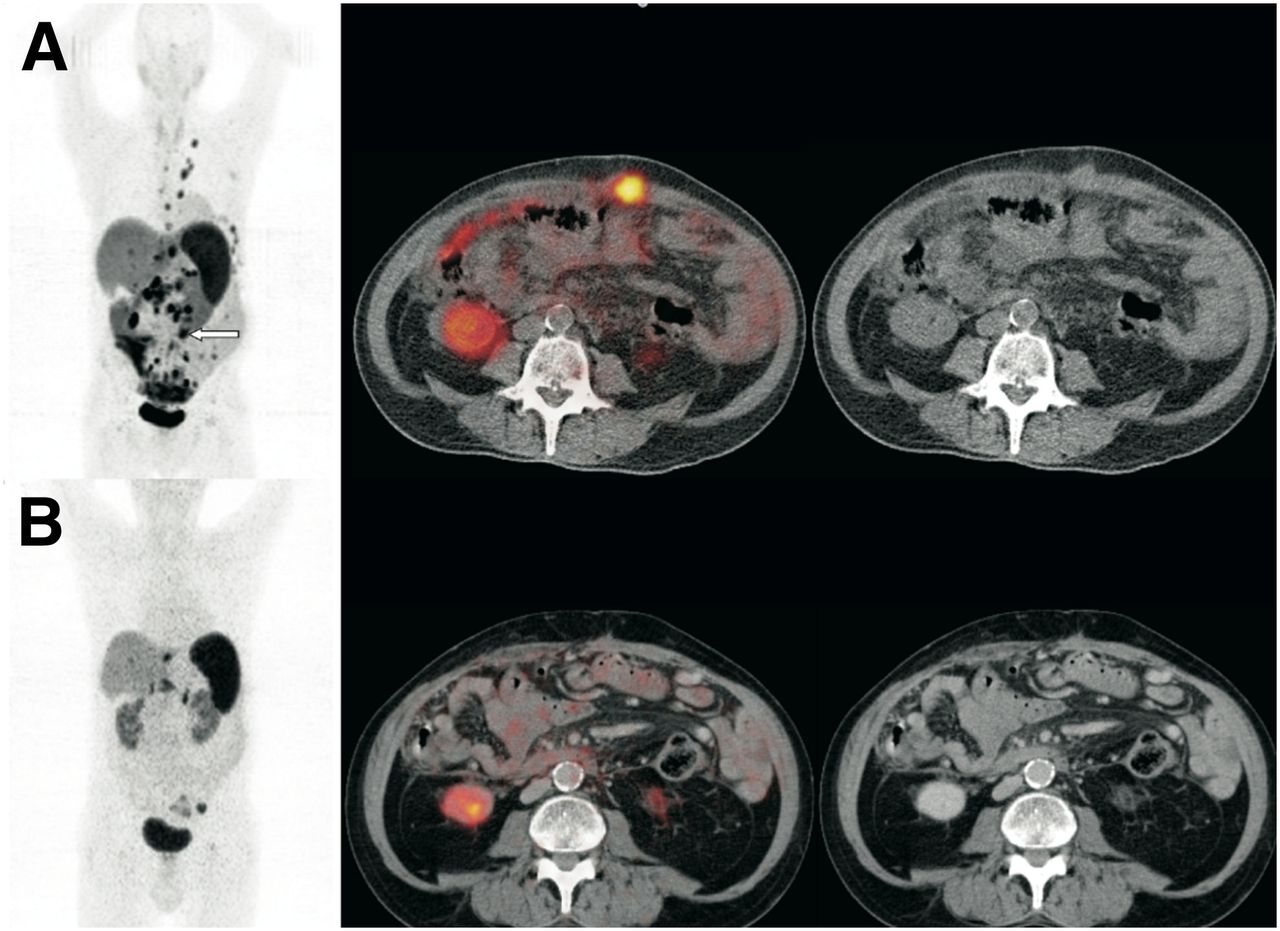
Regression of multiple metastases illustrated by 68Ga-DOTATOC PET/CT imaging before (A) and 3 mo after (B) PRRT in patient with metastatic NET of pancreas. Maximum-intensity-projection PET images (coronal views) are shown on left; fused and unfused CT images are shown on right. Selected lesion is indicated by arrow. This patient remained in partial remission for 20 mo; proliferation index (Ki-67 index) was 20%.
Morphologic Response to PRRT According to Various Baseline Factors
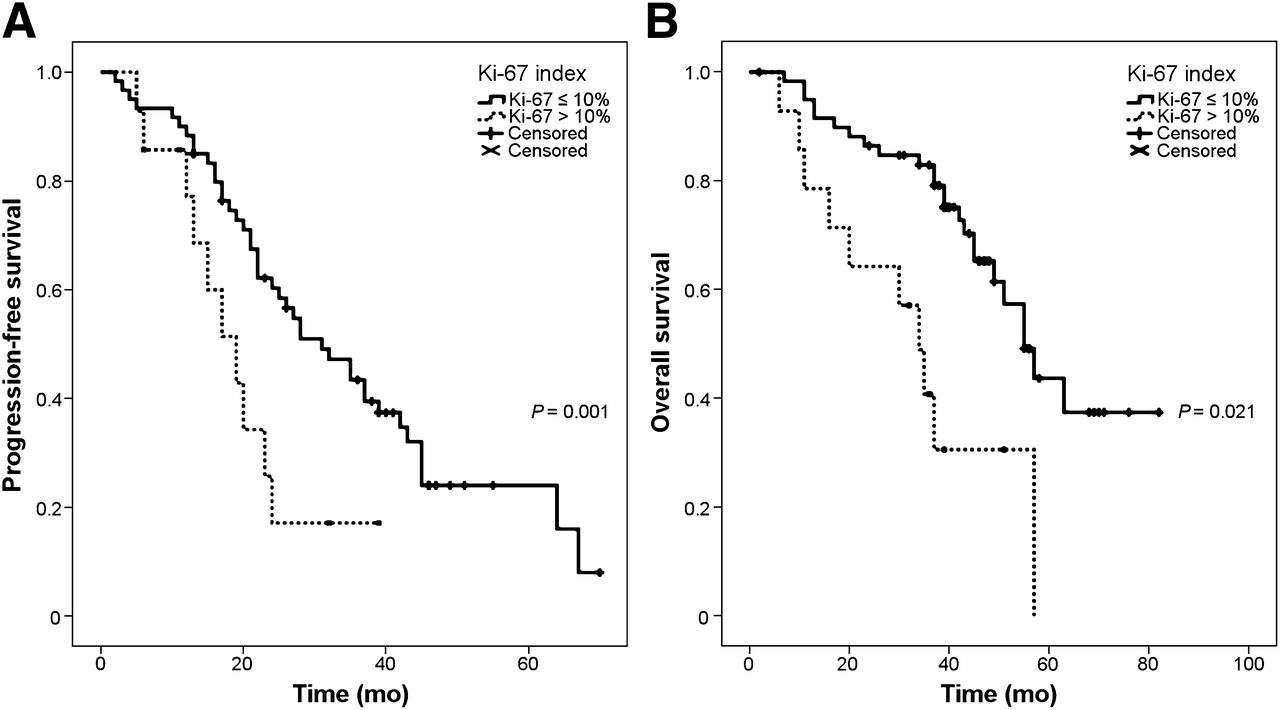
The median PFS was 26 mo (95% CI, 18.3–33.7) from the start of treatment (Fig. 1). The only factors contributing to time to progression in the univariate analysis were the Ki-67 index (cutoff, 10%; log-rank test, P = 0.02) (Fig. 3A) and hepatic tumor burden (cutoff, 25%; log-rank test, P = 0.006). Patients with a Ki-67 index of greater than 10% had a median PFS of 19 mo (95% CI, 12.4–25.6), and patients with a Ki-67 index of less than or equal to 10% had a median PFS of 31 mo (95% CI, 22.1–39.9).
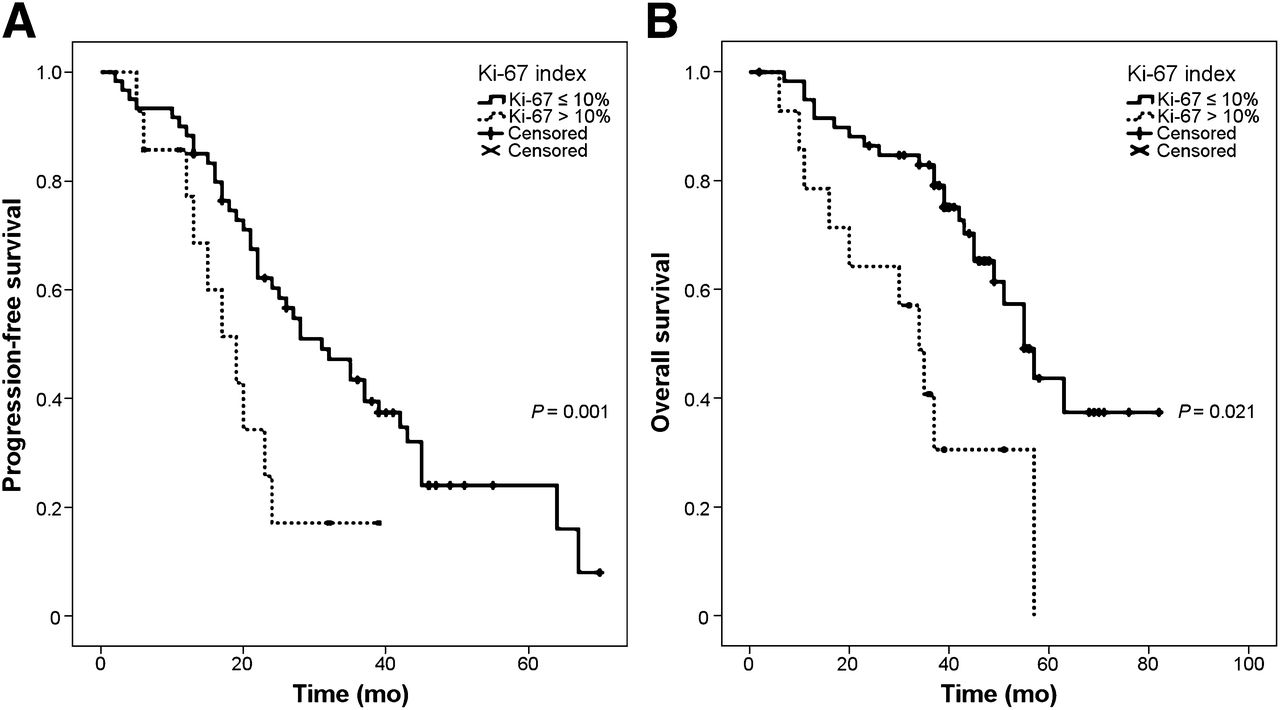
PFS (A) and OS (B) stratified by tumor proliferation index (Ki-67 index of ≤10% vs. >10%).
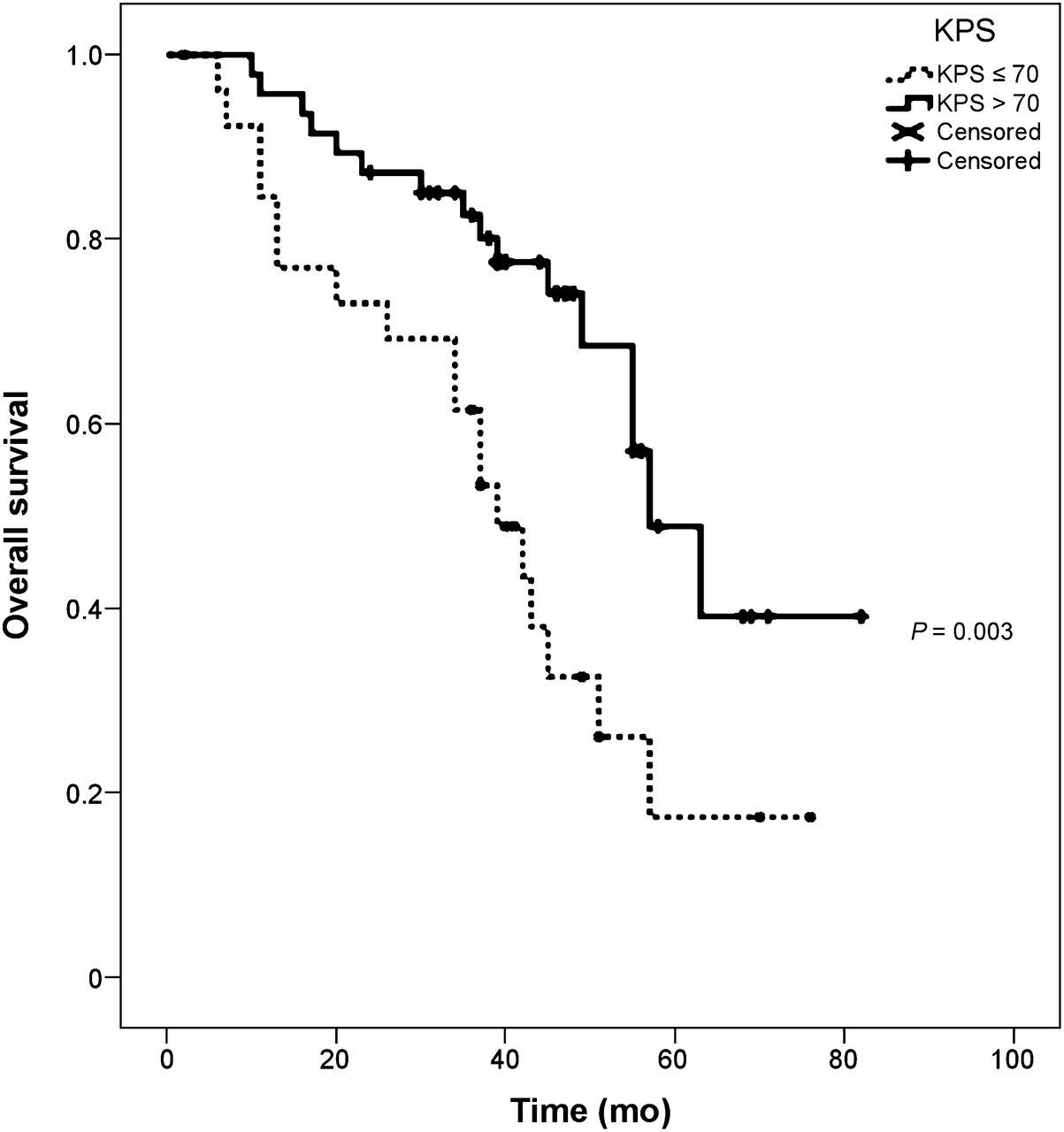
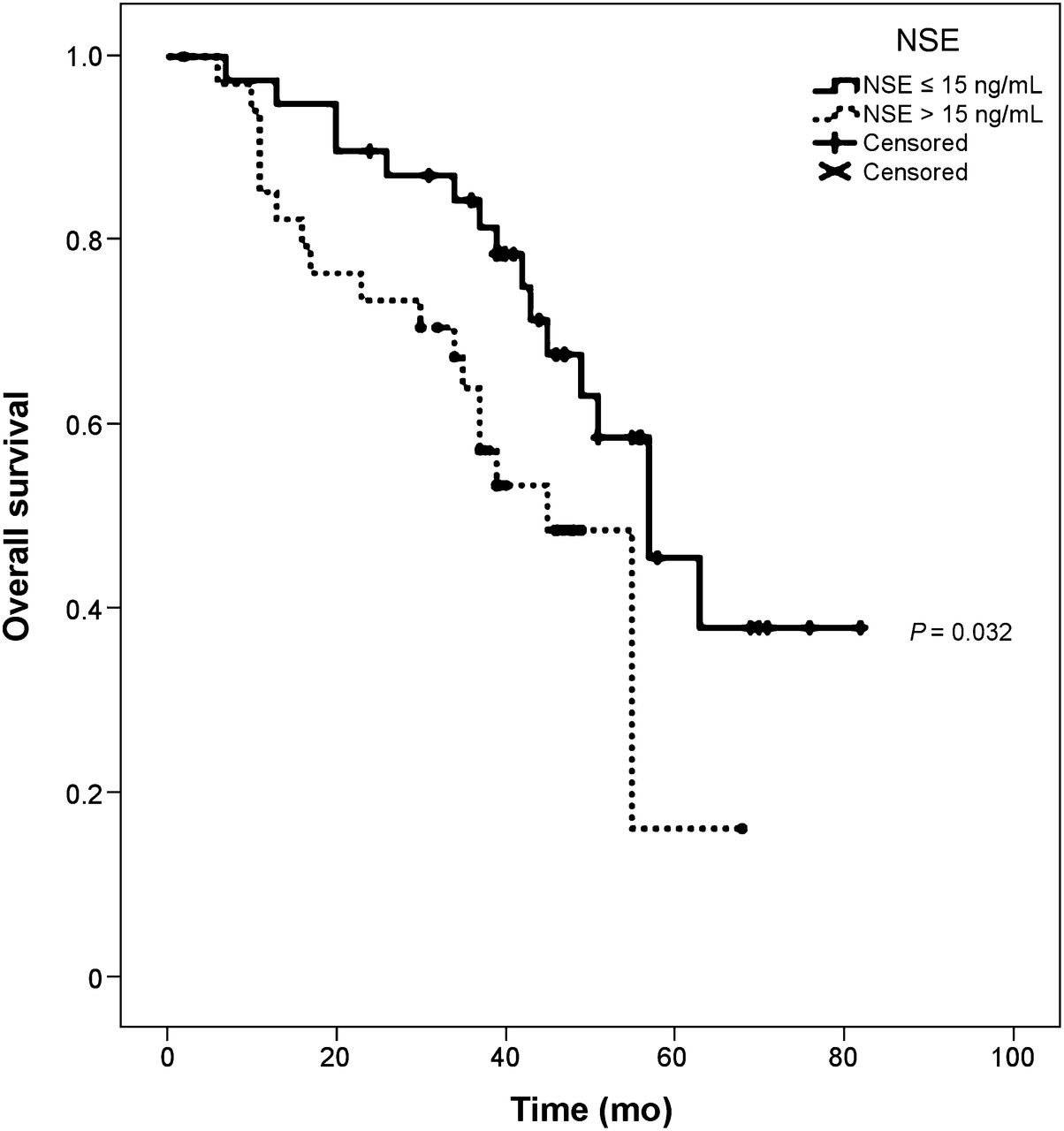
Analysis of the potential impact of various factors on OS is shown in Table 2. Of the contributing factors in the univariate analysis (log-rank test), only the Ki-67 index, tumor burden, Karnofsky performance score (KPS), and neuron-specific enolase (NSE) level at baseline remained significant in the multivariate analysis (Cox regression). Among the risk factors, a Ki-67 index of greater than 10%, a KPS of less than or equal to 70, and a plasma NSE concentration of greater than 15 ng/mL had hazard ratios of approximately 3; a hepatic tumor burden of greater than or equal to 25% was associated with a hazard ratio of 2.1 (Table 3). The Kaplan–Meier curves in Figures 3–6⇓⇓⇓ illustrate the prognostic value of these factors. The use of PRRT as a first-line treatment for metastatic disease did not affect outcome in our cohort (P = 0.936 for PFS; P = 0.364 for OS).
Univariate and Multivariate Analyses of Potential Factors Contributing to OS
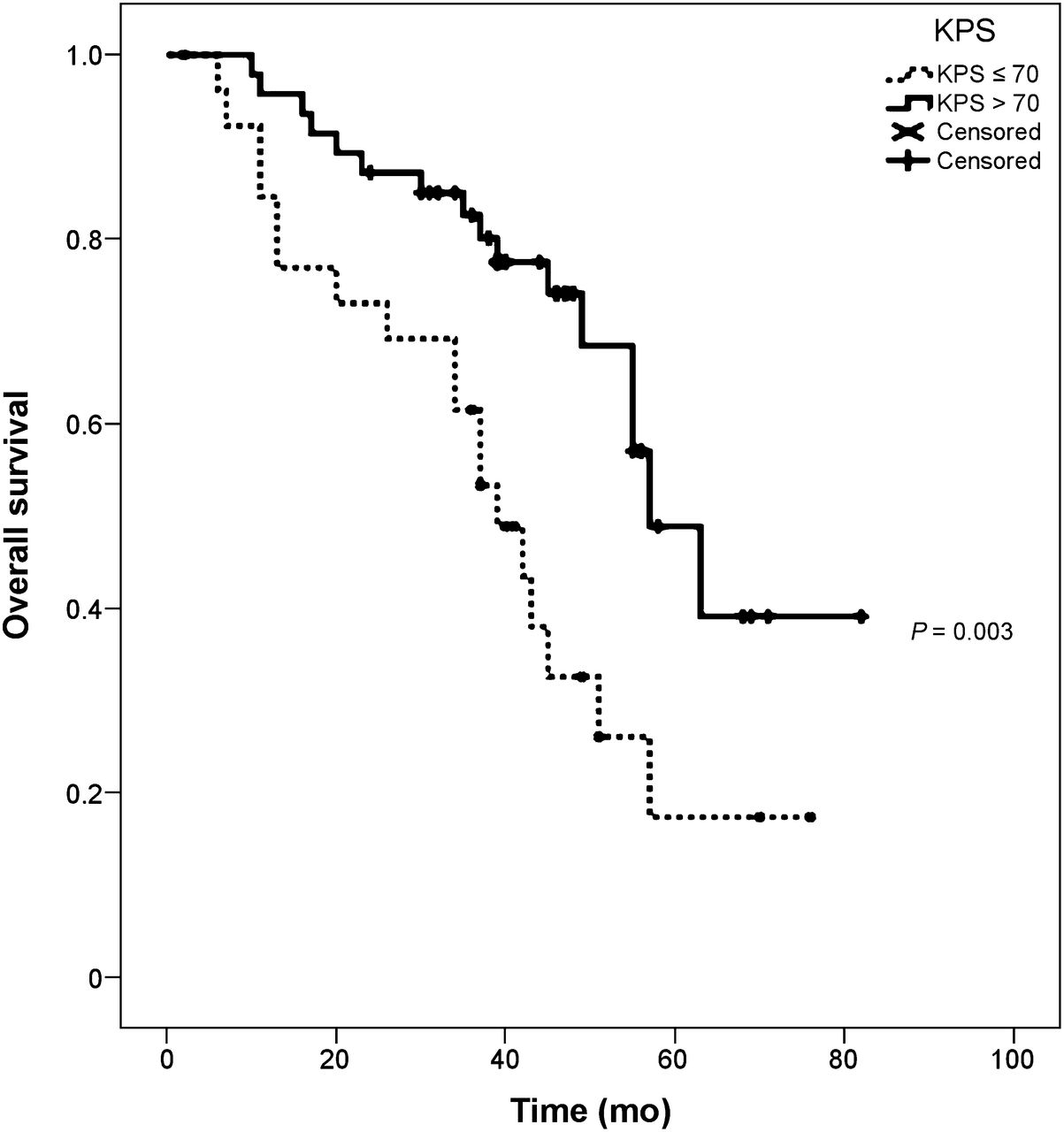
OS stratified by pretreatment KPS (≤70 vs. >70).

OS stratified by pretreatment plasma NSE level (≤15 ng/mL vs. >15 ng/mL).
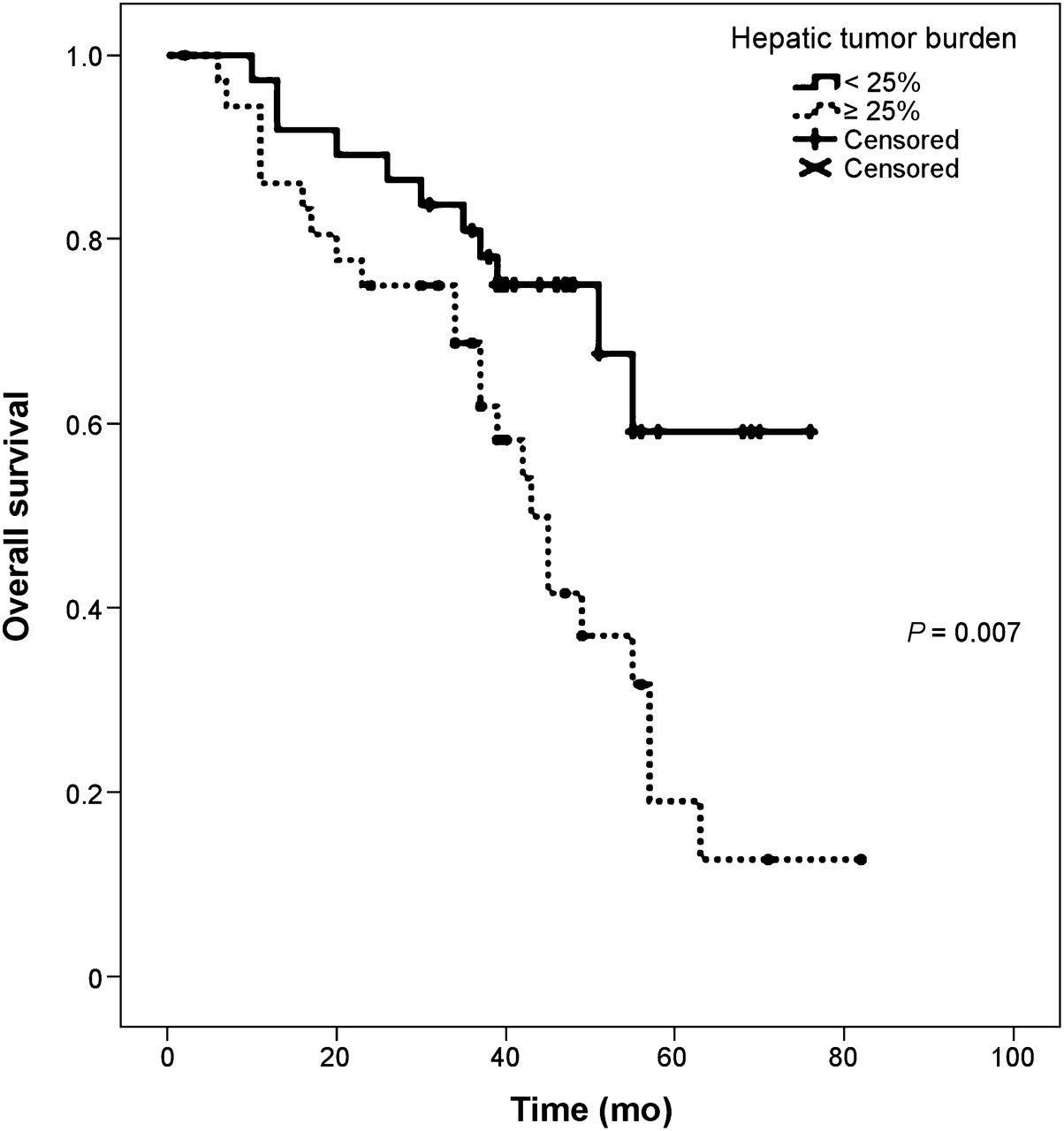
OS stratified by pretreatment hepatic tumor burden (<25% vs. ≥25% of liver volume).
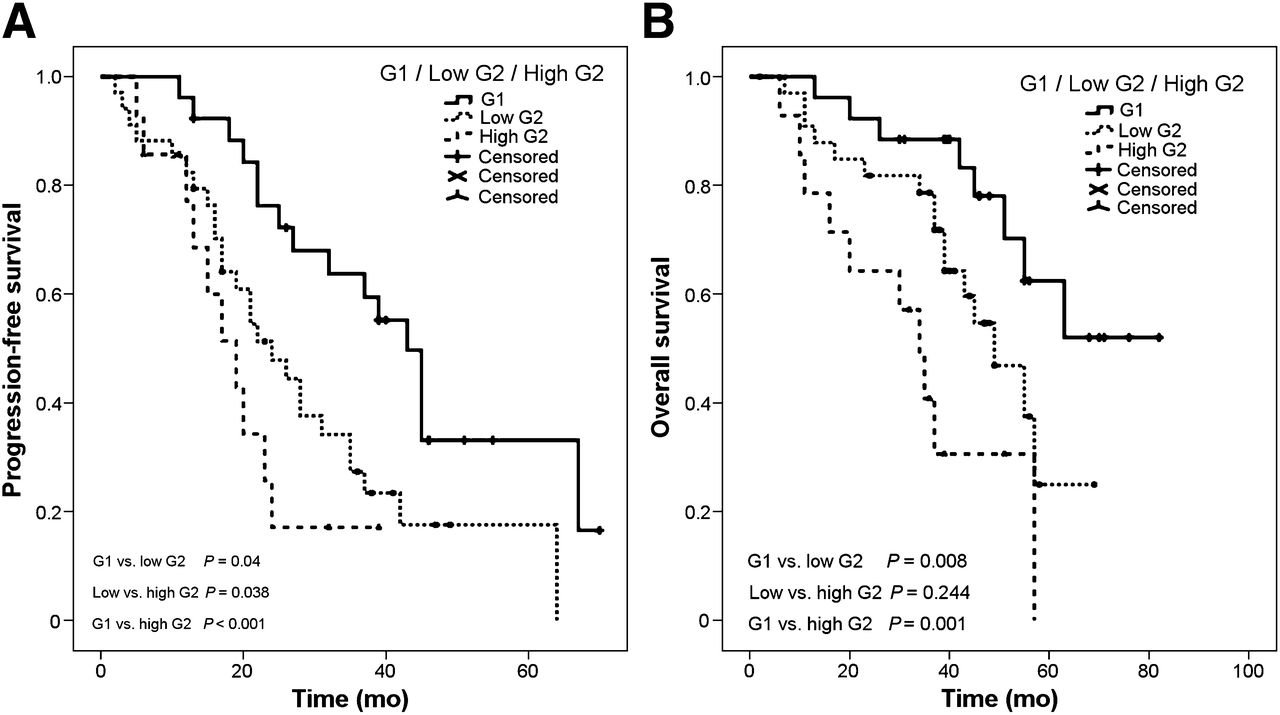
When the proliferation of tumors was stratified as G1 (Ki-67 index of < 3%), low-range G2 (Ki-67 index of 3%–10%), and high-range G2 (Ki-67 index of 15%–20%), the Kaplan–Meier curve analysis revealed a significant impact on PFS and OS (Fig. 7). Even the distinction between G1 and low-range G2 tumors was significant for the outcome; the median OS for patients with low-range G2 tumors was 49.0 mo (95% CI, 37.3–60.7), whereas the median OS for patients with G1 tumors was not reached after 82 mo (P = 0.04). The same was true for the distinction between low-range G2 and high-range G2 tumors (median OS of 34.0 mo; 95% CI, 25.8–42.2) (P = 0.038). With regard to PFS, patients with G1 tumors had a significantly better outcome (median PFS of 43.0 mo; 95% CI, 37.4–48.6) than patients with low-range G2 tumors (median PFS of 24.0 mo; 95% CI, 16.6–31.4) (P = 0.008), as shown in Figure 7.

PFS (A) and OS (B) stratified by tumor proliferation index into G1 (Ki-67 index of <3%; n = 26), low-range G2 (Ki-67 index of 3%–10%; n = 34), and high-range G2 (Ki-67 index of 15%–20%; n = 14). Median PFS times were 43.0 mo (95% CI, 37.4–48.6), 24.0 mo (95% CI, 16.6–31.4), and 19.0 mo (95% CI, 12.4–25.6), respectively. Median OS was not reached after 82 mo, 49.0 mo (95% CI, 37.3–60.7), and 34.0 mo (95% CI, 25.8–42.2), respectively.
For the small subgroup of patients with a Ki-67 index of greater than 10% (n = 14), there was no significant impact of hepatic tumor burden (P = 0.628) or tumor uptake (P = 0.586). In patients with a Ki-67 index of less than or equal to 10% (n = 60), a hepatic tumor burden of greater than or equal to 25% was associated with a shorter median OS (45 mo vs. not reached after 76 mo) (P = 0.016), whereas tumor uptake again had no impact on survival (P = 0.832).
Interestingly, patients in our cohort who had an unknown primary tumor had a significantly worse outcome than patients with nonpancreatic GEP NET for which the origin was determined (“carcinoid” of the foregut, midgut, or hindgut), that is, a shorter PFS (P = 0.001) and a shorter OS (P = 0.003).
DISCUSSION
This retrospective study of 74 patients with well-characterized GEP NET showed the strength of PRRT with 177Lu-octreotate, even in patients with advanced metastatic disease. The overall response rates of 36.5% (partial response) and 54.1% (regression rate; partial response plus minor response) and the median PFS and OS (26 and 55 mo, respectively) are highly promising and compare favorably with those achieved with other treatment modalities (14–18). The data were analyzed in accordance with the new World Health Organization criteria (2010) and should help with comparisons of outcome data from different patient cohorts in various treatment studies. However, given the nature of this retrospective series, with multiple potential biases—including retrospectively selected cutoff points—care must be taken in applying the results to clinical practice. Rather, the results provide strong evidence and a rational starting point for a prospective evaluation of the prognostic impact of various factors.
Well-differentiated GEP NET, especially those of nonpancreatic origin, show only a minor response to systemic chemotherapy. Initial studies with various chemotherapeutic agents reported a limited clinical benefit and a high rate of overall toxicity (19–25). Subsequent studies reported similar response rates after treatment with a temozolomide-based regimen (26–29), with a median PFS of up to 18 mo. Recent trials evaluated a variety of novel targeted agents (14,17,18,30–33) with disappointing low response rates (<20%) for gastrointestinal NET. The outcomes proved significantly better than those of placebo-treated control groups with pancreatic NET; the median PFS in patients treated with sunitinib or everolimus was up to 12 mo (30,34). Our finding of a median PFS of 27 mo and a median PFS of 25 mo for nonpancreatic GEP NET and pancreatic NET, respectively, compare favorably with the findings for systemic treatment in these historic control groups. However, these comparisons should be considered with caution and lack substantial validity, although they may provide some indication of efficacy in the absence of comparative trials in the field of PRRT.
The strongest predictor of outcome in our patient cohort was the proliferation marker Ki-67 index. It contributed to PFS and was 1 of 4 independent variables affecting survival after PRRT. Although the Ki-67 index is being increasingly recognized as a powerful determinant of survival in patients with GEP NET (35–38), its relevance in unresectable metastatic disease and potential cutoff values in the intermediate proliferative range for any treatment modality are still undefined because of a lack of data. In addition, the only published evidence for PRRT, to our knowledge, is an analysis of the impact of the Ki-67 index on responses (5), with no survival data available at that time. That study proved that indices within the entire G1/G2 range (i.e., Ki-67 of ≤20%) had no discernible proliferation–response relationship. Because the documented response was PFS for at least 12 mo (restaging performed >12 mo after the start of treatment), the reported data were clinically meaningful. With the data from the present study, it becomes clear that even though G2 tumors with a Ki-67 index of greater than 10% respond in a manner similar to that of tumors with a Ki-67 index of less than or equal to 10%, they show earlier progression after PRRT (median PFS of 19 mo vs. 31 mo) and produce shorter survival times (median OS of 34 mo vs. 55 mo). However, even this “impaired” survival of patients with NET in the “upper” G2 range is encouraging (median PFS and OS of 19 and 34 mo, respectively). It appears to be at least equal to that achieved with other treatment modalities (14), with reported OS of 11–24 mo (well-differentiated metastatic GEP NET) and 7–27 mo (well-differentiated metastatic pancreatic NET). We are aware that we should be cautious when making comparisons with historic control groups; nevertheless, it is fair to state that even the presented outcome for the subgroup with an unfavorable prognosis (Ki-67 of >10%) still indicates effective treatment and clearly does not provide an argument against performing PRRT in this subgroup.
Interestingly, stratification into G1 (Ki-67 index of <3%), low-range G2 (Ki-67 index of 3%–10%), and high-range G2 (Ki-67 index of 15%–20%) also had a prognostic impact on PFS and OS (Fig. 7). In particular, the distinction between G1 and low-range G2 tumors was significant with regard to PFS and OS (P = 0.008 and P = 0.04, respectively). Although it is well known that G1 and G2 tumors have different prognoses because of a divergence in the tendency to metastasize, we present the first evidence, to our knowledge, that even in patients with metastatic disease the G1/G2 distinction—in particular, between G1 (Ki-67 index of 1%–2%) and low-range G2 (Ki-67 index of 3%–10%)—provides prognostic stratification in a uniformly treated cohort. However, it remains unclear whether Ki-67 acts simply as a broad prognostic marker (i.e., patients with tumors with higher Ki-67 indices would naturally be expected to have shorter times to progression and shorter survival times, perhaps independent of treatment) or as a more specific predictor of the efficacy of PRRT.
Other factors contributing to OS were the patient’s performance status (Karnofsky performance score) (Fig. 4) and the plasma NSE level (Fig. 5). It is not surprising that the Karnofsky parameter predicted survival (2), although it is noteworthy that patients with a KPS of less than or equal to 70% still had a median OS of 39 mo (95% CI, 30–48) after PRRT. Also, the baseline NSE level was recently reported to be negatively associated with survival in patients with pancreatic NET in an interventional study (39), suggesting a prognostic impact of this secretory tumor marker. Although this marker was confirmed to be a general predictor for OS in our cohort, it lacked a respective significant impact in the subgroup analyses of pancreatic tumors (P = 0.06) and nonpancreatic tumors (P = 0.12). Larger investigations may eventually identify tumor subcategories in which an elevated baseline NSE level is of major prognostic relevance.
Previous work established the unfavorable prognostic character of functioning pancreatic tumors (2). In the present study, the responses of pancreatic NET consisted of a partial response in 54.5% of patients, a minor response in 18.2% of patients, stable disease in 18.2% of patients, and progressive disease in 9.1% of patients. Therefore, regression (partial response plus minor response) was observed in 72.7% patients with pancreatic NET. The median PFS was 25 mo (95% CI, 17–33), and the median OS was 57 mo (95% CI, 48–66). These outcomes were notable and compared well with those achieved with other current treatment modalities (14,18,27,30,40). For nonpancreatic GEP NET, the regression rate (partial response plus minor response) was 39.1%. The median PFS was 27 mo (95% CI, 16–38), and the median OS was 43 mo (95% CI, 31–55).
The known predictive factor tumor burden (Fig. 6) was confirmed by our analysis, in that patients with hepatic tumor involvement of greater than or equal to 25% of liver volume at baseline CT or MR imaging had a significantly shorter median OS (43 mo) than the remaining patients (median OS not reached after 76 mo). The difference remained significant in the subgroup with a Ki-67 index of less than 10% and proved to be an independent factor in the multivariate analysis (hazard ratio, 2.1) (P = 0.044). Another factor of known prognostic relevance, tumor uptake (2,3), did not have a significant predictive impact on either PFS or OS. Because the first 177Lu-octreotate therapy scan was uniformly used to classify tumor uptake, this parameter may perform in a manner different from that of others. On the basis of the 177Lu-octreotate scan, most patients fell into the high-uptake group (grade 3; in our cohort, 65/74 patients), probably providing less optimal stratification than a 111In-DTPA-octreotide scan (2) or a 90Y-DOTATOC scan (3). Perhaps a quantitative measurement method or a qualitative assessment at some earlier point after treatment would allow better stratification on the basis of the degree of tumor uptake. It would make biologic sense to expect some correlation between radiation dose and response or outcome.
The main limitation of the present study is its retrospective nature. However, because of the general lack of available prospective studies, potential predictors of outcome for patients with NET have been predominantly analyzed by use of retrospective data (16,35,36,38,41–44). The advantage of the present study is that our cohort of patients underwent the same treatment modality. The parameter Ki-67 index is associated with inherent inaccuracy regarding the time and localization of assessments, but this fact reflects clinicians’ reality and the use of the marker in routine settings as well as in clinical studies investigating and demonstrating the prognostic value of this parameter. It is not current practice to routinely assess the Ki-67 index at different sites during the course of disease, certainly because of the invasive nature of the assessment. The time lag–related inaccuracy of the proliferation index in the present study must be emphasized; however, despite the considerable interval between assessment and the start of PRRT (median, 14.5 mo; >12 mo in 38 patients), the immunohistochemical parameter proved to have high predictive power. Interestingly, even in the subgroup of patients with an interval of more than 12 mo between assessment and the start of PRRT (n = 38), the Ki-67 index was highly predictive of shorter survival times; the median OS in patients with a Ki-67 index of less than or equal to 10% was 55 mo, and that in patients with a Ki-67 index of greater than 10% was 34 mo (P = 0.003). To overcome the obvious problem of temporal and spatial inaccuracy resulting from the invasive nature of the proliferation assessment, supplemental alternative methods for tumor grading, such as noninvasive, whole-body molecular imaging for metabolic grading with 18F-FDG (45,46) or proliferation markers might be helpful in the future.
CONCLUSION
In the present study, we demonstrated a favorable outcome for patients with well-differentiated GEP NET graded as G1-2 after PRRT. Independent predictors of survival were the Ki-67 index, the patient’s performance status, the hepatic tumor burden, and the baseline NSE level. Even patients with a Ki-67 index of greater than 10% seemed to benefit from PRRT in terms of response and long-term outcome. Although it is well known that G1 and G2 tumors have different prognoses because of a divergence in the tendency to metastasize, we present the first evidence, to our knowledge, that even in patients with metastatic disease the G1/G2 distinction—specifically, between G1 (Ki-67 index of 1%–2%) and low-range G2 (Ki-67 index of 3%–10%)—provides prognostic stratification in a uniformly treated cohort. However, given the nature of this retrospective series, with multiple potential biases—including retrospectively selected cutoff points—care must be taken in applying the results to clinical practice. Rather, the results provide preliminary evidence and a rational starting point for prospective studies to establish the impact of the proposed predictors.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We are grateful to Professor Eric Krenning, Professor Dik Kwekkeboom, and Professor Wouter A.P. Breeman (Erasmus Medical Center, Rotterdam, The Netherlands) for sharing their invaluable experience in the receptor-targeting field and making somatostatin receptor–mediated treatment at all possible at our institution. Also, we thank Professor Richard P. Baum (Department of Nuclear Medicine and PET Center, Zentralklinik, Bad Berka, Germany) for his continuous critical and constructive input in this field. We also are thankful to the personnel of the Department of Nuclear Medicine and especially the nursing staff of the therapy ward.
Footnotes
Published online Jan. 16, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 23, 2013.
- Accepted for publication September 6, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety of Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE in Neuroendocrine Tumor Patients with Chronic Kidney Disease
- Parameters to Predict Progression-Free and Overall Survival After Peptide Receptor Radionuclide Therapy: A Multivariate Analysis in 782 Patients
- Twelve-Year Follow-up After Peptide Receptor Radionuclide Therapy
- Prognostic Value of 68Ga-DOTANOC PET/CT SUVmax in Patients with Neuroendocrine Tumors of the Pancreas
- Somatostatin Receptor-Targeted Radiopeptide Therapy with 90Y-DOTATOC and 177Lu-DOTATOC in Progressive Meningioma: Long-Term Results of a Phase II Clinical Trial
- Prognostic Stratification of Metastatic Gastroenteropancreatic Neuroendocrine Neoplasms by 18F-FDG PET: Feasibility of a Metabolic Grading System