


Abstract
The quantification of myocardial blood flow (MBF) and myocardial flow reserve (MFR) using PET with 82Rb in patients with known or suspected coronary artery disease has been demonstrated to have substantial prognostic and diagnostic value. However, multiple methods for estimation of an image-derived input function and several models for the nonlinear first-pass extraction of 82Rb by myocardium have been used. We sought to compare the differences in these methods and models and their impact on prognostic assessment in a large clinical dataset. Methods: Consecutive patients (n = 2,783) underwent clinically indicated rest–stress myocardial perfusion PET with 82Rb. The input function was derived using a region of interest (ROI) semiautomatically placed in the region of the mitral valve, factor analysis, and a hybrid method that creates an ROI from factor analysis. We used 5 commonly used extraction models for 82Rb to estimate MBF and MFR. Pearson correlations, bias, and Cohen κ were computed for the various measures. The relationship between MFR/stress MBF and annual rate of cardiac mortality was estimated with spline fits using Poisson regression. Finally, incremental value was assessed with the net reclassification improvement using Cox proportional hazards regression. Results: Correlations between MFR or stress MBF measures made with the same input function derivation method were generally high, regardless of extraction model used (Pearson r > 0.90). However, correlations between measures derived with the ROI method and other methods were only moderate (Pearson r = 0.42–0.62). Importantly, substantial biases were seen for most combinations. We saw that the relationship between cardiac mortality and stress MBF was variable depending on the input function method and extraction model, whereas the relationship between MFR and risk was highly consistent. Net reclassification improvement was comparable for most methods and models for MFR but was highly variable for stress MBF. Conclusion: Although both stress MBF and MFR can improve prognostic assessment, MFR is substantially more consistent, regardless of choice of input function derivation method and extraction model used.
Noninvasive quantification of myocardial blood flow (MBF) and myocardial flow reserve (MFR) with PET has been shown in several clinical cohorts to improve prognostic (1–6) and diagnostic (7–10) assessment of coronary artery disease (CAD). However, at least 5 models (Fig. 1) are commonly used for the correction of nonlinear extraction of 82Rb when quantifying MBF (11–16). Furthermore, the arterial blood pool input function has been traditionally determined using region-of-interest (ROI) methods, although factor analysis methods have been developed more recently and may have important advantages in reproducibility and accuracy (17,18). Substantial methodologic variation exists in the literature. Small studies have suggested that, on average, different software tools generate similar estimates for MFR, the ratio of stress to rest MBF (19–21), potentially due to cancellation of systematic differences. Further, these studies suggest that although population average MFR estimates are similar and correlations between different methods are reasonable, a substantial variation in individual measurements exists. No prior study comparing different methodologies has used a gold standard based on anatomy or clinical outcomes.

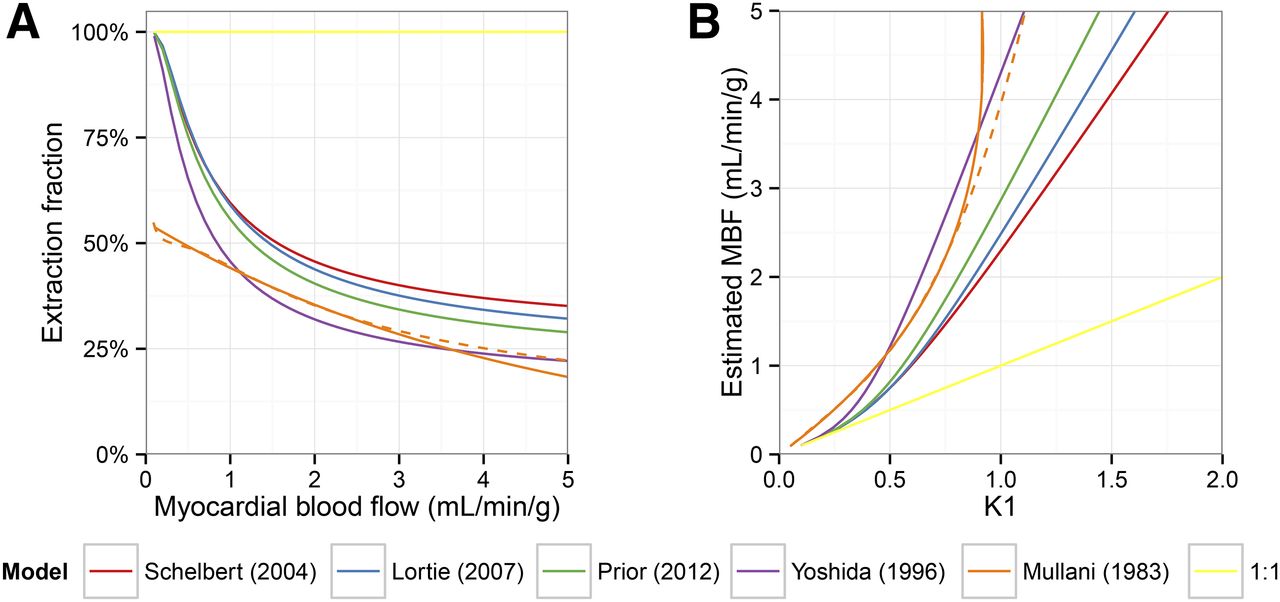
Variety of kinetic models. (A) All 5 of the commonly used models for extraction of 82Rb into myocardium predict substantial decrease in extraction for blood flows in physiologic range. (B) Consequently, estimated MBF grows more rapidly than K1 rate constant, amplifying uncertainty in blood flow estimates at ranges typical of stress hyperemia. Because the Mullani model is not defined for flows above 4.55 mL/min/g and K1 above 0.92, we modified this model slightly to be estimable uniquely across entire range of blood flows and K1 values (dashed lines).
We sought to systematically compare the effects of 3 methods for estimation of the arterial input function and 5 validated extraction models for 82Rb on the incremental prognostic value of blood flow quantification with PET in patients with known or suspected CAD.
MATERIALS AND METHODS
Study Population
We evaluated a previously described cohort of all patients referred for rest–stress cardiac PET at the Brigham and Women’s Hospital between January 1, 2006, and June 30, 2010 (3). The Partners Healthcare Institutional Review Board approved this retrospective study, and the requirement to obtain informed consent was waived.
PET Imaging
Patients were studied with a whole-body PET/CT scanner (Discovery RX or STE LightSpeed 64; GE Healthcare) in 2-dimensional mode using 1,480–2,200 MBq of 82Rb as a flow tracer at rest and stress as has previously been described (3). Dynamic datasets were reconstructed using ordered-subsets expectation maximization with an all-pass filter into 27 frames (14 × 5, 6 × 10, 3 × 20, 3 × 30, and 1 × 150 s). Maximal coronary vasodilation was achieved using dipyridamole, adenosine, regadenoson, or dobutamine, as clinically appropriate. PET images were evaluated semiquantitatively to quantify clinically overt myocardial scarring and ischemia (22) using the Corridor4DM software (INVIA Medical Imaging Solutions).
Flow Quantification
MBF at rest and stress was quantified using Corridor4DM. For each dataset, the arterial input function was quantified from dynamic images using 1 of 3 methods: a semiautomatically generated 3-dimensional region of interest (ROI) (6.5 × 6.5 × 30 mm) spanning the mitral valve, factor analysis (17,18), or a hybrid method with an ROI comprising the 20 highest-intensity pixels identified by factor analysis. Further details about the ROI method are provided in the supplemental material (available online at http://jnm.snmjournals.org). For the factor analysis and hybrid factor analysis methods, a right ventricular blood-pool time–activity curve was also quantified. The time–activity curve for the left ventricular myocardial tissue was generated using a semiautomatically generated ROI and was identical regardless of method used to determine the input function. The data were fit to a 2-compartment kinetic model (1-tissue compartment) to obtain 3 sets of estimates for K1 and k2 for each of the 3 methods. For the factor analysis and hybrid factor analysis methods, spillover from both the right and the left ventricles was also modeled. For the ROI method, only spillover from the left ventricle was modeled. To compute absolute MBF, each of the 3 sets of kinetic rate constants was entered into each of 5 validated extraction models for 82Rb: Mullani et al. (11), Yoshida et al. (13), Schelbert et al. (14), Lortie et al. (15), and Prior et al. (16). Because the model of Mullani et al. (11) has unstable behavior at high flows, several variations have been used. For this study, we used a Taylor series approximation of the original model [ and
and  ], which is shown as a dashed line in Figure 1. The model of Glatting et al. (12) was not included as it has been supplanted by that of Schelbert et al. (14), which was developed with the same dataset using the Renkin–Crone formalism (23,24). A sixth counterfactual model assuming 100% extraction of 82Rb was also included (1:1). In total, for each PET examination, 18 different rest and stress MBF estimates were generated. MFR was computed as the ratio of stress–rest MBF for each of these 18 combinations of arterial input function computation method and extraction model.
], which is shown as a dashed line in Figure 1. The model of Glatting et al. (12) was not included as it has been supplanted by that of Schelbert et al. (14), which was developed with the same dataset using the Renkin–Crone formalism (23,24). A sixth counterfactual model assuming 100% extraction of 82Rb was also included (1:1). In total, for each PET examination, 18 different rest and stress MBF estimates were generated. MFR was computed as the ratio of stress–rest MBF for each of these 18 combinations of arterial input function computation method and extraction model.
Assessment of Outcomes
The primary outcome was death from cardiac causes. Outcomes were ascertained by a combination of public (Social Security Death Index and National Death Index) and institutional databases as well as death certificates and were adjudicated by 2 cardiologists in a blinded manner. Cause of death could not be accurately adjudicated in 16 of 279 cases.
Statistical Analysis
Statistical significance was assessed with Wilcoxon tests, Fisher exact tests, and χ2 tests for continuous, dichotomous, and categoric variables, respectively. MFR and stress MBF computed with different methods were compared with paired t tests and Pearson correlation coefficients. Categorized MFR as <1.5, 1.5–2.0, and >2.0 were compared for different techniques using weighted Cohen κ (discrepancies were weighted by number of categories difference).
Poisson regression with generalized additive models was used to fit cubic splines for annualized event rates. Cox proportional hazards regression was used to adjust for the effects of clinical risk factors, left ventricular systolic function, and traditional semiquantitative measures of left ventricular perfusion. The incremental values of MFR and stress MBF were assessed with the continuous net reclassification improvement (NRI) and the c-index. Confidence intervals for these measures were constructed with bootstrap resampling with 1,000 replicates. All statistical analyses were performed with SAS 9.4 (SAS Institute Inc.) or R 3.1.0 (The R Foundation for Statistical Computing).
RESULTS
The characteristics of patients in this study are summarized in Table 1 and have previously been described in detail (3). During a median follow-up of 1.4 y (interquartile range, 0.7–2.4 y), 137 deaths from cardiac causes occurred.
Patient Characteristics
Variability in Kinetic Parameters
There is substantial variability in the estimated K1 and k2 parameters at both rest and stress based on which method of input function estimation is used (Supplemental Fig. 1; Supplemental Table 1). The ROI method resulted in higher estimates for K1 than the factor analysis and hybrid methods. Both the ROI and the hybrid methods generated higher estimates for k2 than the factor analysis method. Interestingly, when the ROI method was used, the estimates for K1 and k2 were moderately correlated (Pearson r = 0.41 and 0.51 for stress and rest, respectively; both P < 0.0001). No meaningful correlations between K1 and k2 were seen when the hybrid method was used (r = 0.01 and −0.02 for stress and rest, respectively; P = 0.72 and 0.23, respectively). Although statistically significant in this large sample, only minimal correlations were seen between K1 and k2 with factor analysis (r = 0.08 and 0.15 for stress and rest, respectively; both P < 0.0001).
Variability in Stress MBF and MFR Estimates
The distributions of stress MBF for each of the 5 extraction models for 82Rb were substantially different when the ROI method was used (Fig. 2; Supplemental Table 2). In contrast, when the hybrid and factor analysis methods were used, the estimated K1 fell into a range where the various extraction models were nearly identical. Consequently, the estimated distribution of stress MBF by these input function estimation methods was similar regardless of which extraction model was used. In contrast, for each input function estimation method, all 5 extraction models generated similar distributions of MFR (Fig. 3; Supplemental Table 2). However, the distributions of MFR obtained with the ROI method were wider and are skewed toward higher values, compared with the factor analysis and hybrid methods.

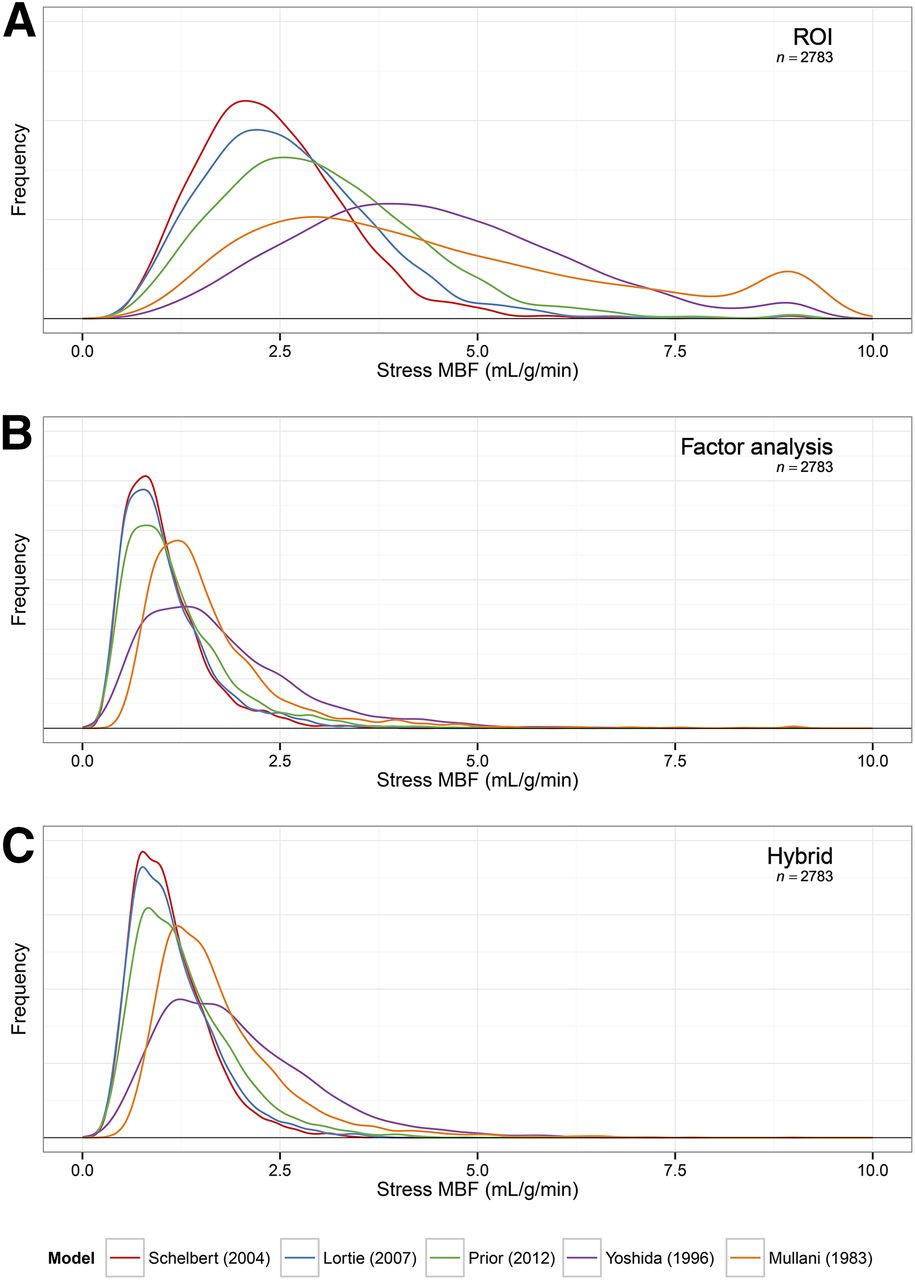
Distribution of stress MBF by input function method and 82Rb extraction model. Distribution of stress MBF estimates using ROI (A), factor analysis (B), and hybrid methods (C) for estimation of input function and 5 different clinically used extraction models.

Distribution of MFR by input function method and 82Rb extraction model. Distribution of MFR estimates using ROI (A), factor analysis (B), and hybrid methods (C) for estimation of input function and 5 different clinically used extraction models.
Overall, when all combinations of input function estimation methods and extraction models were compared against the combination of the hybrid method with the Yoshida extraction model used in prior publications (3,9,25–27), there was tremendous scatter (Supplemental Fig. 2A). Relatively little of this variability was attributable to the extraction model used (Supplemental Fig. 2B). Instead, most of the variability was attributable to differences between the input function estimation methods (Supplemental Fig. 2C). Correspondingly, correlations between stress MBF and MFR estimates were strong (Pearson r > 0.90) across different extraction models, as long as the same input function estimation method was used (Supplemental Figs. 3 and 4). Importantly, correlations between measures obtained using the ROI method and the other 2 methods were only moderate (Pearson r = 0.42–0.62). However, even with measures obtained using the same method for defining the input function, substantial biases in both MFR and stress MBF resulted if different extraction models were used (Supplemental Figs. 5 and 6). Finally, Cohen κ, a measure of repeatability, was used to evaluate the frequency of discrepant categorization of MFR as <1.5, 1.5–2.0, and >2.0, corresponding to validated categories of clinical risk (Supplemental Fig. 7) (3,4). Agreement was generally moderate to strong between MFR measures obtained with the same input function determination method and substantially weaker between different input function methods.
Prognostic Implications of Variation in Stress MBF and MFR
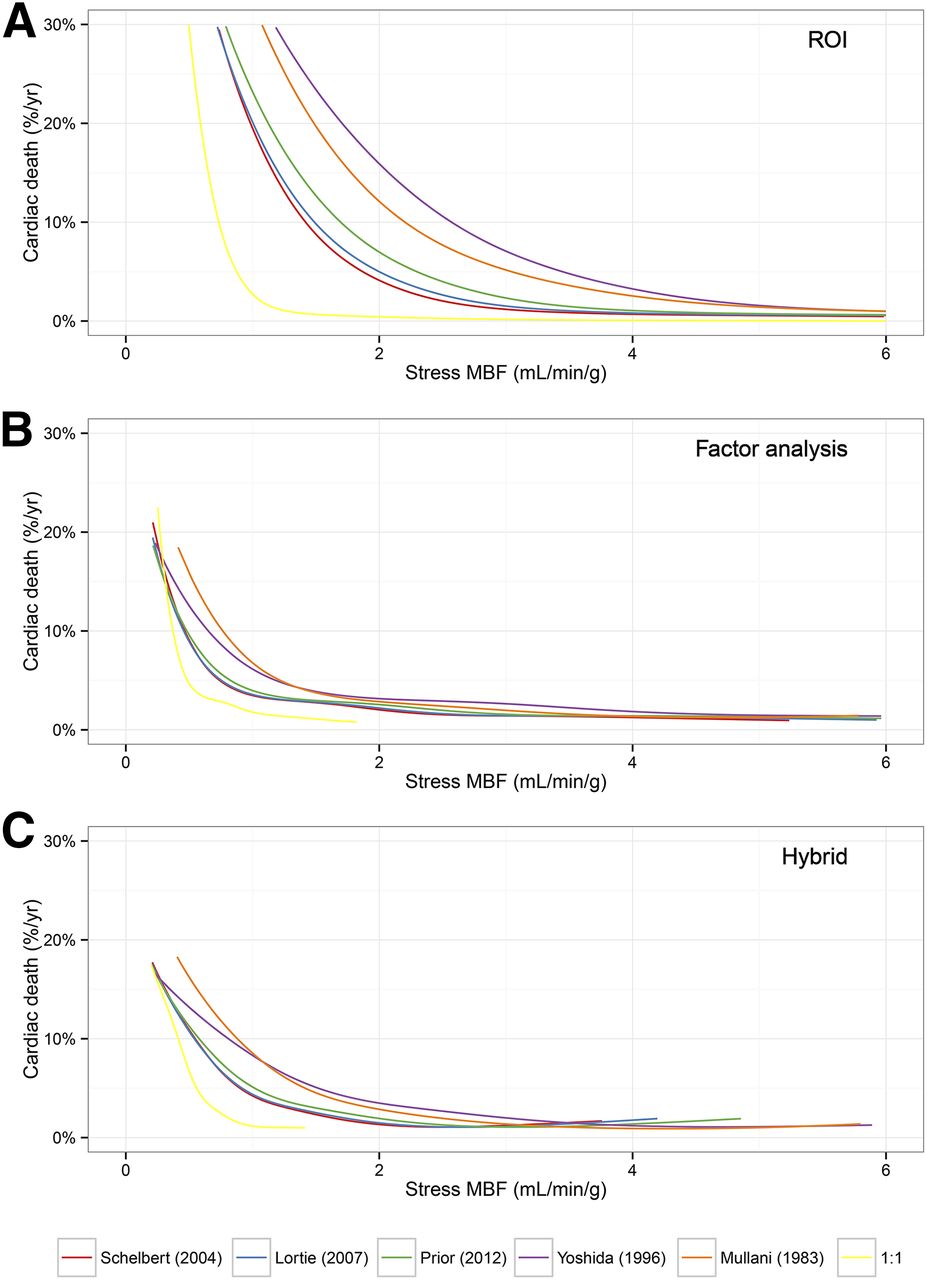
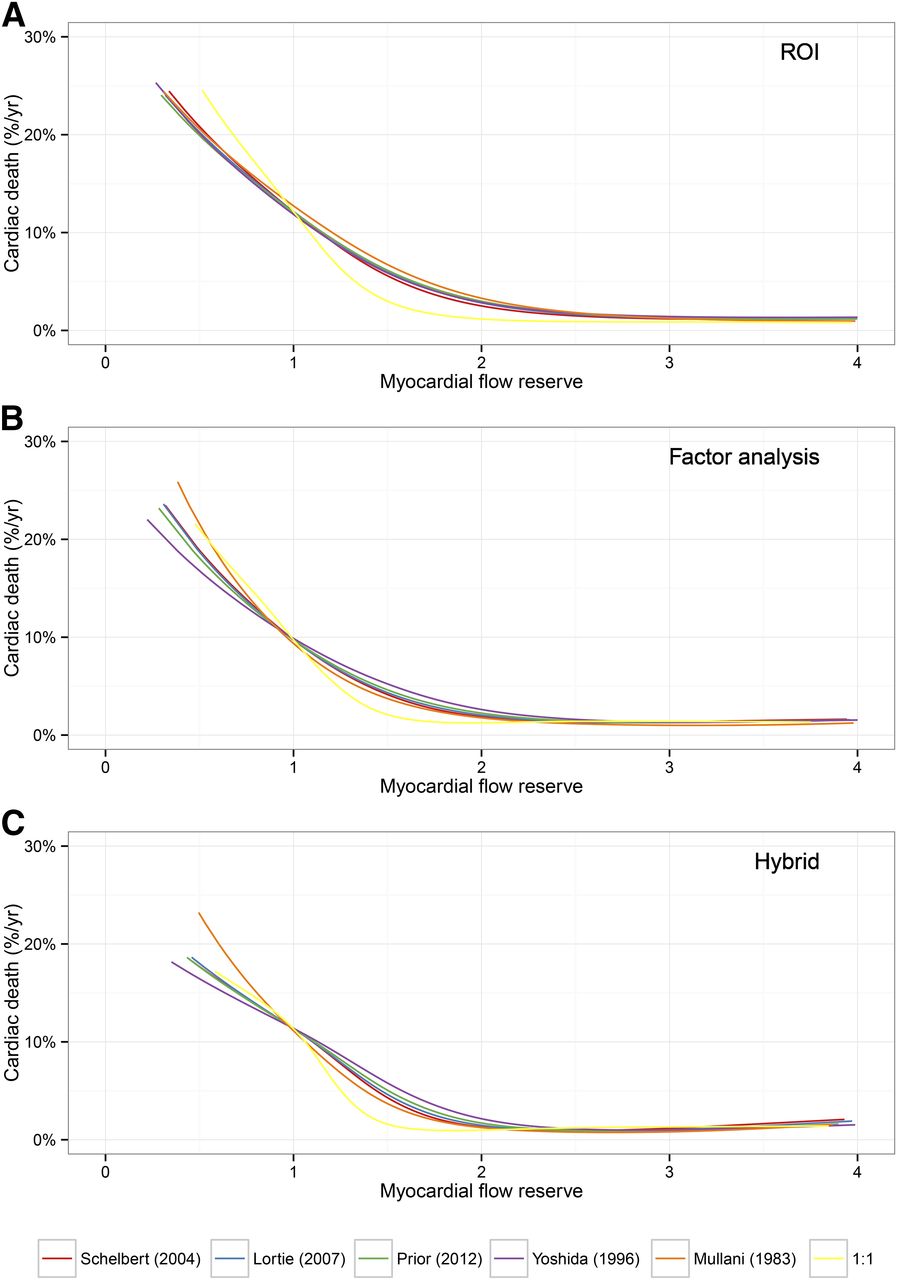
We used unadjusted Poisson regression with smoothing splines to estimate the annual cardiac mortality rate as a function of stress MBF and MFR (Figs. 4 and 5). Both lower MFR and lower stress MBF were associated with a substantial increase in annualized rate of cardiac death. Clear threshold effects were seen in nearly all cases except for stress MBF computed with the ROI method. Importantly, the thresholds below which substantial increases in cardiac mortality rates were seen differed widely across different 82Rb extraction models when the ROI method was used to define the input function. Somewhat less variability was seen when stress MBF measures were obtained using either the factor analysis or the hybrid methods to define the input function. Importantly, the risk versus MFR curves were remarkably similar regardless of which combination of extraction fraction model and input function determination method was used.
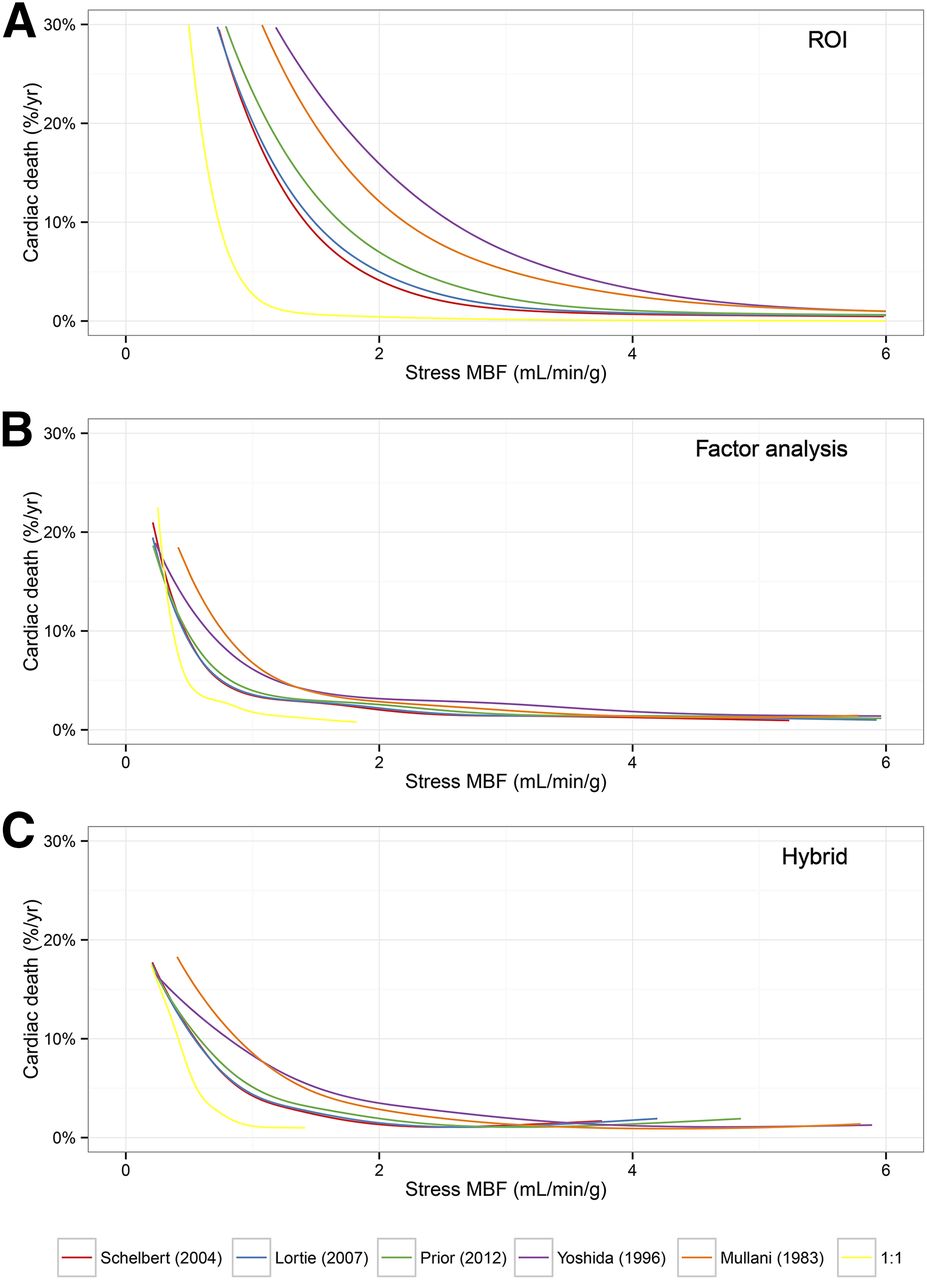
Risk of cardiac death versus stress MBF. Annual rate of death from cardiac causes as function of stress MBF computed using ROI (A), factor analysis (B), and hybrid methods (C) for estimation of input function and 5 different clinically used extraction models for 82Rb and 1 counterfactual model assuming 100% extraction (1:1). Curves were generated using Poisson regression with smoothing splines.
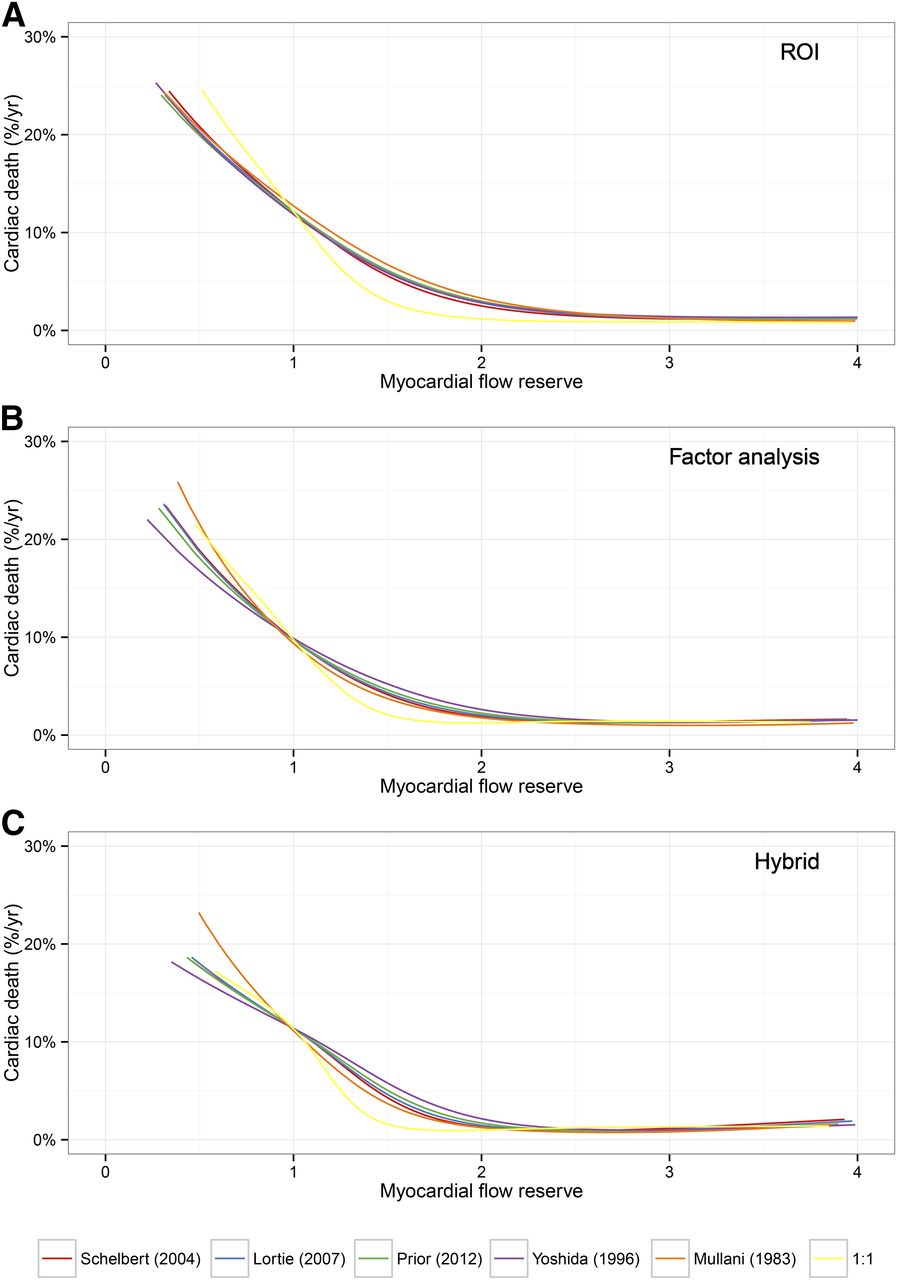
Risk of cardiac death versus MFR. Annual rate of death from cardiac causes as function of MFR computed using ROI (A), factor analysis (B), and hybrid methods (C) for estimation of input function and 5 different clinically used extraction models for 82Rb and 1 counterfactual model assuming 100% extraction (1:1). Curves were generated using Poisson regression with smoothing splines.
Last, we evaluated the incremental value of MFR and MBF measures with the continuous net reclassification improvement, comparing these measures with a base model including age, sex, hypertension, dyslipidemia, diabetes, smoking, family history of CAD, prior CAD, body mass index, chest pain, dyspnea, early revascularization (<90 d), left ventricular ejection fraction, left ventricular ejection fraction reserve, and the combined extent and severity of scar and ischemia (Supplemental Fig. 8A; Supplemental Table 3). We found that NRI was similar when the ROI or hybrid methods were used with any of the extraction models. NRIs for MFR computed using factor analysis were marginally smaller than NRIs from ROI or hybrid methods, though with substantial overlap of confidence intervals. Importantly, the NRIs for stress MBF measures were all lower than for MFR and were highly inconsistent depending on which method was used to define the input function (Supplemental Fig. 8B). Risk discrimination, as assessed by the c-index, was comparable for all combinations of input function estimation method and extraction model for both stress MBF and MFR (Supplemental Fig. 9).
DISCUSSION
We have demonstrated in a large clinical cohort that the choice of method for determination of input function and model for correction of the nonlinear extraction of 82Rb has a substantial impact on the resulting MBF and MFR measurements. Stress MBF measurements are highly variable, depending on technique used, especially when the ROI method is used to generate the input function. Indeed, when used with the ROI method, the extraction models of Mullani et al. (11) and Yoshida et al. (13) lead to extremely high stress MBF estimates, likely beyond what would be expected in clinical cohorts. In contrast, estimates of MFR are more similar, although substantial differences can still exist when different input function methods are used. Importantly, these sources of variability have a substantial impact on the relationship between specific values of stress MBF or MFR and the rate of cardiac mortality as well as on incremental risk reclassification. Overall, we found that MFR measures were substantially more consistent across variations in input function method and extraction model than stress MBF measures.
These data are inconsistent with prior, smaller studies (19–21), suggesting that measures with different software packages, some of which implement different choices with regard to the method of determination of the input function and the extraction model for 82Rb, may not be interchangeable clinically. Potential reasons for this could include limited power in prior studies, which had cohort sizes of 25–90 as compared with the 2,783 subjects analyzed for this study. Second, the other factors may have offset some of the differences. For example, temporal duration of frames used in dynamic acquisitions (28,29), filtering (30), and reconstruction algorithms (31,32) may also affect measured MBFs. Finally, subtle differences between the software method used for defining the ROI and the methods used in prior studies may also contribute.
Importantly, both K1 and k2 were substantially affected by the method used to estimate the input function. Although K1 is directly related to MBF, k2 is related to retention and washout of the tracer from tissue. The K1 measurements from the hybrid and factor analysis methods are lower, in general, than those from the ROI method (Supplemental Fig. 1). In this range of K1 values, the differences between the various extraction models for 82Rb are modest (Fig. 1). In contrast, the higher K1 values determined by the ROI method lead to greater divergences in estimated blood flow for the various 82Rb extraction models. It is possible that the larger variability in K1 and stress MBF with the ROI method could potentially improve sensitivity or specificity, although our analysis did not evaluate the use of these measures for diagnostic purposes.
Prior studies have demonstrated increased washout of 82Rb from nonviable myocardium (33,34). The application of this concept relies on accurate quantification of k2, which we have demonstrated varies markedly based on whether factor analysis, hybrid, or ROI methods are used. Importantly, K1 and k2 are substantially correlated when the ROI method is used and not meaningfully correlated for the hybrid and factor analysis methods. The observed correlation between K1 and k2 with the ROI method has no obvious physiologic basis and suggests that the ROI method may deliver estimates for these parameters with greater bias than factor analysis, as suggested by prior simulation studies (17).
These results have several important implications for clinical risk assessment. First, MFR estimates appear to be substantially more consistent than stress MBF measures. The potential cut points of stress MBF to define low-, intermediate-, and high-risk groups vary considerably depending on the method of input function determination and the extraction model used, limiting widespread clinical translation in the absence of much greater standardization than exists today. In contrast, MFR measures deliver more consistency in the relationship between the degree of reduction in MFR and the absolute cardiac mortality rate. In particular, an MFR greater than 2.0 is associated with favorable prognosis across all of the variations we evaluated and is consistent with the results seen in multiple independent clinical cohorts (1–6). Consequently, these data support the use of both rest and stress imaging to enable estimation of MFR rather than stress-only imaging for which only stress MBF could be measured. Although this combination of both rest and stress imaging results in increased exposures to patients, the effective dose remains modest, compared with SPECT radiopharmaceuticals.
Second, application of the large body of prognostic and diagnostic data for 82Rb PET to other perfusion tracers is uncertain and carries several important concerns. The same method for determination of the input function would be required for the other tracers, particularly for comparison of stress MBF. Translation of cut points across tracers would require highly reliable extraction models for both tracers. Unfortunately, for 82Rb substantial controversy exists as to the correct extraction model. All current extraction models incorporate biases and limitations related to the instrumentation, methodology, and reference standard used for their derivation and are thus more accurately thought of as calibration functions. MFR measures are potentially more reproducible across tracers than stress MBF metrics, although this has yet to be tested rigorously.
Important limitations of our work include that we only corrected for spillover of right ventricular blood pool with the hybrid and factor analysis methods and not with the ROI method. The impact of this discrepancy was minor (supplemental results). Furthermore, MFR and stress MBF were modeled as linear predictors for the purposes of NRI and c-index computation. Because we have demonstrated that risk of cardiac mortality is related to stress MBF and MFR in a highly nonlinear manner, our analyses of NRI and c-indices may substantially underestimate the potential incremental value of stress MBF and MFR. Finally, the cause of death was unknown in a few cases. This uncertainty combined with potential inaccuracies in death certificates could result in modest under- or overestimation of actual mortality rates.
CONCLUSION
Variability in the technique used to determine the input function and the extraction model for 82Rb can lead to large differences in estimates for stress MBF and, to a lesser extent, MFR. The greater variability in stress MBF measures results in substantial variation in the relationship between stress MBF and annual cardiac mortality, depending on the technique used. In contrast, MFR is considerably more consistent, with similar relationships between MFR and cardiac mortality, regardless of technique used. These results suggest that without careful standardization of methods, stress-only imaging cannot be readily generalized across multiple sites for clinical applications and in multicenter research studies.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by National Institutes of Health grant T32HL094301-02, the Blahd Research grant from the Society of Nuclear Medicine and Molecular Imaging, and research grants from the Intersocietal Accreditation Council and INVIA Medical Imaging Solutions. Dr. Ficaro owns equity in INVIA Medical Imaging Solutions. Dr. Sitek receives royalties related to factor analysis. Drs. Lee and Moody are employed by INVIA Medical Imaging Solutions.
Footnotes
Published online Nov. 26, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 5, 2014.
- Accepted for publication October 8, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Impaired Myocardial Flow Reserve on 82Rubidium Positron Emission Tomography/Computed Tomography in Patients With Systemic Sclerosis
- Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC
- Effect of Outflow Tract Contributions to 82Rb-PET Global Myocardial Blood Flow Computations
- Noninvasive Imaging to Evaluate Women With Stable Ischemic Heart Disease
- SPECT Myocardial Perfusion Reserve in Patients with Multivessel Coronary Disease: Correlation with Angiographic Findings and Invasive Fractional Flow Reserve Measurements
- Approaches to Reducing Radiation Dose from Radionuclide Myocardial Perfusion Imaging
- Coronary Microvascular Dysfunction, Microvascular Angina, and Treatment Strategies