


Abstract
Gastroenteropancreatic neuroendocrine tumors (GEPNETs) are indolent neoplasms presenting unpredictable and unusual biologic behavior that causes many clinical challenges. Tumor size, existence of metastasis, and histopathologic classification remain incapable in terms of treatment decision and prognosis estimation. This study aimed to compare 68Ga-DOTATATE and 18F-FDG PET/CT in GEPNETs and to investigate the relation between the complementary PET/CT results and histopathologic findings in the management of therapy, particularly in intermediate-grade patients. Methods: The relation between complementary 68Ga-DOTATATE and 18F-FDG PET/CT results of 27 GEPNET patients (mean age, 56 y; age range, 33–79 y) and histopathologic findings was evaluated according to grade and localization using standardized maximum uptake values and Ki67 indices. Grade 2 (G2) patients were further evaluated in 2 groups as G2a (3%–9%) and G2b (10%–20%) according to Ki67 indices. Results: The sensitivity of 68Ga-DOTATATE and 18F-FDG PET/CT was 95% and 37%, respectively, and the positive predictive values were 93.8% and 36.2%, respectively. The sensitivity in detecting liver metastasis, lymph nodes, bone metastasis, and primary lesion was 95%, 95%, 90%, and 93% for 68Ga-DOTATATE and 40%, 28%, 28%, and 75% for 18F-FDG, respectively. Statistically significant differences were found between grades 1–2, 2a–2b, and 1–2b with respect to 68Ga-DOTATATE PET/CT as well as between 1–2a and 1–2b with respect to 18F-FDG PET/CT. However, no statistical differences were found between 1 and 2a (P > 0.05) for 68Ga-DOTATATE and 2a and 2b (P = 0.484) for 18F-FDG. The impact of the combined 18F-FDG and 68Ga-DOTATATE PET/CT on the therapeutic decision was 59%. Conclusion: Combined 68Ga-DOTATATE and 18F-FDG PET/CT is helpful in the individual therapeutic approach of GEPNETs and can overcome the shortcomings of histopathologic grading especially in intermediate-grade GEPNETs.
Gastroenteropancreatic neuroendocrine tumors (GEPNETs) are rare neoplasms that present many clinical challenges (1). They arise throughout the gastrointestinal tract and pancreas and share certain basic characteristics. However, because of usually unpredictable and unusual biologic behavior, diagnosis is delayed especially in clinically silent tumors. Therefore, the recent World Health Organization 2010 classification was modified in favor of separately grading the GEPNETs based on the number of mitosis and Ki67 index (2). Accordingly, grade 1 (G1) (Ki67 index, <3%) and grade 2 (G2) tumors (Ki67 index, 3%–20%) are described as neuroendocrine tumors (NETs) and grade 3 (G3) (Ki67 index, >20%) as neuroendocrine carcinomas.
The diagnostic utility of 68Ga-labeled somatostatin analogs (68Ga-SMA) and 18F-FDG PET/CT has been well established in GEPNETs. The relation between the tumor grade and uptake has been reported as the higher uptake of 68Ga-SMA in low-grade versus high-grade NETs and the higher uptake of 18F-FDG in high-grade versus low-grade NETs (3). On the contrary, some studies have reported discordant results and failed to demonstrate such relationship (4). Thus, it is not always easy to identify a relation between the tracer uptake and histopathologic indices of tumor proliferation, which can guide therapeutic management. Multiple numbers of lesions with variable tracer uptake at different parts of the tumor, especially in the same organ, may cause the biopsy not to fully reflect in vivo tumor heterogeneity (5,6), thus leading to inaccurate Ki67 values. Likewise, tumors with lower proliferation are supposed to be less aggressive and vice versa, but that is not always the case. Therefore, maximum standardized uptake value (SUVmax) may provide advantages in overcoming the limitations of the histopathologic parameters, especially in intermediate-grade GEPNETs in which discordant results tend to be more common.
In this study, the relation of Ki67 indices with the tracer uptake of the primary and metastatic lesions in GEPNETs is evaluated by 68Ga-DOTATATE and 18F-FDG PET/CT using SUVmax as a semiquantitative measure. Furthermore, G2 tumors are evaluated by being separated into 2 groups.
MATERIALS AND METHODS
The institutional ethics committee approved this prospective study, and written informed consent was obtained from all patients. Twenty-seven consecutive patients (17 women and 10 men; age range, 33–79 y; mean age, 56 y) with histopathologically proven GEPNETs were examined by 68Ga-DOTATATE and 18F-FDG PET/CT. Indications of PET/CT were as follows: staging in patients with recent diagnosis, n= 9; detection of the primary tumor localization in metastatic patients with unknown primary origin, n = 8; and suspected recurrence or determination of disease spread, n = 10. All patients had a histologic diagnosis of GEPNET and were classified according to histologic grade as low (G1, n = 10), intermediate (G2, n = 15), or high (G3, n = 2) using Ki67 indices as determined by World Health Organization 2010 classification. A Ki67 value of less than 10% has been associated with better prognosis (7); therefore, we further grouped G2 patients as G2a (n = 10; Ki67, 3%–9%) and G2b (n = 5; Ki67, 10%–20%) accordingly. The time span between PET/CT scanning of patients with recent diagnosis and Ki67 measurements was 5 wk. When patients with suspected recurrence were considered, the mean time between Ki67 measurements and PET/CT imaging was 4.7 mo (range, 3–7 mo). None of the patients was treated previously at the time of Ki67 sampling. Of 29 histopathologic examinations, the source was the primary tumor in 15 and the metastatic lesions in 14. The source of metastatic tissue was liver (n = 13) and bone (n = 1). Two patients who were diagnosed by liver biopsies also had histopathologic evaluation of their surgically removed primary tumors. Multiple samples demonstrated similar Ki67 values and did not result in a change in histopathologic grade. The source of Ki67 samples and values are shown in Table 1.
Summary of Therapy-Relevant 18F-FDG and 68Ga-DOTATATE PET/CT Findings
68Ga-DOTATATE and 18F-FDG PET/CT
We performed 68Ga-DOTATATE labeling according to a previously described protocol (8). 68Ga-DOTATATE PET/CT was performed at 45–60 min after the intravenous injection of approximately 100 MBq of 68Ga-DOTATATE, and 18F-FDG PET/CT imaging was performed at 1 h after the intravenous injection of 370 MBq of 18F-FDG on a dedicated PET/CT scanner (Biograph TruePoint PET/CT; Siemens Healthcare) on separate days within a time span of 3 wk. An iodine-based, water-soluble high-contrast agent was administered orally to all patients. CT images were acquired on a spiral 6-slice CT scanner, with a slice thickness of 4 mm. After the transmission scan, 3-dimensional PET images were acquired for 4 min per bed position for 6–8 bed positions. CT-based attenuation correction of the emission images was used. PET images were reconstructed by the iterative method using ordered-subset expectation maximization (2 iterations and 8 subsets) with a filter size of 5 mm. After completion of the PET acquisition, the reconstructed PET images, CT images, and fused images of matching pairs of PET and CT images were reviewed using the dedicated software (TrueD VE31A; Siemens).
Image Interpretation
In the newly diagnosed patients, either the metastatic lesions of unknown origin or the primary tumors were detected by CT or MR imaging before biopsy. The indication of restaging PET/CT within patients with known GEPNETs was also based on findings detected by conventional imaging. PET/CT images were reviewed in consensus by 2 experienced and dedicated board-certified nuclear medicine physicians. A positive scan finding was defined as the significant accumulation of the tracer based on visual assessment. Areas of abnormally increased tracer uptake were documented, and findings were compared with both each other and Ki67 indices. Tumors were classified as showing either predominant 68Ga-DOTATATE or 18F-FDG uptake according to the number of detected lesions and SUVmax of the tracer as such; a patient was classified as 68Ga-DOTATATE–predominant if PET/CT detected a higher or equal number of lesions together with visually and quantitatively higher uptake of 68Ga-DOTATATE than 18F-FDG and vice versa. There were no patients with higher uptake and fewer lesions detected in one PET/CT study than the other or vice versa. Results were evaluated by a multidisciplinary board, and the impact of findings on treatment decision was reviewed.
Statistical Analysis
The variables were investigated using visual (histogram, probability plots) and analytic methods (Shapiro–Wilk test) to determine whether they were normally distributed. Descriptive analyses were presented using mean and SD for normally distributed variables, but median, minimum, and maximum were used for those that were nonnormally distributed. The paired Student t test was used for normally distributed related variables. The Wilcoxon test was used for the related nonnormally distributed variables. A P value of less than 0.05 was considered to show a statistically significant result. Analyses were performed by SPSS (version 21.0; IBM). Because of the limited number of patients in G3 (n = 2), statistical analysis was performed between G1, G2, and additionally between G2a and G2b. Sensitivity and positive predictive value were calculated for both PET/CT modalities.
RESULTS
In 8 patients with occult primary tumor, pancreas (n = 3) and bowel (n = 2) were detected as the primary origins whereas only metastatic lesions were detected in 3 patients. However, based on the histopathologic examination of the metastatic lesions and clinical evaluation, the patients were followed up and treated as GEPNETs. Overall, the primary tumor was localized in the pancreas (n = 13), bowel (n = 6), stomach (n = 3), liver (n = 1), and common bile duct (n = 1). Figure 1 demonstrates a metastatic GEPNET patient with unknown primary.

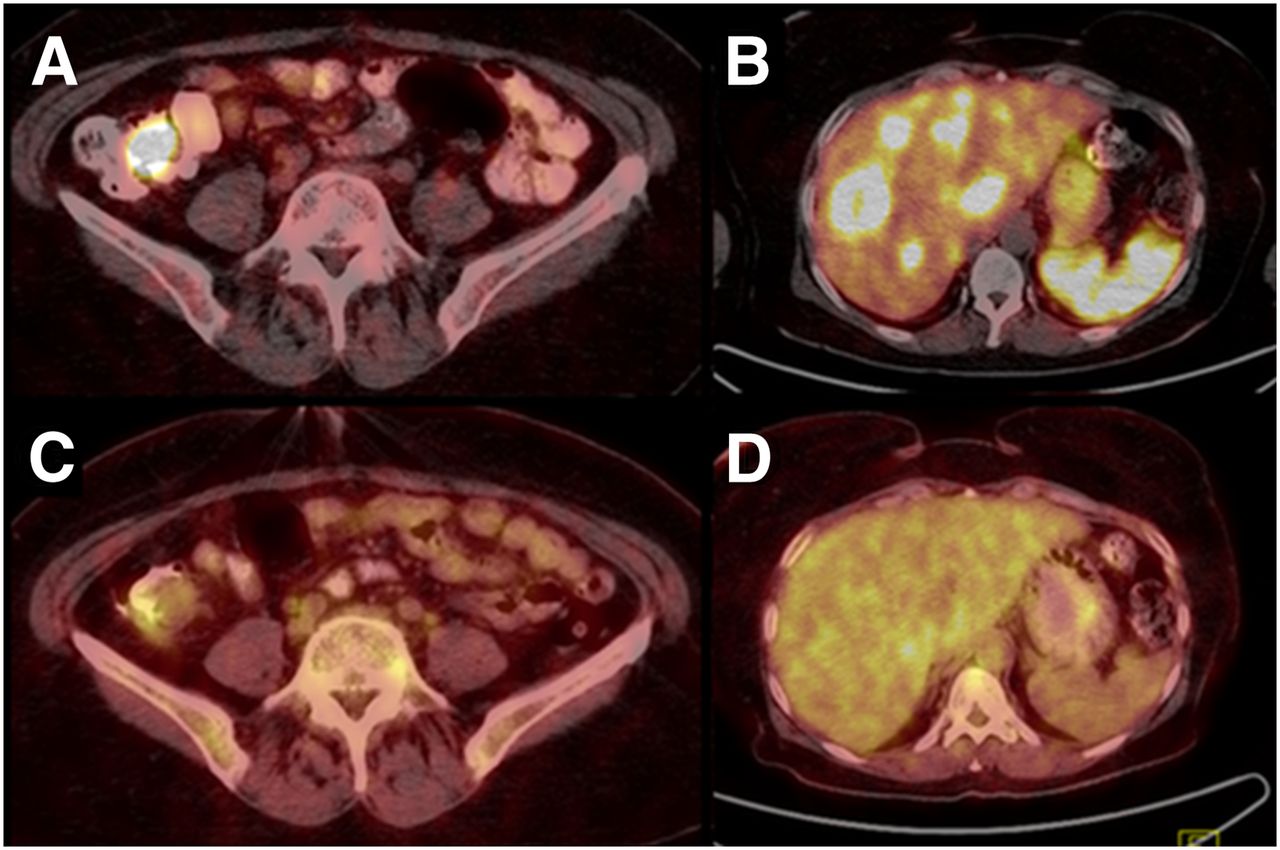
PET/CT was performed because of liver metastasis of G1 NET (Ki67, 1%). 68Ga-DOTATATE PET/CT reveals primary NET of cecum (A) and metastatic liver lesions (B). Primary lesion demonstrates mild 18F-FDG uptake (C) whereas liver lesions show no 18F-FDG uptake (D).
Tumoral lesions (n = 710) were detected in the liver (438), bone (173), lymph nodes (80), pancreas (11), bowel (5), and postoperative residual tumor (3). Two hundred twenty-one lesions corresponded on 68Ga-DOTATATE and 18F-FDG PET/CT; however, 489 lesions did not show a corresponding uptake in the other study (68Ga-DOTATATE, n = 450, and 18F-FDG PET/CT, n = 39) (Table 2).
Number of Metastatic Lesions According to PET/CT
False-positive lesions in 68Ga-DOTATATE (n = 5) and 18F-FDG (n = 8) PET/CT were determined on the basis of histopathology or clinical evaluation. As patients with known GEPNETs were enrolled in this study, only sensitivity and positive predictive value were calculated because of the lack of true-negative patients. The overall sensitivity of 68Ga-DOTATATE and 18F-FDG PET/CT was 95% and 37%, respectively, and positive predictive values were 93.8% and 36.2%, respectively. Table 3 presents sensitivity and median SUVmax of 68Ga-DOTATATE and 18F-FDG PET/CT according to histopathologic grades and anatomic sites. Median SUVmax of 68Ga-DOTATATE and 18F-FDG PET/CT are compared between grades, and statistical results are summarized in Table 4.
Comparison of Uptake Between 68Ga-DOTATATE and 18F-FDG PET/CT
Comparison of SUVmax Between Grades
Discordant and Concordant Findings
Concordant findings were acknowledged as 68Ga-DOTATATE predominance with lower Ki67 index and 18F-FDG positivity with higher Ki67 index. Findings were concordant in 71.4% (19/27) of the patients. Discordance was observed in 29.6% (8/27) of the patients. In 5 patients (Ki67, 1%–7%), 18F-FDG uptake at the primary tumor, liver metastasis, and lymph nodes was the cause of discordance. The lesions expressed somatostatin receptors (SSTRs) in 3 of 5 patients. Additionally, SSTR-positive (SSTR[+]) metastatic bone lesions in 1 of these patients had no 18F-FDG uptake. Significant 68Ga-DOTATATE but no 18F-FDG uptake in the metastatic lesions of a pancreatic NET (Ki67, 15%) was also evaluated as discordant; the patient had rapidly progressing advanced disease and lack of 18F-FDG uptake was not expected. In 2 patients (Ki67, 18% and 25%), 68Ga-DOTATATE PET/CT detected a greater number of metastatic bone and liver lesions and showed significantly higher tracer uptake than 18F-FDG PET/CT. However, there was no 18F-FDG uptake in the metastatic lymph nodes of these patients.
On the basis of the findings of 18F-FDG and 68Ga-DOTATATE PET/CT in comparison to the findings before PET/CT, therapeutic adjustments were made in 16 patients (Table 1). The overall impact of 18F-FDG and 68Ga-DOTATATE PET/CT imaging was 59% on the therapy management.
DISCUSSION
The sensitivity of functional imaging is higher than conventional imaging in GEPNETs (9,10). Several studies have proven the superiority of 68Ga-SMAs over conventional octreotide imaging with 111In-diethylenetriaminepentaacetic acid (111In-DTPA) and have reported high sensitivity values of up to 100% (11,12). 18F-FDG PET/CT imaging has also been compared with SSTR imaging in several studies and has a variable sensitivity of 36%–84% in detecting GEPNETs (3,13–15). However, the number of studies comparing 68Ga-SMA PET/CT with 18F-FDG PET/CT is limited.
The sensitivity of 68Ga-DOTATATE (95%) and 18F-FDG (37%) PET/CT in this study is similar to the reported values in the literature. Naswa et al. (14) reported the sensitivity for 68Ga-DOTANOC and 18F-FDG PET/CT as 91.4% and 42.5%, respectively. The performance of 68Ga-DOTATATE and 18F-FDG PET/CT according to lesion localization demonstrated similar results for primary tumor and lymph nodes when compared with Naswa et al. (14). However, the sensitivity of 68Ga-DOTATATE PET/CT was significantly higher than 18F-FDG in liver and bone metastasis in contrast to what was reported by Naswa et al. for 68Ga-DOTANOC. The patients presented by Naswa et al. lacked data pertaining to tumor biology; thus, uneven distribution of the patients according to grades may be a reason for this dissimilarity. Koukoraki et al. (16) reported the sensitivity of 68Ga-DOTATOC and 18F-FDG PET/CT as 90% and 68%, respectively, whereas Kayani et al. (3) reported 82% for 68Ga-DOTATATE and 66% for 18F-FDG PET/CT. Our results indicate a lower sensitivity when compared with Kayani et al. and Koukoraki et al. particularly for 18F-FDG PET/CT. The limited number of high-grade patients in the present study when compared with Kayani’s study may be a reason for such discrepancy. On the other hand, results of Kayani et al. lack Ki67 values in 13 of 38 patients and include 6 patients with lung NETs. Another issue to be specified is that 68Ga-SMAs other than 68Ga-DOTATATE used in these studies have different affinities for the SSTRs; however, in several studies evaluating the sensitivities and uptake values of 68Ga-DOTATATE versus 68Ga-DOTATOC and 68Ga-DOTANOC, no differences in diagnostic accuracy have been reported (17).
There is, to our knowledge, only 1 study evaluating the SUVmax of GEPNETs according to grade. Kayani et al. (3) reported statistically higher uptake of 68Ga-DOTATATE for G1 patients and 18F-FDG in G3 patients but no significant difference in G2 patients. However, this might be due to the relatively limited number of patients with G2 tumors (n = 6) in their study. In the present study, the median SUVmax of 68Ga-DOTATATE was significantly higher than the median SUVmax of 18F-FDG in both G1 and G2 patients. G3 patients (n = 2) were not evaluated because of the limited number of patients.
The mainstay of the treatment of GEPNETs is surgery (18), but histopathologic findings are usually decisive in the choice of treatment especially for inoperable patients or after surgery. Although Ki67 staining has been shown to have prognostic significance in GEPNETs (19), pitfalls such as tumor heterogeneity may cause misleading determination of tumor grade, especially in intermediate GEPNETs. A pathology report consensus concluded that the optimal method to determine the Ki67 index had yet to be defined because 47% of the participants believed that intraobserver reproducibility of the Ki67 index was not sufficient between pathologists (5). In addition, the availability of new treatment options has raised the need for new predictive biomarkers, and the data from clinical trials fail to provide the establishment of guidelines for Ki67 trigger levels (19). In this respect, PET/CT imaging may establish the missing link between histopathologic findings and clinical approach. Therefore, we evaluated the intermediate-grade GEPNETs in 2 subgroups to overcome the inadequacies of histopathology in terms of treatment approach. Few studies have compared 111In-DTPA octreotide findings with 18F-FDG PET/CT in this regard (13), but, to the best of our knowledge, there are no studies evaluating the 68Ga-DOTATATE PET/CT findings.
The present study demonstrates that the 68Ga-DOTATATE uptake is statistically different between subgroups of intermediate-grade GEPNETs. Median 68Ga-DOTATATE SUVmax of G2a patients is significantly higher than that of G2b patients; however, there is no significant difference between G2a and G1. In G2a patients, the uptake of 68Ga-DOTATATE is also significantly higher than the 18F-FDG uptake. On the contrary to 68Ga-DOTATATE, the median 18F-FDG SUVmax was not statistically different between G2a and 2b. Additionally, in G2b, there was no statically significant difference between the median SUVmax of 18F-FDG and 68Ga-DOTATATE PET/CT. However, the median 18F-FDG SUVmax of G2a and G2b were statistically higher than G1. These data demonstrate that GEPNETs with a Ki67 lower than 10% may be more suited to fall in the low-grade category in terms of SSTR positivity, which can alter the treatment. 68Ga-DOTATATE uptake values of G2b are statistically lower than those of G2a patients, suggesting that G2b (Ki67, >10%) patients may be considered as higher grade GEPNETs. However, it was not possible to draw a statistical conclusion regarding this relation because of the limited number of high-grade patients. Further studies in a larger cohort may prove to be more useful to better present the different biologic characteristics of the tumor on which individual treatment strategies rely.
A statistically significant difference for the median 18F-FDG SUVmax is not introduced between subgroups of G2 patients; however, 18F-FDG PET/CT findings were helpful in a patient-specific therapeutic approach. In 5 of 8 patients with discordant PET/CT findings, 18F-FDG uptake that was higher than expected was the reason. The subsequent therapy change was switching to chemotherapy in 4 of these patients. On the other hand, 18F-FDG positivity did not affect the treatment of choice in 1 patient (Ki67, 1%) with advanced disease. The patient had already received chemotherapy; therefore, the treatment of choice was peptide receptor–targeted radiotherapy (PRRT) as supported by the high uptake of 68Ga-DOTATATE in the metastatic lesions. In a previous study, it has been reported that chemotherapy can be used in tumors with a Ki67 lower than 5% if other therapies have failed (20). Furthermore, 18F-FDG PET/CT reflects high proliferative capacity and aggressive behavior in NETs (21) and correlates with the reduced progression-free survival (22); therefore, chemotherapy is recommended not only in high-grade NETs but also in metastatic intermediate NETs. Strosberg et al. have also reported chemotherapy as an earlier treatment option for tumors with a Ki67 higher than 10% following PRRT or somatostatin therapy (23). In the present study, 6 of 15 intermediate patients had chemotherapy in this regard. To set an example, 18F-FDG PET/CT additionally revealed significant hypermetabolism for the G2 (Ki67, 5%) patient with SSTR(+) progressive metastatic liver lesions; therefore, the ongoing somatostatin therapy was replaced by PRRT to be followed by chemotherapy because of the aggressive nature of the tumor (Fig. 2). In this context, 18F-FDG PET/CT has the potential to help adjust treatment decision in intermediate-grade GEPNETs, such as identifying the patients with the disease progression who can benefit from chemotherapy.
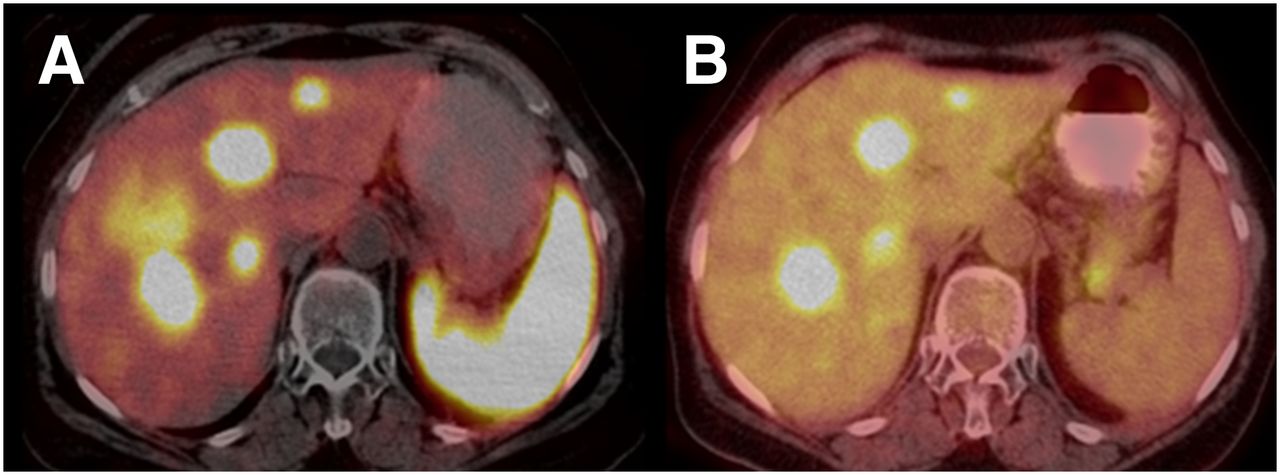
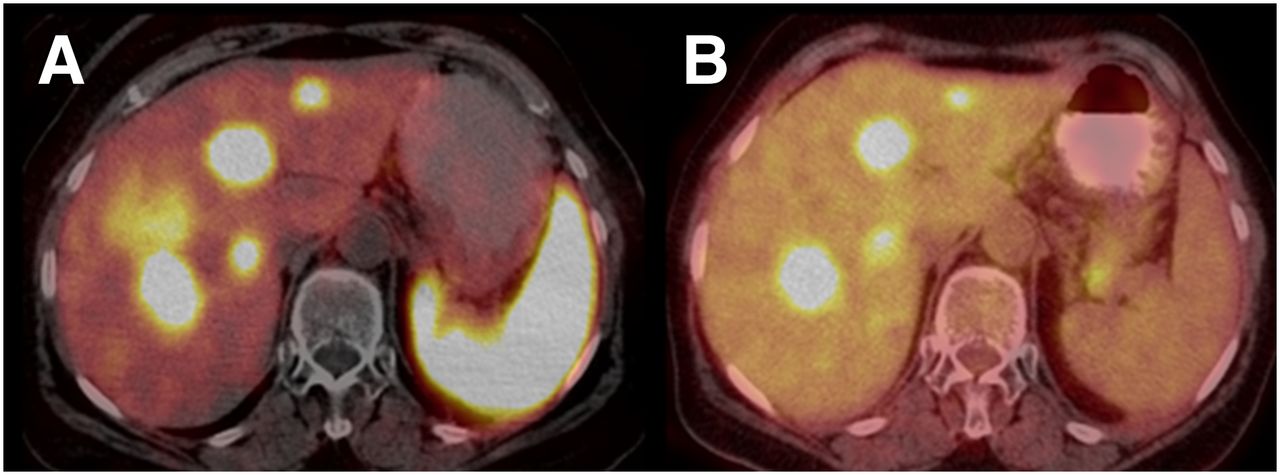
Multiple liver metastases of G2 (Ki67, 5%) pancreatic NET demonstrate high uptake of 68Ga-DOTATATE (A) (SUVmax, 25.3) and unexpectedly high uptake of 18F-FDG (B) (SUVmax, 12.9). PRRT is first choice of treatment. After evaluation of treatment response to PRRT, chemotherapy will be decided.
SSTR imaging is also important in selecting patients for PRRT. In our cohort, the ongoing somatostatin therapy was replaced by chemotherapy in an intermediate-grade patient (Ki67, 4%) with 18F-FDG(+) liver metastasis. However, the therapeutic decision was essentially based on the lack of SSTR on 68Ga-DOTATATE PET/CT (Fig. 3). With respect to 2 patients (Ki67, 15% and 18%) with advanced disease, it was decided that the somatostatin therapy along with transarterial chemoembolization of the 18F-FDG–negative metastatic liver lesion would be continued for one and a switch to PRRT would be made for the other patient, as confirmed by the 68Ga-DOTATATE uptake. On the other hand, it has been reported by Jamali et al. (24) that 18F-FDG–positive high-grade patients could also benefit from PRRT. Similarly, a high-grade patient (Ki67, 25%) in our cohort had SSTR(+) bone and liver metastasis and was referred to PRRT (Fig. 4). The upper limit of the Ki67 index for PRRT has been reported as 30% in the recent Clinical Practice Guidelines of the European Society for Medical Oncology (25). A drawback of the current study is the lack of high-grade patients; therefore, it is not possible to draw a statistical conclusion on the routine use of 68Ga-DOTATATE PET/CT in the management of high-grade patients. In conclusion, in 16 patients—8 of whom had discordant results—complementary PET/CT altered the therapeutic management. The impact of complementary PET/CT in therapeutic management was 59%.

G2 (Ki67, 4%) NET of stomach under somatostatin therapy with progressive metastatic disease demonstrates no 68Ga-DOTATATE uptake (A) in 18F-FDG–positive (B) (SUVmax, 7.2) metastatic liver lesion. Somatostatin therapy was discontinued in favor of chemotherapy.
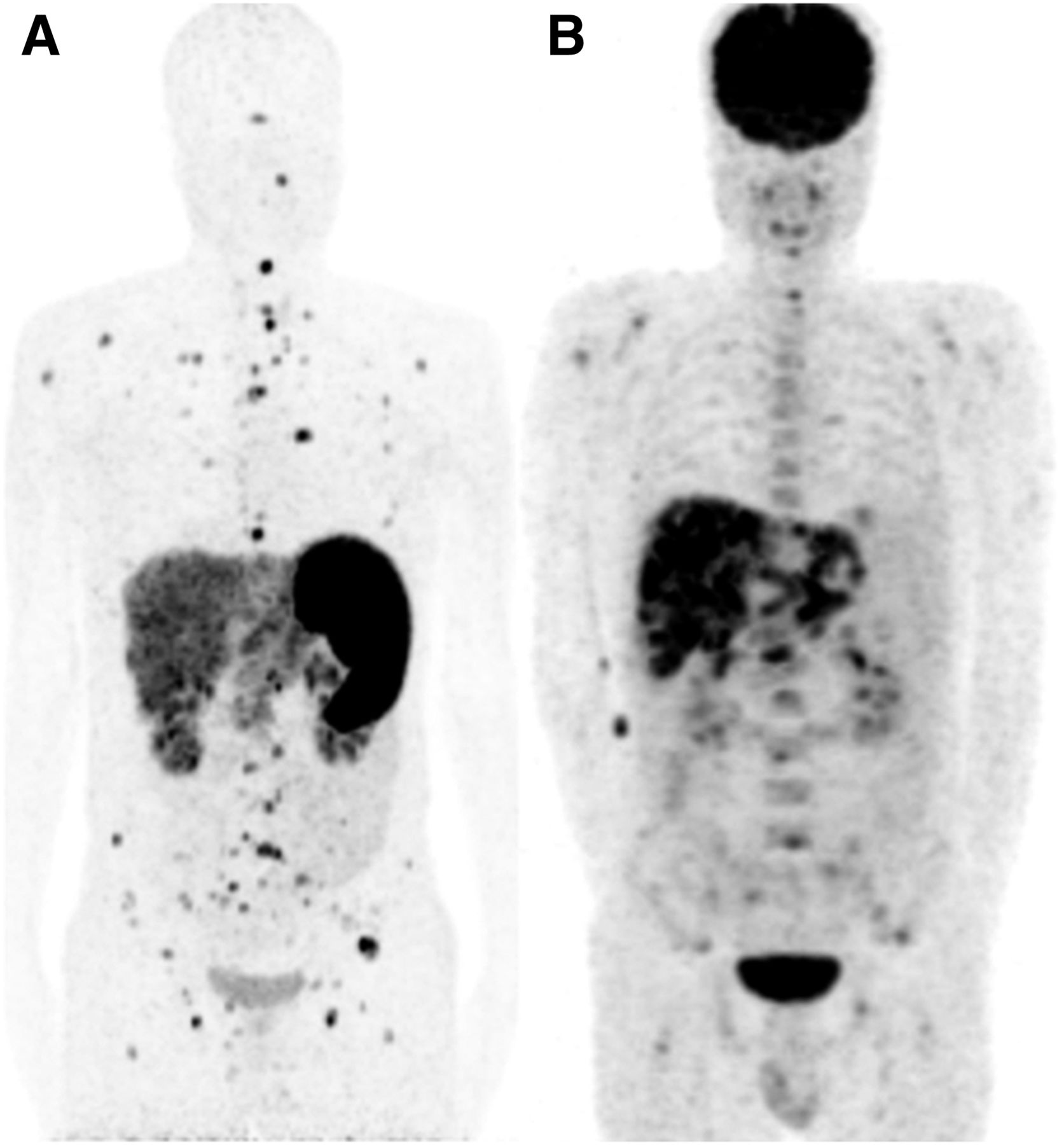
Maximum-intensity-projection images of high-grade (Ki67, 25%) pancreatic NET patient demonstrate multiple 18F-FDG(+) bone and liver metastasis (A); however, unexpectedly higher 68Ga-DOTATATE uptake (B) in metastatic lesions was mainstay of switching to PRRT.
The present study highlights the utility of the combined 68Ga-DOTATATE and 18F-FDG PET/CT in GEPNETs and, to our knowledge, includes the largest number of subjects with 68Ga-DOTATATE, 18F-FDG PET/CT, and Ki67 findings. The promising results with complementary PET/CT support the use of 18F-FDG PET/CT in addition to 68Ga-DOTATATE in the management of the patients with intermediate GEPNETs. On the other hand, high-grade NETs tend to have low-to-absent SSTR expression; thus, the use of 68Ga-DOTATATE in the management of high-grade GEPNETs is required to be confirmed in a larger cohort. Further studies are necessary to determine the impact of complementary PET/CT on high-grade GEPNETs.
CONCLUSION
Combined 68Ga-DOTATATE and 18F-FDG PET/CT is useful in the individual therapeutic approach of GEPNETs in clinically challenging intermediate-grade GEPNETs and may help resolve the limitations of the histopathologic grading. Further studies in a larger cohort can determine the potential benefits of the complementary PET/CT.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 13, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 1, 2014.
- Accepted for publication August 19, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Evaluating the Role of Theranostics in Grade 3 Neuroendocrine Neoplasms
- Imaging-Guided Use of Combined 177Lu-DOTATATE and Capecitabine Therapy in Metastatic Mediastinal Paraganglioma
- Most of the Intended Management Changes After 68Ga-DOTATATE PET/CT Are Implemented
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors
- 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis
- Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors