


Abstract
Planar ventilation–perfusion (V/Q) scanning is often used to investigate pulmonary embolism; however, it has well-recognized limitations. SPECT overcomes many of these through its ability to generate 3-dimensional imaging data. V/Q SPECT has higher sensitivity, specificity, and accuracy than planar imaging and a lower indeterminate rate. SPECT allows for new ways to display and analyze data, such as parametric V/Q ratio images. Compared with CT pulmonary angiography, SPECT has higher sensitivity, a lower radiation dose, fewer technically suboptimal studies, and no contrast-related complications. Any nuclear medicine department equipped with a modern hybrid scanner can now perform combined V/Q SPECT with CT (using low-dose protocols) to further enhance diagnostic accuracy. V/Q SPECT (with or without CT) has application in other pulmonary conditions and in research.
Since its first description by Wagner et al. in 1964 (1), the planar lung scan has been one of the most commonly performed studies in nuclear medicine. It is, however, a test with significant limitations, which have had an adverse impact on its reputation (2,3). Because planar imaging is a 2-dimensional technique, it has inherent limitations, especially related to overlap of anatomic segments. Assigning defects to specific lung segments is often difficult, and the variability in segment size and shape between patients makes accurate determination of the extent of embolic involvement in individual segments a challenge (2). Embolic defects may not be detected if there is shine-through from underlying lung segments with normal perfusion, thus resulting in an underestimation of the extent of perfusion loss (4). Furthermore, the medial basal segment of the right lower lobe is often not visualized on planar scans (2,5). Added to these factors is the widespread use of probabilistic reporting criteria, and a relatively high indeterminate rate, both of which have caused significant dissatisfaction among referring physicians (6,7). It is unsurprising that contrast-enhanced CT pulmonary angiography (CTPA), with its binary reporting approach (i.e., positive or negative), has now become the preferred imaging test to assess pulmonary embolism (PE) in many institutions, particularly in the United States (8,9).
ADVANTAGES OF SPECT OVER PLANAR IMAGING
Although SPECT is routinely used in many areas of nuclear medicine because of its ability to image in 3 dimensions, lung imaging remains a 2-dimensional technique in many institutions. SPECT imaging of the lungs avoids segmental overlap and shine-through of adjacent lung and can more accurately define the size and location of perfusion defects in individual segments (2).
Studies comparing planar and SPECT lung scanning have consistently demonstrated the superiority of SPECT over planar imaging. Studies on dogs (10) and pigs (11), as well as studies using Monte Carlo simulation (5), have all shown a higher sensitivity for the detection of PE with SPECT than with planar imaging. In humans, Bajc et al. found SPECT to be more sensitive than planar imaging (100% vs. 85%) in the detection of PE (12). SPECT had less interobserver variation and better delineation of mismatched defects than did planar imaging in this study. Collart et al. also demonstrated that SPECT was more specific than planar imaging (96% vs. 78%) and had better reproducibility, both intraobserver (94% vs. 91%) and interobserver (88% vs. 79%) (13). In a study of 83 patients, Reinartz et al. demonstrated that, compared with planar imaging, SPECT had a higher sensitivity (97% vs. 76%), specificity (91% vs. 85%), and accuracy (94% vs. 81%) (14). In this series, SPECT increased the detection of segmental defects by approximately 13% and subsegmental defects by over 80%. Based on pooled literature, SPECT has sensitivities ranging from 80% to 100% and specificities ranging from 93% to 100% (8). Ventilation–perfusion (V/Q) SPECT imaging has also been consistently shown to have a much lower indeterminate rate than planar imaging, typically less than 5% (8,15–19). Leblanc et al. demonstrated that SPECT has a very high negative predictive value (98.5%) for PE (20). In that study of 108 patients, only 3% of studies were considered to be indeterminate for PE.
The literature to date is quite consistent and, taken together, indicates that SPECT has a greater sensitivity and specificity, higher reproducibility, and lower indeterminate rate than planar lung scintigraphy.
V/Q SPECT
Technique
As with planar imaging, the usual approach with SPECT is to perform the ventilation study followed by the perfusion study.
For imaging of ventilation, several options exist. Inert radioactive gases such as 81mKr and 133Xe most accurately represent regional ventilation; however, these are used in only a limited number of centers because of the requirement for continuous administration during the acquisition and the high cost and short shelf-life of the 81mKr generator (21). Although 133Xe gas has the advantage of a longer half-life, it is a less than ideal choice because of recirculation, low γ-photon energy, and hence poor spatial resolution (21). Given these limitations, 99mTc-labeled particulate aerosols such as 99mTc-diethylenetriaminepentaacetic acid (99mTc-DTPA) or the ultrafine carbon–labeled nanoparticle 99mTc-Technegas (Cyclomedica) are much more widely used because of their greater availability, low cost, and good image quality (19). Technegas is an ideal agent for ventilation SPECT because of its small particle size (30–60 nm), resulting in greater alveolar penetration and less central deposition than a nebulizer-produced aqueous radioaerosol such as 99mTc-DTPA (22). However, in the United States (where Technegas is not commercially available, a factor that has significantly prevented the transition to SPECT (23)), there is little option but to use agents such as 99mTc-DTPA or 99mTc-sulfur colloid. Although 99mTc-DTPA image quality is adequate in many patients, Technegas is clearly superior in patients with obstructive lung disease because of its better peripheral penetration (24). The typical administered dose of 99mTc-based ventilation agents is 30–50 MBq, which is comparable to that used in planar imaging (14,17,20).
Perfusion is generally assessed using 99mTc-macroaggregated albumin (17). The dose of 99mTc-macroaggregated albumin is dependent on the ventilation agent and dose but is typically on the order of 100–250 MBq if a technetium-based ventilation agent is used. The European Association of Nuclear Medicine guidelines for V/Q SPECT recommend doses at the low end of this range, but ultimately the doses administered should be determined by each institution on the basis of the image quality obtained (which is influenced by factors such as collimator choice, γ-camera sensitivity, and processing parameters) and local radiation protection guidelines (25).
For pregnant patients, the administered dose is usually reduced by half for both the ventilation and the perfusion agents (25), thus requiring a longer acquisition so as to maintain images of good quality. Some centers advocate omitting the ventilation scan; however, the radiation savings from this approach are minimal and diagnostic accuracy may be adversely affected (26).
Image Acquisition, Processing, Display, and Reporting
Multidetector γ-cameras are preferred for V/Q SPECT (19). Generally, a total imaging time of 20–30 min is required to complete both the ventilation and the perfusion SPECT scans—less time than is required for traditional 6- or 8-view planar imaging (14,20). Typical acquisition and processing parameters are shown in Table 1. Images are best reviewed on a workstation using a dedicated software display package that allows automatic or manual image coregistration of ventilation and perfusion data and review of images in each of the orthogonal planes (27).
Typical Acquisition and Processing Parameters for V/Q SPECT*
For those reporting specialists familiar with planar images, these can be generated from SPECT data using several approaches. Although Bailey et al. have described a technique using reprojection (28), many of the commercial vendors offer a simpler approach using an angular summing technique (14). With this approach, images are generated by summing several consecutive projections from the SPECT acquisition. This approach can blur small defects because data are acquired over an arc; however, the images produced approximate true planar images (29). These pseudoplanar images give a familiar and rapid view of the lungs for quick evaluation and may be of particular value during the transition phase from planar imaging to SPECT imaging.
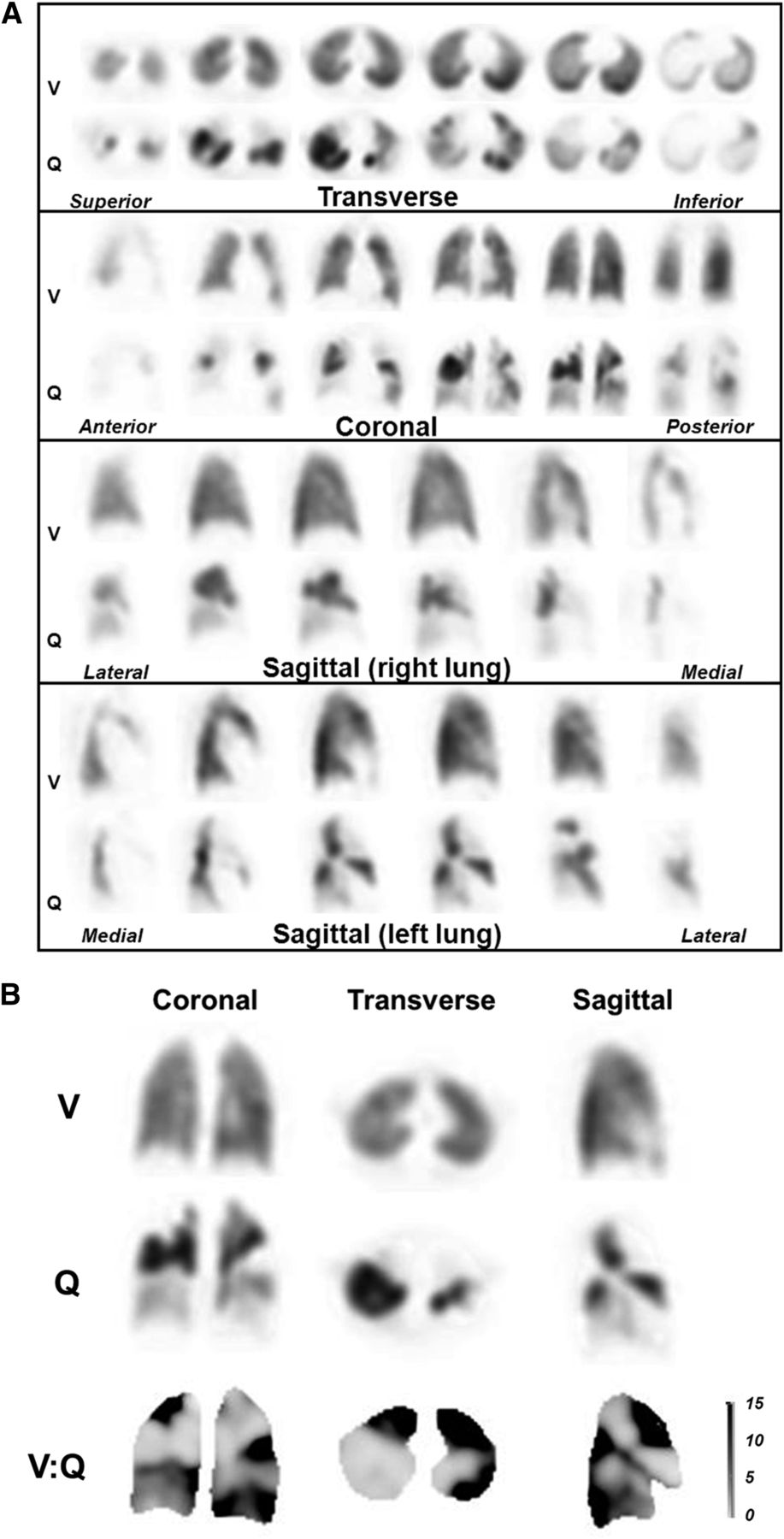
More advanced data processing can be performed with SPECT data. First, defect contrast on perfusion SPECT can be further enhanced by subtracting the background activity remaining from the preceding ventilation scan (12,30). Further, by examining the pixel-based V/Q ratio, quotient images can be generated from SPECT data. These images can facilitate image reporting and improve the demonstration of defect location and extent (Fig. 1) (30). Objective quantification of V/Q ratios is another processing technique that has been shown to increase accuracy and reduce the number of indeterminate studies (31,32).

(A). Example of patient with multiple bilateral PE. Ventilation and perfusion images show multiple mismatched perfusion defects. (B) Representative ventilation, perfusion, and V/Q quotient images. Dark areas on V/Q quotient images, denoting high V/Q ratio, are indicative of V/Q mismatch. (Reprinted with permission from (19).)
V/Q studies are usually reported using the European Association of Nuclear Medicine guidelines, which recommend that studies be reported as positive for PE if there is V/Q mismatch of at least 1 segment or 2 subsegments that conforms to the pulmonary vascular anatomy (17). Probabilistic reporting as used for planar scanning is not recommended, and has not been validated, for V/Q SPECT (14,33).
Comparison with CTPA
Multidetector CTPA has evolved to the point where it is frequently used as the primary imaging investigation in patients with potential PE (34). This is certainly the case in the United States, where it has supplanted the V/Q scan as the initial imaging test for the assessment of PE in many institutions (8,9). This preference has happened for many reasons, including better availability in many centers (especially after hours), rapid acquisition time, the ability to diagnose conditions other than PE that could be accounting for the patient’s symptoms, and referrer preference for binary reporting (8,9).
There are, however, some significant limitations that can affect the use of CTPA for the investigation of PE. First, several studies have shown that the sensitivity of CTPA is less than desirable (18,35). In the large PIOPED II study (Prospective Investigation of Pulmonary Embolism Diagnosis), the sensitivity of CTPA was 83% (78% when technically suboptimal studies were included) (35). Accuracy was particularly suboptimal if there was discordance between the scan results and clinical likelihood (a finding similar to that noted with planar V/Q scintigraphy in the original PIOPED study (36)). Second, technical artifacts can affect image quality. These are primarily related to poor contrast opacification of the pulmonary arteries, motion artifacts, and image noise related to the body habitus of some patients (37). Indeterminate rates due to technical factors have been estimated at between 5% and 11% (38,39). In pregnant patients, the rate is even higher, occurring in as many as one third of CTPA procedures, even with 64-slice CT scanners (40,41), and is thought to be attributable to increased pressure in the inferior vena cava during pregnancy. Third, complications can result from the use of intravenous contrast material. In the PIOPED 2 study, 22% of patients were excluded because of contrast allergy and impaired renal function (35). It has been reported that CTPA is complicated by some type of immediate contrast reaction in 3% (42) and contrast-induced nephropathy in 1%–3% of patients (43). Fourth, radiation exposure can be high from CT. The radiation dose to the breast from CTPA has been estimated at between 10 and 70 mSv, a particular concern in younger women (44,45). By comparison, the breast radiation dose from the V/Q scan is on the order of 0.3–1 mSv (46). CTPA has overall radiation doses on the order of 8–20 mSv, compared with approximately 2.5 mSv with V/Q SPECT (26), also making CTPA unsuitable for follow-up studies to monitor resolution of PE. Finally, there are some concerns related to the detection of incidental or unrelated findings. Although CTPA may diagnose alternate conditions in many patients (up to 33% in one series), these may not be the cause of patient symptoms (47). Investigation of these incidental findings can be expensive and results in additional radiation or contrast exposure and performance of invasive procedures for uncertain return (48). One study showed that only 3.2% of CTPA studies in patients with a low or intermediate pretest probability had a relevant alternate diagnosis that was not evident on the chest radiograph (49).
Overall, relatively few studies have directly compared SPECT V/Q and CTPA. Reinartz et al. showed that SPECT was more sensitive (97% vs. 86%) but less specific (91% vs. 98%) than 4-slice CTPA (14). Miles et al., in a study of 100 patients using 16-slice CTPA, also found the accuracy of each to be comparable. They noted that SPECT had fewer contraindications, a lower patient radiation dose, and fewer nondiagnostic findings (50). In a study of 81 patients, Gutte et al. found that V/Q SPECT had a higher sensitivity (97% compared with 68%) but a lower specificity (88% compared with 100%) than CTPA (16-slice) (18).
These head-to-head studies consistently demonstrate that SPECT has a higher sensitivity, that CTPA has a higher specificity, and that the overall accuracy of each modality is comparable. With each modality having its strengths and weaknesses (Table 2), the test selected for any individual patient should take into account patient factors (including age, sex, renal function, diabetes, and the presence of coexisting lung disease) and institutional factors (e.g., availability and local expertise).
Summary of Strengths and Limitations of CTPA, V/Q SPECT, and V/Q SPECT/CT
V/Q SPECT/CT
Although V/Q mismatch is the hallmark of PE, other conditions can cause this appearance (17). Furthermore, not all patients with PE have the classic V/Q mismatch pattern because some develop pulmonary infarction, resulting in matched defects (17). For these reasons, the chest radiograph appearances have been considered pivotal by many to aid in the interpretation of the V/Q scan, and the findings are often used to improve the accuracy and specificity of V/Q reporting (17,36,51).
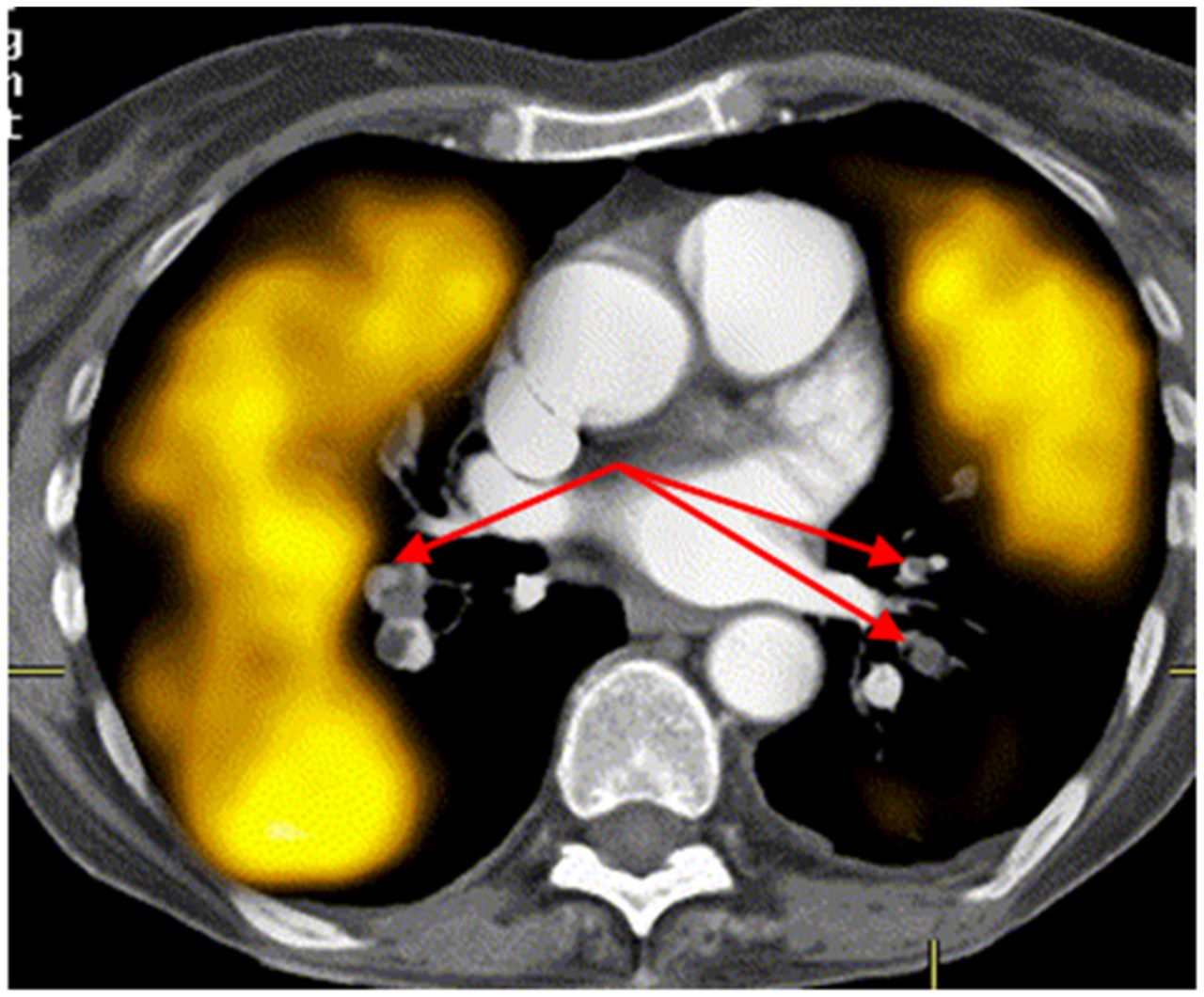
However, with the development of SPECT/CT scanners, the integration of anatomic information from the CT scan with the functional information from the SPECT scan is now feasible. By combining a V/Q SPECT study with a CT study, even one using “low-dose” settings to reduce patient radiation dose, the advantages of each modality can be realized. V/Q mismatch due to conditions other than PE (such as radiation therapy–induced changes, emphysema, and extrinsic vascular compression from conditions such as neoplasm or mediastinal adenopathy) can be detected by SPECT/CT imaging (Fig. 2) (17). Furthermore, SPECT/CT can help to characterize matched changes due to nonembolic etiologies such as pneumonia, abscess, pleural or pericardial effusions, malignancy, and pulmonary infarction (Fig. 3) (3,9,47). Hybrid SPECT/CT imaging therefore has the potential to increase the specificity of V/Q scanning by characterizing the causes of underlying perfusion defects (18,52). V/Q SPECT/CT offers the potential for a single imaging procedure yielding a high sensitivity and specificity for the detection of PE that has the added benefit of being able to identify various other conditions that can account for chest pain and dyspnea.

(A–D) False-positive V/Q scan due to emphysema. Mismatch is evident in right upper lobe (arrows), but CT (E) shows cause to be emphysematous bulla. R = right; A = anterior; L = left. (Reprinted with permission from (14).)

Representative SPECT/CT images in patient with colon cancer and dyspnea. SPECT shows matched defect in right lower lobe (arrows). CT shows this finding to correspond to previously undiagnosed metastasis.
Protocol, Processing, Display, and Reporting
Dual-detector hybrid SPECT/CT γ-cameras are now operational in many nuclear medicine departments. Although most devices can be used for diagnostic-quality CT, they can also be operated solely for attenuation correction and anatomic localization using “low-dose” parameters (52).
For lung scanning, the CT acquisition is typically obtained immediately after the perfusion SPECT acquisition. Intravenous contrast material is not required, and a reduced beam current, typically on the order of 20–80 mA, will suffice. The resulting radiation dose is on the order of 1–2 mSv (18,26), comparing favorably with the 2–2.5 mSv from the V/Q scan itself and well below the levels received from diagnostic CTPA (26,45,53). The CT acquisition is rapid (<1 min) and, combined with the set-up time, adds only a couple of minutes to a V/Q SPECT study. Although typically used for diagnostic CT studies, breath-holding is not feasible with V/Q SPECT because of the prolonged SPECT acquisitions. To reduce respiratory-motion misregistration, it has been recommended that CT scans be acquired during breath-holding at mid-inspiration volume, or with the patient continuing shallow breathing during the CT acquisition (54).
As with V/Q SPECT, the European Association of Nuclear Medicine guidelines are recommended for reporting V/Q SPECT/CT studies. Although these guidelines do not specifically address hybrid imaging, the addition of the CT component is likely to help classify the V/Q SPECT pattern more appropriately. The CT scan will provide patient-specific anatomic information, including the lung and segment borders, fissures, and major vessel locations and the presence of any associated parenchymal disease (Fig. 4). The location of the fissures should be noted, as a linear reduction in perfusion (and to a lesser degree ventilation) corresponding to the fissures can be seen on SPECT imaging. The location of any matched changes should also be noted, as consolidative opacities secondary to PE preferentially occur peripherally whereas lesions induced by inflammatory disease tend to be seen at the proximal portion of defects (55).

Representative SPECT/CT images in patient with multiple PE. Several mismatched defects are evident (arrows). CT shows no underlying structural abnormalities.
Clinical Value
Several studies have shown that combined SPECT/CT lung scanning improves the specificity and overall diagnostic accuracy of lung scintigraphy.
Herald et al. demonstrated a 50% reduction in false-positive V/Q SPECT studies in a study of 48 patients where SPECT was combined with a low-dose (30–50 mAs) CT scan (56).
A larger prospective study from Gutte et al. demonstrated high diagnostic accuracy when V/Q SPECT was combined with low-dose CT (18). In a series of 81 consecutive patients with 81mKr gas used as the ventilation agent, V/Q SPECT/CT had an identical sensitivity to V/Q SPECT (97%). However, the addition of low-dose CT imaging demonstrated that mismatched perfusion defects could be attributed to structures such as fissures and to pathologic conditions such as emphysema, pneumonia, atelectasis, and pleural fluid. As a result, the specificity of scintigraphy increased from 88% to 100%. The inconclusive rate for V/Q SPECT/CT was zero (compared with 5% for V/Q SPECT alone). To our knowledge, this study has been the only direct comparison of CTPA (16-slice) with V/Q SPECT/CT (18). Although CTPA had a high specificity (100%, identical to that reported for V/Q SPECT/CT), it had a sensitivity much lower than either SPECT or SPECT/CT (68% compared with 97%).
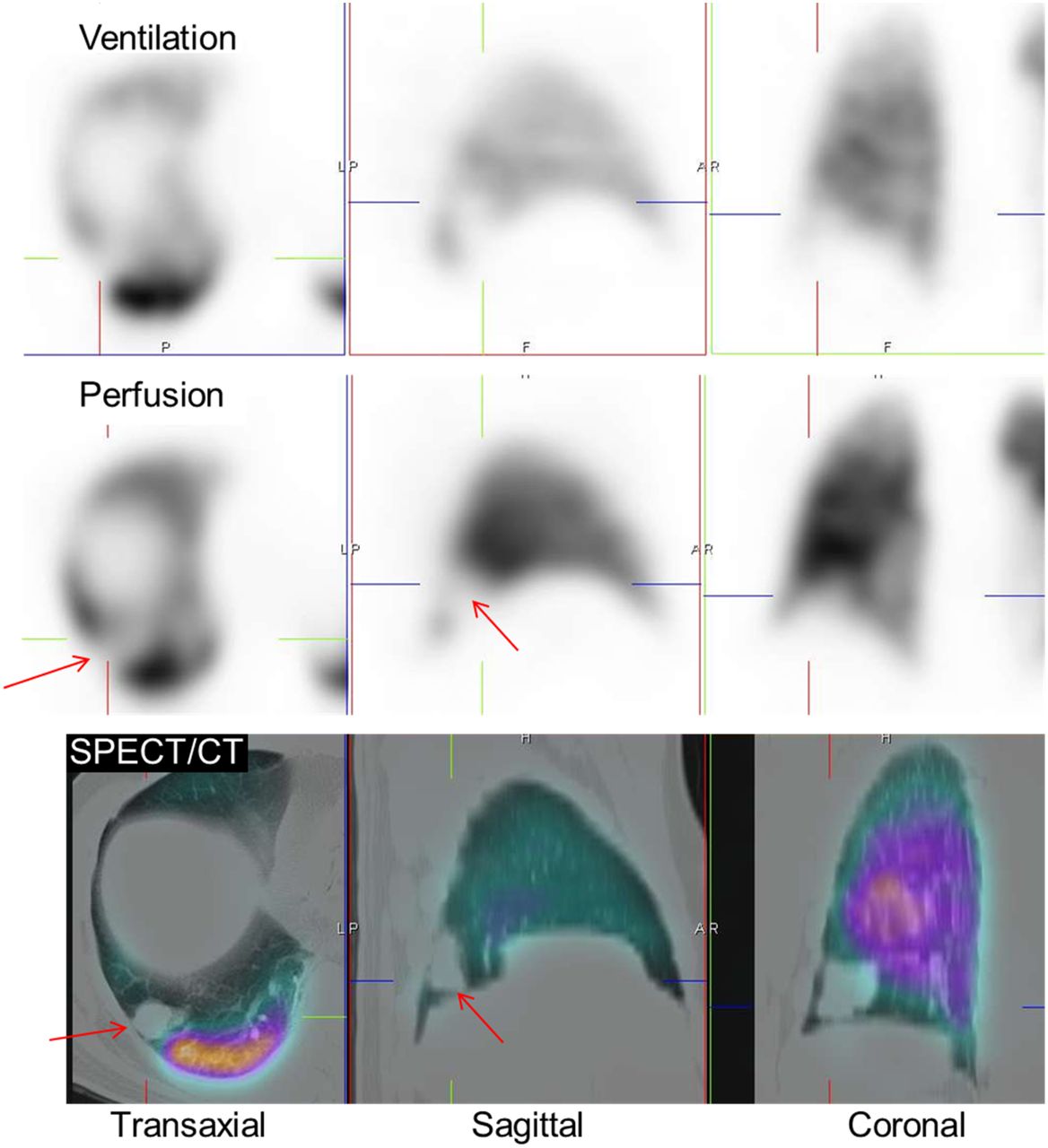
Another benefit of SPECT/CT imaging is the ability to more accurately localize perfusion defects to the correct segments in each individual patient. The segmental reference lung maps that are used to guide SPECT reporting may be erroneous because of the distortion of individual anatomy caused by other lung conditions, such as atelectasis and pleural effusions, which often coexist in patients with PE (Fig. 5) (52,57). This information may be relevant to help guide a reporting radiologist to the correct segmental artery should CTPA be required to confirm the findings on a V/Q SPECT study.
Sagittal (left) and transaxial (right) perfusion, CTPA, and fused slices in patient with PE and lower lobe volume loss due to atelectasis. Although defect (red crosshairs) was initially localized to superior segment of right lower lobe, fusion accurately localizes defect to posterior segment of right upper lobe. (Reprinted with permission from (52).)
Combining V/Q SPECT with CTPA
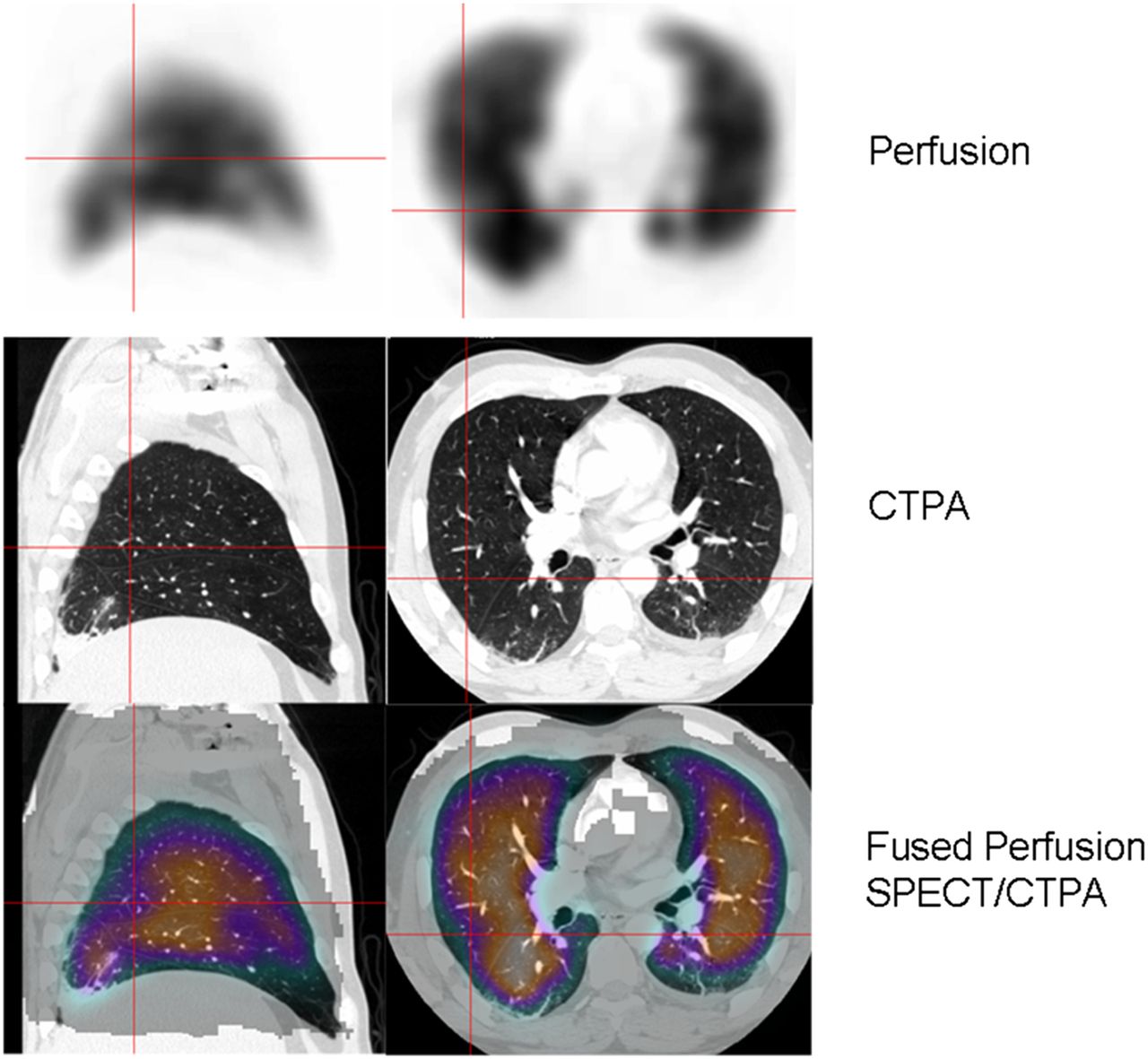
Another option for combining structural and functional images is to fuse perfusion SPECT with diagnostic CTPA, performed on either the same hybrid scanner or another CT scanner using software fusion (Fig. 6) (58). Although requiring appropriate software programs and operator expertise, this approach can be of value in selected patients and may better guide the reporting radiologist to the site of a likely clot on CTPA (59).

Coregistered CTPA and perfusion SPECT scans (transverse slice) demonstrating extensive perfusion defects on SPECT. Findings correspond to proximal bilateral PE shown on CTPA (arrows) (Reprinted with permission from (52).)
CONTROVERSIES
Is the Ventilation Scan Necessary?
With SPECT/CT able to show structural abnormalities, the need for a ventilation study has been questioned. Several studies have demonstrated that specificity falls significantly if ventilation is omitted. Gradinscak et al. showed that parenchymal abnormalities (usually subsegmental atelectasis) were noted on CT in 13% of V/Q SPECT mismatches (60), and Gutte et al. demonstrated that perfusion-only SPECT/CT has a higher nondiagnostic rate (17%) and lower specificity than V/Q SPECT/CT (51% compared with 100%) (18). Although perfusion-only SPECT/CT should be considered in sites without access to a suitable ventilation agent, limited literature suggests that performing a ventilation study does maximize specificity and reduce false-positive results.
Do Additional Clots Detected by SPECT Warrant Treatment?
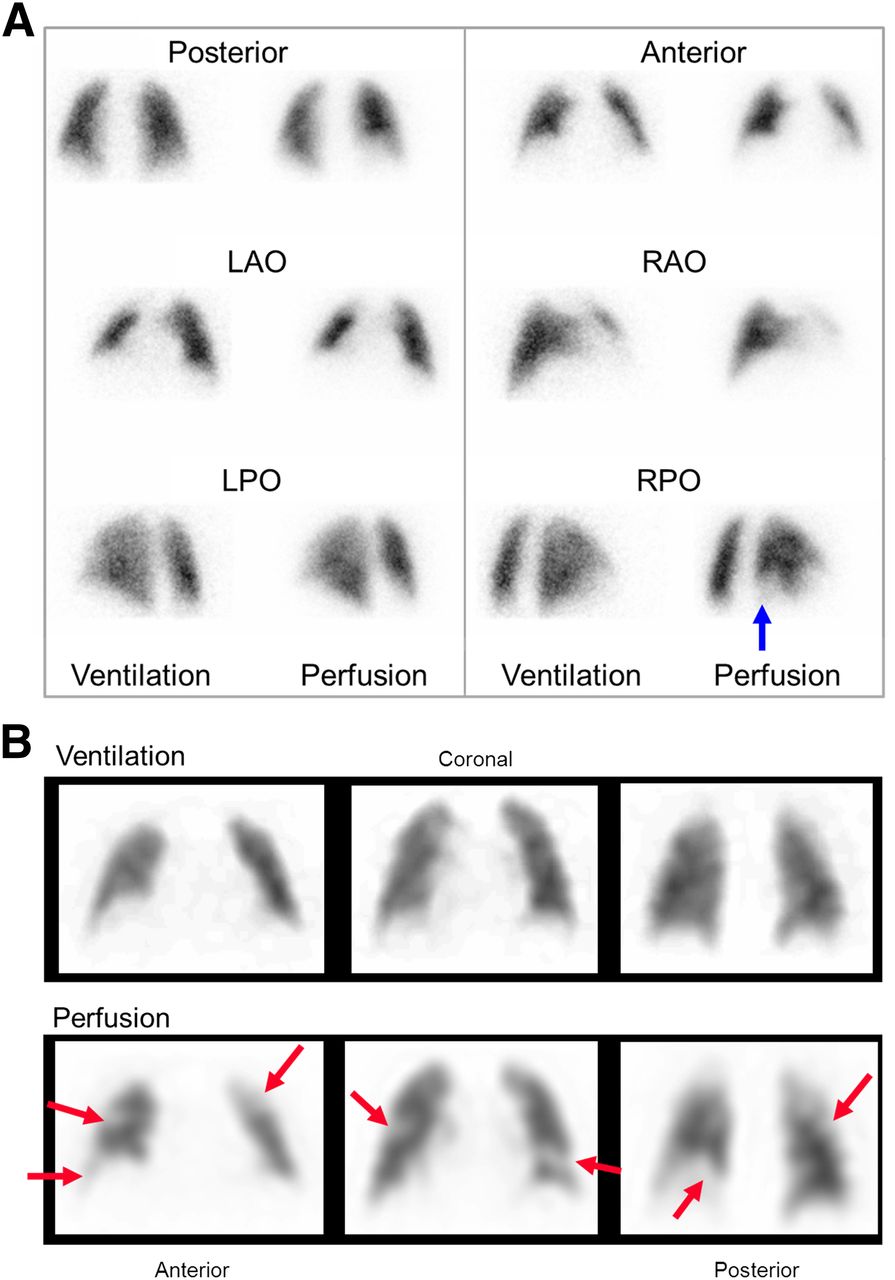
Although V/Q SPECT (and SPECT/CT) has a higher sensitivity than planar imaging, the question has been raised as to whether these clots (which are often subsegmental) are significant enough to warrant anticoagulation (3,23,53,61). Although large prospective outcome studies would be needed to answer this question (and would be welcomed), it is our experience (and that of others) that SPECT detects additional PE not just at the subsegmental level (Fig. 7) (14). Diagnosis of any PE, including small ones, may be of particular importance in patients with impaired cardiopulmonary reserve, coexisting DVT, or recurrent small PE (with its risk of pulmonary hypertension) (62). Although this consideration raises the broader philosophic question as to whether diagnostic accuracy or clinical outcome is more relevant, we consider that the higher sensitivity and accuracy, improved reader confidence, greater ease of reporting, and ability to perform hybrid SPECT/CT imaging are all compelling reasons to replace planar imaging with SPECT for imaging PE.

(A) Planar V/Q scan in patient with dyspnea. Single mismatched defect is seen at right base (arrow), classifying study as intermediate probability of PE. (B) Representative coronal SPECT slices show multiple mismatched defects (arrows) indicative of widespread PE. Patient had extensive deep venous thrombosis.
NON-PE APPLICATIONS AND FUTURE DIRECTIONS
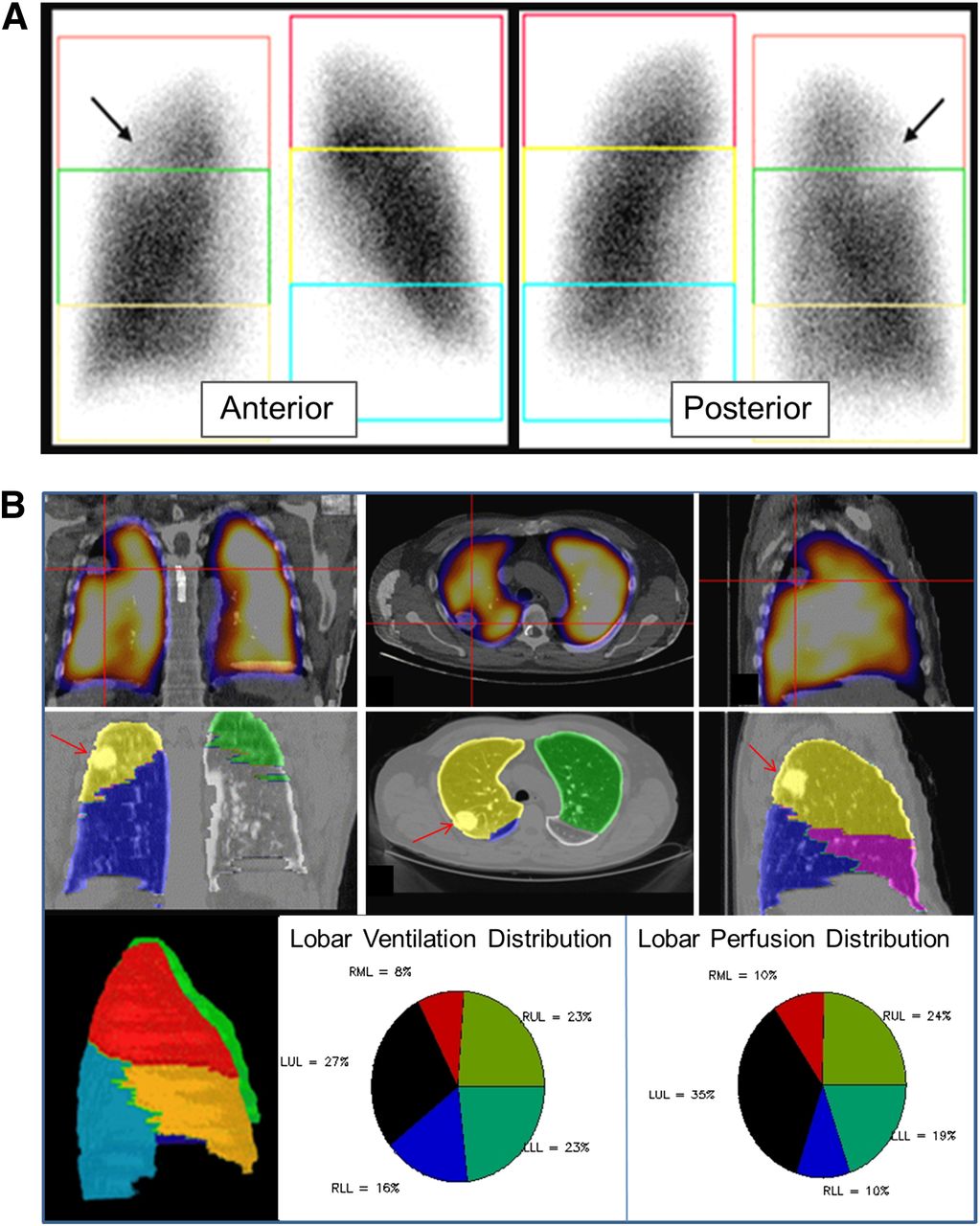
V/Q SPECT and SPECT/CT have utility in areas other than PE. In patients undergoing lung volume reduction surgery, SPECT/CT can provide a more accurate assessment of relative perfusion (and ventilation) of individual segments than planar imaging (Fig. 8). V/Q SPECT has been shown to have use in areas such as predicting postoperative lung function after lung resection in patients with lung cancer, modifying radiotherapy fields to minimize radiation exposure to functioning lung, demonstrating regional changes of ventilation and perfusion in asthma, and estimating regional lung function in patients with interstitial pulmonary disease (63–65).
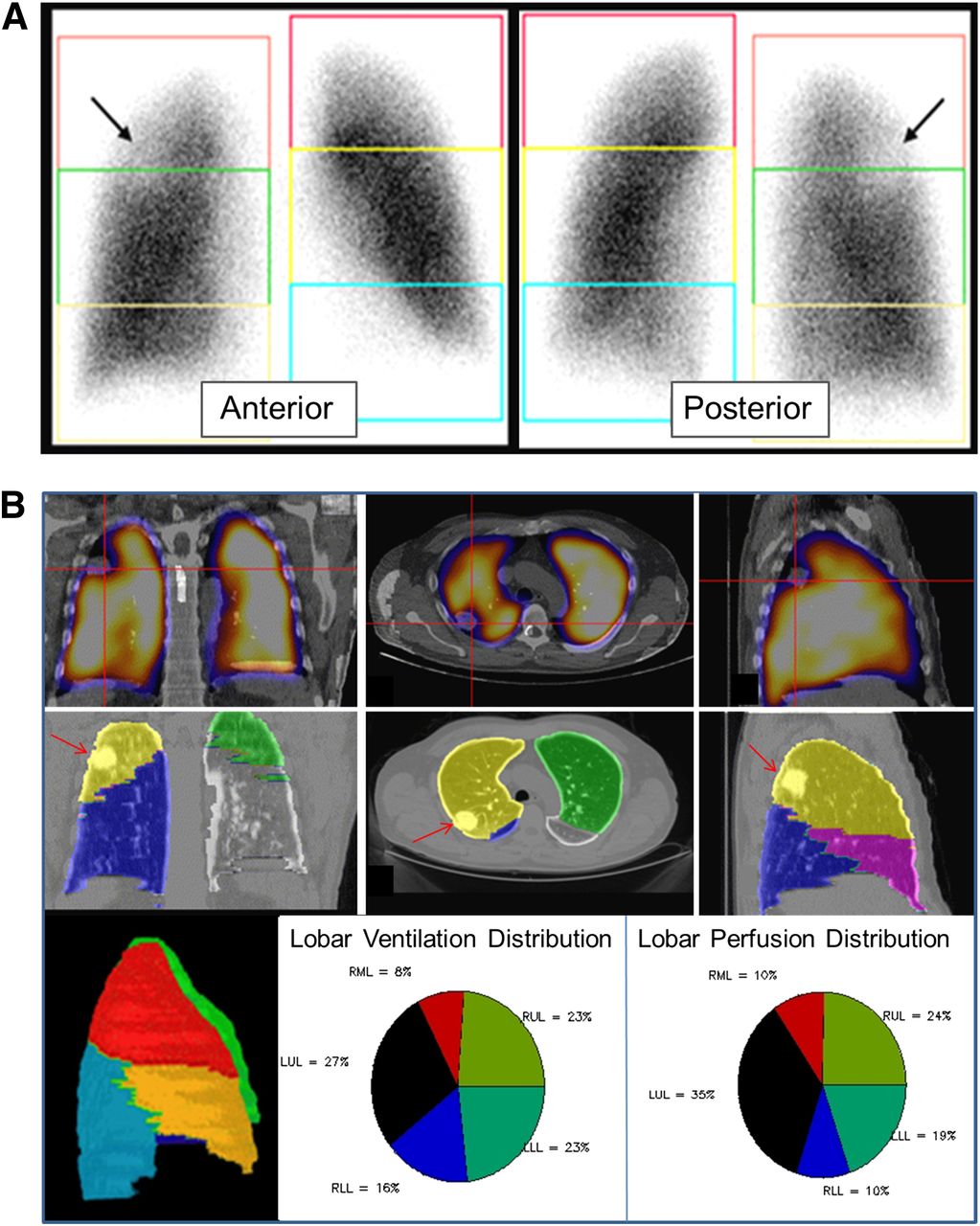
(A) Anterior (left) and posterior (right) planar images in patient with right lung carcinoma (arrows). Boxes over upper, middle, and lower thirds of each lung approximate relative contribution of each region. Because of overlap of segments and differences in individual anatomy, accuracy is lacking. (B) Fused perfusion/CT images (top row) in coronal (left), transverse (middle), and sagittal (right) planes show perfusion defect (due to tumor, denoted with red crosshairs) in right upper lobe. Patient’s individual CT scan can be used to generate patient-specific lobar slices (middle row) in corresponding orthogonal slices and rotating maximum-intensity-projection images (left image, bottom row). SPECT/CT allowed accurate determination of each lobe’s relative contribution to overall ventilation (middle image, bottom row) and perfusion (right image, bottom row). LLL = left lower lobe; LUL = left upper lobe; RLL = right lower lobe; RML = right middle lobe; RUL = right upper lobe.
Future directions for SPECT/CT are likely to include radiolabeled thrombus imaging of PE (66). Quantitative SPECT will benefit from hybrid imaging through derivation of accurate patient-specific attenuation correction (34). Lung scanning using PET radiopharmaceuticals, such as 68Ga-carbon nanoparticles (“Galligas”) and 68Ga-macroaggregated albumin, is a promising development that may further enhance the role of nuclear medicine in the assessment of PE and other lung disorders (49).
CONCLUSION
As with other areas of nuclear medicine, V/Q scanning has been improved significantly with SPECT imaging. V/Q SPECT has a higher sensitivity and specificity than planar imaging, as well as reduced interobserver variability, increased overall accuracy, and improved reporter confidence. The low rate of technically adequate studies, absence of contrast-related risks, and higher sensitivity and lower radiation dose than CTPA are all arguments supporting the use of V/Q SPECT as the initial screening test for PE in most patients (33,41). Specificity is further enhanced by V/Q SPECT/CT, which provides the potential for a single imaging procedure to assess PE with high accuracy while also excluding various alternative causes of chest pain and dyspnea.
Footnotes
Published online Aug. 1, 2013.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) advantages and shortcomings of planar versus SPECT V/Q scanning, (2) advantages and disadvantages of CT pulmonary angiography versus V/Q SPECT in the investigation of pulmonary embolism, and (3) an overview of image acquisition, processing, display, and reporting of V/Q SPECT studies.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, participants can access this activity through the SNMMI Web site (http://www.snmmi.org/ce_online) through September 2016.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 30, 2013.
- Accepted for publication June 28, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pulmonary embolism
- V/Q SPECT and SPECT/CT in Pulmonary Embolism
- A Technical Overview of Technegas as a Lung Ventilation Agent
- Imaging of pulmonary hypertension in adults: a position paper from the Fleischner Society
- The effects of lung volume reduction treatment on diffusing capacity and gas exchange
- Nuclear Medicine Clinical Practice in the United States During the COVID-19 Era and Beyond
- Pulmonary Arterial Hypertension With Abnormal V/Q Single-Photon Emission Computed Tomography
- The Importance of Quality in Ventilation-Perfusion Imaging
- SPECT V/Q for the diagnosis of pulmonary embolism: protocol for a systematic review and meta-analysis of diagnostic accuracy and clinical outcome
- Correlation of 68Ga Ventilation-Perfusion PET/CT with Pulmonary Function Test Indices for Assessing Lung Function
- Pulmonary Scintigraphy for the Diagnosis of Acute Pulmonary Embolism: A Survey of Current Practices in Australia, Canada, and France