


Abstract
We evaluated (−)-2-(6-[18F]fluoro-2,3′-bipyridin-5′-yl)-7-methyl-7-aza-bicyclo[2.2.1]heptane (18F-AZAN), a novel radiotracer that binds to α4β2 nicotinic acetylcholine receptors (α4β2-nAChRs) and shows high specific binding and rapid and reversible kinetics in the baboon and human brain. Methods: We tested safety tolerability and test–retest reliability (n = 5) and proposed initial quantification of 18F-AZAN receptors in 3 healthy human subjects who had nicotine exposure and 9 who did not. We also present a receptor blocking study in a nicotine subject dosed with the α4β2-nAChR–selective partial agonist varenicline. Results: Radiation dosimetry PET/CT experiments indicated that most human organs received doses between 0.008 and 0.015 mSv/MBq, with an effective dose of approximately 0.014 mSv/MBq. The tracer rapidly entered the brain, and the peak was reached before 20 min, even for thalamus. Ninety-minute scans were sufficient for 18F-AZAN to obtain the ratio at equilibrium of specifically bound radioligand to nondisplaceable radioligand in tissue (BPND) using plasma reference graphical analysis, which showed excellent reproducibility of BPND (test–retest variability < 10%) in the nAChR-rich brain regions. Regional plasma reference graphical analysis BPND values exceeded 2 in the midbrain tegmental nuclei, lateral geniculate body, and thalamus for nonsmokers (n = 9) but were less than 1 in the nAChR-poor brain regions. There was a dramatic reduction of 18F-AZAN brain uptake in smokers and varenicline-treated subjects. Conclusion: 18F-AZAN is a highly specific, safe, and effective PET radioligand for human subjects that requires only 90 min of PET scanning to estimate high-affinity α4β2-nAChR in the living human brain.
Nicotinic acetylcholine receptors (nAChRs) are associated with several disorders involving alteration of the density of the receptor in the central nervous system, such as Alzheimer and Parkinson diseases, schizophrenia, attention deficit hyperactivity disorder, autosomal dominant nocturnal frontal lobe epilepsy, and tobacco dependence (1–5).
The α4β2-nAChR is the most prominent subtype of nicotinic acetylcholine receptors in mammalian brain, with the highest density of this receptor being in the thalamus, an intermediate density in the cortical regions and caudate, and the lowest density in the cerebellum (1,6). Available radioligands for the quantitative PET imaging of nAChR in humans, 2-18F-fluoro-3-(2(S)-azetidinylmethoxy)pyridine (2-18F-FA) (7) and 6-18F-fluoro-3-(2(S)-azetidinylmethoxy)pyridine (6-18F-FA), exhibit slow distribution kinetics in primates, requiring hours of scanning (3,8–15). Even the bolus-plus-infusion approach, which allows a shorter scanning time, does not resolve the problem completely because of the long postinjection waiting period of more than 6 h (16). As a result, imaging of nAChR is logistically difficult for researchers and patients.
In contrast, we recently presented a substantially improved α4β2-nAChR radiotracer, (−)-2-(6-[18F]fluoro-2,3′-bipyridin-5′-yl)-7-methyl-7-aza-bicyclo[2.2.1]heptane (18F-AZAN), showing high specific uptake in the mouse brain (17) and high specific binding and rapid and reversible kinetics in the baboon brain (18). In the current study, we validated the PET properties of 18F-AZAN in the human brain. Specifically, we tested whether it allows a shorter scan time (<90 min) than alternatives; whether the desired variable (the ratio at equilibrium of specifically bound radioligand to nondisplaceable radioligand in tissue [BPND] (19)) is accessible, has acceptable values, and is reproducible in a test–retest paradigm; and whether binding is displaced by nicotine and an α4β2-nAChR–selective partial agonist, varenicline.
MATERIALS AND METHODS
This was a single-center, open-label, nonrandomized study. The study received human subject protection approval from the Johns Hopkins School of Medicine Institutional Review Board and was conducted under a U.S. investigational new drug application after appropriate animal toxicology studies of the unlabeled ligand and radiation dosimetry. All participants provided written, informed consent.
Preparation of 18F-AZAN
18F-AZAN was prepared as described in the literature (17,18). 18F-AZAN was formulated as a sterile and pyrogen-free solution in saline with 8% ethanol at a pH of 5.5–6.5, with radiochemical purity greater than 99% and specific radioactivity in the range of 277–1,591 GBq/μmol (7,500–43,000 mCi/µmol) at the time synthesis ended.
Whole-Body Dosimetry
Data from mouse whole-body dissection studies provided an initial estimate of the overall safety of administration of 18F-AZAN, and estimates of the whole-body and internal organ radiation of absorbed doses for retest injections were taken from the first (test) injection. Male CD-1 mice weighing 25–30 g from Charles River Laboratories were used for biodistribution studies. The animals (n = 3 per time point) were sacrificed by cervical dislocation at 5, 15, 30, 60, 120, and 240 min after injection of 18F-AZAN (∼2.8 MBq [75 μCi]; specific radioactivity, ∼370 GBq/μmol [10,000 mCi/μmol], in 0.2 mL of saline) into a lateral tail vein. The organs were rapidly removed and dissected on ice. For the bladder assay, the external urethral meatus was tied off under ether anesthesia. The organs of interest were weighed and their radioactivity content was determined in an automated γ-counter with a counting error below 3%. Aliquots of the injectate were prepared as standards and their radioactivity content was counted along with the tissue samples. The percentage injected dose per gram of tissue was calculated, and time–activity curves for various organs were generated. The estimates of human absorbed radiation dose per organ and total dose-equivalents were calculated using OLINDA/EXM software (20). All experimental protocols were approved by the Animal Care and Use Committee of the Johns Hopkins Medical Institutions.
Distributions of the radioactivity in the human body were determined for 2 male subjects. After a CT scan, participants had a multiple-bed-position PET scan with a Discovery PET/CT scanner (GE Healthcare) at 4 time points over 90 min after a bolus injection of 18F-AZAN. Time–activity curves of organs were submitted to OLINDA/EXM software (20) to obtain the radiation dose estimates for human organs. This information, along with the physiologic monitoring, allowed the complete safety of 18F-AZAN administration to be assessed.
Human Brain Study
Subjects
Six men (age, 47.5 ± 7.9 y [mean ± SD]) and 9 women (37.4 ± 10.7 y) participated in the brain study. Subjects were confirmed to be nonsmoking by self-report, drug-free by urinary tests, and physically and mentally healthy by history and physical examination on the day of the scan. Six subjects (3 male and 3 female) participated in test–retest scans, about 1 mo apart. Of 8 subjects who had a single scan, 1 subject had nicotine gum on the day of the scan, 2 subjects disclosed after the scan that they had been exposed to second-hand smoke the night before the scan, and 1 subject was treated with an α4β2-nAChR–selective partial agonist, varenicline, for 12 d before the scan (days 1–3, 0.5 mg/d; days 4–7, 0.5 mg twice per day; days 8–12, 1 mg twice per day).
PET Experiments
PET studies were performed on a High-Resolution Research Tomograph (CPS Innovations, Inc.), with a spatial resolution of 2.5 mm in full width at half maximum (21). The subjects had a venous catheter for the radioligand injection and an arterial catheter to obtain arterial blood samples for the determination of radioactivity in plasma. Subjects were positioned in the scanner with their heads restrained with a custom-made thermoplastic mask to reduce head motion during the PET data acquisition. A 6-min transmission scan was acquired using a rotating 137Cs source for attenuation correction. A dynamic PET acquisition was then performed in a 3-dimensional list mode for 90 min after an intravenous bolus injection of 18F-AZAN. Radial arterial blood samples were collected at short intervals (<5 s) initially and at gradually prolonged intervals throughout the PET study. Selected blood samples taken at 0, 5, 10, 20, 30, 60, and 90 min were analyzed by high-performance liquid chromatography (HPLC) for the presence of 18F-AZAN and its radioactive metabolites (17,18).
Reconstruction
Emission PET scans were reconstructed using the iterative ordered-subset expectation-maximization algorithm corrected for attenuation, scatter, and dead time (22). The radioactivity was corrected for physical decay to the injection time and rebinned to 30 dynamic PET frames of 256 (left-to-right) by 256 (nasion-to-inion) by 207 (neck-to-cranium) voxels. The schedule was four 15-s, four 30-s, three 1-min, two 2-min, five 4-min, and twelve 5-min frames. The final spatial resolution is expected to be less than 2.5 mm in full width at half maximum in 3 directions (21).
MR Imaging
A 3-dimensional magnetization-prepared rapid gradient echo sequence MR image of each subject was obtained for anatomic identification of the structures of interest using the following parameters: repetition time, 2,110 ms; echo time, 2.73 ms; flip angle, 8; slice thickness, 0.80 mm with zero gap; field of view, 24 × 18 cm2; and image acquisition matrix, 288 × 320.
Volumes of Interest
Cortical volumes of interest were automatically defined using Freesurfer software (http://surfer.nmr.mgh.harvard.edu (23)) and combined into standard regions including frontal, temporal, parietal, and occipital cortices, fusiform gyrus, cingulate, and insula. Subcortical regions were defined with FIRST software (http://www.fmrib.ox.ac.uk/fsl (24)) and manually adjusted on individual MR images. Subcortical regions included putamen, caudate nucleus, globus pallidus, thalamus, hippocampus, and amygdala. Volumes of interest were transferred from MR imaging to PET spaces following MR imaging–to–PET coregistration parameters given by SPM5 (25) to obtain time–activity curves of regions.
Derivation of PET Outcome Variables
A set of standard plasma input methods was used to identify the optimal method for derivation of the total volume of distribution (VT) for 18F-AZAN. The following 4 methods were tested: a 1-tissue-compartment model with 3 parameters (K1 and k2′ (19) and v0 [tissue vascular volume]), 2-tissue-compartment models (TTCMs) with 5 parameters (K1, k2, k3, k4 (19), and v0) without and with constraining the K1/k2 ratio (nondisplaceable distribution volume, VND (19), to the cerebellum estimate [TTCM-C]), and the plasma reference graphical analysis (PRGA (26)). In TTCM and TTCM-C, BPND was given as the k3/k4 ratio. The Akaike information criterion was used to select the method that showed the lowest Akaike information criterion values among the 1-tissue-compartment model, TTCM, and TTCM-C. Metabolite-corrected plasma time–activity curves were obtained by applying percentage parent ligand time-profiles given by HPLC analysis to total plasma time–activity curves, after using interpolation (piecewise cubic Hermite) in Matlab (MathWorks).
To visually confirm regional differences in BPND in control subjects, and displacement of 18F-AZAN binding in subjects with nicotine-exposure history and varenicline treatment, BPND maps were generated by applying PRGA on voxels, spatially normalized using parameters of PET-to-MR imaging coregistration (25) and MR imaging-to-standard MR imaging spatial normalization (SPM unified segmentation method (25)), and averaged across members.
Test–Retest Variability (TRV)
TRV of VT and BPND was calculated using the following equation (expressed as a percentage) to estimate the reproducibility of the PET outcome variables in individual regions:
RESULTS
Whole-Body Dosimetry
In the mouse dosimetry studies, most organs received about 0.007–0.03 mSv/MBq (Table 1). The urinary bladder received the highest dose, about 0.2 mSv/MBq. This was likely an overestimate because of the procedure of bladder instrumentation. The human bladder dosimetry is the most appropriate. The effective dose was about 0.03 mSv/MBq. In the human dosimetry studies, the 18F-AZAN dose for the 2 participants was 168.2 ± 20 MBq (4.55 ± 0.54 mCi), specific radioactivity was 851 ± 518 GBq/μmol (23 ± 14 Ci/μmol), mass dose was 0.07 ± 0.05 μg, and mass dose per kilogram was 0.8 ± 0.7 ng/kg. Most organs (Table 2) appeared to receive around 0.008–0.015 mSv/MBq (0.032–0.055 rem/mCi). The urinary bladder received the highest dose, around 0.023 mSv/MBq (0.085 rem/mCi). The effective dose was about 0.014 mSv/MBq (0.052 rem/mCi).
Human Radiation Dose Estimates (Adult Male Model) from CD1 Mouse Distribution Study
Human Radiation Doses (2 Men, Whole-Body PET/CT)
Human Brain Study
Three scans were eliminated from data analysis due to scanner (n = 1) or HPLC-related (n = 2) problems. Thus, method evaluation was performed on 18 scans from 13 subjects, test–retest evaluation was done on 5 subjects, and regional VT and BPND values were obtained on 9 control (14 scans), 3 nicotine-exposed, and 1 varenicline-treated subjects.
Tissue and Plasma Time–Activity Curves
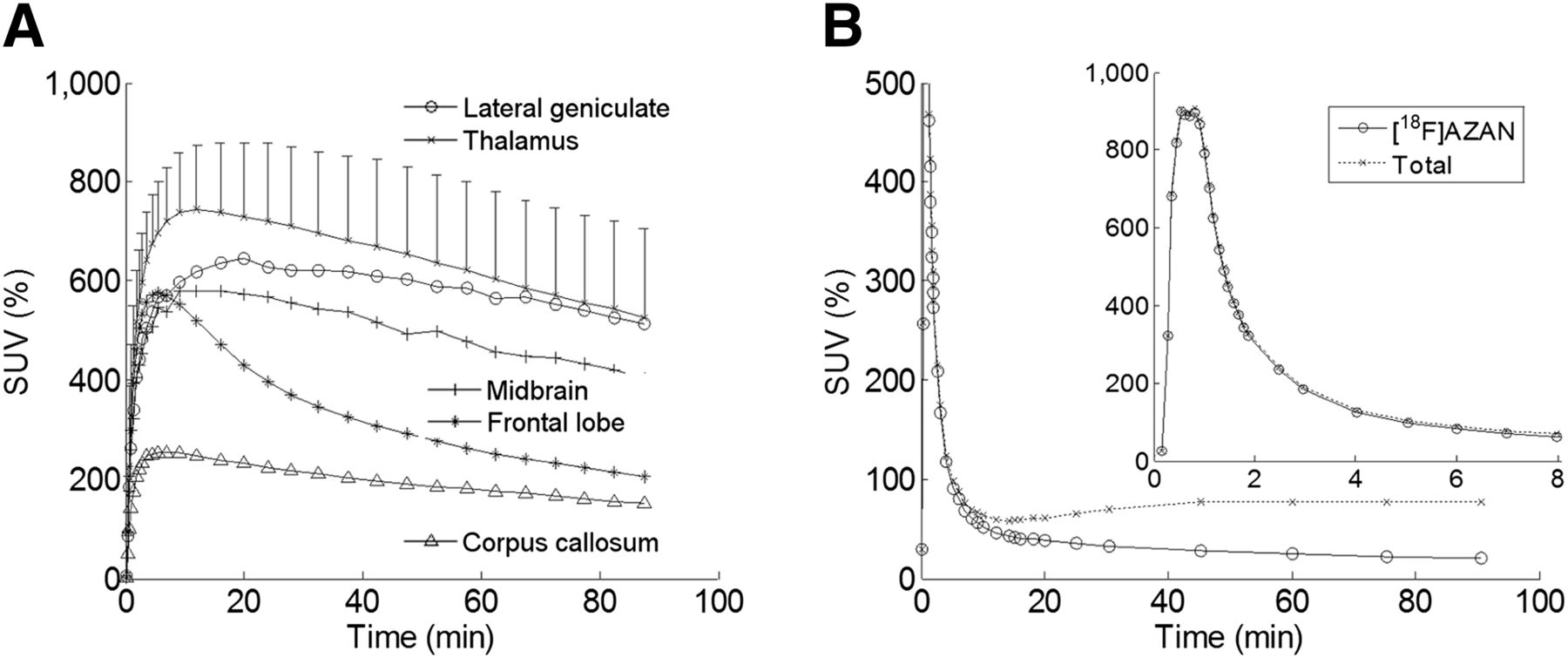
Injected doses of 18F-AZAN ranged from 186 to 599 MBq (5.03–16.19 mCi), with specific radioactivity ranging from 128 to 1,138 GBq/μmol (3.46–30.77 Ci/μmol). Time–activity curves of selected brain regions are shown in Figure 1, expressed as average percentage standardized uptake value across subjects without a recent history of nicotine exposure. Thalamus time–activity curves peaked before 20 min after injection and then decreased monotonically. The lateral geniculate body and midbrain tegmentum nucleus, 2 regions of high uptake, showed slightly slower uptake than did the thalamus. Other cortical and subcortical regions showed rapid uptake (peaked before 10 min) and clearance, as exemplified by frontal cortex in Figure 1A. The corpus callosum showed lower accumulation of the radioactivity than did gray matter structures characterized by slow uptake and clearance. Total and metabolite-corrected plasma time–activity curves are shown as percentage standardized uptake value in Figure 1B. Total radioactive metabolites averaged (±SD) 4.4% ± 4.4% at 5 min, 24.9% ± 9.1% at 15 min, 48.4% ± 9.3% at 30 min, 64.3% ± 8.7% at 60 min, and 70.2% ± 8.5% at 90 min.

(A) Plots of time–activity curves of selected brain regions after injection of 18F-AZAN expressed as percentage standardized uptake value averaged across scans of subjects without recent history of nicotine exposure (9 subjects, 14 scans). SD bars are shown for thalamus for reference. (B) Plots of total and metabolite-corrected plasma time–activity curves. Inset shows first 8 min after slow-bolus injection.
Evaluation of Data Analysis Methods
The 1-tissue-compartment model was rejected because TTCM showed lower Akaike information criterion values than the 1-tissue-compartment model in all cases. However, TTCM suffered unstable estimates of VT and BPND (e.g., coefficients of variation > 50% in regions) compared with TTCM-C (coefficient of variance < 30%). PRGA showed excellent time consistency (0–60 min, that is, using data obtained between 0 and 60 min after injection vs. 0–90 min) on VT and BPND estimates (Fig. 2) with t* (the start of asymptote) set at 20 min. However, TTCM-C suffered some outliers (VT or BPND > 40) and showed similar time consistency to PRGA only after removal of outliers (R2 [the coefficient of determination] = 0.994 for VT; R2 = 0.948 for BPND). The use of larger cortical regions stabilized estimates of VND (e.g., coefficient of variance decreased from 31.1% in corpus callosum to 15.3% in occipital cortex) without eliminating outliers or improving time consistency. These findings suggested that PRGA may be the optimal method for the derivation of VT and BPND for 18F-AZAN. However, TTCM-C was used for TRV calculation to confirm the findings of this section.

Scatterplots of regional VT (A; using 18 scans from 13 subjects, 25 regions per scan, including corpus callosum) and BPND (B; excluding corpus callosum) given by PRGA, 0–60 min (i.e., using frames taken between 0 and 60 min after injection [y]) vs. 0–90 min (x). Regression equations are shown with coefficient of determination (R2). P < 0.001 for both A and B.
TRV
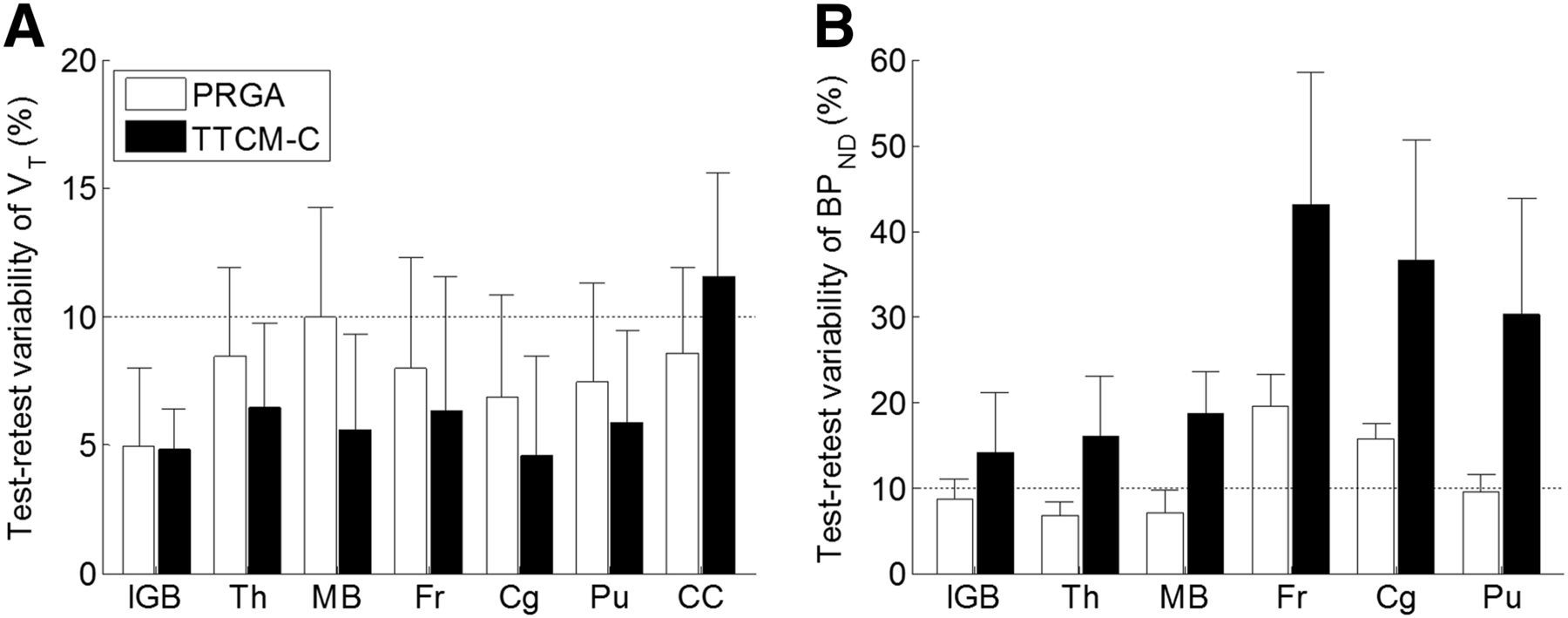
TRV estimates of selected regions are shown in Figure 3 (VT, Fig. 3A; BPND, Fig. 3B), together with the frontal lobe to exemplify cortical regions and corpus callosum, the reference region. TRV estimates of VT did not differ between the 2 methods, slightly below 10%, except for corpus callosum by TTCM-C. However, PRGA showed TRV estimates below 10% in high-BPND regions, a widely accepted level (27,28) in high-BPND regions, whereas TTCM-C showed higher TRV estimates across regions.

TRV (%) of VT (A) and BPND (B) for PRGA and TTMC-C (5 subjects). Horizontal dotted lines indicate 10% TRV level for reference.
Regional VT and BPND
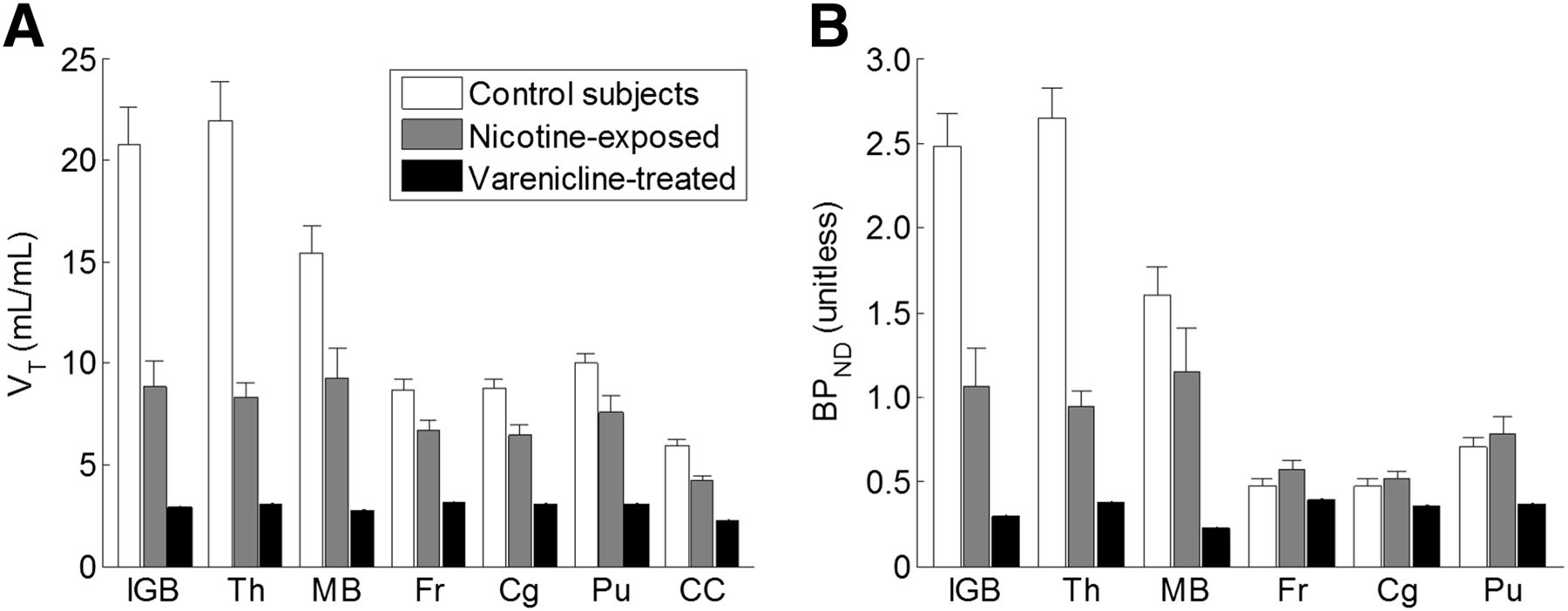
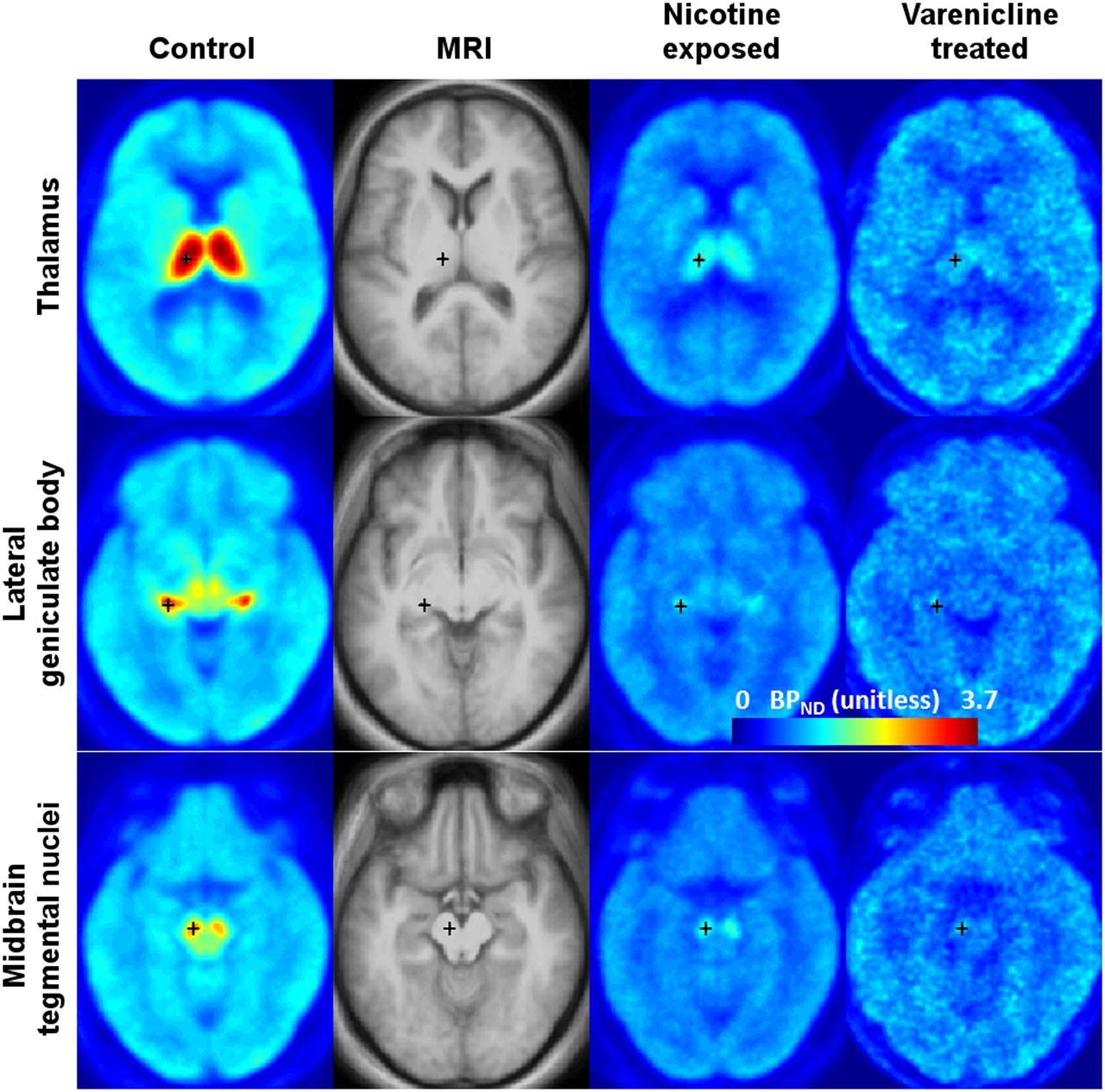
Regional VT and BPND values given by PRGA are shown in Figure 4 for selected brain regions. In control subjects without a recent history of nicotine exposure, the lateral geniculate body, thalamus, and midbrain tegmentum nucleus showed the highest VT and BPND values among the 25 brain regions. Frontal and cingulate cortices, of particular importance in cognition, showed middle-range VT and BPND among cortical regions, whereas putamen showed the highest VT and BPND among subcortical regions. None of the subcortical regions, except for the lateral geniculate body, thalamus, and midbrain tegmentum nucleus, exhibited BPND values greater than 1. These regional differences in BPND, given by the above volume-of-interest–based analyses, were visually confirmed by spatially normalized, averaged BPND maps (Fig. 5; left column). BPND images also confirmed displacement of BPND in subjects with nicotine-exposure history and in 1 subject who received varenicline pretreatment (Fig. 5; right columns).

Regional VT (A; mean boxes with SE bars) and BPND (B) of 18F-AZAN given by PRGA for subjects without (control; n = 9) and with (nicotine-exposed; n = 3) recent history of nicotine, and with varenicline treatment (n = 1). Regions are lateral geniculate body (lGB), thalamus (Th), mid brain tegmental nucleus (MB), frontal (Fr) and cingulate (Cg) cortices, putamen (Pu), and corpus callosum (CC).

Transaxial BPND images, spatially normalized and averaged across several subjects, of 18F-AZAN at levels of thalamus, lateral geniculate body, and mid brain tegmental nucleus for subjects without (control; n = 9) and with (nicotine-exposed; n = 3) recent history of nicotine, and with varenicline treatment (n = 1). Second column shows matching MR images.
DISCUSSION
Because of the relatively low density of central nervous system α4β2-nAChR, the development of a quality PET radioligand for nAChRs with high specific binding and sufficiently rapid brain kinetics is a challenge. The kinetic drawbacks of existing nAChR radioligands (2-18F-FA and 6-18F-FA) prompted the development of radioligands with faster brain kinetics by our group and others (8–12,14,15,29). Studies in our labs on the radioligand structure–imaging properties relationship (17,30–32) led us to synthesize 18F-AZAN, an α4β2-nAChR antagonist with rapid brain kinetics and high binding potential values in mice and baboons (17,18). Further, a blockade PET study (18) with the selective partial α4β2-nAChR agonist cytisine strongly suggested that 18F-AZAN binds predominantly at α4β2-nAChRs. Moreover, unlike 2-18F-FA, a radioligand with exceptionally low lipophilicity, 18F-AZAN exhibits an optimal value of lipophilicity for blood–brain permeability (Table 3).
Molecular Determinants and nAChR Subtype Binding Affinity of 2-FA and AZAN (17)
The baseline PET experiments in human subjects showed that 18F-AZAN rapidly enters the brain and is distributed in brain regions with high densities of α4β2-nAChR. In the thalamus, a region with the greatest density of α4β2-nAChR, the radioactivity peaked at 10–15 min after injection with robust washout throughout the rest of the scanning. The uptake was more rapid in the cortex and corpus callosum, the regions with intermediate and the lowest densities of nAChR, respectively.
As expected, brain uptake of 18F-AZAN was substantially lower in patients exposed to nicotine, because of competition with 18F-AZAN. The accumulation of 18F-AZAN radioactivity in human brain was blocked by oral preadministration of (−)-nicotine (Fig. 5). The blocking effect of nicotine was more evident in the nAChR-rich thalamus and lateral geniculate body than in the striatum and corpus callosum, confirming that 18F-AZAN specifically binds at nAChR in the human brain. Blocking was also demonstrated after varenicline administration, further confirming the α4β2-nAChR in vivo specificity.
The rate of the 18F-AZAN metabolism is slightly faster than that of 2-18F-FA, but the metabolism rate is not likely to be a confounding factor for 18F-AZAN since its scanning time is so much shorter than that used with 2-18F-FA. In fact, 18F-AZAN showed stable regional estimates of VT and BPND after 60 min with PRGA. In addition, the HPLC analysis demonstrated that radiometabolites of 18F-AZAN are the same as those in baboon and mouse plasma and are hydrophilic and unlikely to penetrate the blood–brain barrier (17), which is an advantage of 18F-AZAN since 2-18F-FA generates a lipophilic radiometabolite in human plasma (33).
Evaluation of standard methods for VT and BPND identified PRGA as the optimal method for 18F-AZAN PET studies, using corpus callosum as the reference region in human subjects for BPND, as proposed for 6-18F-FA (33) and 2-18F-FA (34). Critical findings for this methodologic conclusion can be summarized as follows: first, this method showed time-constant estimates of VT and BPND when the PET duration was set at 60 min or longer. Second, TRV on BPND was less than 10% in most regions, although TRV was greater than 20% for VT. In contrast, other plasma input methods showed some negative findings. Both TTCM and TTCM-C yielded some outliers for VT for 60- and 90-min scanning periods, although the longer scanning duration decreased outliers. BPND might not be obtained as k3/k4 ratio for 18F-AZAN, potentially because of the fact that these methods could not identify VND (i.e., large variations of VND among subjects). Unstable estimates of VND by TTCM were also reported by other receptor radioligands such as 11C-OMAR for CB1 (35) and 11C-ABP688 for the metabotropic glutamate receptor subtype 5 (36). An alternative approach for BPND (i.e., [target VT/corpus callosum Vt] − 1), which appeared successful for PRGA, resulted in high TRV values for TTCM-C because of unacceptably large TRV values on the corpus callosum. It was speculated that small errors in measurements of plasma radioactive metabolites with high metabolite percentages (i.e., >75% at 60 min) could have different effects on PRGA and compartmental analysis; the errors caused outliers and unstable estimates of VT in the corpus callosum (the region of the lowest radioactivity) for TTCM and TTCM-C, which could be prone to errors. The errors cause higher TRV on VT (which is directly affected by errors in plasma data) but low TRV on BPND (with plasma errors canceled out) for PRGA, assuming PRGA is robust against errors in plasma data. We specifically chose not to use the free fraction as a variable in our analysis because neither that nor blood–brain transport is directly related to our chosen outcome measures (BPND and VT). It is also our assertion that the free fraction is a variable that can add more inaccuracy, that plasma free fraction–corrected variables are not used as commonly in the literature, and that true in vivo free fraction is controversial.
To our knowledge, only a few PET imaging studies using α4β2-nAChR radiotracers have been attempted to study important neuropsychiatric disorders such as schizophrenia (7) and Alzheimer disease (37,38), as well as smoking (5,34,39). 18F-AZAN provides an essential tool for the expansion of imaging research in these areas.
CONCLUSION
18F-AZAN allows data acquisition times of less than 1.5 h, as compared with the 6 or more hours required for the other existing human radioligands. 18F-AZAN exhibits greater specific binding and is likely to be more accurate than 2-18F-FA. PRGA and RTGA were identified as appropriate for obtaining BPND with 18F-AZAN. With a calculated radiation dosimetry that could permit multiple studies in a single subject to be conducted, these data support 18F-AZAN as an important tool for studying neuropsychiatric disorders, possible therapeutic drugs, and the effects of tobacco smoke.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by NIH grants DA020777, R33MH079017, DA026823-01, 5T32EB006351-05, R03DA027522, and K24 DA000412; SRI toxicology study M617-08; some pilot work from unrestricted funds provided by the Philip Morris USA External Research Program; and primary funding from unrestricted funds from the Johns Hopkins Department of Radiology. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Maria Thomas, PhD, Ayon Nandi, Stephanie Darnley, Andrew Crabb, Arman Rahmim, PhD, Hayden T. Ravert, PhD, and Daniel P. Holt for their expertise with radiotracer chemistry. We are grateful to Dr. Mike Stabin of Vanderbilt University for calculation of absorbed doses.
Footnotes
Published online Jun. 25, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication May 8, 2013.
- Accepted for publication February 28, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A thalamic circuit represents dose-like responses induced by nicotine-related beliefs in human smokers
- Rare coding variants in CHRNB2 reduce the likelihood of smoking
- PET Imaging of Cholinergic Neurotransmission in Neurodegenerative Disorders
- 18F-XTRA PET for Enhanced Imaging of the Extrathalamic {alpha}4{beta}2 Nicotinic Acetylcholine Receptor