


Abstract
The development of noninvasive imaging techniques using monoclonal antibodies (mAbs) is a quickly evolving field. Immuno-PET uses positron-emitting isotopes to track the localization of mAbs with excellent image quality. Procedures for labeling mAbs with 89Zr or 124I using good manufacturing procedures have been established, and therefore these radiopharmaceuticals are being investigated for clinical use. This short review will focus on immuno-PET with full mAbs using long-lived positron-emitting isotopes (89Zr and 124I) over the past 5 y and discuss their progress into clinical use.
The idea of the magic bullet was first suggested by Paul Ehrlich more than a century ago (1). He theorized that if a compound could target a disease selectively, then that compound could be combined with a therapeutic agent to treat the disease. This concept has inspired many drugs, both for treatment and for detection of a variety of diseases including cancer. Over the past 2 decades, targeted cancer therapy using monoclonal antibodies (mAbs) has shown that mAbs have many of the properties of Ehrlich’s magic bullets. Currently, 22 mAbs have been accepted by the U.S. Food and Drug Administration for therapy, with most being for the treatment of cancer (2). These molecules have high specificities for their targets and, when coupled with their high binding affinities, provide an attractive targeting tool to image and treat tumors.
Typically, mAbs achieve optimal tumor-to-nontumor ratios at 2–4 d after injection, which limits the choices of suitable radionuclides based on their physical half-lives (3). Common radiometals, such as 99mTc, 86Y, 68Ga, or 64Cu, have half-lives less than 15 h, resulting in decay of the isotope before the attached radiolabeled mAbs achieve peak tumor-to-background ratios. However, 64Cu-labeled mAbs have found some success in clinical trials. Currently, phase I trials are investigating the relationship between 64Cu-labeled U3-1287 and human epidermal growth factor receptor 3, as well as the dosimetry in humans. In a separate trial, the correlation between 64Cu-labeled trastuzumab uptake, tumor expression of human epidermal growth factor receptor 2 (HER2), and the inactivation of the phosphatidylinositol-3-kinase/protein kinase B pathway are being investigated (4). The use of a longer-lived radionuclide enables the labeled mAb to achieve high tumor-to-background ratios before decay. 124I and 89Zr, with half-lives of 4.18 and 3.27 d, respectively, are good candidates for immuno-PET for this reason (5). The use of each isotope has its own advantages and disadvantages. Iodine has relatively simple and well-developed labeling chemistry; however, its decay involves high-energy positrons (687 and 974 keV), which decrease image resolution (6). The decay pathway of zirconium involves a lower positron energy emission; however, it also releases a high-energy, highly penetrating photon (909-keV γ-ray) 99% of the time. This photon means that more shielding and care in shipping and handling are required for 89Zr than for many other PET isotopes. Additionally, the labeling chemistry is not as developed as that of iodine, usually using the conjugation of zirconium to a multidentate ligand such as deferoxamine (DFO) (Desferal; Macrocyclics). Furthermore, 124I is commonly used with noninternalizing mAbs, which avoids dehalogenation from intracellular enzymes. 89Zr is used with internalizing mAbs because it is a residualizing radionuclide and stays in the target cell after catabolism (7).
LABELING CHEMISTRY
Several exceptional reviews exist on the subject of immuno-PET. An excellent review by Knowles and Wu gives readers a full introduction to the field (8). Koehler, Gagnon, and Wuest give an overview of the use of 124I, and a review by Deri and Lewis provides a comprehensive history of 89Zr (9,10). In general, radioiodination of peptides and proteins is performed via the use of IODO-GEN (Pierce)–coated reaction vessels, eliminating the need to include the oxidizing agent in the reaction mixture and allowing for a simple filtration purification (11).
Radiolabeling of biomolecules with 89Zr is most commonly performed through the modification of a native lysine side chain with activated esters of DFO. Until recently, most researchers applied Verel and van Dongen’s method of conjugation using an activated 2,3,5,6-tetrafluorophenol ester of DFO. This method requires multiple steps, including protection of the DFO with iron, conjugation to the biomolecule, and then deprotection of the DFO (12). Recently, a much simpler method by Vosjan and van Dongen used p-isothiocyantobenzyl-DFO (Df-Bz-NCS) to conjugate DFO to the biomolecule in 1 step with good yields (13). This method lends itself to clinical translation because it requires fewer steps and the materials are commercially available.
CLINICAL STUDIES: 124I
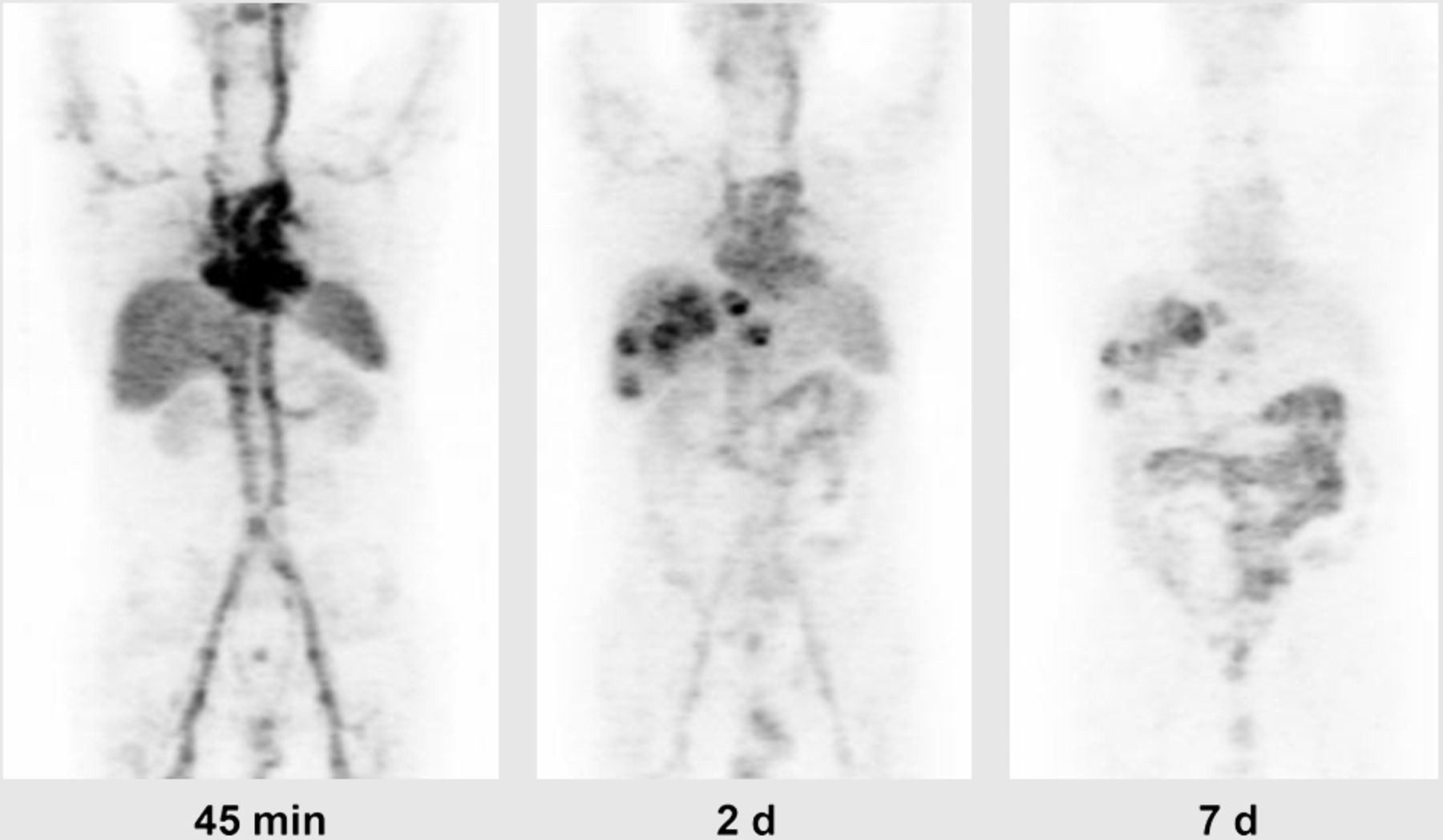
Several radioiodinated mAbs have recently been evaluated for clinical use. Carrasquillo et al. have evaluated a humanized A33 (huA33) for PET imaging with 124I (14). This mAb recognizes A33 antigen, which is known to be expressed in greater than 95% of human colon adenocarcinomas. In this study, 25 patients with primary or metastatic colorectal cancer (CRC) were administered 44.4–396 MBq (median, 343 MBq) of 124I-huA33 with a total of 10 mg of huA33. The authors observed no adverse side effects during the treatment that could be attributed to the huA33. Treatment could be administered via intravenous administration or hepatic arterial infusion (HAI), with HAI giving no detectable advantage over intravenous injection. Eleven patients had 12 primary tumors, 10 of which were observed via immuno-PET. Ten patients had liver metastases, all of which were identified by 124I-huA33 (Fig. 1). Four of 7 patients with nodal metastases displayed uptake of the 124I-huA33, and 2 of 5 patients with lung lesions were visualized by immuno-PET. Furthermore, the tracer uptake in the tumors displayed an extended retention time, and in some cases this retention was so long the authors were unable to determine the time required for clearance. Even with this issue, the study was still in agreement with the half-life that had been reported by others, and displayed an average clearance of 3.10 ± 5.6 mL/h for intravenous injection, 36.8 ± 8.4 mL/h for intravenous IgG, and 35.2 ± 8.0 mL/h for HAI (14). The authors also note that even with the superior localization of the 124I-A33 in the tumor in comparison to the colon tissue (4:1 tumor-to-colon ratio), there was some difficulty in identifying the primary colon tumors and lymph node lesions because of high background activity. They suggest that this problem could be remedied by delaying imaging further to allow for clearance of the tracer from the bowel.

Example of 124I-huA33 imaging in patient with CRC metastasized to liver. Images show blood-pool activity at 45 min, excellent localization in liver lesions at 2 d, and persistent uptake in liver lesions at 7 d. (Reprinted with permission of (14).)
Although intact mAbs do not cross the blood–brain barrier, imaging and treatment of metastatic tumors is possible because of a compromised blood–brain barrier. In a recent investigation, Poli et al. evaluated 124I-labeled L19SIP (radretumab) for use in determining provisional doses of 131I-labeled radretumab in 6 patients with brain metastasis (3 from non–small cell lung cancer and 3 from breast carcinoma). Radretumab, a fully humanized mAb, has been thoroughly investigated previously as a 131I-labeled targeting agent (15). This mAb targets an epitope contained in the extra-domain B of fibronectin, a domain rarely found in normal adult tissue but often found in the extracellular matrix surrounding newly formed blood vessels in tumors (16). In this study, each of the 6 patients was administered an average of 167 MBq (roughly 3.3 mg of protein), and the bone red marrow, tumor lesion, and healthy organ doses were monitored. The bone red marrow dose was found to be approximately 0.2 Gy/GBq and always less than 2 Gy, suggesting that up to 7.4 GBq could be injected without compromising the blood-building system long-term. These results correlated favorably with clinical findings for 131I-radretumab (≤9.3 GBq allowed) (15). The absorbed lesion dose was observed to be an average of 2.4 Gy (range, 0.70–8.1 Gy) for brain metastases and 7.3 Gy (range, 1.1–35.8 Gy) for extracranial lesions. The absorbed dose in the healthy organs was constant among all 6 patients. Only the thyroid displayed variable uptake among patients; however, this variability was explained by the fact that 3 of the patients did not strictly follow the thyroid-blocking therapy that was prescribed and is attributed to dehalogenation.
In a study published early this year, Divgi et al. reported the results of a multicenter phase III clinical study evaluating the effectiveness of 124I-labeled cG250 (girentuximab) in detecting clear cell renal cell carcinoma (ccRCC) (17). This chimeric antibody binds carbonic anhydrase IX (CAIX), which is expressed in more than 95% of ccRCC. The 124I-girentuximab was administered to 204 patients at 14 centers in the United States and was monitored by PET/CT and contrast-enhanced CT (CECT). Of the 204 patients, 203 underwent CECT and 202 had surgery to confirm or remove the tumors. No allergic reactions to the drug were observed in the patients during the study; however, adverse effects to the treatment were reported in 30 of the patients (13.3%). The most commonly reported event was headache (10 patients, 4.4%). The authors reported that 1 patient had a grade 3 agent-related event (transient liver enzyme increase); however, the patient had also received ciprofloxacin before the event. The average sensitivity and specificity for detection of ccRCC were 86.2% and 85.9%, respectively, and all lesions below 1 cm were visualized. In comparison, the average sensitivity and specificity for CECT were 75.5% and 46.8%, respectively. Additionally, the accuracy of the PET/CT estimates was consistently greater than that of the CECT (range, 85.6%–86.7%, compared with 66.2%–69.2%). This study confirmed the efficacy of 124I-girentuximab as a noninvasive method of identifying ccRCC. Although the requirement for participation in the study was that patients be able to undergo surgery, the imaging strategy has the potential to reduce unnecessary surgeries in patients with benign renal masses.
PRECLINICAL PROGRESS: 89ZR
The success of the earlier phase I study of Divgi et al. inspired Stillebroer et al. to investigate the comparison of 124I-labeled girentuximab and 89Zr-labeled girentuximab (18). In this study, nude mice with subcutaneous ccRCC xenografts were treated with either 89Zr-Df-girentuximab or 124I-girentuximab, and the biodistribution was observed 7 d after injection. Uptake of 89Zr-Df-girentuximab was significantly higher than that of 124I-girentuximab in CAIX-expressing tumors (114.7 ± 25.2 percentage injected dose [%ID] vs. 38.2 ± 18.3 %ID) but was similar in the CAIX-negative tumors (48.7 ± 15.2 %ID vs. 32.0 ± 22.9 %ID). Images of the 89Zr-Df-girentuximab tumors had higher contrast and less noise than those of 124I-girentuximab. Comparison of the biodistribution in both models displayed a higher amount of 89Zr-Df-girentuximab in the liver and spleen, whereas the 124I-girentuximab scans showed higher activity in the thyroid. Additionally, the tumor uptake was assessed by comparing the 89Zr-Df-girentuximab with an irrelevant control mAb (89Zr-Df-MOPC21). Uptake of 89Zr-Df-girentuximab in the CAIX-positive tumors was greater than that of the irrelevant mAb (36.5 ± 6.2 %ID vs. 6.8 ± 2.3 %ID), showing that the uptake was due to the affinity of the mAb for CAIX. The high specificity and greater contrast demonstrated here, combined with the success of the recent phase III trial by Divgi et al., show promise for 89Zr-Df-girentuximab.
Development of a mAb that targets a receptor commonly overexpressed by multiple tumor types would allow for a more general treatment for patients. The epidermal growth factor receptor (EGFR), a member of the ErbB tyrosine kinase receptor family, is known to be overexpressed in most tumors (19). Panitumumab is a fully humanized antibody that is approved by the Food and Drug Administration for treatment of metastatic CRC; however, it has been demonstrated that panitumumab can be effective against other malignancies as well (20,21). EGFR expression can vary between primary and metastatic tumors, and thus a noninvasive method for determining EGFR expression in patients would allow for a more accurate dosing regimen. Attempting to solve this issue, both Nayak et al. (20) and Chang et al. (21) have explored the use of panitumumab labeled with 89Zr with promising results. Nayak et al. investigated the efficacy of imaging with 89Zr-panibumumab in 2 CRC xenografts (LS-174T and A375 cells). Imaging results showed high uptake in the highly EGFR-expressing LS-174T and low uptake in the EGFR-negative A375 cells (20). In the study by Chang et al., 89Zr-panitumumab imaging was examined in 4 different xenografts (A431, HTC116, MDA-MB435, and T47D cells) of varying levels of EGFR expression. The imaging results showed high uptake in the highly EGFR-expressing A431 tumors and moderate intensity in the moderately expressing HCT116 tumors. The intensity for the low and nonexpressing tumors was minimal. Cold panitumumab was shown to block uptake in both HCT116 tumors (21) and LS-174T tumors (20), demonstrating a significant decrease in intensity after 5 d and illustrating the specificity of the tracer. Use of this radiotracer would enable EGFR expression to be quantified in patients to determine the effectiveness of this type of treatment.
CLINICAL STUDIES: 89ZR
Several researchers have investigated 89Zr-labeled mAbs in a clinical setting. Böjesson et al. investigated the safety of a chimeric mAb known as U36 labeled with 89Zr to target the v6 region of CD44 of head and neck squamous cell carcinoma (22). This study was a follow-up to their earlier work, in which they demonstrated the diagnostic capabilities of this radiolabeled antibody. Twenty patients underwent imaging with 89Zr-U36 before surgery (10 mg, 74.9 MBq). From the study, Böjesson et al. determined that the 89Zr-U36 was safe for all subjects. No adverse reactions were observed during the study. The mean dose for patients, about 40 mSv, will limit the number of times a patient can repeat the treatment. The authors do suggest that the use of newer PET/CT scanners will give better images, halve the mean dose, and reduce the number of treatments required.
Trastuzumab (Herceptin; Genentech) targets the HER2, a well-researched receptor known for its involvement in cell proliferation, metastasis, and angiogenesis (23). Dijkers et al. conducted the first-in-human investigation of 89Zr-trastuzumab in 2010, with the goal of determining the optimal dosage and time of administration. Fourteen patients were administered 38.4 ± 1.6 MBq of 89Zr-trastuzumab, and no reactions or adverse events were observed during the study. Patients with HER2-positive metastatic breast cancer were split into 3 groups and administered either 10 mg of 89Zr-trastuzumab, 50 mg of 89Zr-trastuzumab, or 10 mg of 89Zr-trastuzumab plus trastuzumab therapy and then were imaged after 5 d. Lesions were visualized in only one of the patients receiving 10 mg of the imaging agent only. A high uptake in the liver and a prominent intestinal excretion were observed, which corresponded with previous pharmacokinetic studies (23). Trastuzumab-naïve patients treated with 50 mg of 89Zr-trastuzumab showed decreased uptake in the liver in comparison to the 10-mg dose and an increased presence in the blood pool, suggesting retarded blood clearance. Patients undergoing trastuzumab treatment in addition to the 10 mg of 89Zr-trastuzumab also displayed a decreased blood clearance. Most of the metastatic lesions were visualized and confirmed via CT and MR imaging in both 50-mg and 10-mg-plus-therapy groups; however, it was noted that in 6 of 12 patients, not all known lesions were detected. The authors suggest that this is due to varying expression of HER2 between lesions or from suboptimal imaging conditions. Unexpectedly, Dijkers et al. were able to visualize brain lesions with an 18-fold-higher uptake in the tumors than in normal tissues and were able to discover previously undetected lesions that were later confirmed by MR imaging (Fig. 2). This suggests that the trastuzumab-based therapies can be used to treat patients with HER2-positive brain metastases. Several clinical trials are currently under way investigating 89Zr-labeled trastuzumab as a diagnostic tool for HER2-positive metastases. Additionally, several more clinical trials are looking at other 89Zr-labeled mAbs, such as cetuximab and bevacizumab, as PET imaging agents (24).

Example of HER2-positive brain lesion undetected by conventional scans, revealed with 89Zr-trastuzumab imaging and subsequently confirmed by MR imaging. Arrow indicates lesion. (Reprinted with permission of (23).)
CONCLUSION
The field of immuno-PET is rapidly progressing toward clinical use. 124I has been shown to be a long-lasting and effective radionuclide for imaging various types of lesions, both primary and metastatic, and for determining the effectiveness of 131I treatments. Phase III clinical trials using 124I-girentuximab have been shown to be an effective method for detecting ccRCC in more than 200 patients. 89Zr-labeled mAbs, although still requiring more research, have shown promising results in targeting a wide variety of receptors and tumor types. In an effort to hasten the localization of the radiometals, some researchers have also looked to engineered mAb fragments, diabodies, minibodies, and other mAb fragments Future work in the field will likely improve current procedures and make use of these other engineered targeting moieties to improve imaging capabilities.
DISCLOSURE
This work is supported in part by DOE grant DESC0008432. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the Lapi Research Group for useful discussions.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 26, 2013.
- Accepted for publication July 9, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Bicyclic Peptides as a New Modality for Imaging and Targeting of Proteins Overexpressed by Tumors
- Fc-Mediated Anomalous Biodistribution of Therapeutic Antibodies in Immunodeficient Mouse Models
- Noninvasive Imaging of Human Immune Responses in a Human Xenograft Model of Graft-Versus-Host Disease
- Update on Time-of-Flight PET Imaging