


Abstract
Reported experience with systemic 131I-metaiodobenzylguanidine (131I-MIBG) therapy of neuroendocrine tumors comprises different dosing schemes. The aim of this study was to assess the long-term outcome and toxicity of treatment with 11.1 GBq (300 mCi) of 131I-MIBG per cycle. Methods: We performed a retrospective review of 31 patients with advanced metastatic neuroendocrine tumors (20 with carcinoid tumors and 11 with other tumors) treated with 131I-MIBG. Treatment outcome was analyzed for patients with carcinoid tumors (the most common tumors in this study), and toxicity was analyzed for the entire patient cohort (n = 31). Treatment comprised 11.1 GBq (300 mCi) per course and minimum intervals of 3 mo. The radiographic response was classified according to modified Response Evaluation Criteria in Solid Tumors. Toxicity was determined according to Common Terminology Criteria for Adverse Events (version 3.0) for all laboratory data at regular follow-up visits and during outpatient care, including complete blood counts and hepatic and renal function tests. Survival analysis was performed with the Kaplan–Meier curve method (log rank test; P < 0.05). Results: The radiographic responses in patients with carcinoid tumors comprised a minor response in 2 patients (10%), stable disease in 16 patients (80%; median time to progression, 34 mo), and progressive disease in 2 patients (10%). The symptomatic responses in patients with functioning carcinoid tumors comprised complete resolution in 3 of the 11 evaluable symptomatic patients (27%), partial resolution in 6 patients (55%), and no significant change in 11 patients. The median overall survival in patients with carcinoid tumors was 47 mo (95% confidence interval, 32–62), and the median progression-free survival was 34 mo (95% confidence interval, 13–55). Relevant treatment toxicities were confined to transient myelosuppression of grade 3 or 4 in 15.3% (leukopenia) and 7.6% (thrombocytopenia) of applied cycles and a suspected late adverse event (3% of patients), myelodysplastic syndrome, after a cumulative administered activity of 66.6 GBq. The most frequent nonhematologic side effect was mild nausea (grade 1 or 2), which was observed in 28% of administered cycles. No hepatic or renal toxicities were noted. Conclusion: Dose-intensified treatment with 131I-MIBG at a fixed dose of 11.1 GBq (300 mCi) per cycle is safe and offers effective palliation of symptoms and disease stabilization in patients with advanced carcinoid tumors. The favorable survival and limited toxicity suggest that high cycle activities are suitable and that this modality may be used for targeted carcinoid treatment—either as an alternative or as an adjunct to other existing therapeutic options.
- neuroendocrine tumors
- 131I-MIBG therapy
- radionuclide therapy
- carcinoid tumors
- targeted radiotherapy
- oncology
Despite the recent developments in cytoreductive therapies, treatment options for nonresectable metastatic neuroendocrine tumors (NET) are still limited. Targeted radionuclide therapy with radiolabeled somatostatin analogs or 131I-metaiodobenzylguanidine (131I-MIBG) offers an effective systemic treatment with low overall toxicity. 131I-MIBG provides efficient internal radiotherapy of chromaffin tumors (neuroblastoma, pheochromocytoma, and paraganglioma), carcinoid tumors, and other, less common tumors (1–6). Such therapy makes use of specific cellular structures, the reuptake mechanism, and storage granules in specialized neuroendocrine cells to target and concentrate within tumor cells (7,8). Since their introduction into routine clinical practice in the 1980s, most reported 131I-MIBG treatment protocols have comprised therapeutic activities between 3.7 and 11.1 GBq (100 and 300 mCi, respectively) per course (9,10). Some centers use body weight–adapted schedules, such as 92.5 MBq/kg (2.5 mCi/kg) (9,10). In more recently introduced dose-intensified schedules, activities of 14.8–18.5 GBq (400–500 mCi) per treatment course were used; high-dose schedules might incorporate more than 22.2 GBq (600 mCi) supported by potential autologous stem cell rescue (11,12). The practice at the University Hospital Bonn is to use 11.1 GBq (300 mCi) per treatment course.
In this study, we evaluated the response and long-term outcome of this regimen in patients with carcinoid tumors, the predominant tumor type in our cohort, as well as the incidence and severity of toxicity observed in the entire cohort, including patients with other NET.
MATERIALS AND METHODS
This study was performed in accordance with the Declaration of Helsinki and with national regulations. Approval by an institutional review board is not required for retrospective studies on nonexperimental interventions at our institution. 131I-MIBG therapy of patients with inoperable metastatic neuroendocrine tumors is considered the standard of care and a nonexperimental therapy in Germany. As stated later, all patients had given informed consent to the treatment. In addition, explicit approval from the local ethics committee was obtained for general prospective and retrospective assessments of the outcomes of patients with NET throughout follow-up at our institution, including this retrospective investigation.
Patients
Thirty-one consecutive patients (34–79 y old; 16 women) who had histologically proven, inoperable, metastatic NET treated with 131I-MIBG at our institution and for whom restaging had been completed were included in the retrospective analysis. Prerequisites for the treatment consisted of sufficient tumor uptake (i.e., greater than that of normal liver tissue), as documented with a diagnostic 131I-MIBG scan, and either an uncontrolled symptomatic functional tumor or documented tumor progression. All patients had given informed consent to the treatment. The composition of the tumors in the study cohort was as follows: carcinoid tumors (n = 20; 11 men and 9 women; mean age, 62 y; range, 34–79 y), pheochromocytoma or paraganglioma (n = 6), medullary thyroid cancer (n = 3), insulinoma (n = 1), and unknown primary NET (n = 1). Table 1 shows the characteristics of the patients and the administered therapeutic doses.
Characteristics of Patients in Entire Study Cohort
131I-MIBG Therapy
The standard activity of 11.1 GBq (300 mCi) of 131I-MIBG (GE Healthcare Amersham Buchler GmbH & Co. KG) per treatment course was administered for a minimum of 2 courses and at intervals of 3 mo. Repeat cycles (up to 4 cycles for patients with carcinoid tumors) were dependent on observed clinical responses and patients’ requests. The specific activity of 131I-MIBG was in the given range of 1.1–1.5 GBq/mg. Potentially interfering medication was paused within an adequate time frame on the basis of the interaction mechanism (13). Thyroid uptake of free 131I was blocked by oral administration of sodium perchlorate at 1.800 mg/d, split into 3 doses, starting 1 d before the treatment and continuing for at least 4 wk. If perchlorate was not well tolerated, then patients received 100 mg of oral iodine per day instead. Because of the excessive amount of cold pharmacologically active 131I-MIBG molecules in the infusion solution (specific activity, <1.5 GBq/mg), the radiopharmaceutical was administered with monitoring of heart rate and blood pressure and at a constant rate of 1.85 GBq/h (50 mCi/h) to avoid relevant adverse pharmacologic effects of 131I-MIBG (14). Higher specific activities would allow more rapid administration with virtually no risk of pharmacologic adverse effects (15).
Toxicity
Treatment toxicity was assessed in the entire patient cohort (n = 31). Blood pressure was monitored throughout all administrations and was analyzed to assess the risk of acute hypertension. Complete blood counts were determined and hepatic and renal function tests were conducted at the recommended 2-wk intervals between the treatment courses and during the follow-up period. General gastrointestinal toxicity was recorded by thorough hospital documentation before, during, and after the procedure. Toxicity was determined according to Common Terminology Criteria for Adverse Events (version 3.0; CTCAE).
Response Assessment, Follow-up, and Survival Analysis
The morphologic response was assessed 3 mo after the last treatment cycle and confirmed by a repeat measurement 3–9 mo from the first claim of a response. The imaging modality was the same as that used at the baseline (CT or MR imaging). Response Evaluation Criteria in Solid Tumors were applied, and the response category “minor remission,” defined as a 15%–30% remission (reduction in the sum of the longest diameters), was added to better address the limited shrinking tendency of carcinoid tumors. The symptomatic response in functioning carcinoid tumors (n = 11) was assessed according to the change in the intensity and frequency of tumor-specific symptoms such as diarrhea and flushing. It was categorized as complete resolution, partial resolution (≥50% reduction), no significant change, and progression of functional symptoms.
Response and long-term outcome were investigated only in 20 patients with carcinoid tumors. Outcome was not analyzed in patients with other tumor entities (pheochromocytoma or paraganglioma, medullary thyroid cancer, and other NET) because of the heterogeneity and small number of patients in each group. Monitoring of overall survival and progression-free survival was discontinued at the commencement of another significant treatment, such as peptide receptor radionuclide therapy (PRRT), chemotherapy, or debulking surgery, but not biotherapy with somatostatin analogs or interferon.
Survival analysis was performed with the Kaplan–Meier curve method. The log rank test was used to compare the survival of different groups (e.g., responders vs. nonresponders) by implementing a common statistical software package (SPSS; version 15.0; SPSS Inc.). A 2-tailed P value of less than 0.05 was considered significant.
RESULTS
Response and Treatment Outcome
Twenty patients with carcinoid tumors received a median of 2 treatment courses (range, 1–4). Before the initiation of treatment with 131I-MIBG, 12 patients (60%) showed morphologic tumor progression within less than 12 mo, and 11 patients (55%) had uncontrolled functional symptoms under somatostatin analog treatment. Three patients had both documented morphologic tumor progression and uncontrolled functional symptoms. Predominant symptoms were diarrhea (n = 7) and flushing (n = 6). Increased indices of liver dysfunction (i.e., transaminases and bilirubin) at baseline were observed in 7 of 16 patients with hepatic metastatic disease. All patients had undergone somatostatin receptor scintigraphy (111In-DTPA-octreotide; OctreoScan; Covidien, Petten, The Netherlands) within 4 wk of the diagnostic 131I-MIBG scan. On intraindividual comparison of the 2 modalities, 5 patients displayed more intense tracer uptake in somatostatin receptor scintigraphy in at least 1 lesion. However, sufficient 131I-MIBG accumulation, as far as discernible on planar imaging, was present in all tumor lesions.
In 4 patients, treatment was stopped after 1 cycle because of documented disease progression (n = 2) or at the patient’s request (n = 2). The median cumulative activity was 22.2 GBq (range, 11–44), and the median follow-up period was 68 mo (95% confidence interval [CI], 43–93). Morphologic responses consisted of a minor response in 2 patients (10%), stable disease in 16 patients (80%), and progressive disease in 2 patients (10%). Notably, 7 of the 8 patients without documented morphologic tumor progression at baseline also had stable disease as the outcome after treatment. The remaining patient experienced a minor response.
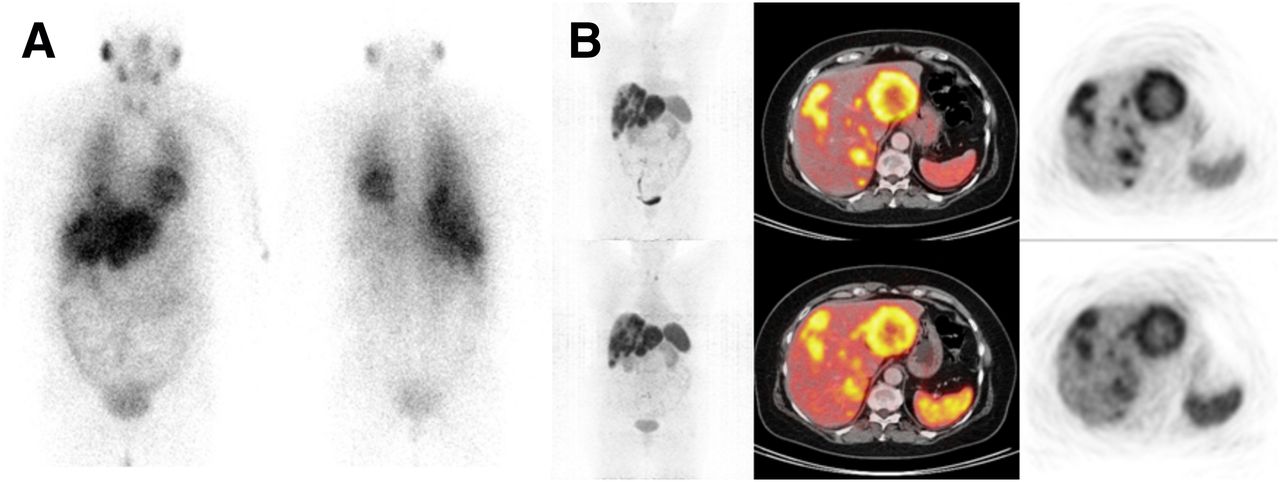
Figure 1 shows a common imaging result (disease stabilization) in a patient with a carcinoid tumor after 3 cycles of 131I-MIBG therapy. The median time to progression in patients in whom radiographic stable disease or a minor response was achieved (n = 18) was 34 mo (95% CI, 18–50). Three of 11 patients (27%) with symptomatic carcinoid tumors had a complete resolution of symptoms after treatment, and 6 patients (55%) had a partial resolution of symptoms after treatment. This symptomatic relief resulted in a reduction in the required doses of somatostatin analog treatment in 9 patients (≥50% reduction in 5 patients); this effect lasted for a mean of 14 mo (range, 8–26) from the completion of 131I-MIBG therapy. Only 2 patients (18%) had no significant symptomatic improvement.

(A) 131I-MIBG whole-body scans of patient with metastatic midgut carcinoid tumor. (B) Liver-dominant metastatic tumor load illustrated by axial 68Ga-DOTATOC PET/CT slices before (top) and after (bottom) 3 cycles of 11.1 GBq of 131I-MIBG each. Response was classified as stable disease according to Response Evaluation Criteria in Solid Tumors. Patient was still stable at end of study (analysis of progression-free survival discontinued at 69 mo after treatment).
The median overall survival and progression-free survival of patients with carcinoid tumors were 47 mo (95% CI, 32–62) and 34 mo (95% CI, 13–55), respectively. For 4 patients who received PRRT in a later follow-up, survival analysis was discontinued at the time of the new treatment. Limited tumor burden and high intensity of 131I-MIBG uptake were both associated with a longer time to progression (P = 0.03 and P = 0.002, respectively). The 5-y survival rate was 31% (95% CI, 9–54). Thirteen patients (65%) had died by the end of the study. Table 2 shows the survival data for patients with carcinoid tumors.
Treatment Outcomes in Patients with Carcinoid Tumors
Toxicity
Acute adverse events recorded during or shortly after the radiopharmaceutical infusion consisted of nausea in 28% of applied cycles, vomiting in 6%, and transient elevation of arterial blood pressure in 4%. These transient adverse events were uncomplicated and managed by simple symptomatic measures. The incidences of hematologic and nonhematologic toxicities in the entire cohort (31 patients; 78 treatment cycles) as well as in patients with carcinoid tumors (20 patients; 43 treatment cycles) are shown in Table 3. Treatment-induced myelosuppression was invariably of a transient nature. Supportive measures were required only after 1 administration in 1 patient in the entire cohort (3%).
Toxicities According to CTCAE After Dose-Intensified 131I-MIBG Treatment
Regarding significant leukopenia, CTCAE grade 4 was not observed, whereas grade 3 leukopenia was documented in 6 patients (19.3%) and after 12 administrations (15.3%). Significant thrombocytopenia (grade 3 or 4) occurred in 4 patients (12.9%) and after 6 treatment cycles (7.6%). Altogether, only 1 event of grade 4 hematotoxicity was observed; this event was documented at 4 wk after the second cycle in the form of transient thrombocytopenia (patient 2), with complete spontaneous recovery. The relationship between cumulative administered activity and myelosuppression is shown in Figure 2 (for leukocytes, P = 0.69; for platelets, P = 0.49). There was no significant association between the presence of bone metastases or a previous history of chemotherapy and the observed hematotoxicity (P > 0.1).
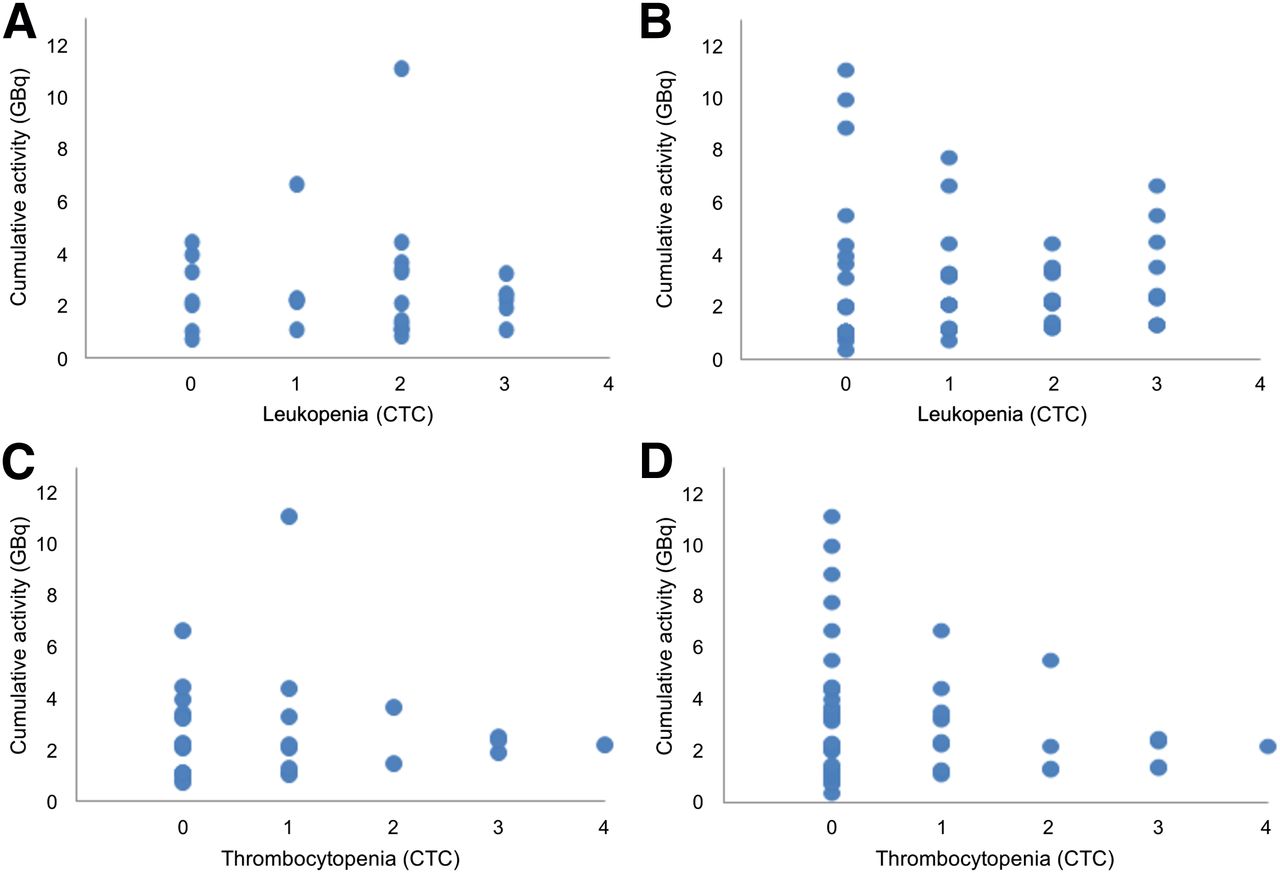
Relationship of cumulative administered activity and associated posttreatment myelosuppression. (A and B) Maximum leukopenia (CTCAE) observed per patient (A) and after each treatment cycle (B). (C and D) Maximum thrombocytopenia (CTCAE) observed per patient (C) and after each treatment cycle (D). There was no significant association between cumulative activity and degree of hematotoxicity in any graph (P > 0.1).
The only late adverse event in our cohort was the development of myelodysplastic syndrome in 1 patient with metastatic pheochromocytoma (patient 23); this event was documented 35 mo after the sixth treatment cycle (cumulative dose of 66.6 GBq [1,800 mCi]), when the patient was 69 y old. The patient had received prior external-beam radiation and had well responded to 131I-MIBG therapy, with partial remission. She had experienced transient leukopenia of grade 2 or 3 in a repetitive and nonincreasing manner after each administration, with complete recovery of blood counts before the next treatment cycle.
No other toxicities were observed. In particular, no case of hepatic failure (even in a heavily infiltrated metastatic liver), no case of hypothyroid dysfunction, and no deterioration of renal function were noted within the follow-up period. In 3 patients, the pretherapeutically increased liver function indices improved after 131I-MIBG therapy, whereas in 4 patients, there was no significant posttreatment alteration in the abnormal liver function profile. However, 1 of the latter 4 patients did experience a deterioration of liver enzyme levels 8 mo after the start of 131I-MIBG treatment (5 mo after the last cycle); this effect was obviously due to tumor progression. Hypothyroid dysfunction as a long-term side effect of the treatment has not occurred, although thyroid function tests for the given follow-up period were missing for 4 patients.
DISCUSSION
Our retrospective study of 31 patients with advanced metastatic NET confirmed that the dose-intensified regimen of 131I-MIBG was a safe and generally well-tolerated form of treatment and suggested a survival benefit for patients with carcinoid tumors. Given the absence of any treatment-induced nephrotoxicity, this therapeutic modality can be considered a reasonable tumor-targeted systemic treatment option for carcinoid tumors with sufficient tracer uptake in the diagnostic scan.
Therapeutic 131I-MIBG can provide significant symptomatic relief in many patients (50%–91%) with functioning metastatic carcinoid tumors (9,16–21). In agreement with previous studies, we found a symptomatic response (complete or partial resolution) in 82% of patients with functioning carcinoid tumors. This finding was particularly encouraging considering the difficulty in controlling carcinoid symptoms, which frequently determine patients’ quality of life and increase morbidity rates (22).
A morphologic tumor response after 131I-MIBG therapy, on the other hand, was less frequently observed for carcinoid tumors, with reported response rates of 0%–35% (10,11,23–27). The main observed outcome in the present study was disease stabilization (with or without minor remission) in 80%–90% of patients. This lower tendency toward tumor shrinkage in carcinoid tumors than in pancreatic NET has also been observed with other therapeutic modalities, including PRRT with 90Y-DOTATOC (28–31). However, it is not the morphologic tumor response, a common but sometimes misleading surrogate of therapeutic benefit, but the alleviation of symptoms and the prolongation of survival that comprise the true therapeutic benefit for patients with carcinoid tumors.
The observed survival of the carcinoid tumor patients in the present study, with a median overall survival of 47 mo, compared favorably with most reported outcomes for similar patient cohorts and with various protocols (23,25,27,32). There are also few other reports of considerably longer survival of patients with carcinoid tumors after 131I-MIBG treatment (10,11,24), with some evidence suggesting a survival benefit after the administration of higher 131I-MIBG activities (11,12). For instance, Safford et al. observed significantly improved survival after the use of higher initial activities, that is, more than 14.8 GBq (400 mCi) of 131I-MIBG (median overall survival of 56 vs. 28 mo) (11). This finding may support dose escalation as a key augmentation for this treatment modality. However, there is no consensus regarding the most appropriate administered activity, and most studies have reported the use of a standard activity of 3.7–7.4 GBq (9,10,18). On the basis of the results presented here, especially with regard to safety and treatment outcome, we anticipate the application of higher activities per treatment cycle (>11.1 GBq [>300 mCi], which represented a pragmatic dose selection); dose escalation with conventional or extremely highly specific (no-carrier-added) 131I-MIBG has been successfully introduced in adults with metastatic pheochromocytoma and paraganglioma (12,33).
In agreement with previous reports, hematotoxicity was the primary side effect of 131I-MIBG therapy in the present study (1,10,24–26,34,35); this side effect was noted at a higher frequency (10%–20% per-patient incidence of grade 3 or 4) with the studied treatment regimen than with previously reported treatment regimens with lower single activities (23,24,26,27). However, it was of a transient nature in our cohort and triggered no hospitalization, granulocyte stimulation, or thrombocyte substitution, except in 1 patient with grade 4 thrombocytopenia (cumulative activity of 66.6 GBq). This side effect seems acceptable for the benefit of disease control. No apparent association between the cumulative dose, previous chemotherapy, or bone marrow involvement on the one hand and the incidence or severity of myelosuppression on the other hand was observed. In contrast, the results of previous studies suggested that these features were risk factors for more pronounced posttreatment myelosuppression (4,36–38).
The incidence of myelodysplastic syndrome in 1 patient after the administration of a high cumulative activity (66.6 GBq) highlighted this relatively uncommon delayed side effect of many antineoplastic treatments, including systemic chemotherapies and radionuclide therapies. The low incidence of myelodysplastic syndrome (<5%) may have been partly due to the limited prognosis of advanced NET not allowing this delayed sequela to manifest within the survival period. Other, nonhematologic toxicities were mild and confined to subacute gastrointestinal symptoms, such as nausea (28%) and vomiting (6%). These incidences were comparable to those reported by other groups for low-dose protocols (10,24,25) and therefore do not preclude the use of dose-intensified schemes. No other previously reported toxicities, such as liver failure (24,39), were seen in our cohort, even in patients with an extensive and infiltrative hepatic tumor burden. Also, renal impairment was not observed, in agreement with cumulative published clinical data.
Although PRRT with 177Lu- or 90Y-based compounds yields higher morphologic response rates in carcinoid tumors than 131I-MIBG therapy (29,40), renal safety remains a major advantage of 131I-MIBG. The present study showed that a regimen of 11.1 GBq (300 mCi) per treatment cycle was well tolerated and could be safely performed. We observed effective palliation of functionality-related symptoms of metastatic carcinoid tumors as well as disease stabilization with remarkable progression-free survival and overall survival. These results compare favorably with the results of previous reports on the response rates for various chemotherapy regimens (41–46). Because up to 85% of carcinoid tumors may display sufficient diagnostic 131I-MIBG uptake (47), tumor-targeted therapy with 131I-MIBG may be an effective alternative to PRRT for inoperable metastatic carcinoid tumors, especially in patients with renal impairment. The dual use of 131I-MIBG and radiolabeled somatostatin analogs to reduce treatment toxicity in such patients is another possibility to be investigated (48).
The general limitations of the present study were the relatively small patient cohort and the retrospective nature of the study. Unfortunately, biomarkers, such as urinary 5-hydroxyindoleacetic acid, that would support the response to treatment were not systematically assessed and therefore were not available for analysis. We were unable to correlate several factors, such as bone marrow involvement and morphologic or symptomatic responses, with survival because of the small number of patients. Furthermore, the assessment of survival depended on comparisons of epidemiological data in the absence of a control group.
CONCLUSION
The present study showed that 131I-MIBG therapy with a fixed dose of 11.1 GBq (300 mCi) per cycle was well tolerated, with toxicity mainly confined to transient myelosuppression. Despite the lack of significant regression of carcinoid tumors, the favorable survival outcome, efficient disease stabilization, and alleviation of symptoms make this treatment an attractive modality for use either as an adjunct or as an alternative to other existing therapeutic measures. Further increases in cycle activities (>11.1 GBq) seem to be worth evaluation in larger studies and may represent an important modification for improving efficacy and outcome.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 7, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 28, 2012.
- Accepted for publication May 29, 2013.





{kind=link}
{kind=link}