


Abstract
The purpose of this study was to evaluate the biodistribution of 11C-labeled methionine in non–tumor-involved organs in pediatric patients studied for malignant diseases. Methods: Ninety-three children and young adults with known or suspected malignancies underwent 11C-methionine PET and CT scans. Imaging began 5–15 min after injection of 740 MBq (20 mCi) per 1.7 m2 of body surface area. Images were acquired from the top of the head through the mid thighs. Standardized uptake values were determined using regions of interest drawn on the CT image and transferred to the corresponding transverse PET slice. Results: The highest concentrations of 11C-methionine were found in the pancreas and liver. Less intense uptake was seen in other regions, such as the salivary glands, tonsils, and bone marrow. There was little uptake in the lungs, fat (including brown adipose tissue), and muscle. Uptake in bone marrow, parotid glands, and tonsils was slightly but statistically significantly higher in men than women. Testicular, bone marrow, and left ventricular uptake increased with age. There was little variability statistically between comparisons of uptake change and groupings of age, race, sex, and patients studied at the time of diagnosis versus previously treated patients. Conclusion: High uptake of 11C-methionine is reliably found in the pancreas and liver, consistent with the anabolic functions of these organs. Low uptake in the brain, neck, chest, pelvis, and extremities will facilitate tumor localization in those areas. However, intense uptake in the upper abdomen may limit the diagnostic utility of 11C-methionine in that area.
The most commonly used radiotracer for the staging and monitoring of neoplastic disease is 18F-FDG (1). Elevated 18F-FDG uptake is common in many tumors, and 18F-FDG PET with CT is frequently used in the management of patients with lung tumors, lymphomas, melanomas, and others (2–4). However, there are limitations to its use. 18F-FDG uptake in brain tumors is complicated by intense background activity in the cerebral cortex, thus limiting its use in monitoring low-grade gliomas (5). In addition to central nervous system (CNS) tumors, 18F-FDG has limited utility for the study of bronchioloalveolar carcinomas, renal cell carcinomas, bladder tumors, prostate cancer, and others (6–8). 18F-FDG uptake is also a feature of some nonneoplastic conditions, such as inflammation and infection (9). Thus, new radiotracers are being developed to overcome the limitations and drawbacks of 18F-FDG in certain clinical conditions.
Methionine, a naturally occurring essential amino acid, can be labeled with the positron-emitting isotope 11C and studied using PET scanning. Methionine, which is transported into cells via the L-type amino acid transporter 1 (LAT1), is crucial for the formation of proteins and is involved in the synthesis of phospholipids. The formation of proteins is an integral part of cellular growth and replication. As cells replicate, the demand for protein and phospholipid synthesis increases, rendering transport and reclamation of essential amino acids crucial for tumor growth. Methionine has been found to accumulate in a variety of tumors (10–12). In particular, for non–small cell lung carcinomas, the uptake of methionine closely correlates with cellular replication (11). In gliomas, uptake of methionine correlates with both cellular proliferation and microvessel density (12).
The pharmacokinetics and dosimetry for 11C-methionine in adult humans have been reported by Deloar et al. (13) based on whole-body PET data. The pancreas, liver, bladder, and kidney showed the greatest initial uptake of 11C-methionine. The subjects in that study underwent scanning at multiple time points for calculation of dosimetry. The pancreas and liver had the highest retention of activity among the organs studied.
In this study, we examined the biodistribution of 11C-methionine in non–tumor-involved organs of young patients with newly diagnosed neoplasms and patients with secondary or recurrent neoplasms of childhood. Specifically, we examined methionine uptake variability across age, sex, and race. Uptake in organs not containing tumors was assessed and semiquantitatively evaluated to document the normal biodistribution of the tracer in children and young adults. We also compared uptake between patients with newly diagnosed malignancies who had not begun treatment and those who had recurrent tumors and were candidates for further antineoplastic therapy (radiation, chemotherapy, or both) for their primary malignant neoplasm. Patients with recurrent disease had not received therapy for at least 90 d.
MATERIALS AND METHODS
Patients
Patients (n = 93) with known or subsequently proven neoplastic disease were studied from July 2009 to July 2011. Demographic data are summarized in Table 1. Of 93 patients, there were 55 men (60%) and 38 women (40%). Ages ranged from 2 to 29 y (median, 12 y). Inclusion criteria for patient enrollment had no limits on age, sex, race, or type of diagnosis. Patients with newly diagnosed disease who had not yet undergone therapy (n = 62) and those with recurrent disease who had not received treatment in 3 or more months (n = 31) were included. Major diagnoses were CNS tumors (n = 43), sarcomas (n = 19), lymphomas (n = 8), carcinomas (n = 8), and others (n = 15, including Wilms tumors and neuroblastoma). Although many patients subsequently underwent multiple scans, only data from the baseline study were included. The St. Jude Children’s Research Hospital institutional review board approved this study, and all subjects or one or both of their parents signed a written informed consent document.
Patient Demographics Based on Sex, Race, and Status of Diagnosis
Radiochemistry
For this study, 11C-methionine was produced by the method of Ishiwata et al. (14), starting from 11C-methyl iodide and l-homocysteine thiolactone, and adapted for preparation on a PETChem Solutions automated synthesis module. This method has been shown to produce less than 3% d-11C-methionine. A detailed description of the radiochemistry is provided in Vavere and Snyder (15).
PET/CT Technique
Before imaging, participants fasted for at least 4 h. Patients were then given intravenous injections of 740 MBq (20 mCi) of 11C-methionine per 1.7 m2 of body surface area (maximum prescribed dose, 740 MBq). Transmission CT images, for attenuation correction and lesion localization, and PET images were acquired approximately 5–15 min later using a Discovery LS PET/CT system (GE Healthcare). CT acquisition parameters included the following: slice thickness, 0.5 cm; tube rotation, 0.8 s; table speed, 1.5 cm/rotation; pitch, 1.5:1; 120 kV; 90 mA, with dose modulation. PET images were obtained from the top of the skull through the mid thighs for 3 min per bed position in 2-dimensional mode. Data were reconstructed into multiplanar cross-sectional images using standard vendor-supplied software and displayed on a nuclear medicine workstation (Hermes Medical Solutions) for analysis.
Image and Data Analysis
Standardized uptake values (SUVs) for the structures listed in Table 2 were determined using regions of interest drawn on selected CT images and then transferred to the corresponding PET image in the transverse plane.
Complete List of Target Tissues/Organs Encompassed by Hand-Drawn Region of Interest
The number of selected regions of interest per patient varied slightly due in some cases to complete resection of a specific tissue or organ or due to organ involvement by diseased tissue. Table 2 accounts for this discrepancy and reports the actual number of data points used per selected tissue or organ and statistical analysis including minimum, first quartile, median, third quartile, and maximum SUV (SUVmax).
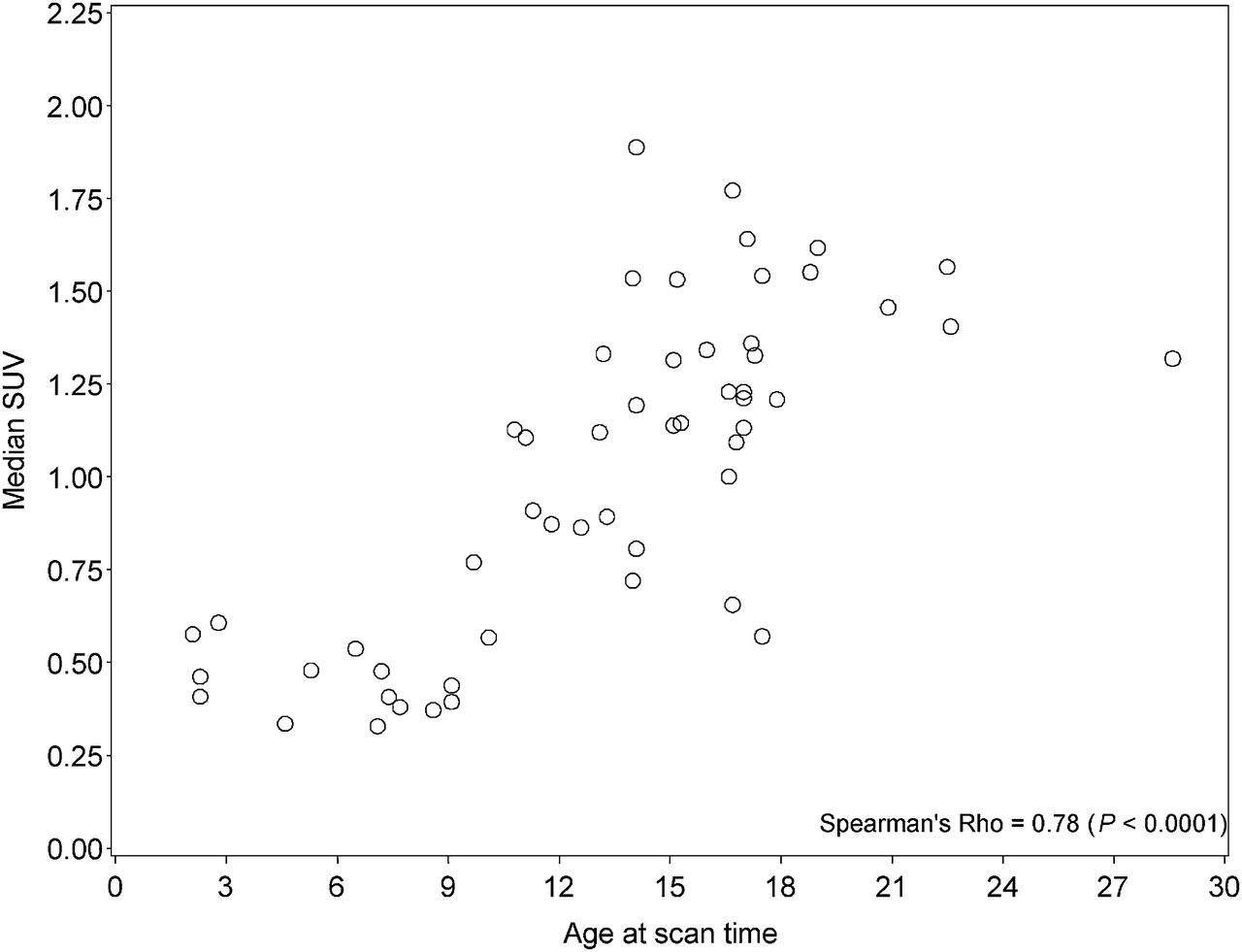
Graphical and descriptive statistics were used to display and compare methionine SUVmax data. The median SUV for a given region of interest was used for statistical analysis because this measurement is least affected by outliers. SUV distribution was statistically compared among subgroups of patients using the Wilcoxon–Mann–Whitney test, a nonparametric counterpart of the 2-sample t test. Comparisons of SUV by location, between right and left for paired organs, within sites for the lungs and vertebral bodies, between newly diagnosed patients and those with recurrent disease, and by age were performed. The association of age at scan time and SUV was investigated using Spearman rank correlation. Results were considered significant at a P value limit of 0.05 or less in a hypothesis-generating context, and the P values reported were not adjusted for multiplicity.
RESULTS
The highest accumulation of 11C-methionine was found in the pancreas and liver, both of which were readily recognizable as areas of prominent activity on emission images (Fig. 1; Table 2). The median SUVmax was 12.4 in the pancreas and 8.5 in the liver. There were no statistical differences between lobes of the liver or between pairs of other organs examined, including the tonsils, salivary glands, kidneys, and lungs (Figs. 1–⇓⇓⇓⇓6). Activity was evident in Waldeyer’s ring lymphoid tissue, submandibular glands, bone marrow, and kidneys. Activity was visually homogeneous in most organs. Intestinal uptake was quite variable in intensity, extent, and location and could not be quantified further because of the imprecision of localization on noncontrast, low-resolution CT scans.

SUVs for tissues examined. The group median (solid horizontal line in rectangular box), group mean (⋄ symbol), first and third quartiles above and below group median (rectangular box), and minimum and maximum SUV values (top and bottom horizontal lines) are depicted.
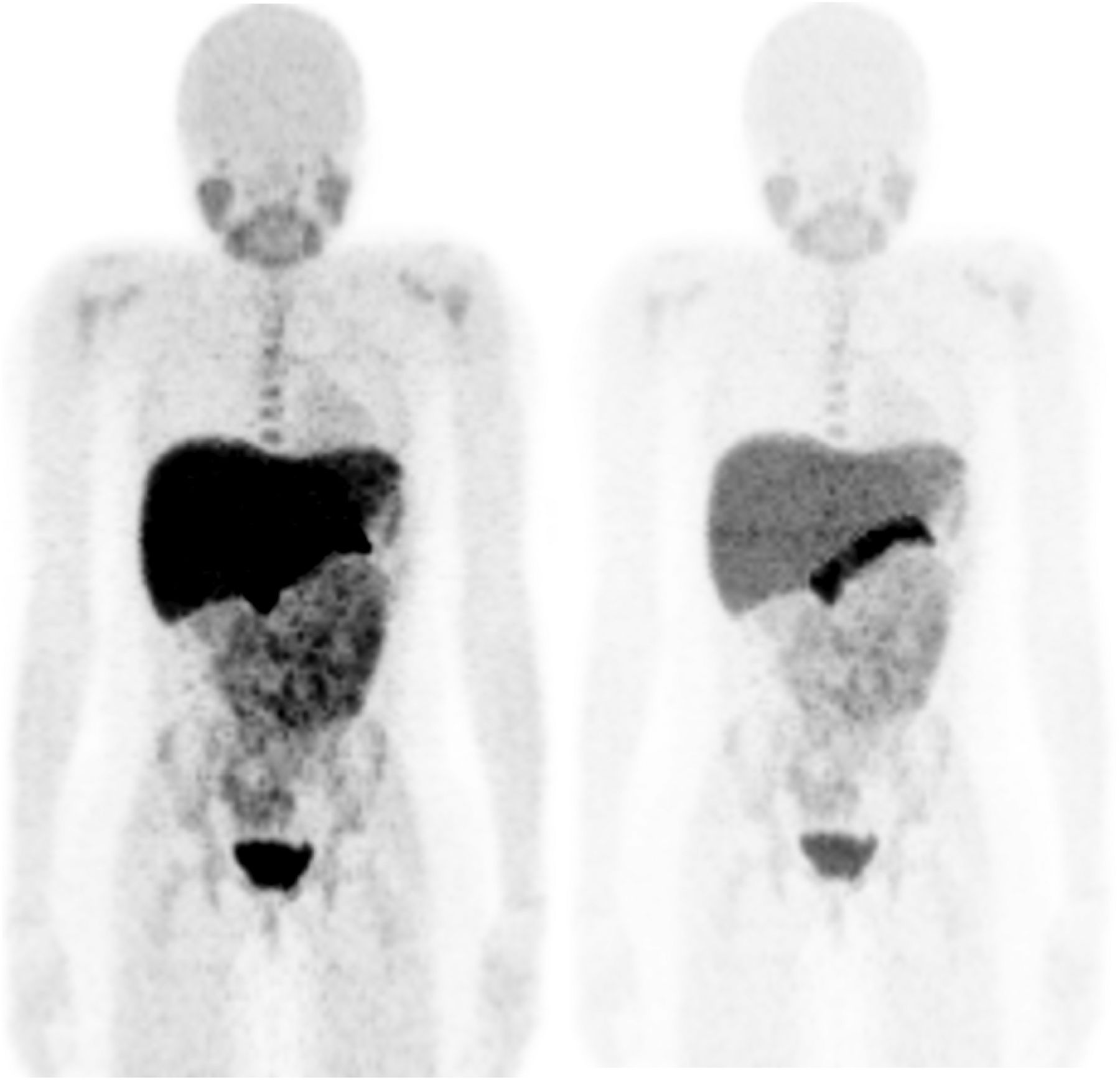
Whole-body anterior maximal intensity projection image of 7-y-old girl studied for cerebral neoplasm. Images are displayed at 2 different intensities to show relative distribution of tracer. Pancreas and liver contain highest concentrations.
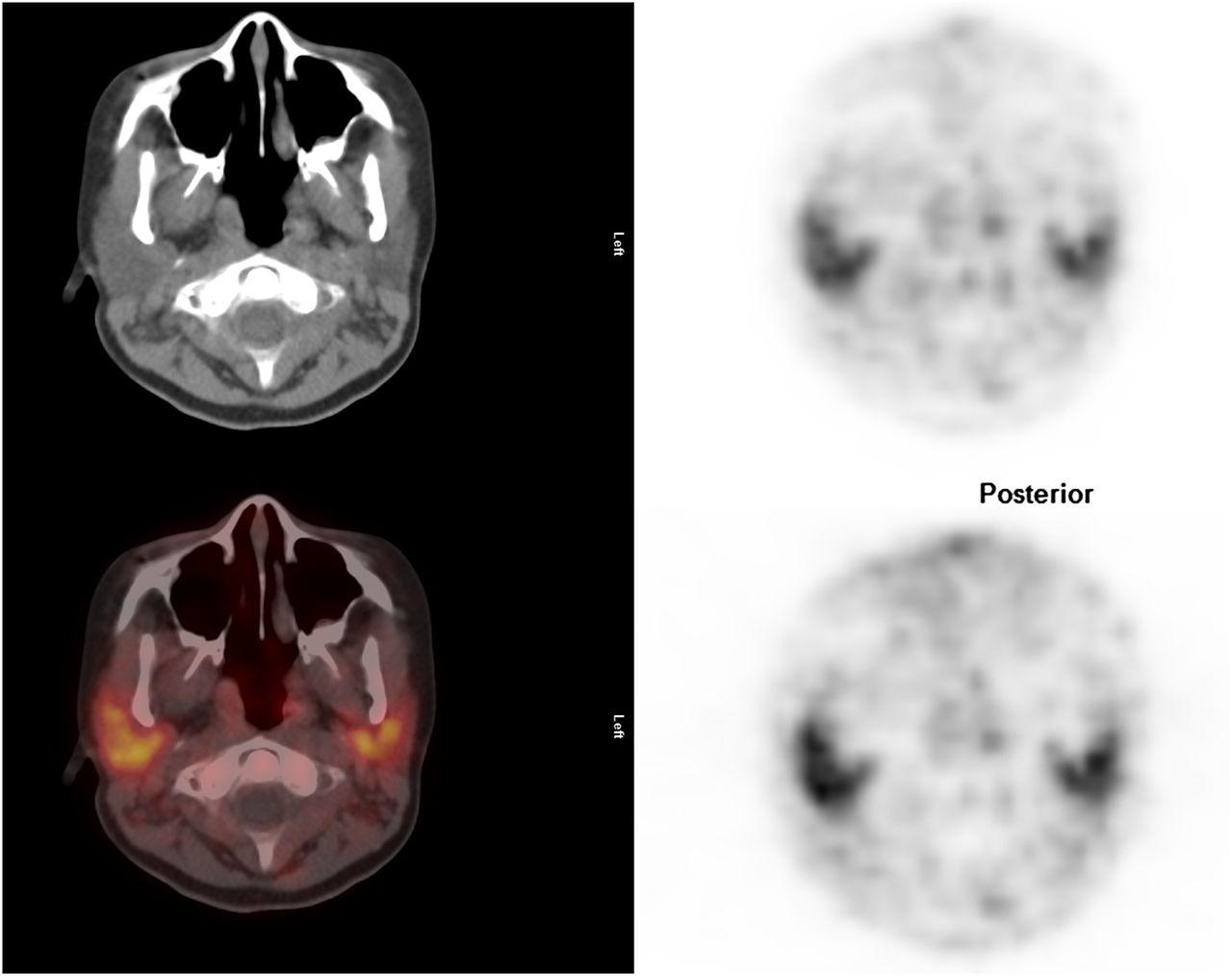
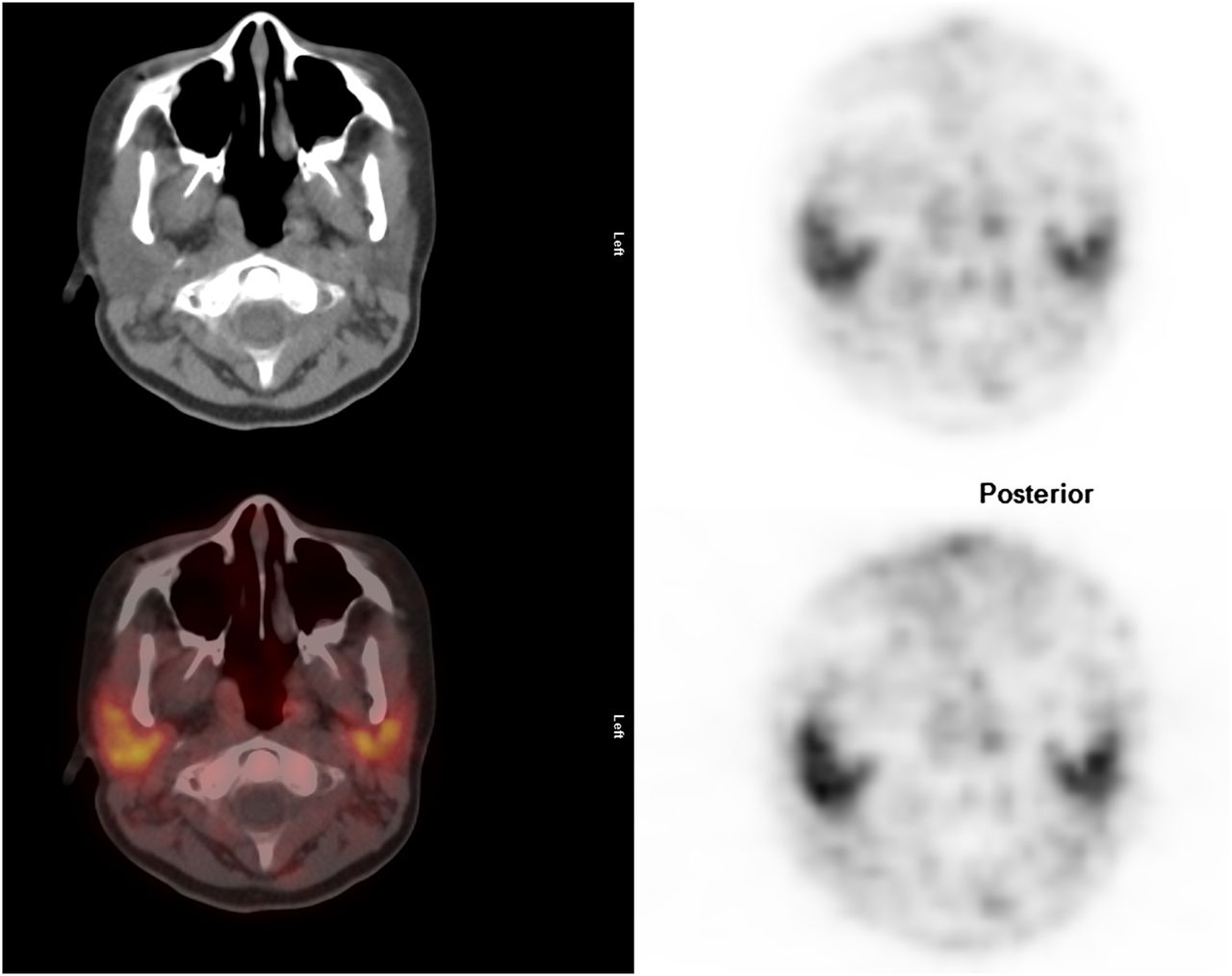
Image of neck; cross-sectional representations of activity seen at various levels of body: attenuation-correction CT scan (top left), attenuation-corrected PET image (top right), fusion image of CT and attenuation-corrected PET image (bottom left), and non–attenuation-corrected PET image (bottom right). Attenuation-corrected PET image is scaled to SUVmax of 5.0.
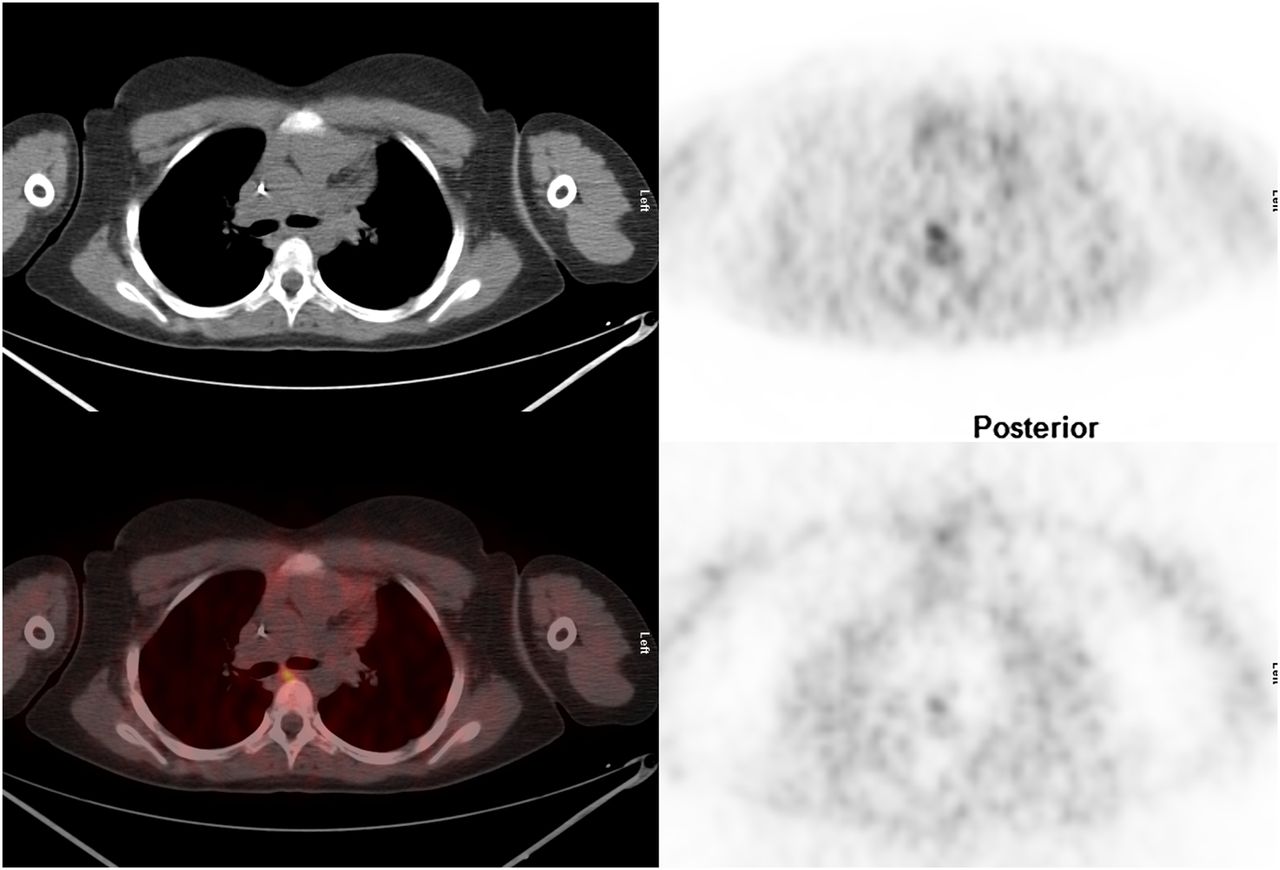
Image of mid chest; cross-sectional representations of activity seen at various levels of body: attenuation-correction CT scan (top left), attenuation-corrected PET image (top right), fusion image of CT and attenuation-corrected PET image (bottom left), and non–attenuation-corrected PET image (bottom right). Attenuation-corrected PET image is scaled to SUVmax of 5.0.
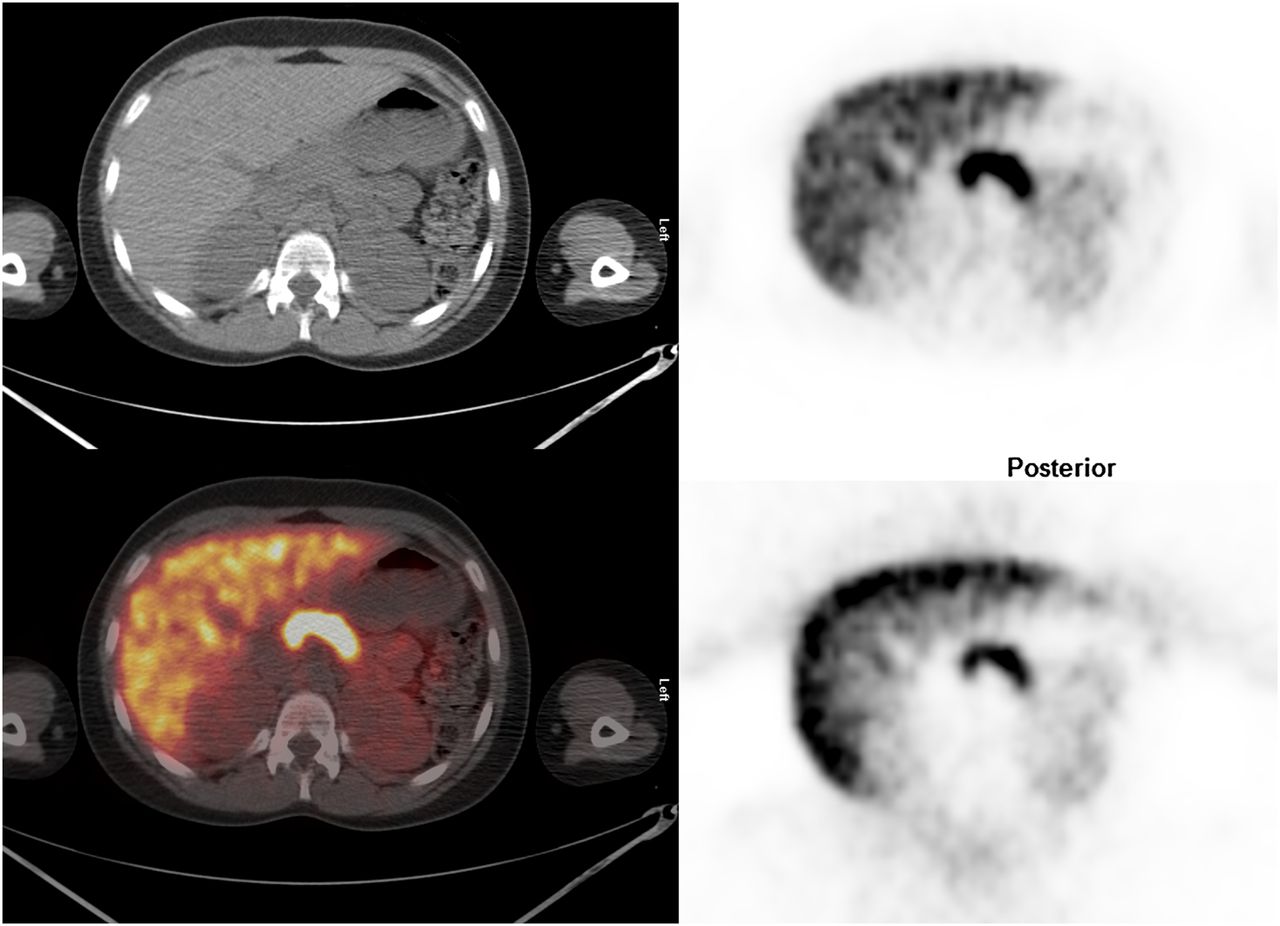
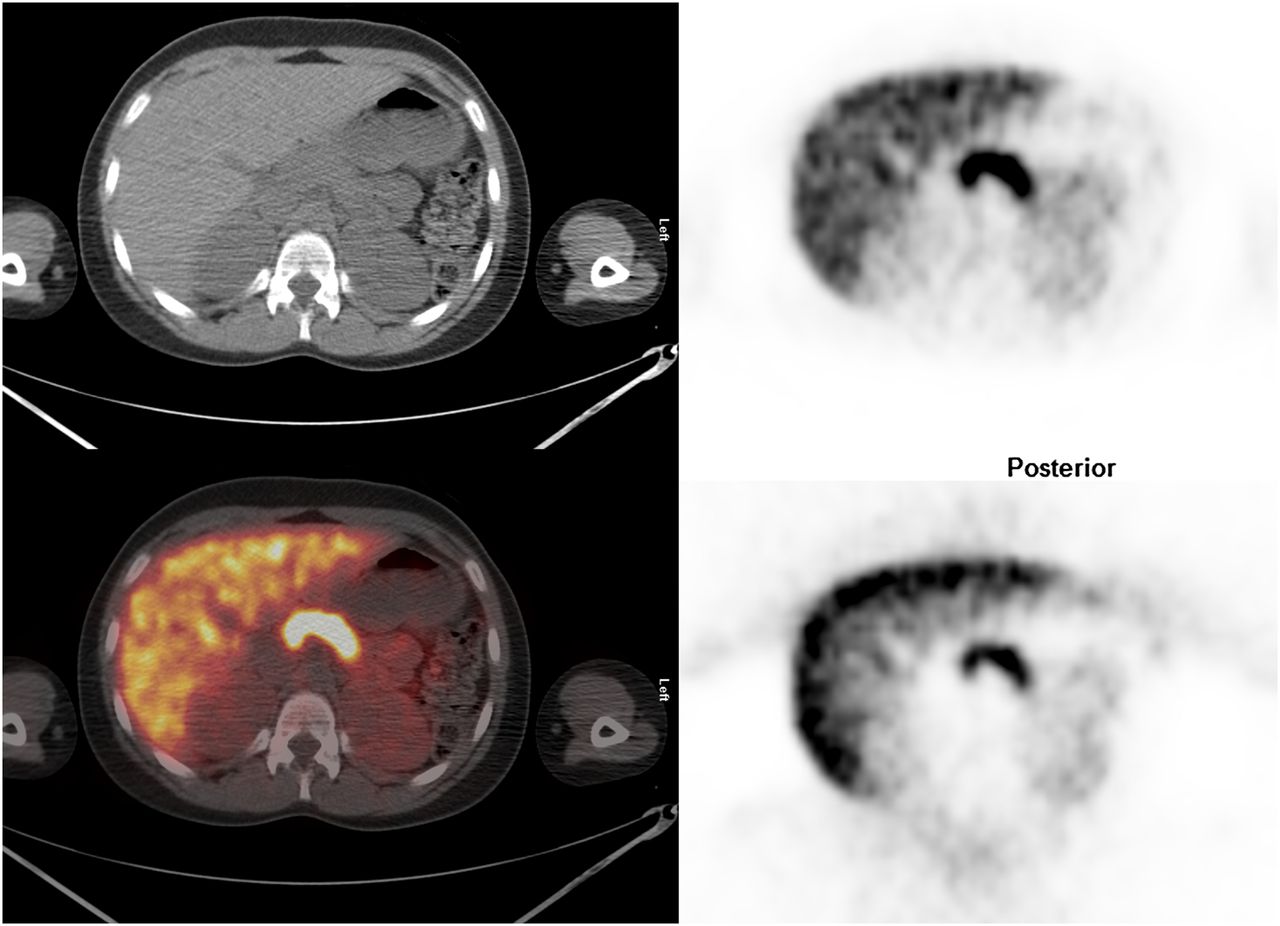
Image of mid abdomen; cross-sectional representations of activity seen at various levels of body: attenuation-correction CT scan (top left), attenuation-corrected PET image (top right), fusion image of CT and attenuation-corrected PET image (bottom left), and non–attenuation-corrected PET image (bottom right). Attenuation-corrected PET image is scaled to SUVmax of 12.

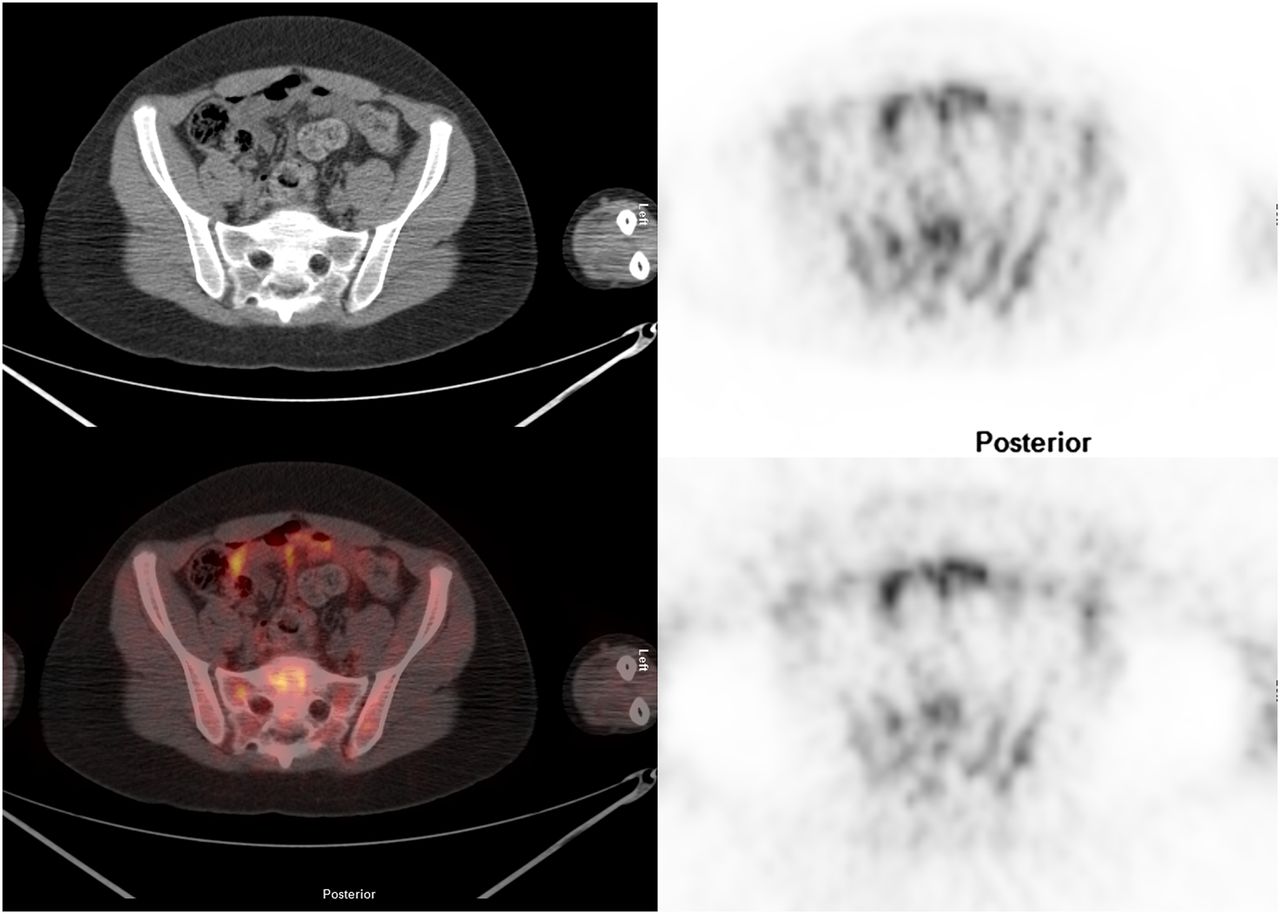
Image of pelvis; cross-sectional representations of activity seen at various levels of body. Attenuation-correction CT scan (top left), attenuation-corrected PET image (top right), fusion image of CT and attenuation-corrected PET image (bottom left), and non–attenuation-corrected PET image (bottom right). Attenuation-corrected PET image is scaled to SUVmax of 5.0.
Newly Diagnosed Versus Not Newly Diagnosed
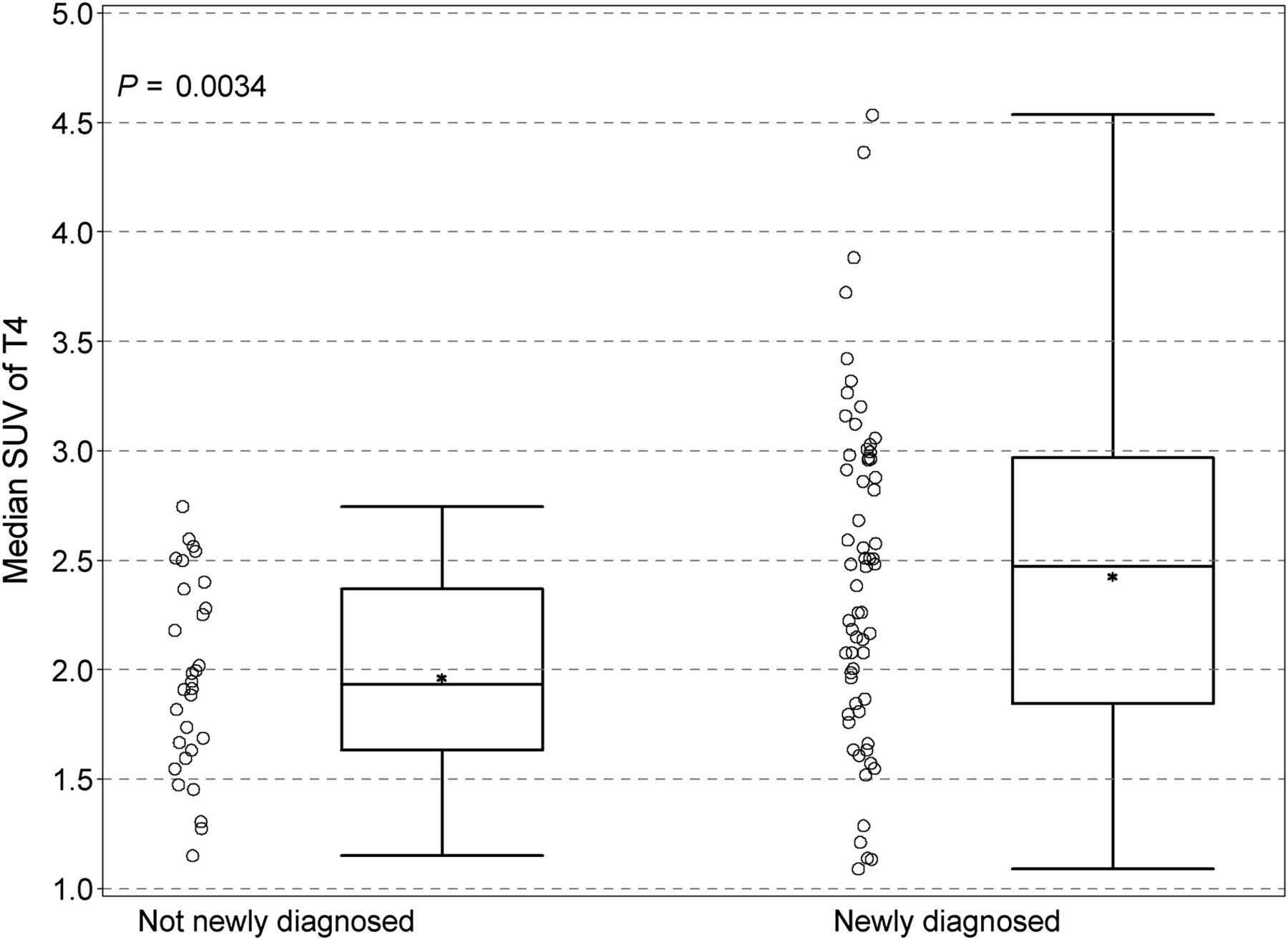
There were few and minor differences in biodistribution between patients with newly diagnosed disease and patients with previously treated disease. The uptake in T4 and T5 vertebral bodies in previously treated patients was slightly less (T4, median, 1.93 vs. 2.48, P = 0.0034; T5, median, 2.03 vs. 2.38, P = 0.0077) (Fig. 7) than in untreated patients. None of the differences in other regions reached a P value of 0.01, although the pattern for T6 (P = 0.06) was similar to that seen in T4 and T5.
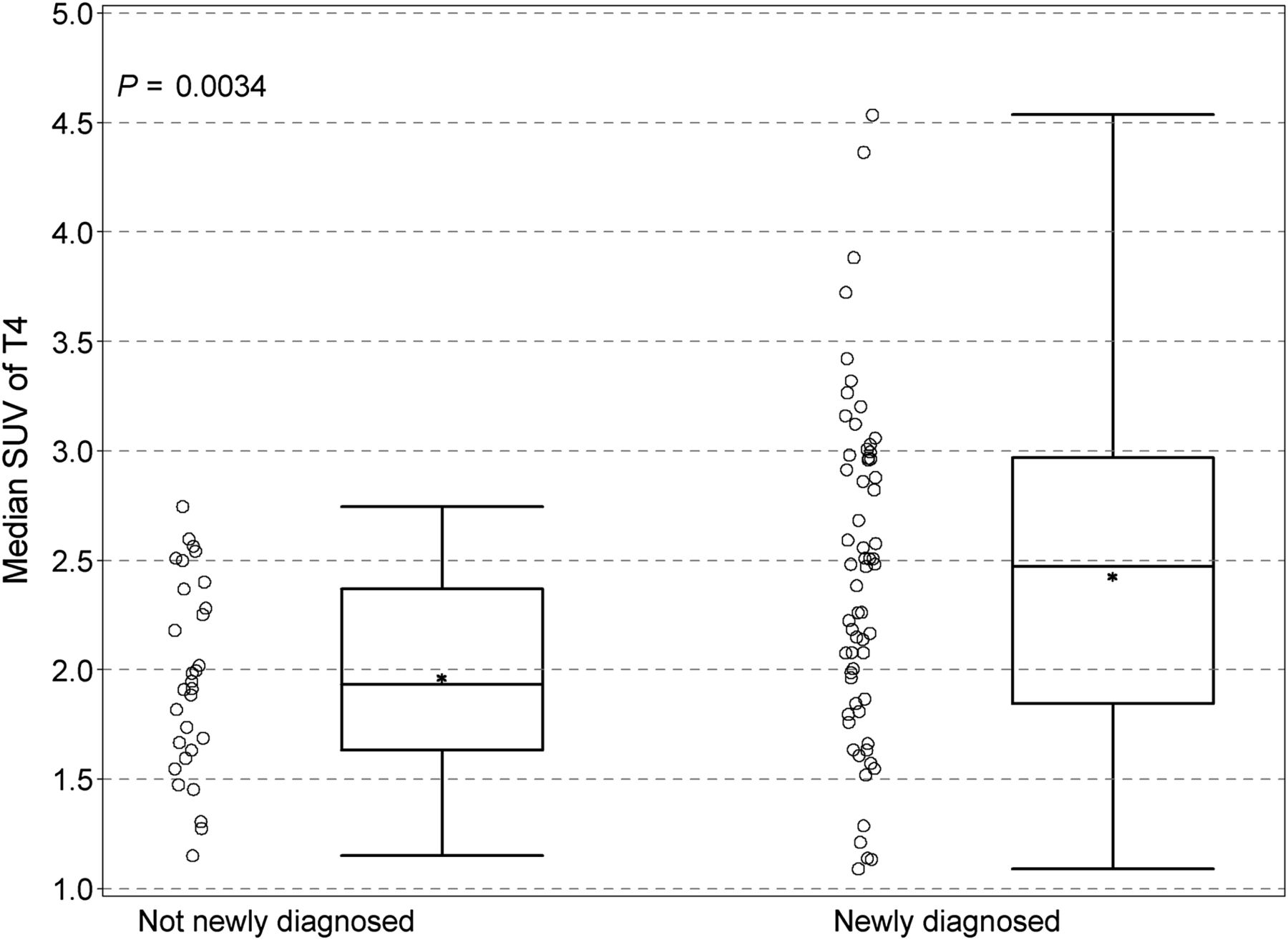
Comparison of SUV in T4 between previously treated patients and patients at initial diagnosis before therapy. Individual data points are depicted, along with group median (solid horizontal line in rectangular box), group mean (*), first and third quartiles above and below group median (rectangular box), and minimum SUV and SUVmax (top and bottom horizontal lines).
Sex Comparisons
Male and female patients compared by median SUV showed a modest number of statistically variant tissues and organs. In the tonsillar tissues of the Waldeyer ring and in the salivary glands (parotid and submandibular), uptake was greater in men than women (P values ranged from 0.0009 to 0.026). The vertebral bodies showed greater uptake in men than women, although only T10 and T5 were statistically significant (P = 0.0075 and 0.0079, respectively) (Fig. 8).

Comparison of uptake between women and men in T5. Slightly greater uptake in both median (*) and mean SUVmax was present in men. Individual data points are depicted, along with group median (solid horizontal line in rectangular box), the group mean (*), first and third quartiles above and below group median (rectangular box), and minimum and maximum SUV values (top and bottom horizontal lines).
Dosimetry
Dosimetry was calculated for age groups using data provided by the International Commission on Radiological Protection (Table 3) (16).
Administered Activity (MBq), Effective Dose Equivalent (mSv), and Organ Radiation Doses (mGy) for 11C-Methionine
Age Comparisons
The uptake in many regions increased slightly with age. These areas included the testicles (P < 0.0001) (Fig. 9), the liver (P < 0.0001), the left ventricular myocardium (P = 0.0002), and multiple vertebral bodies.
Testicular uptake as function of age. Individual data points are shown.
DISCUSSION
In our study of pediatric patients undergoing 11C-methionine studies for malignancies, the pancreas and liver consistently showed the greatest uptake of 11C-methionine. This is similar to the findings of Deloar et al. (13), who described high uptake and retention of 11C-methionine in the pancreas and liver of 5 adult healthy volunteers. The exocrine pancreas produces enzymes, such as trypsin and chymotrypsin, for the breakdown of ingested proteins, fats, and carbohydrates. Similarly, the liver requires amino acids for the synthesis of plasma proteins, such as albumin, fibrinogen, and transferrin. Thus, the high uptake in both these organs may reflect the need for methionine and other large neutral amino acids for protein synthesis.
Among the tissues and organs analyzed for 11C-methionine uptake, bone marrow in the axial skeleton was consistently prominent. This is likely due to the demand for protein synthesis in the replicating cells in the bone marrow. The vertebral bodies analyzed showed small but statistically significant differences based on age, sex, and newly diagnosed versus not newly diagnosed disease. This finding suggests that axial bone marrow uptake increases slightly with age and is slightly greater in men than women. The small differences between patients who had been treated and not treated may reflect a slight decline in bone marrow reserve in patients who have been previously exposed to a variety of antineoplastic agents.
The left ventricle had greater uptake in men than in women. In addition, uptake in the left ventricle increased over time. This increase could be due to a greater average body mass in men than in women and an increase in body mass over time. Methionine increases contractility of the heart by N-methlylation of membrane phospholipids of the sarcoplasmic reticulum and sarcolemma (17). The parotid glands showed a pattern of uptake similar to that in the left ventricle for sex and age, although the changes were quite small.
The data on biodistribution of 11C-methionine in adult patients are limited principally to analysis of tumor uptake. Nonetheless some nontumor organ uptake has been described.
The median SUVmax in T11 of our patients, 2.0, was similar to the mean SUVmax of T11 in 10 adult control patients with hyperparathyroidism, 1.8 ± 0.3 (18). These values are lower than the vertebral body uptake described by Nettelbladt (19). In that study, vertebral body uptake was 4.2 ± 1.3 in 17 patients with lung and mediastinal tumors. Liver uptake in our study (SUVmax, ∼8.5 averaging both lobes) was lower than that in the study of Nettelbladt et al. (SUVmax, 11.2 ± 2.2) and lower than that found in a study of 10 patients with malignant melanoma (12.6 ± 3.6; 4 patients had only liver measurements) (20). In the latter study, salivary gland uptake was 5.9 ± 1.3 (3 patients), compared with our findings of approximately 3.0 for submandibular glands and 2.5 for parotid glands. Lung uptake in the study of Nettelbladt et al. (19), 0.6 ± 0.1, was quite close to the 0.6–0.7 found in our study.
There were limitations to our study. For practical reasons, scanning was performed at only a single time point after injection; thus, dynamic organ uptake and retention could not be assessed. The time to the start of body imaging in patients also studied for CNS disease was longer than in those studied for extracranial involvement because the body imaging occurred after a dedicated brain study. However, Deloar et al. (13) showed that the uptake of methionine occurs quite quickly and that the decline in activity over time was due to physical decay. Thus, the retention of tracer was quite high with little efflux during the time of imaging, indicating that the small differences in the time intervals from injection to imaging should not affect our results. Intrasubject reproducibility could not be assessed for practical and ethical concerns of scheduling and performing repeated scans before initiation of further treatment.
The calculated dosimetry (Table 3) shows that the effective dose equivalent ranged from 5.8 to 6.9 mSv. The target organ is the bladder wall, followed by the kidneys, pancreas, and liver. The bladder contributes 65% of effective dose equivalent (16). The calculated value for the bladder wall, 81 mSv for an adult, may represent a considerable overestimation of absorbed dose, as the data of Deloar indicate a value of 20 mSv. Newer scanners with 3-dimensional acquisition and other features of modern PET/CT cameras may allow dose reduction yet preserve or enhance image quality. Fluid administration to promote diuresis, early voiding, or bladder catheterization may also reduce bladder and thereby patient exposure.
The principal tumors studied with 11C-methionine have been CNS neoplasms, which have been studied for more than 20 y. Unlike with 18F-FDG, which is normally concentrated within the brain, particularly cerebral gray matter, the brain shows little uptake of 11C-methionine under normal circumstances (21). O’Tuama et al. (22) examined 13 children, ages 1.8–15.8 y, with brain tumors using 11C-methionine. This was the first documented report of 11C-methionine in childhood brain tumors. Increased 11C-methionine was found in the tumors of 11 of the 13 patients. Other studies have also shown utility for 11C-methionine for the study of childhood and adult brain tumors (23–25). The regional uptake of 11C-methionine in normal brain tissue has been described by Coope et al. (26). The highest uptake was found in the cerebellum and occipital cortex, with less in white matter. The study of Nagata also showed high uptake in the cerebellum of healthy children and increasing SUV in the frontal lobes and cerebellum with age (27).
Non-CNS tumors have been studied less extensively. These include bronchogenic carcinomas, melanomas, multiple myeloma, colorectal carcinomas, hepatomas, ovarian and uterine tumors, and bladder and prostate carcinomas (18–20,28–30). Parathyroid adenomas have been successfully localized using 11C-methionine (31).
Methionine, along with other neutral amino acids that have large, branched, or aromatic side chains—such as leucine, isoleucine, phenylalanine, tyrosine, histidine, tryptophan, and valine—are transported into cells by LAT1 (32). LAT1 is Na+-independent and functions as an amino acid exchanger (33). It consists of 507 amino acids with a molecular weight of approximately 55 kDa and 12 transmembrane-spanning nonglycoproteins (34,35). LAT1 is also the transporter for amino acid–related molecules such as l-dopa, thyroxine, and triiodothyronine and the chemotherapeutic agent melphalan (l-phenylalanine mustard) (36). LAT1 is found in the brain, placenta, and liver, and it is overexpressed in many types of tumors (33,37–40), including gliomas, gastric carcinomas, non–small cell carcinomas of the lungs, and esophageal carcinoma. Inhibition of LAT1 has been reported to have antitumor activity in vitro and in vivo (35). If effective therapies using LAT1 inhibitors are developed, it is possible that 11C-methionine could serve as a method to assess antitumor efficacy.
CONCLUSION
We have explored the biodistribution of 11C-methionine in non–tumor-involved organs in children and young adults with known or suspected malignancies. The high uptake within the pancreas and liver suggests that their background activity may impair the search for neoplasms in the abdomen. Relatively low uptake of this agent in brain tissue facilitates tumor localization in the brain. Low background in the neck, chest, and extremities will likely facilitate tumor localization in those regions.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The researchers were supported by 5R25CA023944 from the National Cancer Institute (NCI) and by generous support from the American Lebanese Syrian Associated Charities (ALSAC). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Sandra Gaither for secretarial expertise and David Galloway of Scientific Editing for editorial support. We are grateful to the Molecular Imaging Research laboratory staff for production of 11C-methionine.
Footnotes
Published online Sep. 19, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 13, 2012.
- Accepted for publication May 17, 2013.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nononcologic Applications of PET/CT and PET/MRI in Musculoskeletal, Orthopedic, and Rheumatologic Imaging: General Considerations, Techniques, and Radiopharmaceuticals
- Comparison of 11C-Methionine and 18F-FDG PET/CT for Staging and Follow-up of Pediatric Lymphoma
- Anti-1-Amino-3-18F-Fluorocyclobutane-1-Carboxylic Acid: Physiologic Uptake Patterns, Incidental Findings, and Variants That May Simulate Disease