


Abstract
This study aimed to assess the role of a quantitative dynamic PET model in pancreatic cancer as a potential index of tumor aggressiveness and predictor of survival. Methods: Seventy-one patients with 18F-FDG–avid adenocarcinoma of the pancreas before treatment were recruited, including 27 with localized tumors (11 underwent pancreatectomy, and 16 had localized nonresectable tumors) and 44 with metastatic disease. Dynamic 18F-FDG PET images were acquired over a 60-min period, followed by a whole-body PET/CT study. Quantitative data measurements were based on a 2-compartment model, and the following variables were calculated: VB (fractional blood volume in target area), K1 and k2 (kinetic membrane transport parameters), k3 and k4 (intracellular 18F-FDG phosphorylation and dephosphorylation parameters, respectively), and 18F-FDG INF (global 18F-FDG influx). Results: The single significant variable for overall survival (OS) in patients with localized disease was 18F-FDG INF. Patients with a high 18F-FDG INF (>0.033 min−1) had a median OS of 6 and 5 mo for nonresectable and resected tumors, respectively, versus 15 and 19 mo for a low 18F-FDG INF in nonresectable and resected tumors, respectively (P < 0.04). In metastatic disease, multivariate analysis found VB, K1, and k3 to be significant variables for OS (P < 0.043, <0.031, and <0.009, respectively). Prognostic factors for OS in the entire group of patients that were significant at multivariate analysis were stage of disease, VB, K1, and 18F-FDG INF (P < 0.00035, <0.03, <0.024, and <0.008, respectively). Median OS for all patients with a high 18F-FDG INF, low VB, and high K1 was 3 mo, as opposed to 14 mo in patients with a low 18F-FDG INF, high VB, and low K1 (P < 0.021), irrespective of stage and resectability. Conclusion: Quantitative 18F-FDG kinetic parameters measured by dynamic PET in newly diagnosed pancreatic cancer correlated with the aggressiveness of disease. The 18F-FDG INF was the single most significant variable for OS in patients with localized disease, whether resectable or not.
Pancreatic cancer (PC) is the tenth most common malignancy and the fourth leading cause of cancer death in the United States, with 1- and 5-y survival rates of 26% and 6%, respectively, for all stages combined and of only 23% at 5 y in patients with local disease. At presentation, less than 20% of patients are candidates for surgery, with the remainder having either locally advanced nonresectable or metastatic disease (1).
Patients with the same stage of PC exhibit variable clinical behavior. Although most patients with early-stage disease amenable to pancreatectomy will have further locoregional or metastatic failure, 20% of them will enjoy long-term survival. Histopathologic factors including tumors larger than 2 cm, moderate to poor histology grade, positive resection margins, and lymph node involvement are associated with shorter survival (2). Defining the aggressiveness of PC before surgery is a clinical challenge. If this challenge can be met, it may enable identification of subgroups of resectable tumors with different prognoses and prediction of the need for and efficacy of surgery and neoadjuvant or adjuvant therapy. Locally advanced nonresectable PC can show rapid progression during treatment or, alternatively, a response sufficient to warrant exploration and resection of the tumor. Furthermore, a small subgroup of patients with metastatic PC has been reported to have prolonged survival after treatment with gemcitabine (3). These differences in response and survival provide evidence for the heterogeneity of PC and for the clinical importance of accurate risk stratification and subsequent tailored treatment in patients with advanced disease as well.
18F-FDG PET/CT has an established role in the work-up of various malignancies. The metabolic activity of a tumor, expressed by the degree of 18F-FDG uptake, is assessed using visual parameters of presence, size, and intensity of tracer uptake or using semiquantitative measurements of the standardized uptake value (SUV), prone, however, to variability (4).
Uptake of 18F-FDG is the result of a dynamic process. A dynamic 18F-FDG PET protocol for quantitative analysis using kinetic modeling has been previously described (5–11). These studies have assessed the value of kinetic PET parameters in the differential diagnosis of benign versus malignant lesions and for evaluating response to treatment and survival in colorectal carcinoma, soft-tissue sarcomas, and multiple myeloma (6–10).
The working hypothesis of the current study assumes that 18F-FDG kinetics quantitation may define tumor aggressiveness and predict prognosis in clinically heterogeneous malignancies such as PC, with a potential impact on individual treatment tailoring. The present study aimed to assess whether dynamic 18F-FDG PET/CT parameters can be used as prognostic tools in PC.
MATERIALS AND METHODS
Study Population
Seventy-one patients with adenocarcinoma of the pancreas who had not yet been treated were recruited between September 2006 and April 2009 (Table 1). There were 40 men and 31 women, with a median age of 68 y (range, 39–79 y). Twenty-seven patients had localized disease, including 11 patients who underwent pancreatectomy (followed by adjuvant chemotherapy and chemoradiation in 1 patient each, whereas 9 patients were followed up only), and 16 patients had locally advanced nonresectable PC (14 received gemcitabine-based chemotherapy, with radiation therapy added in 7). Forty-four patients had disseminated disease, 5 with single and 39 with 2 or more metastases, and were treated with single-agent gemcitabine or with gemcitabine and cisplatin in combination.
Clinical Characteristics of 71 Patients with PC
The study was approved by the institutional ethical (Helsinki) committee. All patients signed an informed consent form.
Imaging Protocol
Patients fasted for 4 h before the administration of 18F-FDG except for glucose-free hydration. Dynamic PET was started with the intravenous administration of 370–555 MBq of 18F-FDG for a single field of view (FOV) over the upper abdomen to include the pancreas for a total acquisition time of 60 min, including a 28-frame series acquired at 4 intervals: 10 × 30 s/frame, 5 × 60 s/frame, 5 × 120 s/frame, and 8 × 300 s/frame.
After the completion of this research protocol, oral contrast material was administered. A whole-body PET/CT acquisition study started 2 h after radiotracer injection using the routine protocol including 5–7 FOVs and 4 min/FOV, for a total acquisition time of 20–28 min.
The study was performed using a PET/CT device (Discovery LS; GE Healthcare) starting with a CT acquisition, followed by a PET study of the same axial range. PET images were reconstructed using ordered-subset expectation maximization software, with CT attenuation correction. PET, CT, and fused PET/CT images were reviewed in axial, coronal, and sagittal planes on the Xeleris workstation (GE Healthcare).
Dynamic PET data analysis was performed using the PMOD software package (PMOD Technologies Ltd.).
Data Processing and Analysis
For the quantitative evaluation, irregular volumes of interest (VOIs) consisting of several regions of interest were drawn manually in target areas over the tumor and over a large artery within the FOV. Parametric tumor images were calculated on the dynamic PET data, fitting a linear regression function to time–activity data for each voxel (11). Tracer kinetics were assessed using the standard 2-tissue-compartment model methodology (12). The accurate input function measurement, which theoretically requires arterial blood sampling, is retrieved with this protocol, from the mean arterial VOI values with previously demonstrated good accuracy (13). The arterial VOI consisted of at least 7 ROIs defined on sequential PET images. The descending aorta was preferentially used because it can be easily defined on the dynamic image sequence and because of low spill-over from other organs. A preprocessing PMOD tool allowed a fit of the input curve by a sum of up to 3 decaying exponentials to reduce the noise that could otherwise affect parameter estimates.
The transport constant K1 and rate constants k2, k3, and k4 were calculated using a 2-compartment model implemented in PMOD considering the vascular fraction (VB) in a VOI as an additional variable (11). The model parameters were accepted when VB was between 0 and 1 and K1–k4 were less than 1 (as required by the model convergence). Rate constants K1–k4 are expressed in 1/min. VB reflects the fraction of blood within the evaluated volume. After compartment analysis, the global influx of 18F-FDG (18F-FDG INF) was calculated from the compartment data as (K1 × k3)/(k2 + k3).
A noncompartment model based on the fractal dimension (FD) was also used. FD is a parameter of heterogeneity and was calculated for the time–activity data in each individual voxel of a VOI. FD values vary between 0 and 2, representing the deterministic or chaotic tracer activity distribution (14).
Whole-body 18F-FDG PET/CT was analyzed visually by an experienced nuclear medicine physician with knowledge of the patient’s clinical history and the report of previously performed CT. Areas of focal increased 18F-FDG activity that could not be assigned to physiologic radiotracer distribution or benign processes were defined as malignant. 18F-FDG avidity in the primary pancreatic tumor and metastases was recorded as 18F-FDG–positive or 18F-FDG–negative. Semiquantitative maximum SUV assessment of the intensity of 18F-FDG uptake was measured twice: on the last frame of the dynamic study (SUV1) and on the whole-body study (SUV2) measured 2 h after injection, using the same region of interest surrounding the tracer-avid tumor.
Statistical Analysis
The relationship between kinetic parameters, clinical and histopathologic risk factors, and overall survival (OS) was assessed for the whole group with PC and for subgroups with localized and metastatic disease.
Univariate analysis was performed for the following variables: for the whole study group—patient age, tumor stage, location in pancreas, and differentiation; for patients with localized disease who underwent pancreatectomy—tumor size, margins, lymph node status, and adjuvant therapy; and for patients with metastatic disease—extension to one or more sites of malignancy. PET-related variables included VB, K1, k2, k3, k4, 18F-FDG INF from the compartmental analysis, FD from the fractal dimension analysis, SUV1, and SUV2.
Multivariate Cox proportional hazards regression analysis was performed only on variables with a P value of less than 0.2 on univariate analysis. The significant variables on multivariate analysis were plotted on Kaplan–Meyer curves with a cutoff value established by receiver-operating-characteristic analysis as a discriminator. The statistical analysis of survival curves used the log rank test, and statistical evaluation was performed using the MedCalc (MedCalc) and GraphPad software (GraphPad Inc.).
RESULTS
Univariate survival analysis of clinical–pathologic and kinetic PET parameters in the study group is shown in Tables 2 and 3, and multivariate analysis of the significant variables is shown in Table 4.
Univariate Survival Analysis of Clinical and Pathologic Parameters
Univariate Survival Analysis of Parameters Measured by 18F-FDG PET
Cox Multivariate Survival Analysis of Significant Clinicopathologic and Kinetic 18F-FDG PET Variables
Localized PC
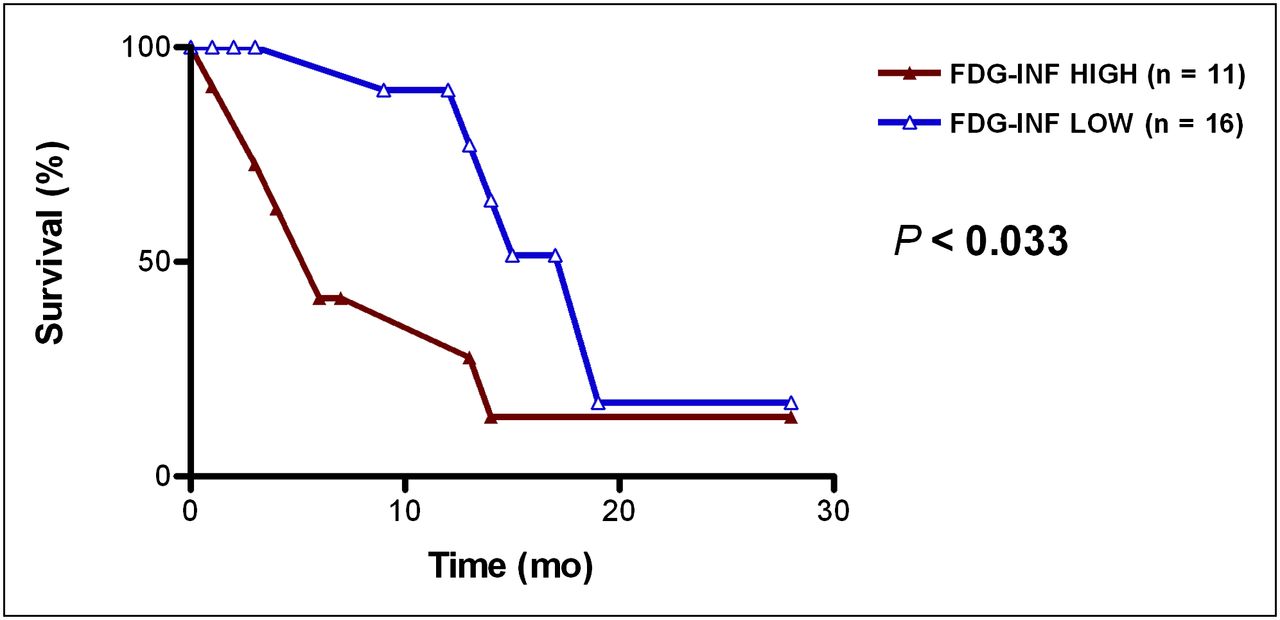
Median OS for 27 patients with localized disease was 14 mo, with no difference between resected and nonresectable disease. Prognosticators of OS by univariate analysis, to be included in the multivariate analysis, were VB, K1, FD, 18F-FDG INF, and SUV2. Multivariate analysis found 18F-FDG INF as the only significant variable for OS (P < 0.0092). Patients with a high and low 18F-FDG INF (above and below 0.033, respectively) had a median OS of 6 and 19 mo, respectively (P < 0.033; Fig. 1).

OS curves for patients with localized PC with high and low 18F-FDG INF.
In 11 patients who underwent pancreatectomy, univariate analysis found lymph node status, adjuvant therapy, VB, K1, k2, FD, 18F-FDG INF, SUV1, and SUV2 as prognosticators of OS, and these parameters were further included in the multivariate analysis. Multivariate analysis found 18F-FDG INF as the only significant variable for OS (P < 0.046). Patients with a high (n = 5) and low (n = 6) 18F-FDG INF (above and below the value of 0.026, respectively) had a median OS of 6 and 19 mo, respectively (P < 0.032).
In 16 patients with locally advanced unresectable disease, univariate analysis prognosticators for OS included tumor location, FD, and 18F-FDG INF. Multivariate analysis found tumor location and 18F-FDG INF to be significant variables for OS (P = 0.019 and 0.016, respectively). Patients with a high and low 18F-FDG INF (above and below the value of 0.042, respectively) had a median OS of 6 and 15 mo, respectively (P < 0.005). Median OS was 13 and 2 mo in patients with tumor in the pancreatic head and other locations, respectively (P < 0.04).
For the whole group with localized disease, the 18F-FDG INF cutoff value of 0.033 predicted a median OS of 5, 6, 15, and 19 mo for patients with resected high 18F-FDG INF, nonresectable high 18F-FDG INF, nonresectable low 18F-FDG INF, and resected low 18F-FDG INF, respectively (P < 0.041; Fig. 2). Examples of the relationship between OS and 18F-FDG tumor uptake kinetic curves used for the calculation of 18F-FDG INF are displayed in Figure 3.
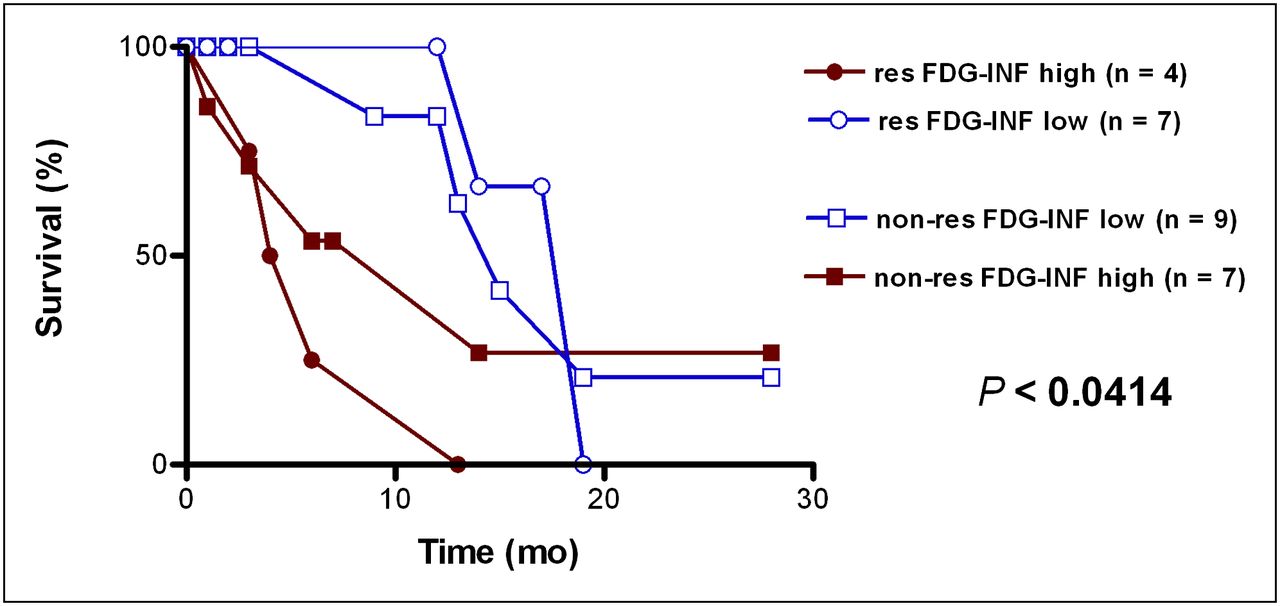
Overall survival curves for patients with resected and nonresectable PC with high and low 18F-FDG INF. P value displayed is calculated on all curves from log-rank analysis. non-res = nonresectable; res = resectable.
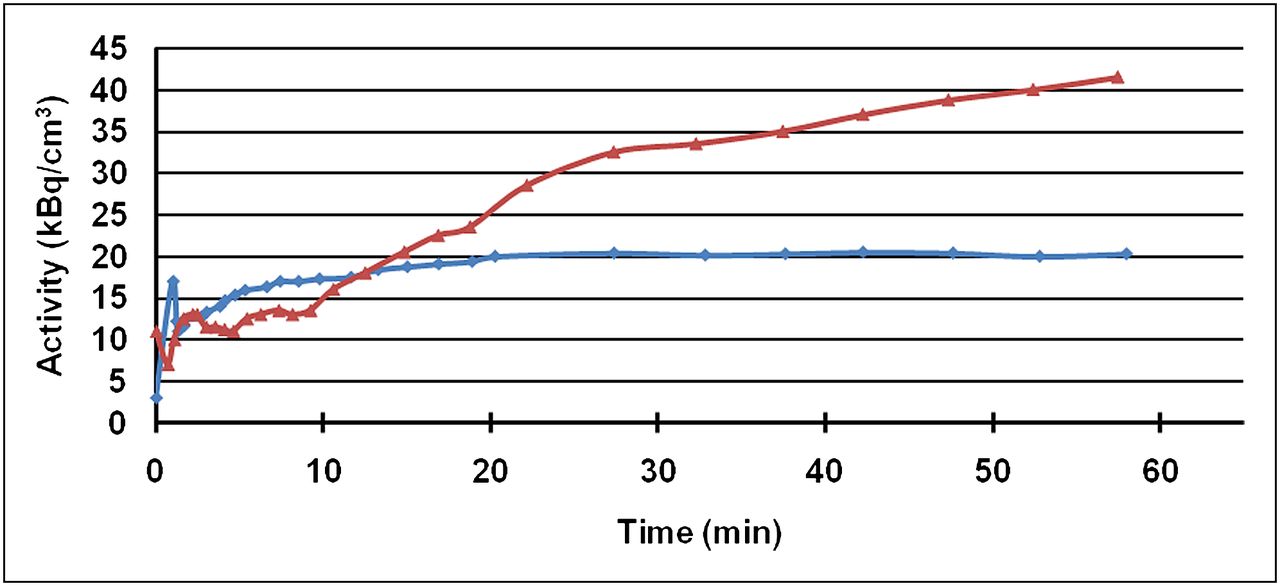
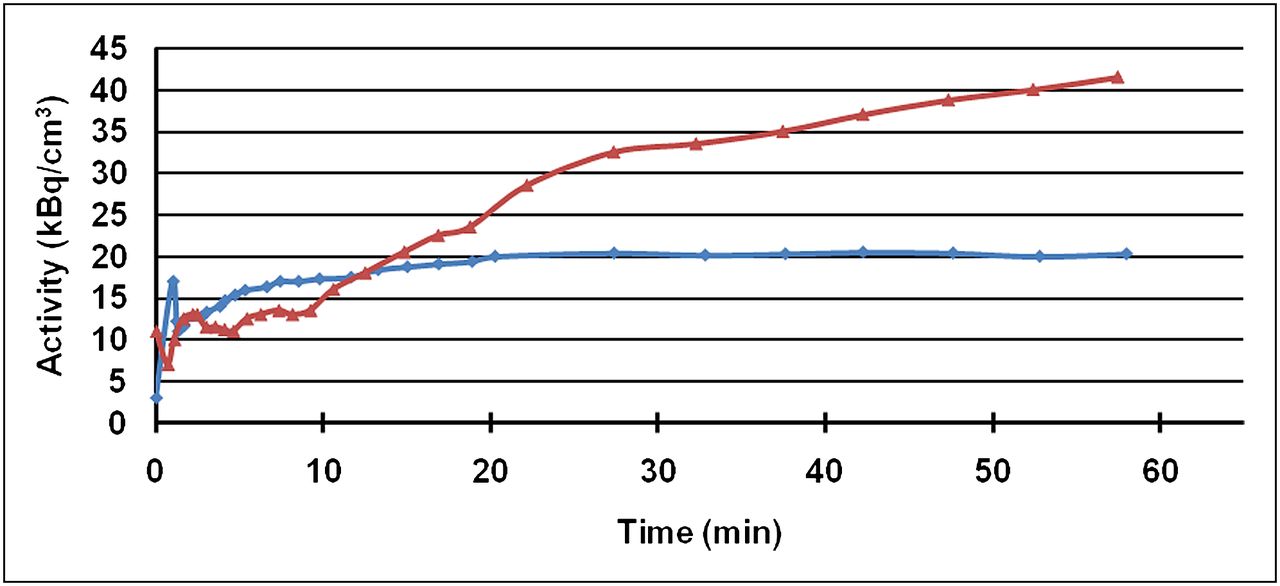
Examples of relationship between OS and 18F-FDG tumor uptake kinetic curves used for calculation of 18F-FDG INF. Blue curve = patient with OS of 19 mo and 18F-FDG INF of 0.015; red curve = patient with OS of 4 mo and 18F-FDG INF of 0.043.
Metastatic PC
The median OS of 44 patients with metastatic disease was 5 mo. Univariate analysis prognosticators of OS (P < 0.2), further included in the multivariate analysis, were VB, K1, k2, k3, and 18F-FDG INF. Multivariate analysis found VB, K1, and k3 to be significant variables for OS (P < 0.043, <0.031, and <0.009, respectively). The median OS was 5 and 7 mo in patients with VB below and above the value of 0.071 (P < 0.05), 4 and 6 mo for K1 above and below 0.35 (P < 0.02), and 4 and 8 mo for k3 above and below 0.041 (P < 0.02), respectively.
Total Group of Patients with PC
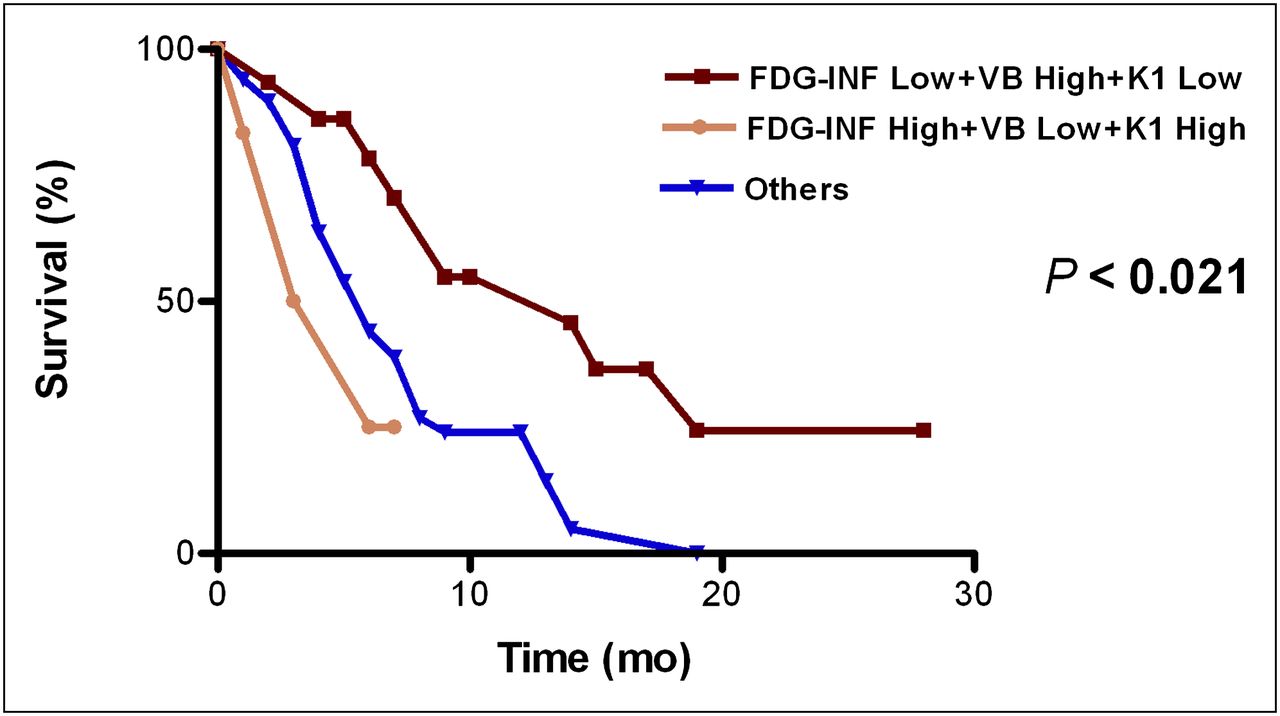
The total group of patients included 27 patients with localized PC (resected in 11 patients and locally advanced and nonresectable in 16 patients) and 44 patients with metastatic disease. There were no significant statistical differences between kinetic variables, equally distributed in localized and metastatic disease. Univariate analysis parameters related to OS were stage of disease, VB, K1, k3, FD, 18F-FDG INF, SUV1, and SUV2. Prognostic factors for OS significant at multivariate analysis were stage of disease, VB, K1, and 18F-FDG INF. A high 18F-FDG INF and K1 with low VB were related to a short median OS of 3 mo, whereas a low 18F-FDG INF and K1 with high VB were related to a prolonged median OS of 14 mo (P < 0.021). Patients with other combinations of these 3 parameters had an intermediate prognosis, with a median OS of 6 mo (Fig. 4).
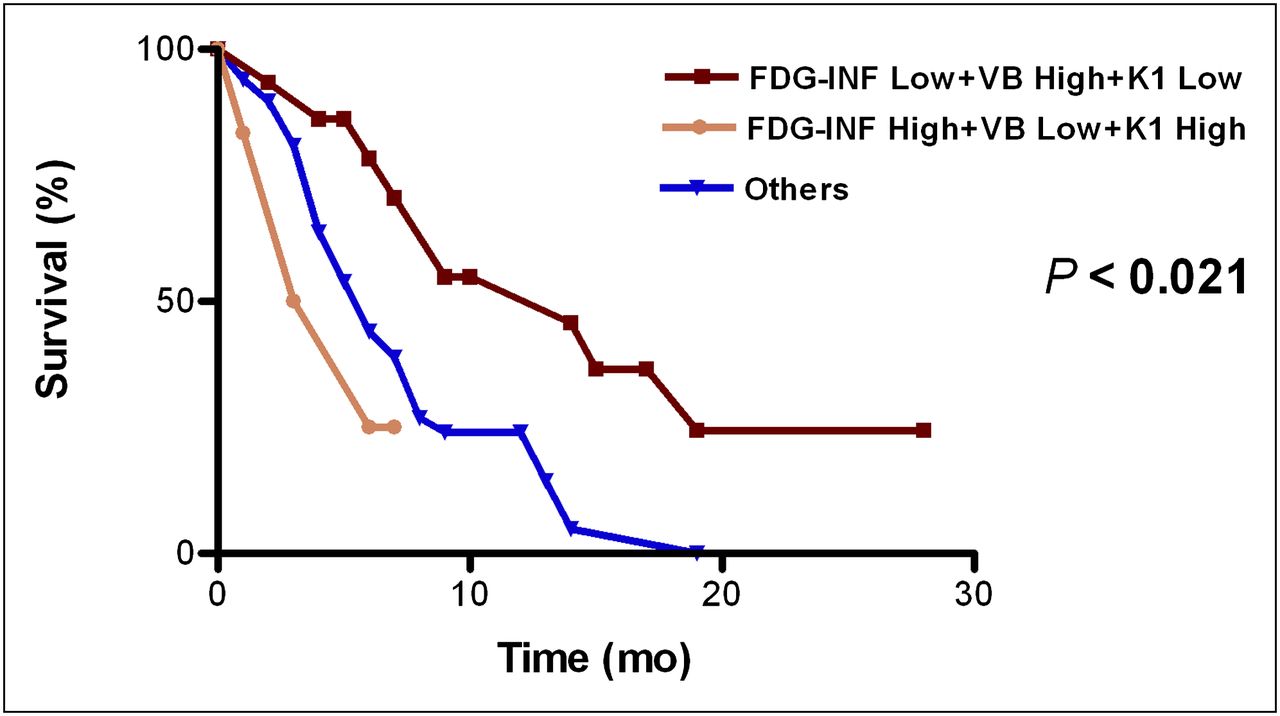
OS curves for whole study group of patients with PC classified by combination of high and low significant VB, K1, and 18F-FDG INF values.
DISCUSSION
The present study aimed to assess quantitative 18F-FDG PET kinetics as indices of tumor aggressiveness and predictors of outcome in patients with PC, a clinically heterogeneous malignancy.
Elevated glucose consumption plays an essential role in carcinogenesis and cancer progression (15–17). 18F-FDG is an indicator of enhanced glycolysis in malignant tissues. The intensity of 18F-FDG uptake cannot always accurately define the metabolic activity of tumor cells because nonphosphorylated intravascular and interstitial radiotracer can contribute to the overall intratumoral uptake. Therefore, visual assessment that does not always correlate with the tumor glucose metabolic rate was not used in the current study. Furthermore, confounding factors such as length of the uptake period after injection, lesion size, blood glucose levels, and insulin levels can influence semiquantitative 18F-FDG uptake measurements (4).
The kinetic model used in the present study discriminates and further associates between molecular tumor patterns and parameters of 18F-FDG kinetics. This model is based on the concept of 2 compartments containing 18F-FDG, linked by kinetic processes that provide an exchange of 18F-FDG and rate constants proportional to the rate of 18F-FDG exchange between compartments: K1 and k2 define transmembrane transport of 18F-FDG in both directions, and k3 and k4 define intracellular 18F-FDG phosphorylation and dephosphorylation. The 18F-FDG INF is calculated using the rate constants. The model also uses the VB of the target volume, because 18F-FDG uptake is modulated by the fractional blood volume in the tumor. Additionally, a noncompartment model calculates the time–activity curve FD, which helps to quantify heterogeneity. Different expressions of these factors resulted in different 18F-FDG accumulation profiles in benign versus malignant lesions and in low grade versus more aggressive tumors (7,9,10,18,19).
In primary and recurrent soft-tissue sarcoma, 18F-FDG kinetic parameters improved the low specificity of visual analysis of PET, discriminating grades I and III tumors with a positive predictive value above 80% (18). The comparison of kinetic parameters at baseline and after 1–2 chemotherapy cycles predicted the outcome of chemotherapy for advanced sarcoma early (9,19). The combination of kinetic parameters measured before chemotherapy (k3, k4, VB, and FD) and after the fourth cycle (K1, k4, and VB) identified short- and long-term survivors with metastatic colorectal cancer (7). In multiple myeloma, k3 and FD before and after 1 cycle of anthracycline-based chemotherapy predicted progression-free survival, high baseline k3 being an indicator of worse outcome (10). These results demonstrate that the use of parametric images and quantitative parameters of tracer kinetics add a new dimension to 18F-FDG PET/CT (20).
The relationship between 18F-FDG activity and prognosis in PC has been previously analyzed using 18F-FDG SUV measurements. Pretreatment-measured SUV significantly predicted OS in 55 patients with locally advanced PC receiving stereotactic body radiotherapy and gemcitabine-based chemotherapy (21). In 24 patients with advanced PC under chemotherapy, a high SUV predicted shorter OS (22). In both studies, SUV was a significant, independent factor for OS by multivariate analysis (21,22). In 56 patients with PC before resection, a high SUV was a risk factor for early postoperative recurrence (23). In the present study on univariate analysis, SUV1 and SUV2 were predictors of survival in all patients and in the subgroup with localized PC. However, these parameters were not significant for survival by multivariate analysis, probably because of the highly predictive significance of 18F-FDG INF for OS.
In this study, kinetic 18F-FDG parameters before therapy were analyzed as predictors of the clinical behavior of PC. The most important single parameter correlating with clinical outcome of localized PC was 18F-FDG INF. High values predicted the same short median OS in patients with localized PC, whether resected or not (5 and 6 mo, respectively). Patients with a low 18F-FDG INF fared significantly better and had a prolonged median OS in both subgroups (15 and 19 mo, respectively). 18F-FDG INF, generated by a 2-tissue-compartment model from the transport and phosphorylation constant (K1, k2, and k3), indicates the net tracer influx rate constant, provides an accurate estimate of tumor glucose consumption and metabolism, and thus reflects tumor aggressiveness and progression. In the present study, 18F-FDG INF provides significant prognostic information on localized PC, which, if confirmed in further large-scale studies, might bring about questions on the rationale of performing pancreatectomy in a subgroup of patients with clinically resectable but aggressive disease, as well as possibly affecting the therapeutic strategy in patients with locally advanced, nonresectable disease.
Kinetic 18F-FDG transport parameters (K1, k2) and the vascular fraction of tumor (VB) were significant factors for survival in metastatic PC. Stage was the most significant variable for OS in the whole study group, together with 18F-FDG INF, K1, and VB. However, grouping of the 3 significant kinetic parameters showed that a high 18F-FDG INF and K1 with low VB were related to a short OS (median, 3 mo), whereas a low 18F-FDG INF and K1 with high VB were indicators of a longer OS (median, 14 mo), irrespective of stage. These results are in accordance with the previously reported poor prognosis in PC with increased metabolic activity and decreased blood flow (24). A perfusion/metabolism mismatch—that is, low tumor blood flow and high 18F-FDG uptake—has been described in a variety of tumors and is associated with adverse tumor biology (25). A high metabolic rate and/or blood flow at baseline, calculated using dynamic PET, was more frequent in more aggressive triple-negative locally advanced breast cancer (26) and was associated with a poor response to neoadjuvant chemotherapy (27).
The present study is limited by the relatively small number of patients in the different subgroups and the nonuniform treatment strategies. However, the present results demonstrate the presence of a previously unknown relationship between kinetic 18F-FDG parameters and the clinical course of disease that can have significant management consequences in patients with PC. Quantitative PET analysis is a cumbersome technique with value demonstrated mainly in a research setting. After the validation of its diagnostic and predictive value, it is to be expected that the acquisition protocol and software will be simplified for future clinical use.
CONCLUSION
Tumor aggressiveness and survival in patients with PC can be predicted by kinetic 18F-FDG uptake parameters generated by dynamic PET studies performed at diagnosis, before the initiation of treatment. 18F-FDG INF was found to be the single statistically significant variable for OS in patients with localized disease, whether nonresectable or after surgery. Survival of all patients, regardless of the stage of disease, was related to the 18F-FDG INF, K1, and VB kinetic variables. On the basis of the current preliminary results, absolute quantitation of 18F-FDG kinetics represents a potential tool for noninvasive characterization of tumor aggressiveness and may, in the future, be integrated into a prognostic score for individualized treatment tailoring in patients with newly diagnosed cancer of the pancreas—most importantly, in those with localized disease. Treatment can be intensified in patients with a high 18F-FDG INF, whether resectable or not, while using a less aggressive therapeutic approach in patients with a low 18F-FDG INF and conservative treatment without initial surgery in patients with borderline resectable tumor and low 18F-FDG INF.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported in part by a grant from the Israel Cancer Association. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 19, 2012.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 14, 2012.
- Accepted for publication July 25, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}