


Abstract
The assessment of treatment response in glioblastoma is difficult with MRI because reactive blood–brain barrier alterations with contrast enhancement can mimic tumor progression. In this study, we investigated the predictive value of PET using O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET PET) during treatment. Methods: In a prospective study, 25 patients with glioblastoma were investigated by MRI and 18F-FET PET after surgery (MRI-/FET-1), early (7–10 d) after completion of radiochemotherapy with temozolomide (RCX) (MRI-/FET-2), and 6–8 wk later (MRI-/FET-3). Maximum and mean tumor-to-brain ratios (TBRmax and TBRmean, respectively) were determined by region-of-interest analyses. Furthermore, gadolinium contrast-enhancement volumes on MRI (Gd-volume) and tumor volumes in 18F-FET PET images with a tumor-to-brain ratio greater than 1.6 (Tvol 1.6) were calculated using threshold-based volume-of-interest analyses. The patients were grouped into responders and nonresponders according to the changes of these parameters at different cutoffs, and the influence on progression-free survival and overall survival was tested using univariate and multivariate survival analyses and by receiver-operating-characteristic analyses. Results: Early after completion of RCX, a decrease of both TBRmax and TBRmean was a highly significant and independent statistical predictor for progression-free survival and overall survival. Receiver-operating-characteristic analysis showed that a decrease of the TBRmax between FET-1 and FET-2 of more than 20% predicted poor survival, with a sensitivity of 83% and a specificity of 67% (area under the curve, 0.75). Six to eight weeks later, the predictive value of TBRmax and TBRmean was less significant, but an association between a decrease of Tvol 1.6 and PFS was noted. In contrast, Gd-volume changes had no significant predictive value for survival. Conclusion: In contrast to Gd-volumes on MRI, changes in 18F-FET PET may be a valuable parameter to assess treatment response in glioblastoma and to predict survival time.
- glioblastoma
- assessment of treatment response
- prognosis
- amino acid PET
- 18F-fluoroethyl-L-tyrosine (18F-FET)
Despite all efforts to improve treatment strategies, the prognosis of patients with glioblastoma to date remains poor (1). Standard therapy includes surgery and radiotherapy with concomitant and adjuvant temozolomide chemotherapy (2). MRI is the most important diagnostic tool for assessing brain neoplasms, and in malignant gliomas (3) the extent of contrast enhancement on MRI is used as an indicator of therapeutic response although the reliability in distinguishing tumor tissue from unspecific treatment effects such as postsurgery blood–brain barrier breakdown is limited (4). For example, reactive transient blood–brain barrier alterations with consecutive contrast enhancement can mimic tumor progression. This phenomenon, so-called pseudoprogression, is seen in 20%–30% of cases (5) and may result in an unnecessary overtreatment. Consequently, alternative diagnostic methods are needed to improve the assessment of treatment response (6).
The rationale for using radiolabeled amino acids such as O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) to measure treatment response in cerebral gliomas is based on high uptake of the radiotracer in these tumors—uptake that is likely to reflect an increased expression of amino acid transporters (7). Amino acid uptake in gliomas is independent of blood–brain barrier disruption, and increased 18F-FET uptake has also been observed in nonenhancing tumor areas that are difficult to delineate using MRI (8). Furthermore, contrast-enhancing nontumoral tissue on MRI, for example, due to radionecrosis, is usually negative on 18F-FET PET (9). Thus, 18F-FET PET may be a promising tool to improve the evaluation of treatment response.
Current experience with radiolabeled amino acids concerning treatment monitoring and prediction of outcome is promising (10–15), but the parameters derived from amino acid PET to assess treatment response vary among different studies. Some studies suggested that a change of the maximal tumor-to-brain ratio (TBR) may be the most reliable parameter for the identification of tumor progression (9), whereas other studies suggest that changes in the tumor volume delineated by amino acid PET may be more sensitive than standardized uptake values (16).
This prospective study systematically evaluated the time course of different parameters derived from 18F-FET PET during treatment of glioblastoma in comparison to conventional MRI for assessing treatment response with respect to survival time of the patients. A preliminary evaluation of the data indicated that 18F-FET PET was indeed helpful at predicting treatment response and outcome of the patients at an early stage of the disease (17). In this final evaluation, the ultimate size of the patient population and a longer follow-up period are considered. In addition, various parameters derived from 18F-FET PET and the examination of tumor volume on MRI are included in the analysis.
MATERIALS AND METHODS
Patients
From January 2007 to June 2010, a group of 25 consecutive patients with glioblastoma were included in this prospective study. There were 15 men and 10 women; the mean age was 54 y (range, 36–73 y). The tumor was located in the frontal, temporal, parietal, and occipital lobes in 9, 7, 8, and 1 patients, respectively. All patients were treated with cytoreductive surgery. According to neurosurgical reports, 13 surgical interventions were rated as partial resections and 12 as gross total resections, although considerable tumor remnants were detected on 18F-FET PET in most of these patients (Table 1). Surgery was followed by an external fractionated radiotherapy with concomitant temozolomide (RCX; 75 mg of temozolomide per square meter of body surface area per day, 7 d per week from the first to the last day of radiotherapy) and, after a 4-wk break, by adjuvant temozolomide chemotherapy (150–200 mg of temozolomide per square meter of body surface area over 5 d, repeated every 23 d, 6 cycles) according to EORTC trial 22981/26981 (2). During adjuvant temozolomide therapy, patients underwent a monthly clinical evaluation, and after completion of adjuvant temozolomide therapy a clinical evaluation was performed every 2–3 mo.
Patient Characteristics, TBRmax, TBRmean, and Tvol 1.6 in 18F-FET PET, Gd-Volumes in MRI, PFS, and OS
The general prognosis of the patients was classified by the commonly used recursive partitioning analysis (RPA) scores including a set of pretreatment- and treatment-related prognostic variables (18). O6-methylguanine-DNA methyltransferase status (MGMT) could be determined in 22 patients (19). Further details on the patient group are given in Tables 1 and 2. The university ethics committee and federal authorities approved this study. All subjects gave written informed consent before their participation in the study.
Univariate Survival Analysis of General Prognostic Factors
Radiotherapy
In all patients, a total dose of 60 Gy was administered to the planning target volume 1 (PTV1), defined as the contrast-enhanced area from pre- and postoperative MRI including a safety margin of 2–3 cm and including the surrounding preoperative edema. The dose was prescribed to the reference point of the International Commission on Radiation Units and Measurements (20), and the fractionation was 2 Gy daily, 5 times weekly. Radiation treatment was planned in 5 of the 25 patients with the standard 3-dimensional radiation treatment. The remaining 20 patients underwent intensity-modulated radiotherapy. In these patients, an additional planning target volume (PTV2) was created and defined as the 18F-FET–positive tumor volume within a cutoff of 1.6 or more for the TBR of 18F-FET uptake. In all patients, the pathologic 18F-FET volume PTV2 was covered by the PTV1. The total dose for PTV2 was 72 Gy, and the mean dose for the larger PTV1 was 60 Gy, as in the other patients. The Pinnacle irradiation treatment planning system (version 8.0m; Philips) was used for radiation treatment planning.
MRI and Analysis
All patients underwent routine MRI using a 1.5-T scanner with a standard head coil before and after administration of gadolinium–diethylenetriaminepentaacetic acid (T1, T2, and fluid-attenuated inversion recovery sequences; slice thickness, 1 mm). The first MRI scan (MRI-1) was obtained within 11–20 d after surgery, the second MRI scan (MRI-2) 7–10 d after completion of RCX, and the third MRI scan (MRI-3) 6–8 wk after completion of RCX. After MRI-3, a follow-up MRI scan was obtained every 8–12 wk. As previously described (21), in all patients gadolinium contrast–enhancing volumes on MRI (Gd-volume) were measured by performing a 3-dimensional threshold-based volume-of-interest analysis using the VINCI tool (22). The threshold for contrast enhancement on MRI was determined by varying the value of the lower threshold to identify and separate the area of contrast enhancement from the tissue with lower intensity (21).
PET with 18F-FET and Analysis
The amino acid 18F-FET was produced via nucleophilic 18F-fluorination with a specific radioactivity of greater than 200 GBq/μmol, as described previously (23). All patients fasted for at least 12 h before the PET studies. Dynamic PET studies were performed up to 50 min after intravenous injection of 200 MBq of 18F-FET on an ECAT EXACT HR+ scanner (Siemens Medical Systems, Inc.) in 3-dimensional mode (32 rings; axial field of view, 15.5 cm). Further evaluation was based on the summed 18F-FET PET data from 20 to 40 min after injection. Attenuation correction and data reconstruction were performed as described previously (8). The PET studies were done in temporal correspondence to MRI.
18F-FET PET and MRI were automatically coregistered using the VINCI tool (22). The fusion results were inspected and, if necessary, adapted using anatomic landmarks. 18F-FET uptake in the unaffected brain tissue was determined by a larger region of interest (ROI) placed on the contralateral hemisphere in an area of normal-appearing brain tissue including white and gray matter (mean area, 2,082 ± 369 mm2). The tumor area on 18F-FET PET scans was determined by a 3-dimensional autocontouring process using a cutoff of 1.6 or more for the TBR of 18F-FET uptake. This cutoff was based on a previous biopsy-controlled study in which a lesion-to-brain ratio of 1.6 had best separated tumor from nontumor tissue (8). Manual corrections of the tumor ROI were applied if the radioactivity in blood vessels or tracer uptake in postoperative extracerebral soft tissue exceeded the cutoff value. Maximum and mean TBR (TBRmax and TBRmean, respectively) were calculated by dividing the mean and maximum ROI value (Bq/mL) of the tumor lesion by the mean ROI value of normal brain tissue in the 18F-FET PET scans. The 18F-FET–positive tumor volume at a cutoff of 1.6 or more for the TBR (Tvol 1.6) was determined.
Definition of Pseudoprogression
Usually, contrast enhancement on MRI during pseudoprogression occurs within the first 8 wk after completion of RCX and invariably undergoes spontaneous clinical and radiographic improvement without intervention (6). Accordingly, in our study we identified patients with an increase of the Gd-volume of more than 50% between MRI-1 and MRI-3, followed by subsequent regression of contrast enhancement on follow-up MRI scans.
Definition of Survival Times
Overall survival (OS) time was defined as the interval from date of surgery to date of death or, if the patients were still alive, as the interval from date of surgery to date of last contact. Progression-free survival (PFS) was defined as the interval from date of surgery to date of first documented evidence of disease progression, based on decline shown by the MR image or neurologic deterioration. Progressive disease on the MR image was defined according to the criteria of Macdonald et al. (24).
Assessment of Treatment Effects on Prognosis
The relative and absolute changes of TBRmax, TBRmean, Tvol 1.6, and Gd-volumes at the second diagnostic scan (MRI and 18F-FET PET early [7–10 d] after completion of radiochemotherapy with temozolomide [RCX] [MRI-2 and FET-2, respectively]) and at the third diagnostic scan (MRI and 18F-FET PET 6–8 wk later [MRI-3 and FET-3, respectively]) after completion of RCX were determined in relation to baseline imaging (MRI and 18F-FET PET after surgery [MRI-1 and FET-1, respectively]). To analyze the prognostic value of changes of TBRmax, TBRmean, metabolically active tumor volumes (Tvol 1.6), and Gd-volumes in serial 18F-FET PET and MRI on OS and PFS, patients were subdivided into responders and nonresponders according to the changes of the different imaging parameters. In an approximation process, different cut points of the various parameters were used to determine the value best separating the patients into 2 prognostic groups (Table 3; Supplemental Tables 1–4 [supplemental materials are available online only at http://jnm.snmjournals.org]). The diagnostic value of the various parameters for the prediction of treatment success was also tested using a receiver-operating-characteristic (ROC) analysis. Therefore, the patient population was divided into a partition with longer survival (PFS/OS > median) and a partition with shorter survival (PFS/OS < median). Along with the ROC analysis, the extent to which the individual parameters identified those patients with shorter survival was examined (Supplemental Table 1).
Prognostic Impact of Changes of TBRmax, TBRmean, Tvol 1.6, and Gd-Volume on Survival
On the basis of our experiences with other tyrosine derivates, we assumed only a change of greater than 5% of the TBR of 18F-FET uptake as significant (25). Furthermore, all changes in rest tumor volumes in 18F-FET PET below 2 cm3 were considered as insignificant and set to zero for statistical evaluation (patients 8, 13, and 25) because the calculation of Tvol 1.6 of 18F-FET uptake in small residual tumor volumes is considerably influenced by partial-volume effects.
Statistics
Survival analysis was performed using Kaplan–Meier estimates for PFS and OS (data are presented as median values). The log-rank test was used for global comparison of PFS and OS curves between the subgroups. As general prognostic factors, the RPA score, extent of resection, MGMT status, and Tvol 1.6 in FET-1 at a cutoff of 25 cm3 were considered (Table 2) (14). To evaluate the prognostic impact of treatment-related variations in PET and MRI, the changes of TBRmax, TBRmean, and Tvol 1.6 in 18F-FET PET and Gd-volume in MRI were tested. A P value of 0.05 or less was considered statistically significant. The data of the statistical tests are corrected for multiple statistical testing using the Bonferroni adjustment. The results of the statistical tests are given without correction for multiple statistical testing. It is explicitly noted, however, if the significance level was greater than 0.05 after performing a Bonferroni correction.
A multivariate Cox regression analysis was performed for the changes of each TBRmax, TBRmean, and Tvol 1.6 in 18F-FET PET, and Gd-volume in MRI in relation to RPA score, prescribed radiation dose, MGMT status, postoperative Tvol 1.6 (FET-1), and extent of resection to investigate which of these variables constitutes an independent prognostic factor with respect to PFS and OS. This analysis was done for each parameter separately. Hazard rate ratios and their 95% confidence intervals were calculated (Table 4). All statistical tests to which they apply were 2-sided.
Multivariate Analysis (Cox Proportional Hazards Model) of Imaging-Related Factors vs. RPA Score, Prescribed Radiation Dose, MGMT Status, Postoperative Tvol 1.6 (FET-1), and Extent of Resection
ROC curves were drawn for the changes of TBRmax, TBRmean, and Tvol 1.6 in 18F-FET PET and Gd-volume in MRI, and the areas under the curves (AUC) were calculated. For a specific parameter, the cutoff level that resulted in the highest product of sensitivity and specificity was considered the optimal cutoff for prognostication.
Statistical analysis was performed using SigmaStat software (for Windows 11.0; SigmaPlot) and PASW statistics software (Release 18.0.3; SPSS Inc.).
RESULTS
Patient Data
The median follow-up was 13.8 mo (range, 3–29 mo). The clinical data of the patients and the results of TBRmax, TBRmean, and Tvol 1.6 in 18F-FET PET and Gd-volumes in MRI are presented in Table 1. The statistical influence of general prognostic factors is shown in Table 2.
Survival According to General Prognostic Factors
The mean PFS and OS of all patients (n = 25) were 9.2 mo (median, 7.2 mo; range, 2.8–28.7 mo) and 14.1 mo (median, 13.8 mo; range, 2.8–28.7 mo). Well-established prognostic factors such as the RPA score and extent of tumor resection showed a trend toward significance on PFS and OS. For the MGMT status and postoperative Tvol 1.6 in FET-1 less than 25 cm3, respectively, a significantly longer PFS and OS could be observed (Table 2). In our patient group, neither radiation technique (3-dimensional radiation treatment vs. intensity-modulated radiotherapy) nor prescribed radiation dose had a significant influence on prognosis.
Survival According to Gd-Volume
The relationship of survival and treatment-related changes of the Gd-volume between MRI-1 and MRI-2, and between MRI-1 and MRI-3, was tested at cutoff values of ≤0% vs. >0% and ≤−25% vs. >−25% (Tables 3 and 4; Supplemental Table 4). Testing of further cutoff values led to strong disparity of group sizes and was discarded. No significant differences of PFS and OS between the different groups could be detected. ROC analysis yielded no significant results.
Survival According to Changes of TBRmax and TBRmean of 18F-FET Uptake
Using the approximation procedure, the best discriminative power to separate the patients in 2 prognostic groups was identified at a decrease of the TBRmax of more than 10% (≤−10% vs. >−10%) (Table 3). Testing of further cutoff values led to strong disparity of group sizes (Supplemental Table 2). Early metabolic 18F-FET PET responders with a decrease of the TBRmax between FET-1 and FET-2 (≤−10%) had a significantly longer median PFS (9.3 vs. 4.7 mo; P = 0.002) and OS (15.4 vs. 8.5 mo; P < 0.001) than nonresponders (Table 3). ROC analysis confirmed also the best cut point for TBRmax to predict PFS at −10%. For prediction of OS, the optimal cut point of TBRmax was slightly different (−20%), as may be explained by statistical effects due to the small size of the group. According to ROC analysis, a decrease of the TBRmax between FET-1 and FET-2 of more than 20% allowed the identification of patients with OS less than median, with a sensitivity of 83% and a specificity of 67% (AUC, 0.75; P = 0.04; Supplemental Table 1). Also, the follow-up at FET-3 showed a longer OS for metabolic responders than for nonresponders (15.4 vs. 9.3 mo; P = 0.02); however, this difference is not significant after Bonferroni adjustment.
For TBRmean, similar results were obtained. The best discriminative power was identified at a decrease of TBRmean more than 5% (≤−5% vs. >−5%) using the approximation procedure (Table 3). With a trend toward significance, the same cut point was determined by ROC analysis to predict PFS and OS. The decrease of the TBRmean between FET-1 and FET-2 allowed the identification of patients with PFS and OS less than median with a sensitivity of 67% and a specificity of 75% (AUC, 0.72; P = 0.08 and 0.07, respectively; Supplemental Table 1). Again, early metabolic responders with a decrease of the TBRmean between FET-1 and FET-2 (≤−5%) exhibited a significantly longer median PFS (10.3 vs. 5.1 mo) and OS (16.1 vs. 9.3 mo) (P < 0.001 for both PFS and OS; Table 3). The varying of thresholds (≤0% vs. >0% and ≤−10% vs. >−10%) showed results with poorer discrimination power (Supplemental Table 2).
Multivariate Cox regression analysis confirmed early changes of TBRmax and TBRmean (FET-2 vs. FET-1) as significant independent predictors of PFS and OS (Table 4). The Kaplan–Meier plots of PFS and OS of early metabolic responders and nonresponders according to the TBRmean of 18F-FET uptake (≤−5% vs. >−5%) are shown in Figure 1.

Kaplan–Meier curves of PFS (left) and OS (right) of patients with glioblastoma according to treatment-related changes of TBRmean in 18F-FET PET early after completion of RCX (FET-2 vs. FET-1). Metabolic responders with decrease of TBRmean of more than 5% (≤−5%) show significantly longer PFS and OS than nonresponders. Censored observations are marked with dots.
Survival According to Changes of Tvol 1.6
To evaluate the prognostic influence of changes of the tumor volume in 18F-FET PET, patients were separated into a group of metabolic responders who showed a stable or decreasing Tvol 1.6 in 18F-FET PET (relative change ≤ 0%) and a group of nonresponders who showed an increasing Tvol 1.6 in 18F-FET PET (relative change > 0%) (Table 3; Supplemental Table 3). Separating the groups at other cutoff values led to a strong disparity of group sizes and was discarded. Early after completion of RCX (FET-2), the metabolic responders with stable or reduced tumor volume in 18F-FET PET had a weakly significantly longer PFS than the nonresponders (9.4 vs. 5.8 mo; P = 0.04; Table 3). However, after Bonferroni adjustment this observation was not significant. At 6–8 wk after completion of RCX (FET-3), however, changes of Tvol 1.6 in 18F-FET PET had a more significant prognostic value, especially for PFS (9.3 vs. 5.1 mo; P = 0.002; Table 3). For OS, only a trend could be observed (P = 0.06). ROC analysis yielded no significant results.
Multivariate Cox regression analysis confirmed changes of Tvol 1.6 at further follow-up (FET-3 vs. FET-1) as an independent predictor of PFS (Table 4).
Pseudoprogression
Five of 25 patients (20%) had pseudoprogression on MRI (patients 1, 6, 16, 19, and 23; Fig. 2 shows images of patient 1). All these patients had a favorable median PFS and OS (9.3 and 16.1 mo, respectively). Furthermore, in patients with pseudoprogression the median reduction of TBRmax and TBRmean was 22% and 11%, respectively, and the Tvol 1.6 remained stable (median change, 0%). In contrast, all patients showed an increase of the Gd-volume (median change, 433%).
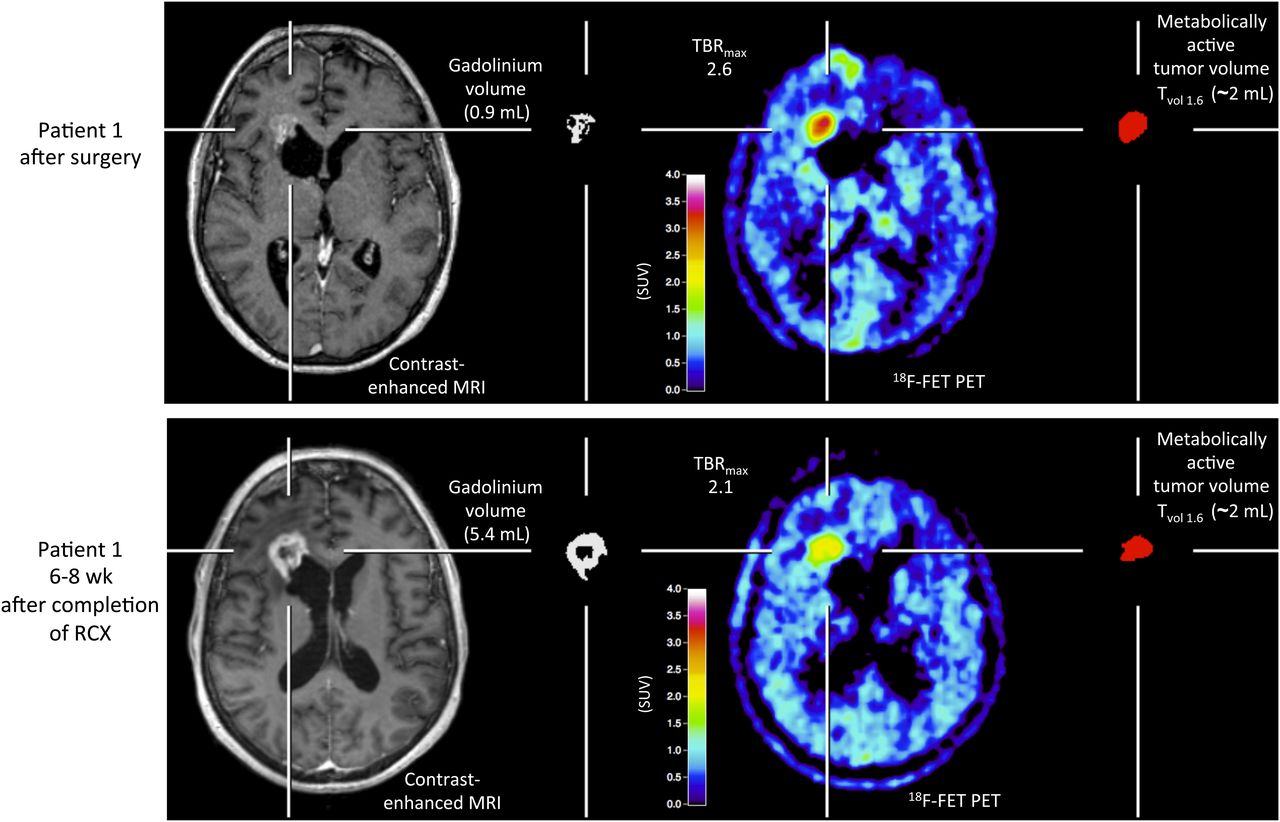
Patient example of pseudoprogression (patient 1). Brain imaging after surgery (upper; MRI-/FET-1) and 6–8 wk after completion of radiochemotherapy (lower; MRI-/FET-3). Contrast-enhanced MRI with corresponding Gd-volume is shown on left and 18F-FET PET with corresponding Tvol 1.6 on right. Enlargement of Gd-volume on MRI after 6- to 8-wk completion of RCX (lower) is suggesting tumor progression, whereas 18F-FET PET indicates responder with decreasing amino acid uptake (reduction of TBRmax) and unchanged Tvol 1.6. Patient had favorable outcome, with PFS of 14.1 and OS of 16.1 mo.
DISCUSSION
The results of this prospective study suggest that the decrease of 18F-FET accumulation as indicated by TBRmean and TBRmax reflects the reaction of the tumor to the therapeutic intervention at an early stage of the disease (FET-2) and predicts outcome. At a later stage (FET-3), changes of the TBR in relation to baseline are less predictive, and changes of Tvol 1.6 may be of additional value. Therefore, the data indicate that various parameters derived from 18F-FET PET may be useful to predict treatment response at an early stage of disease and may thereby help to optimize individual treatment. Moreover, especially the reduction of TBRs derived from 18F-FET PET may add valuable additional information to diagnose pseudoprogression within 6–8 wk after RCX.
In contrast to the 18F-FET PET results, in our study treatment-related changes of Gd-volumes in contrast-enhanced MRI failed to predict treatment response and showed no relationship with patient survival. Although the extent of MRI contrast enhancement in malignant gliomas is routinely used as an indicator of therapeutic response (26), this approach is limited by the difficulty in distinguishing between tumor and treatment-induced necrosis (27). Reliable prognostic information can be obtained only several months after the initiation of treatment. For several reasons, however, the ability to differentiate tumor progression from pseudoprogression is essential (Figs. 2 and 3). First, considerable morbidity is associated with unnecessary surgical interventions; second, because pseudoprogression spontaneously resolves, the ability to identify such lesions could prevent futile treatment from being given; and third, because chemotherapy is often adjusted after tumor progression (6).
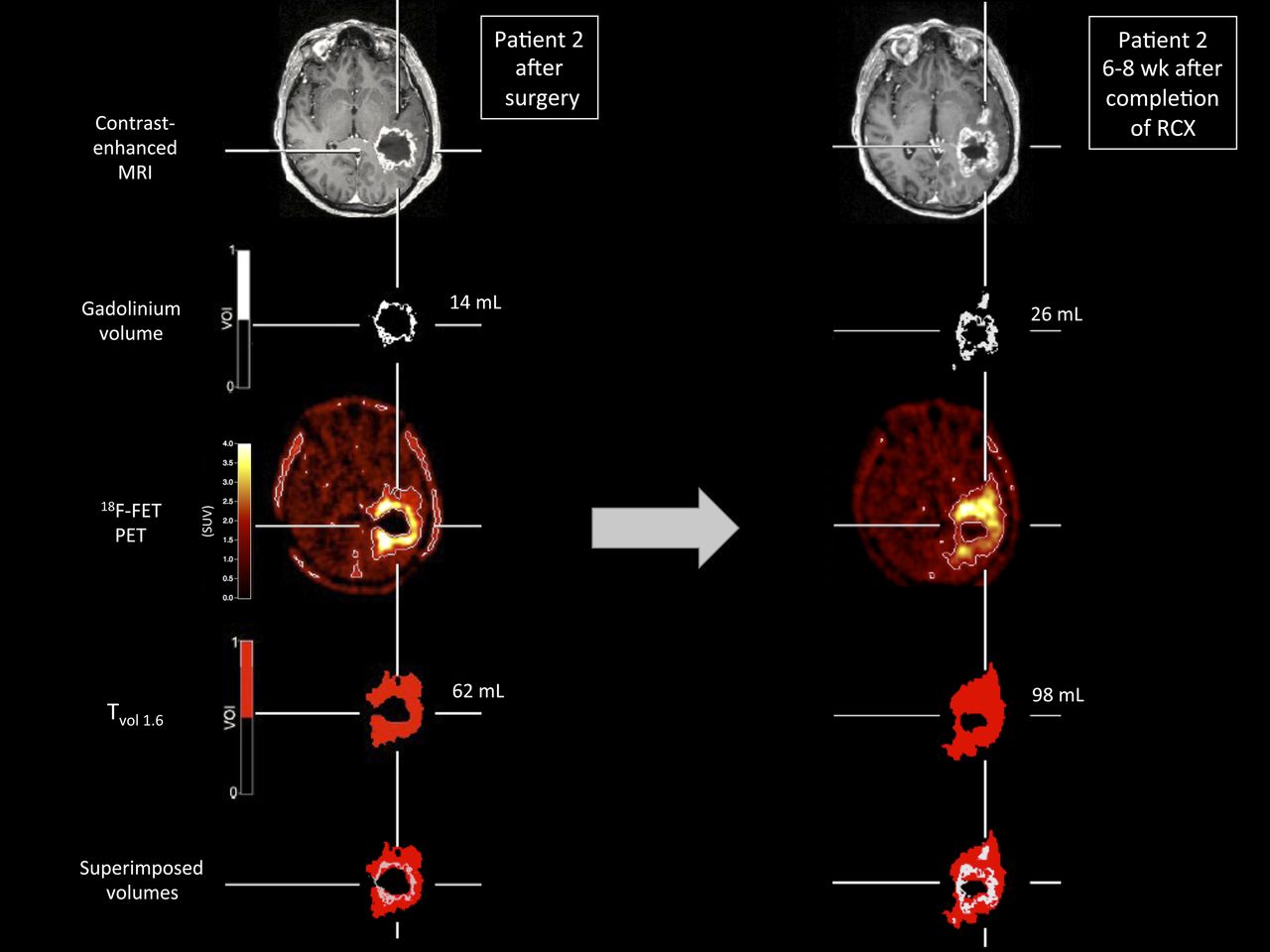
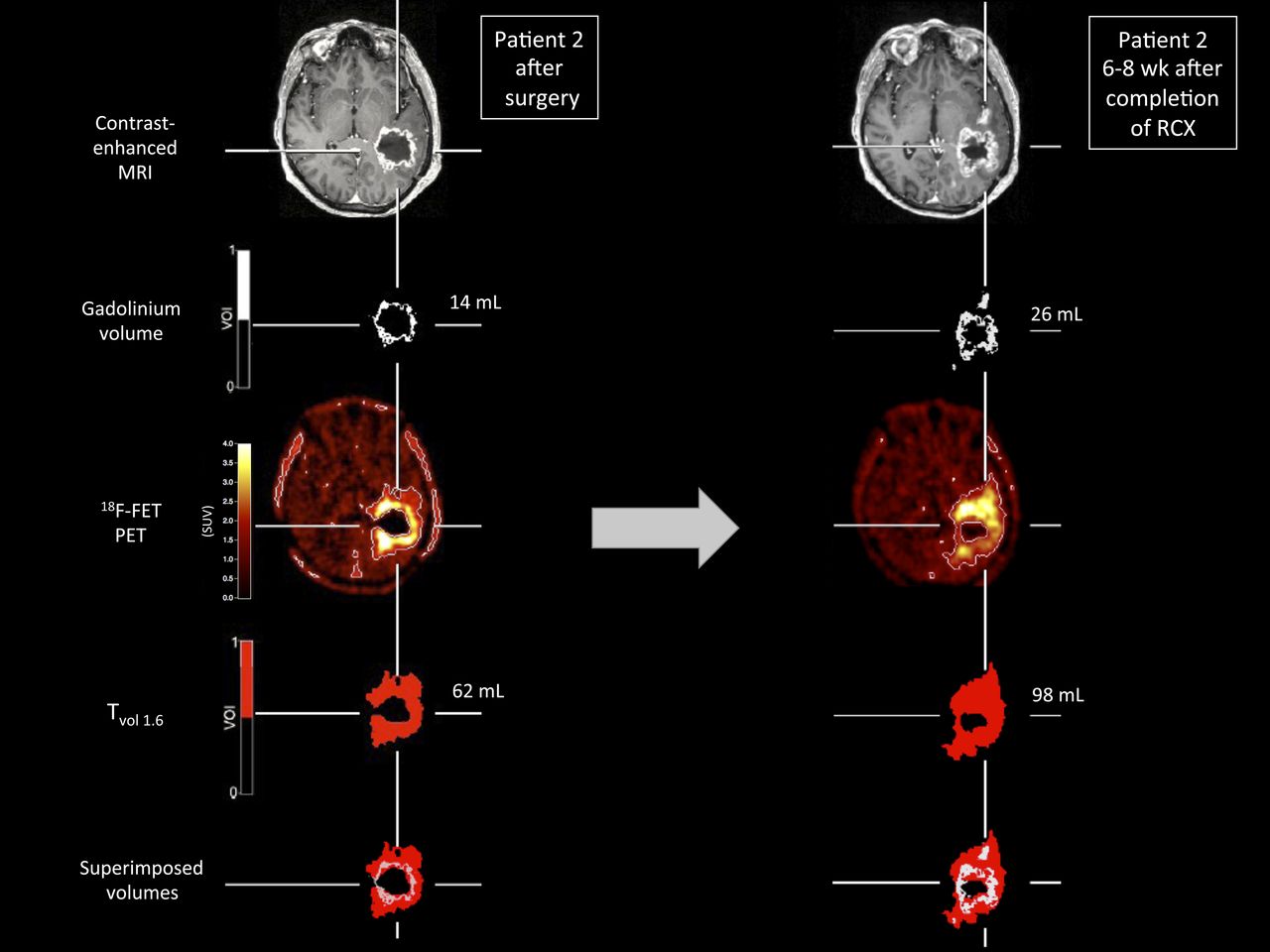
Patient example of nonresponder according to 18F-FET PET (patient 2). (Left) Imaging after surgery (FET-1/MRI-1). (Right) Imaging results 6–8 wk after completion of RCX (FET-3/MRI-3). Patient exhibits increasing 18F-FET uptake in course of disease (right). In comparison to imaging after surgery, coregistration of 18F-FET PET scan, contrast-enhanced MRI, and volumes of interest of contrast enhancement and Tvol 1.6 in transaxial orientation exhibit that metabolically active tumor volume is considerably larger than volume of contrast enhancement, has eccentric configuration, and covers entire contrast-enhancing volume (bottom). In this patient, PFS and OS were relatively short, at 8.3 and 9.3 mo, respectively.
The results of our study are in line with the observations of several studies that evaluated the role of amino acid PET using 11C-methionine and 18F-FET to monitor treatment effects in smaller groups of patients during a standard chemotherapy regimen—that is, adjuvant temozolomide (5/28) or procarbazine, lomustine (CCNU), and vincristine (PCV) chemotherapy (10,28); dose-intensified chemotherapy with temozolomide (29); and experimental treatment (e.g., intracavitary radioimmunotherapy, convection-enhanced delivery of paclitaxel, and tyrosine kinase inhibitor treatment) (12,13,30). Furthermore, the relevance of metabolically active tumor volumes in amino acid PET to assess treatment response is further supported by more recent studies (16,21,31,32).
Although conventional MRI cannot reliably distinguish between tumor and pseudoprogression, several alternative MRI techniques are presently evaluated that may overcome this problem (6,33). For example, diffusion and perfusion-weighted imaging have been considered (34,35), but the clinical relevance of these methods is not yet established (6). These developments are rather encouraging, and comparative studies are needed to investigate the relationship, diagnostic performance, and complementary character of amino acid PET and modern MRI techniques.
Some shortcomings of this study need to be discussed. Inasmuch as data on the reproducibility of the TBR of 18F-FET uptake in brain tumors are not yet available, experience with other tyrosine derivates had to be considered. With the tyrosine analog 123I-iodo-α-methyltyrosine, a maximal deviation of the TBR of 5% has been observed in repeated studies, indicating that the TBR of amino acid uptake in brain tumors is a rather stable parameter (25). Furthermore, it cannot be excluded that the PET signal in the baseline scan may have been due to postoperative changes and not residual macroscopic tumor tissue. Although residual uptake of 18F-FET after surgery has not yet been investigated histologically, 11C-methionine uptake after repeated surgery of residual childhood brain tumors showed that increased tracer uptake corresponded well with vital tumor tissue (36). Because the results with 11C-methionine and 18F-FET in brain tumors are similar (37), we assume unspecific 18F-FET uptake with a TBR of more than 1.6 in the postoperative phase is unlikely.
Finally, the patient number in this prospective study is small, and the results need to be considered with caution. Nevertheless, to the best of our knowledge, there is to date no larger prospective study in the literature concerning this topic.
CONCLUSION
The results of this study suggest that therapeutically induced changes in 18F-FET PET may be a useful measure to predict treatment response at an early stage of disease and may thereby help to optimize individual treatment. In contrast to Gd-volumes on MRI, changes in 18F-FET PET may be a valuable parameter to assess treatment response in glioblastoma and to predict survival time. Further studies are needed to investigate the clinical role of modern approaches of MRI in combination with amino acid PET to solve this important clinical issue.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online May 29, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication September 23, 2011.
- Accepted for publication February 8, 2012.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Early Treatment Response Assessment Using 18F-FET PET Compared with Contrast-Enhanced MRI in Glioma Patients After Adjuvant Temozolomide Chemotherapy
- Diagnosis of Pseudoprogression Following Lomustine-Temozolomide Chemoradiation in Newly Diagnosed Glioblastoma Patients Using FET-PET
- Treatment Monitoring of Immunotherapy and Targeted Therapy Using 18F-FET PET in Patients with Melanoma and Lung Cancer Brain Metastases: Initial Experiences
- Influence of Bevacizumab on Blood-Brain Barrier Permeability and O-(2-18F-Fluoroethyl)-L-Tyrosine Uptake in Rat Gliomas
- Combined PET Imaging of the Inflammatory Tumor Microenvironment Identifies Margins of Unique Radiotracer Uptake
- Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM
- Clinical Impact of Amino Acid PET in Gliomas
- Comparison of 18F-FET PET and Perfusion-Weighted MR Imaging: A PET/MR Imaging Hybrid Study in Patients with Brain Tumors
- Diagnostic Performance of 18F-FET PET in Newly Diagnosed Cerebral Lesions Suggestive of Glioma