


Abstract
In oncology, staging forms the basis for prognostic consideration and directly influences patient care by determining the therapeutic approach. Cross-sectional imaging techniques, especially when combined with PET information, play an important role in cancer staging. With the recent introduction of integrated whole-body PET/MRI into clinical practice, a novel metabolic–anatomic imaging technique is now available. PET/MRI seems to be highly accurate in T-staging of tumor entities for which MRI has traditionally been favored, such as squamous cell carcinomas of the head and neck. By adding functional MRI to PET, PET/MRI may further improve diagnostic accuracy in the differentiation of scar tissue from recurrence of tumors such as rectal cancer. This hypothesis will have to be assessed in future studies. With regard to N-staging, PET/MRI does not seem to provide a considerable benefit as compared with PET/CT but provides similar N-staging accuracy when applied as a whole-body staging approach. M-staging will benefit from MRI accuracy in the brain and the liver. The purpose of this review is to summarize the available first experiences with PET/MRI and to outline the potential value of PET/MRI in oncologic applications for which data on PET/MRI are still lacking.
In oncology, staging forms the basis for prognostic consideration and directly influences patient care by determining the therapeutic approach. The periodically revised standardized TNM cancer staging system (1) is pivotal for comparative treatment studies, which in an ongoing process define the most suitable therapy regime for each tumor stage and entity. Imaging plays a key role in the evaluation of local tumor extent and in the detection of potential locoregional lymph node or distant metastases. Diagnostic accuracy in the determination of the individual TNM stage, besides methodologic safety, operational availability, and cost, is the most questioned attribute when it comes to the choice of the most appropriate and accurate imaging modality for cancer staging. With the launch of integrated whole-body PET/MRI, the purpose of this review is to summarize the available first experiences with PET/MRI and to outline the potential value of PET/MRI in oncologic applications for which data on PET/MRI are still lacking. In parts of this article, we refer to our own unpublished experiences with PET/MRI that have not yet undergone a peer-review process. This contribution needs to be understood as supported solely by the authors’ experience and should not be misinterpreted as evidence-based knowledge.
TECHNICAL ADVANCES IN DIAGNOSTIC IMAGING
In the past decade, the introduction of integrated metabolic–anatomic imaging with PET/CT has had a substantial influence on tumor staging and has set a new benchmark in TNM staging accuracy when compared with conventional imaging modalities (2). On the other hand, because of the lower soft-tissue contrast, PET/CT could not replace MRI in certain staging indications, such as T-staging of soft-tissue sarcomas, primary hepatic malignancies, and M-staging of cerebral or liver metastases (3). MRI itself has advanced significantly over the past few years and can now provide high-resolution images within a reasonable scanning time (4). In addition, several different functional MRI techniques have evolved. Among others, diffusion-weighted imaging (DWI) and nuclear MR spectroscopy provide a new dimension of biologic information in MRI by enabling measurements of tissue cellularity and amino acid composition. On the PET side, detectors needed to be developed that could be operated in the presence of a high magnetic field. Avalanche photodiode detectors allow for the contemporaneous use of MRI (5), an advance that facilitated the integration of MRI and PET. This new combination was eagerly awaited to enhance the T-staging accuracy in those tumors that could not dispense with MRI and the N-staging and M-staging performance in body compartments that were superiorly depicted by PET (3). Regardless of these advances, PET/MRI has the same natural restrictions in the detection of micrometastases as other imaging modalities. Because of the technically limited spatial resolution of MRI and PET scanners, and differences in the avidity of tumors to the radionuclide, very small metastases are frequently missed when unselective radionuclides such as 18F-FDG are used (6). This general limitation has to be kept in mind when the role of new imaging modalities is discussed in an oncologic context.
ADVANCED MRI TECHNIQUES IN ONCOLOGY
MRI can provide different image contrasts through adjustment of echo and repetition times, parameters that represent specific tissue characteristics. T1- and T2-weighted sequences form the basis of morphologic MRI information. In addition to mere morphologic imaging, molecular imaging is provided through a variety of functional MRI techniques. As a measure of cellularity, DWI assesses the degree to which diffusion of water molecules is restricted in the extracellular space (7). By calculation of the apparent diffusion coefficient, MR DWI, for example, increases the detection rate of metastases in normal-sized lymph nodes from 7% to 76% (8). MR spectroscopy provides a quantitative measure of the amino acid composition of a region of interest (9). These specific amino acid profiles can be used to differentiate brain tumor entities (10). Dynamic contrast-enhanced MRI allows for the calculation of different fractions of tumor perfusion, providing information on the amount of neovascularization. Quantitative dynamic contrast-enhanced MRI can be helpful for differentiating benign from malignant breast tumors and can be of use for assessing the effects of antiangiogenic tumor therapy (11). With DWI, MR spectroscopy, and dynamic contrast-enhanced MRI, we present just a selection of molecular MRI techniques valuable for oncologic applications to point out the principle that the use of MRI in integrated PET/MRI goes beyond the anatomic correlation of PET findings. The simultaneous acquisition of multiparametric MRI and PET data is awaited to create new options in molecular tumor imaging.
Our review will have 2 parts. As part 1, this article addresses tumors of the brain, head and neck, chest, abdomen, and pelvis. Part 2, to be published in a subsequent issue, reviews tumors of the bone and soft tissues, as well as melanoma and lymphoma. In both parts, distant metastases are addressed on an organ basis rather than separately for each primary tumor.
TUMORS OF THE BRAIN
Cerebral Metastases
Cerebral metastases represent the most frequent brain tumors and occur in 20%–40% of cancer patients. Generally, patients with cerebral metastases have a relatively short survival. Among patients with brain metastases, those with solitary or few metastases face a rather favorable prognosis. However, sensitive detection is essential to supply an appropriate potentially curative or palliative therapy to the patient. In most cases, cerebral metastases become symptomatic with headache, focal neurologic deficits, and seizures but may also be found coincidentally on staging scans. When it comes to imaging, CT and MRI are the standard modalities for the assessment of the brain. In a randomized prospective trial on preoperative staging of lung cancer patients (12), significantly smaller metastases (as small as 0.5 mm) were seen on MRI than on CT. Because of the high physiologic 18F-FDG uptake of the cortex, 18F-FDG PET does not compensate for the shortcomings of CT in the detection of subcentimeter metastases. Retrospective comparative studies on 18F-FDG PET and MRI reported that 18F-FDG PET detected only 61% of the metastases that were detected with MRI (13). Consequently, the diagnostic performance of integrated 18F-FDG PET/CT for the detection of brain metastases was found to be weak, with a maximum sensitivity, specificity, and accuracy of 50%, 97%, and 76% when MRI was used as the reference standard (14). On the other hand, in a prospective study 18F-FDG PET was shown to be valuable for the specification of morphologically indistinguishable contrast-enhancing lesions found on MRI, because a significantly higher maximal standardized uptake value (SUV) (4.1 ± 1.7) was found in cerebral metastases than in high-grade gliomas (1.9 ± 0.8) and benign lesions (0.6 ± 0.3) (15). In addition, dual-phase 18F-FDG PET is able to discriminate residual tumor from necrosis with 96% accuracy by measuring the increase in the ratio of lesion SUV to gray matter SUV (16), thus overcoming a common problem encountered in the interpretation of posttreatment MR images. Furthermore, imaging of the brain with PET is not restricted to the use of 18F-FDG as a radiotracer. 11C-choline PET, for example, yielded significantly higher detection rates than 18F-FDG PET (23/23 [100%] vs. 3/23 [13%]) in prospectively evaluated patients with cerebral metastases from thoracic cancer (17).
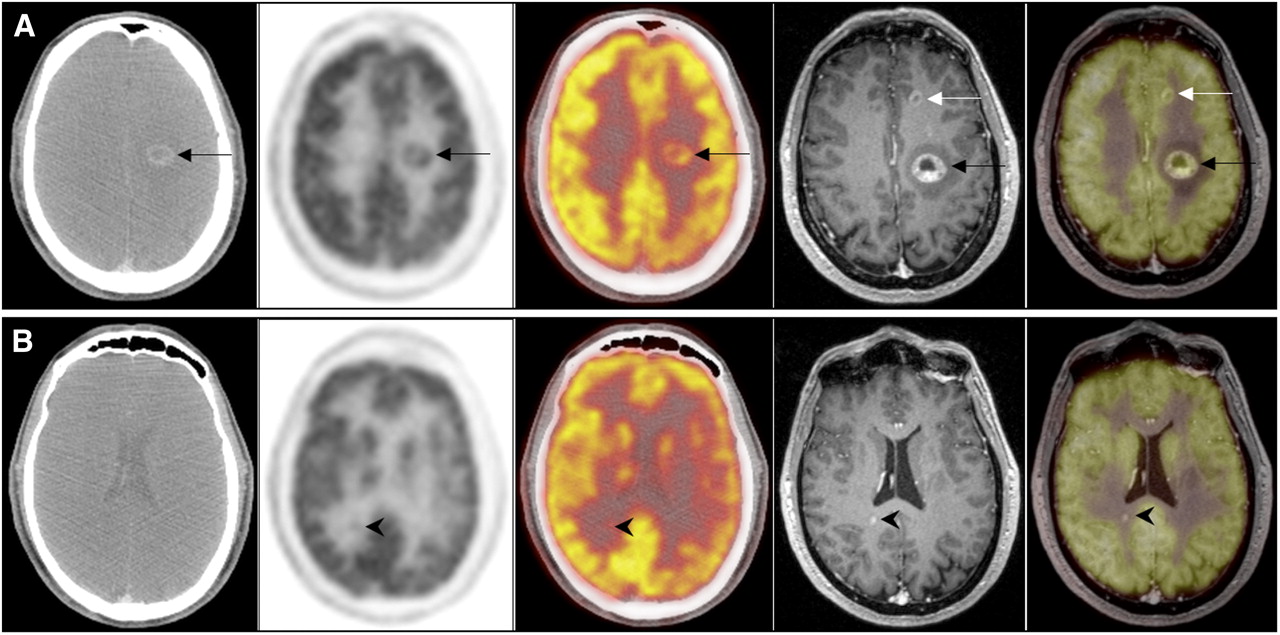
Integrated PET/MRI of the brain was the first application available in humans (18); research using this technique focused on evaluation of primary brain tumors (19) rather than detection of metastases but established the feasibility of integrated PET/MRI of the brain. Data on the diagnostic accuracy of integrated PET/MRI for the detection of cerebral metastases hence are not available at present. Staging the brain with PET/MRI will rely mostly on the MRI component, as indicated by the presented clear advantages of MRI over PET and PET/CT (Fig. 1). However, these data were taken from studies using dedicated brain MRI protocols. A prospective study on 32 consecutive patients with solid tumors provided evidence that MRI of the brain embedded in whole-body MRI protocols detects fewer brain metastases than do dedicated brain scans (17 vs. 40) (20). Thus, the best estimate of the awaited diagnostic performance of PET/MRI in brain metastasis detection is provided by whole-body MRI studies. Prospectively comparing the diagnostic accuracy of PET/CT and whole-body MRI for M-staging demonstrated that MRI, even if not performed as a dedicated brain scan, is more accurate than 18F-FDG PET/CT for the detection of cerebral metastases of different tumors (21). Whether the addition of functional MRI sequences, such as dynamic contrast-enhanced MRI and MR spectroscopy, will potentially benefit PET/MRI has not been considered so far.
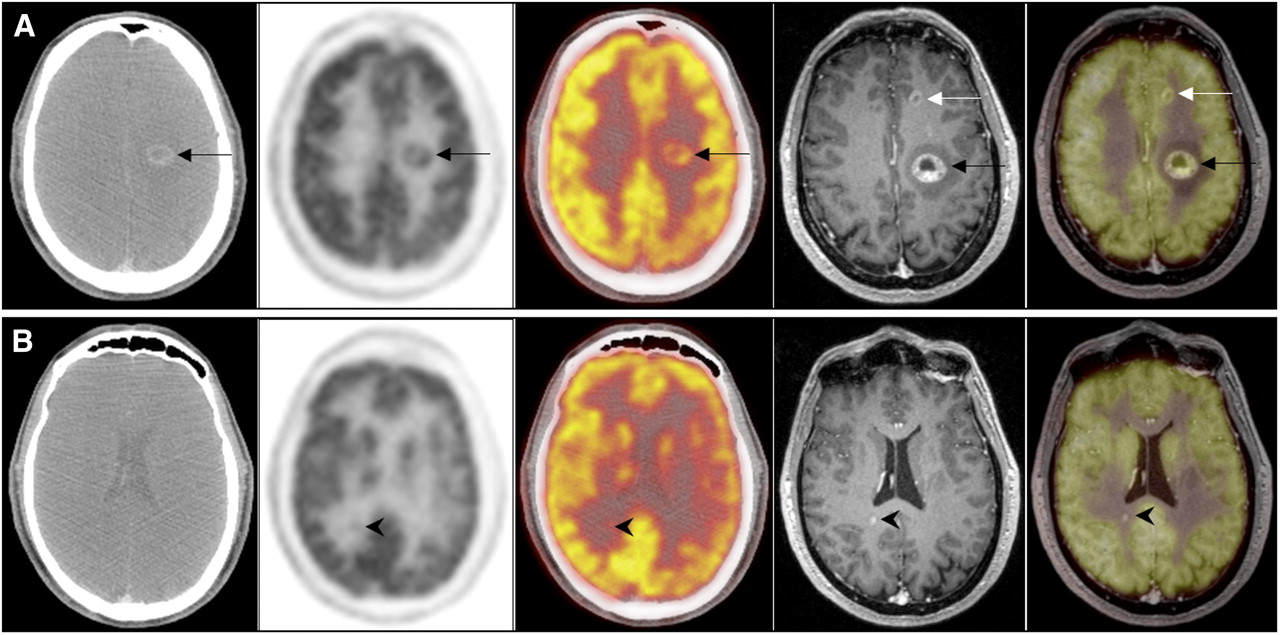
A 54-y-old patient with cerebral metastases from cancer of unknown primary. (A) Large left-hemisphere metastasis (black arrow) is visible on (from left to right) axial contrast-enhanced CT, 18F-FDG PET, PET/CT, axial contrast-enhanced MRI, and PET/MRI, whereas smaller metastasis of left frontal lobe (white arrow) is visible solely on MRI and PET/MRI. Location of this metastasis directly adjacent to highly 18F-FDG–avid cortex leads to problems with diagnosing this lesion on 18F-FDG PET scan. (B) Another subcentimeter-sized metastasis of right temporal lobe, clearly visible on MRI and PET/MRI of same patient (arrowhead), was only retrospectively seen as faintly increased 18F-FDG activity on 18F-FDG PET and PET/CT because of lack of anatomic correlate on CT.
HEAD AND NECK SQUAMOUS CELL CARCINOMA
Initial Diagnosis and T-staging
Although the initial diagnosis of squamous cell carcinoma (SCC)—the most important tumor entity of the head and neck area—is based on clinical and endoscopic findings, clinical inspection is regularly followed by imaging for confirmation of the suspected tumor and assessment of its extent. In recent years, PET/CT has broadly been applied for this indication and has been shown more accurate than CT alone for tumor detection and precise anatomic localization (22). The first report on integrated PET/MRI of head and neck cancer patients demonstrated superior tumor delineation (Figs. 2 and 3) and a good correlation between the metabolic ratios measured using PET/MRI and PET/CT (23). Nevertheless, reliable data on the diagnostic performance of PET/MRI to date still must be gained from studies using post hoc fusion images of MRI and PET datasets. The reported sensitivity of PET/MRI images for the detection of the primary tumor in patients with suspected head and neck SCC was 100% according to the results of a prospective study (24), but the same study revealed that PET/MRI had little additional value compared with MRI alone, as the diagnosis was changed in only 1 of 46 patients. In cases of cervical metastases from an unknown primary tumor, the diagnostic performance of PET/MRI to date is unknown. In a report with a limited cohort of 2 patients, a clinically occult carcinoma of the tonsil was detected by fused PET/MRI but not by stand-alone MRI (24). On the basis of the available data and initial experiences, PET/MRI in this field can be (or at least can be expected to be) as valuable as PET/CT, which has been reported to locate occult primary tumors in up to 39% of these patients (25). Considering these data from the literature, we have to acknowledge that cancer of unknown primary has not been defined consistently. If considering cancer of unknown primary as a tumor not detected even after imaging, endoscopy, and masked biopsies, the detection rate of the tumor with PET/CT goes down to 10% (in our own experience). It will be interesting to find out whether PET/MRI is able to improve this detection rate.

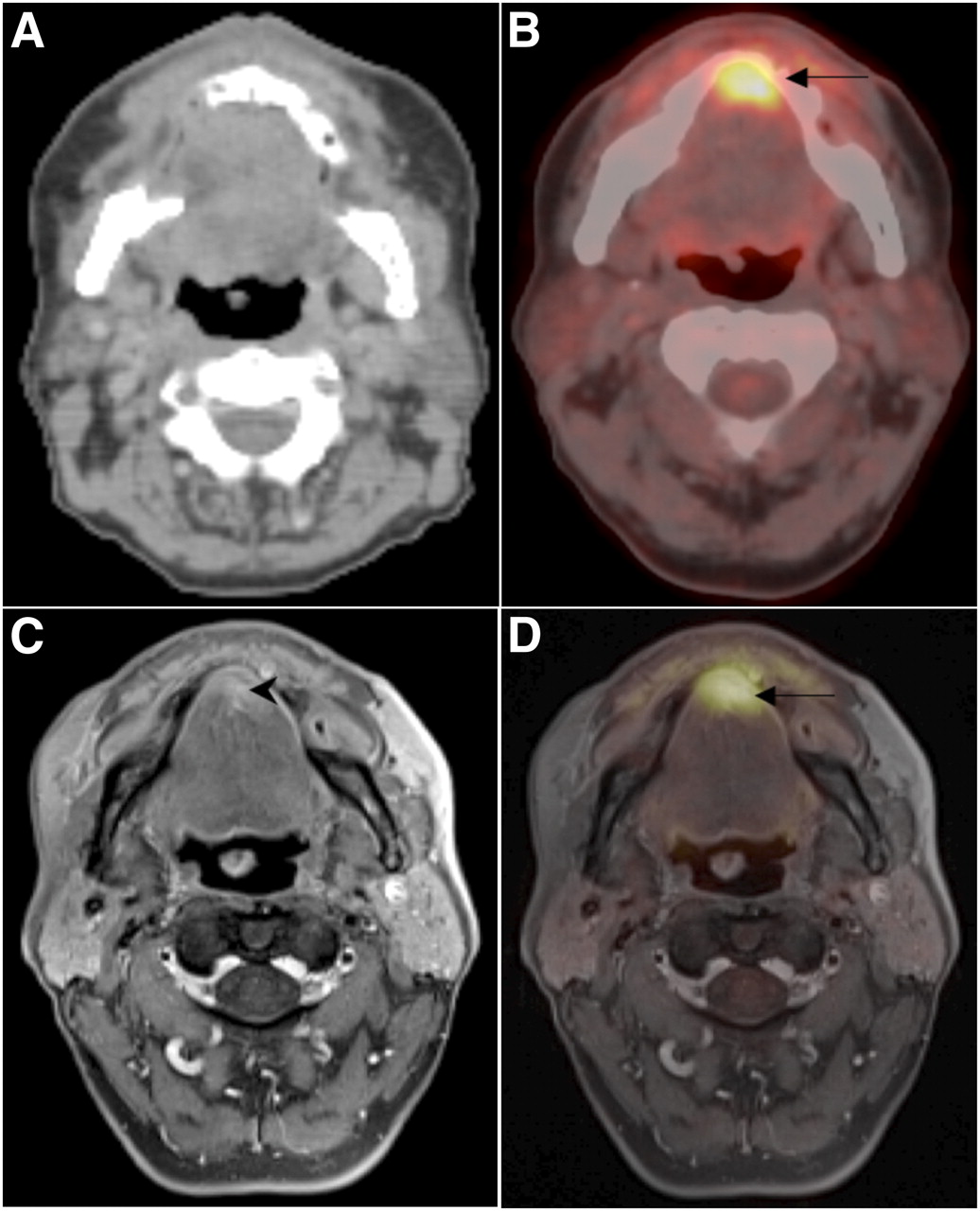
A 54-y-old man with gingival SCC arising from maxilla. Axial contrast-enhanced CT (A) shows poorly delineated soft-tissue mass (arrow) adjacent to right maxillary bone, which is clearly depicted on axial contrast-enhanced fat-suppressed T1-weighted MR image (C). 18F-FDG PET/MRI (D) facilitates more precise metabolic–anatomic allocation of 18F-FDG–avid mass than does 18F-FDG PET/CT (B).

A 66-y-old patient with SCC of tongue. Axial whole-body 18F-FDG PET/CT (B) shows 18F-FDG–avid lesion of tongue (arrow) without identifiable anatomic correlate on dedicated axial contrast-enhanced neck CT (A). Axial fat-suppressed T1-weighted MRI (C) shows contrast-enhancing mass of base of tongue (arrowhead). PET/MRI (D) shows that this tumor corresponds to 18F-FDG–avid lesion known from PET/CT.
N-Staging
For PET/MRI and the detection of metastasis in regional lymph nodes, a sensitivity, specificity, and accuracy of 85%, 92%, and 89% have been reported in a prospective trial (24). PET/MRI thus exceeded the diagnostic performance found in prospective PET/CT studies—a sensitivity of 78% and a specificity of 58% for lymph node staging (26). However, PET/MRI suffers from the same weakness: a substantial number of patients (6/20) with pathologically confirmed lymph node metastases were under-staged (24). Of these under-staged patients (n = 6), 1 patient was falsely staged N0 instead of N1. Even if this result is considered preliminary, it gives note to a well-known problem in PET/CT studies. Because of the limited spatial resolution and the dependence of tumor avidity on the radionuclide in use, small metastases or micrometastases in morphologically normal lymph nodes are frequently diagnosed by histologic work-up only (6). Combining MRI with 18F-FDG PET instead of CT may enhance diagnostic performance by adding functional MRI. MR DWI is capable of the detection of SCC metastases in normal-sized (<10-mm short-axis diameter) lymph nodes with a sensitivity of 76% (8), which has been a tremendous improvement when compared with morphologic MRI (7% sensitivity). Data on the combination of DWI and PET for lymph node staging in head and neck SCC are currently not available. Surgical staging by neck dissection remains the gold standard in head and neck cancer patients and most likely will not be replaced by PET/MRI.
Restaging and Response to Therapy
Metabolic–anatomic cross-sectional imaging is relevant to evaluation of the therapeutic response of head and neck SCC because of the high negative predictive value (NPV), which in cases of a negative posttherapeutic scan minimizes the risk of local or nodal tumor recurrence (27). A recent metaanalysis comprising 2,335 head and neck SCC patients revealed a pooled sensitivity, specificity, positive predictive value (PPV), and NPV of 79.9%, 87.5%, 58.6%, and 95.1%, respectively, for posttreatment 18F-FDG PET/CT of the primary tumor site. For the evaluation of nodal metastasis of the neck, these data were 72.7%, 87.6%, 52.1%, and 94.5%, respectively (28). A first prospective study on the value of PET/MRI in assessments for local tumor recurrence in head and neck SCC patients reported a sensitivity of 92% (24). On the basis of these first results, PET/MRI seems to improve therapy-response evaluation because of the combination of the high NPV (PET component) and the high sensitivity derived from the MRI component. Moreover, functional MRI techniques in combination with PET bear currently unused potential to further increase the performance of PET/MRI. Although the discrimination of reactively enlarged or inflammatory lymph nodes from residual or recurrent metastatic lymph nodes poses a problem that cannot be solved by PET/CT and results in false-positive findings and a low PPV of around 43% (29), MR DWI has been reported to perform well in exactly this setting, with a sensitivity and specificity of up to 93% (30).
TUMORS OF THE CHEST
Lung Tumors
Even with modern imaging sequences, such as contrast-enhanced T1 weighting with isotropic voxels, MRI is still less sensitive than CT for detection of pulmonary metastases. Prospective comparative studies on whole-body MRI and PET/CT have demonstrated the superiority of PET/CT over MRI in the detection of pulmonary metastases (139 vs. 170 pulmonary metastases) (Fig. 4) (4,21). This superior performance of PET/CT is based on CT accuracy rather than the PET data. On the other hand, MRI, including DWI sequences, has been shown to detect 100% of lung metastases larger than 7 mm found on CT (31), and the presence of small metastases below this cutoff size might be irrelevant to therapeutic decisions (32). There is also evidence that the lung-tissue contrast of MRI has the potential to be further improved by certain sequences—that is, half-Fourier, single-shot, turbo spin echo sequences (21). On the basis of the available evidence, the clinical launch of integrated PET/MRI is expected to have no benefit with regard to lung metastasis detection or primary pulmonary tumors. However, for the assessment of local tumor extent, MRI data can have benefits over CT. Local tumor infiltration into adjacent structures, such as the bronchial tree, pulmonary vessels, thoracic wall, or mediastinum, may be assessed more accurately with MRI because of its high soft-tissue contrast. Therefore, determination of the T-stage may be better with PET/MRI than with PET/CT. This question will, however, have to be addressed in future studies.
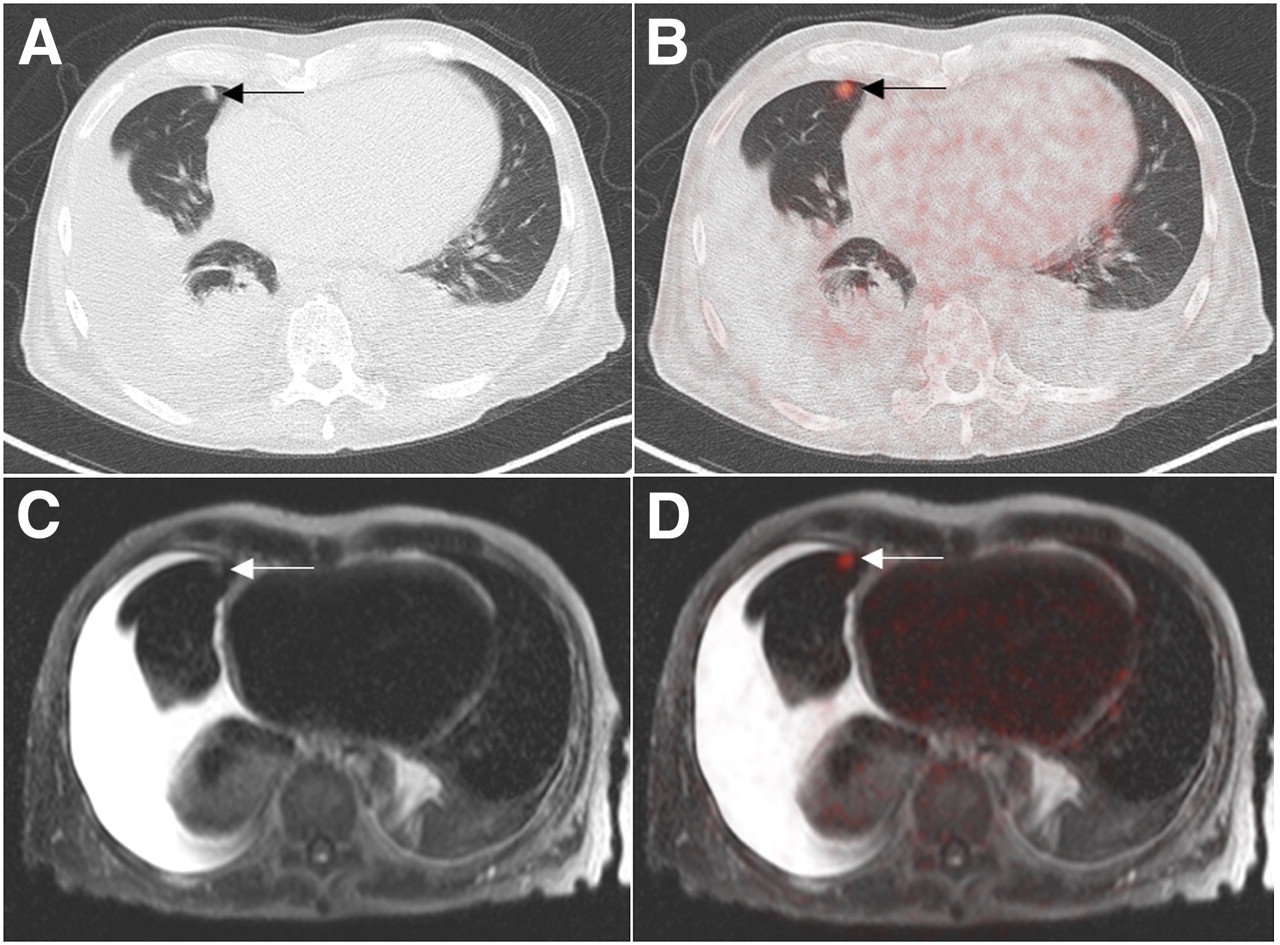
A 72-y-old patient with bronchial carcinoma of right hilum. Metastasis of right lung (arrows) found on CT (A) was confirmed by 18F-FDG–avid lesion on axial 18F-FDG PET/CT (B). This metastasis is hardly visible on whole-body MRI using half-Fourier, single-shot, turbo spin echo sequence (C), demonstrating superior contrast of lung tissue provided by CT. PET/MRI (D) demonstrates metastasis with increased 18F-FDG uptake.
Breast Cancer
Initial Diagnosis and T-Staging.
The awaited diagnostic performance of PET/MRI for the detection of primary breast cancer lesions and for the evaluation of local tumor extent can be deduced from several studies on software-based fusion of 18F-FDG PET and MR mammography datasets. For the detection of primary breast carcinomas, MR mammography itself is a sensitive imaging method that uses morphologic and functional parameters but lacks specificity and PPV and is strongly dependent on the reader’s degree of experience (33). In a prospective study on 36 patients, the addition of metabolic 18F-FDG PET information to MR mammography increased specificity for the detection of malignant breast lesions from 53% to 97% (34). This increase may also be expected for simultaneous PET/MRI of the breast. Our own group, however, did not find any statistically significant diagnostic benefit from software-based fusion of 18F-FDG PET and MR mammography (35) over MR mammography alone. Equivocal lesions on MRI are typically small, and these small lesions frequently do not show increased 18F-FDG uptake, even if they are malignant (in our own experience).
18F-FDG uptake has been reported to be a relevant prognostic factor in breast cancer patients, with higher SUVs indicating a poorer prognosis and being correlated with other predictors of a shorter survival such as tumor relapse, higher-grade tumors, and hormone receptor negativity (36). Hence, not only might 18F-FDG PET/MR mammography be of value for the delineation of local tumor extent, but the maximal SUV measurements might also help to estimate the prognosis of breast cancer patients. On the other hand, because of the limited sensitivity of the PET component when using 18F-FDG as the radiotracer, integrated PET/MRI will be liable to the same limitations in the detection of small breast tumors. In view of these false-negative findings with 18F-FDG PET in small lesions, and other pitfalls in the use of 18F-FDG PET for the breast (e.g., false-positive lesions such as 18F-FDG–avid fibroadenomas), the development of joint criteria and specific reading recommendations for PET/MRI mammography seems of the utmost importance.
N-Staging.
A recent metaanalysis on the diagnostic accuracy of MRI for the detection of axillary lymph node metastases reported a sensitivity and specificity of 90% (37). The reported sensitivity, specificity, PPV, NPV, and accuracy of 18F-FDG PET/CT for the detection of axillary lymph node metastases is 58%, 92%, 82%, 77%, and 79%, respectively (38). Both imaging modalities lead to false-negative and false-positive results and thus cannot compete with invasive staging procedures such as sentinel lymph node biopsy and axillary lymph node dissection. These restrictions are mainly due to the lack of ability to detect micrometastases, as morphologic criteria (small axis diameter, shape, loss of a fatty hilum, central necrosis, or hypervascularization) do not apply to micrometastases, nor do micrometastases show significant 18F-FDG uptake. Because of these premises, the awaited benefit of 18F-FDG PET/MRI for the detection of axillary lymph node metastases in breast cancer patients is rather low. From the clinical point of view regarding N-stage, PET/MRI will most likely be used just as PET/CT is—as a pretest before invasive staging with the chance to avoid unnecessary axillary lymph node dissections and to triage patients to an immediate therapeutic axillary lymph node dissection if extended axillary disease is detected (38). For the detection of extraaxillary lymph node metastases and distant metastases, PET/MRI, according to our first evaluation, is as accurate as 18F-FDG PET/CT (Fig. 5), which has excellent accuracy and a direct impact on patient management (39).
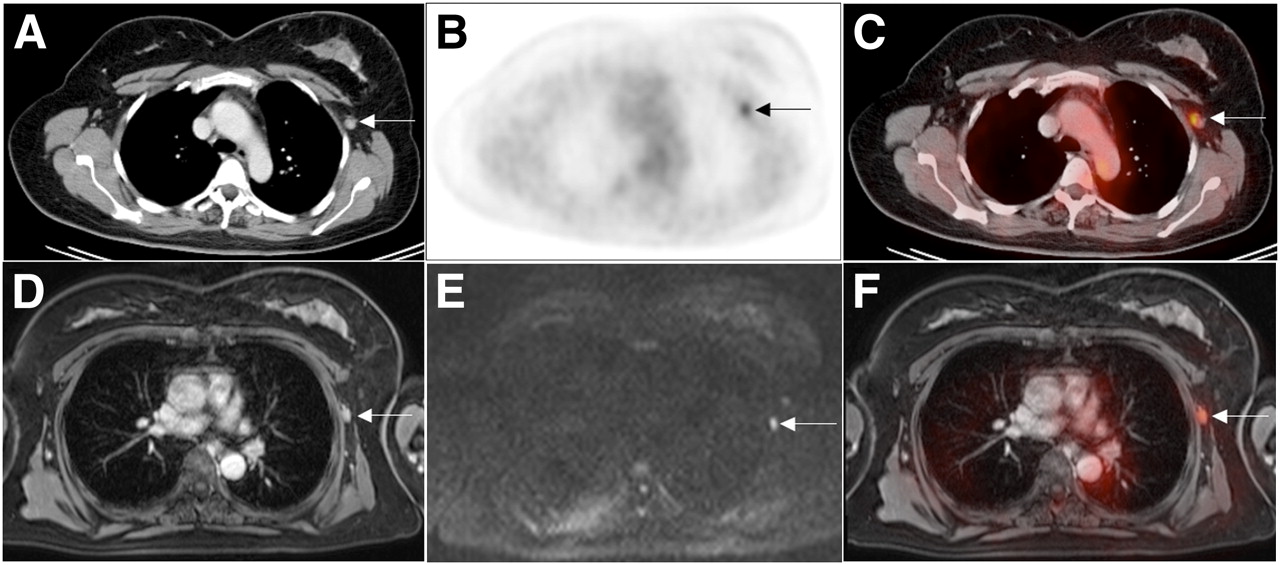
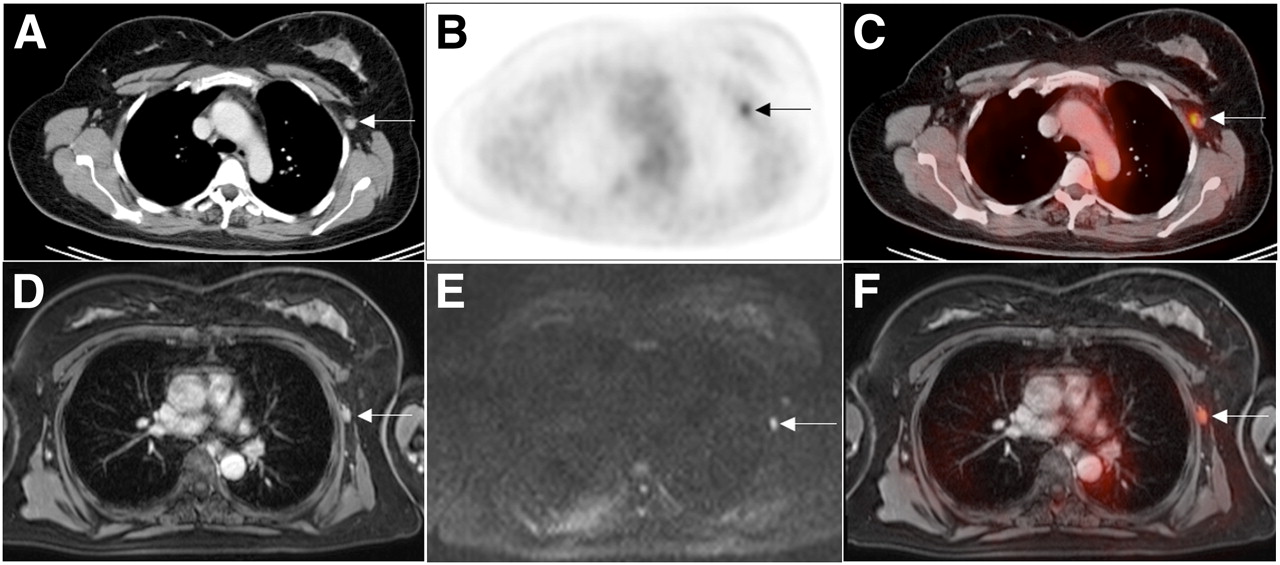
A 48-y-old patient with carcinoma of left breast. Axial contrast-enhanced CT (A), 18F-FDG PET (B), and 18F-FDG PET/CT (C), and axial contrast-enhanced fat-suppressed T1-weighted MRI (D), MR DWI (E), and 18F-FDG PET/MRI (F), all show lymph node metastasis of left axilla (arrows).
Restaging and Response to Therapy.
Both MRI and 18F-FDG PET are robust imaging modalities in the case of suspected breast cancer recurrence. 18F-FDG PET/CT, in a retrospective study, was proven to be an accurate modality for whole-body restaging of breast cancer patients, providing a sensitivity, specificity, PPV, NPV, and accuracy of 96%, 91%, 92%, 95%, and 94%, respectively (40). Especially in breast cancer patients with elevated tumor markers but negative or equivocal findings on conventional imaging, 18F-FDG PET/CT has a tremendous impact on therapeutic management (41). In view of a report that 80% of breast tumor patients have an incomplete pathologic response (42), reliable tools for the discrimination of responders from nonresponders or incomplete responders are required. In this regard, MRI is of distinct value for the prediction of pathologic complete response and the detection of residual disease, with an overall sensitivity, specificity, and accuracy of 81%, 93%, and 84%, respectively (43). The potential of MRI to assess therapeutic response is further enhanced when functional MRI techniques are added to the protocol. DWI, for example, has been shown to be sensitive to early response in a prospective study on 88 breast cancer patients undergoing neoadjuvant treatment (44). 18F-FDG PET is capable of predicting therapeutic response to neoadjuvant therapy significantly earlier than conventional imaging modalities and as early as after 1 or 2 chemotherapy cycles (45). The adequate and early differentiation of responders from nonresponders has strong and direct implications toward patient management, as ineffective therapies with potentially highly toxic side effects can be stopped and alternatives can be administered. Integrated PET/MRI, joining all the benefits of morphologic and functional MRI information and metabolic PET information, is most likely to acquire an established role in the diagnostic algorithm for breast cancer patients, potentially in the settings of tumor recurrence and neoadjuvant therapy.
TUMORS OF THE ABDOMEN AND PELVIS
Hepatocellular Cancer (HCC)
Initial Diagnosis and T-staging.
Data on the diagnostic performance of PET/MRI for the initial detection of hepatic primary tumors are not available. Through our evaluations of PET/CT over the past few years, we have found that 18F-FDG PET/CT is of limited use in the primary diagnosis of HCC, mainly because 18F-FDG PET has limited sensitivity for well-differentiated HCCs, which tend to be non–18F-FDG-avid (46). Prospective trials have reported that for the detection of HCC, 18F-FDG PET/CT has a sensitivity of around 64%–68% but that the sensitivity of PET may be improved by the use of radiotracers other than 18F-FDG (46,47). Using 11C-acetate (46) and 18F-fluorocholine (47), the sensitivity of PET for HCC primary tumor detection was reported to rise to 84% and 88%, respectively. Nonetheless, for the detection of small primary HCC (<2 cm), the soft-tissue contrast of liver MRI is clearly superior to that of PET, especially when liver-specific contrast material such as gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid (gadolinium-EOB-DTPA) or gadobenate acid (gadolinium-BOPTA) is applied. With liver-specific contrast material, sensitivities of around 85% have been reported in prospective studies (48,49). Moreover, the additional value of functional MRI techniques in combination with PET has to be considered: MR DWI, for example, has been demonstrated to significantly improve the detection of subcentimeter-sized intrahepatic metastasis of HCC compared with conventional liver MRI alone (84% vs. 69%) (50). If the high sensitivity of dedicated liver MRI and the obvious potential of functional MRI can be successfully transferred to combined PET/MRI, it can be expected to perform at least as well as MRI for the primary diagnosis of HCC. The major advantage of PET/MRI scanners in the diagnostic algorithm for HCC patients is the replacement, with a single examination, of sequential MRI acquisitions for evaluation of primary tumor extent and of PET/CT for whole-body staging.
N-staging.
Lymph node metastases occur predominantly in poorly differentiated or undifferentiated highly aggressive HCCs and thus are frequently 18F-FDG–avid (51). A prospective study found that PET in combination with morphologic imaging detected more lymph node metastases than did stand-alone CT and MRI (52). Again DWI, as an example of functional MRI, can provide additional information, such as discrimination between benign and malignant abdominal lymph nodes (53).
Restaging and Response to Therapy.
In the evaluation of tumor volume and viability, PET/MRI unites the metabolic information of PET, the high soft-tissue contrast of MRI, and functional MRI data. PET, by measuring tumor 18F-FDG uptake (SUV), serves as a tool for differentiation between HCCs with low biologic behavior and HCCs with highly aggressive biologic behavior. The aggressiveness of biologic behavior correlates with the volume-doubling time of HCC and thus is predictive of patient survival, with an inverse relation between SUV and survival rate (54). Furthermore, 18F-FDG PET/CT has proven useful for the detection of tumor recurrence in HCC patients after liver transplantation and interventional therapy, with an overall sensitivity, specificity, and accuracy of 90%, 83%, and 88%, respectively (55). In hybrid PET/MRI scanners, dynamic contrast-enhanced sequences can add to the restaging performance. For the detection of residual viable HCC with dynamic gadolinium-enhanced MRI after transarterial chemoembolization, a sensitivity of 68%, specificity of 100%, and accuracy of 72% have been reported (56). However, the small number of patients in that study makes the 100% specificity questionable, and further studies are required. In a retrospective evaluation of 44 patients who had undergone hepatic tumor resection, MR DWI was shown able to differentiate histopathologic grades of HCC tumors and predict early recurrence after resection (57). These results outline the high potential of functional MRI techniques such as dynamic contrast-enhanced MRI and DWI as partners in combination with PET. The exact sensitivity and specificity of PET/MRI for tumor recurrence are currently unknown. First experiences with patients undergoing PET/CT and PET/MRI after selective internal radiotherapy using 90Y-labeled particles have shown that PET/MRI improves therapeutic response assessment and early diagnosis of tumor recurrence over PET/CT (in our own experience).
Liver Metastases
Metastases to the liver are common in various malignancies and are far more frequent than primary hepatic cancers. The presence of hepatic metastases defines a high tumor stage, which is an important prognostic factor generally associated with a shorter overall survival (1). On the other hand, early and sensitive detection of liver metastases is desirable because resectioning of solitary lesions or palliative systemic and local interventional therapy for multiple hepatic metastases could prolong the patient’s survival (58). Beside ultrasonography, contrast-enhanced CT represents the standard diagnostic tool in liver imaging, with a sensitivity of up to 85% for the detection of metastases (59). Liver MRI with hepatobiliary contrast agents (gadolinium-EOB-DTPA or gadolinium-BOPTA) is the most accurate currently available imaging modality for the detection of small hepatic metastases (60). With a sensitivity, specificity, NPV, and PPV of 100%, 71%, 97%, and 100%, MRI outperforms 18F-FDG PET/CT (93%, 71%, 97%, and 57%) (60). 18F-FDG PET has been shown to be valuable in the response assessment of liver metastases undergoing systemic or local interventional therapy. 18F-FDG PET can solve the problem of distinguishing between a marginal zone of reactive hyperperfusion, which is frequently found at the rim of metastases on contrast-enhanced CT after radiofrequency ablation, and residual viable tumor tissue (61) and hence is superior to CT in radiofrequency ablation response assessment (65% vs. 44%) (62). Significantly reduced SUVs have been found in liver metastases from colorectal carcinoma with a pathologically confirmed response to systemic therapy, compared with nonresponsive metastases (63). Metastases treated by radiofrequency ablation that were found to be 18F-FDG PET–negative within 3 wk after treatment were less likely to relapse; in contrast, most persistently 18F-FDG PET–positive metastases recurred within the follow-up time of 16 mo (64). Recently, a change in maximal SUV between the preinterventional stage and 3 mo after selective internal radiation therapy of liver metastases from breast cancer was identified as the only independent predictive factor for patient survival (65). In this regard, functional MRI sequences and PET could provide complementary information on the viability of tumor tissue after therapy.
A study by Donati et al. on the diagnostic performance of PET/MRI compared fused 18F-FDG PET and gadolinium-EOB-DTPA–enhanced MRI retrospectively versus standalone gadolinium-EOB-DTPA–enhanced MRI and integrated PET/CT for liver lesion detection (66). In that study, PET/MRI, with a sensitivity and specificity of up to 93% and 96%, respectively, was significantly more accurate than PET/CT (76% and 85%, respectively). The evaluating radiologists rated PET/MRI as providing significantly greater confidence for discrimination between benign and malignant liver lesions. For the detection of hepatic lesions larger than 1 cm, PET/MRI had an area under the receiver-operating-characteristic curve of up to 0.96, representing a perfect test of this question. Compared with stand-alone MRI, PET/MRI led to a nonsignificant increase in sensitivity from 91% to 93%, with a slightly lower specificity of 96% for PET/MRI versus 100% for MRI alone. Interestingly, both gadolinium-EOB-DTPA–enhanced MRI and PET/MRI performed better than PET/CT for the detection and characterization of lesions smaller than 1 cm (66). Another study, on the diagnostic accuracy of retrospectively fused PET/MR images, was performed on patients who had neuroendocrine tumors with suspected liver metastases (67). In that study, 68Ga-DOTATOC, a radiolabeled somatostatin analog, was used for PET (68). Fusion 68Ga-DOTATOC and gadolinium-EOB-DTPA PET/MRI for the detection of hepatic neuroendocrine tumor metastases had a sensitivity, specificity, NPV, and PPV of 91%, 96%, 87%, and 97%, respectively, and compared with PET/CT (74%, 88%, 69%, and 93%, respectively) was significantly more accurate and slightly but not significantly more accurate than stand-alone MRI (88%, 87%, 83%, and 93%, respectively). A subanalysis on the influence of tumor grade revealed that stand-alone 68Ga-DOTATOC PET had a low sensitivity (5%) for metastases of poorly differentiated neuroendocrine tumors. In these tumors, the additional MRI information increased lesion detection over PET alone (67). In summary, both presented studies on PET/MRI for the detection of hepatic metastases attested a high accuracy for this technique that exceeded the performance of PET/CT (Fig. 6). It seems that MRI better compensates for the drawbacks in PET, especially in small hepatic lesions (67), and enhances reader confidence in lesion discrimination (66). However, PET/MRI does not seem to have any benefits over MRI alone.
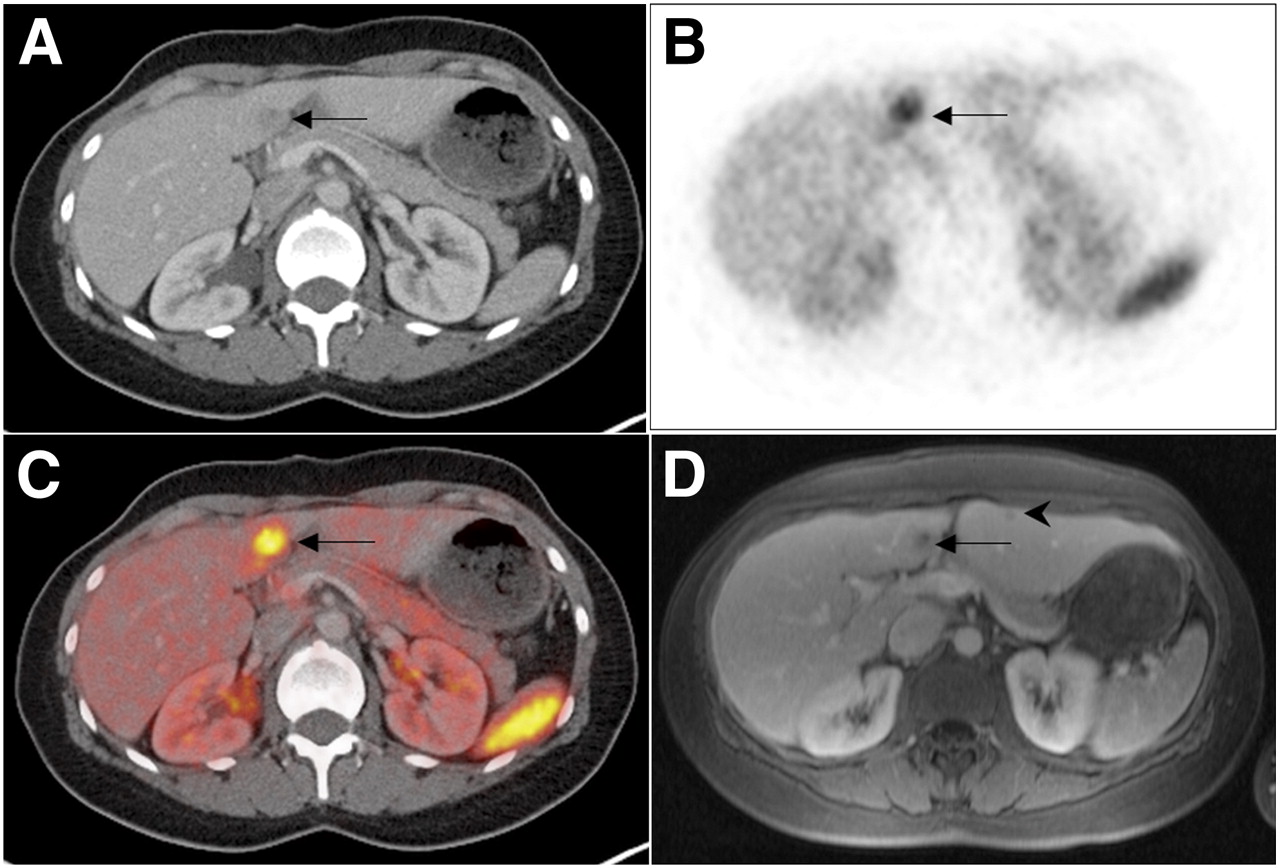
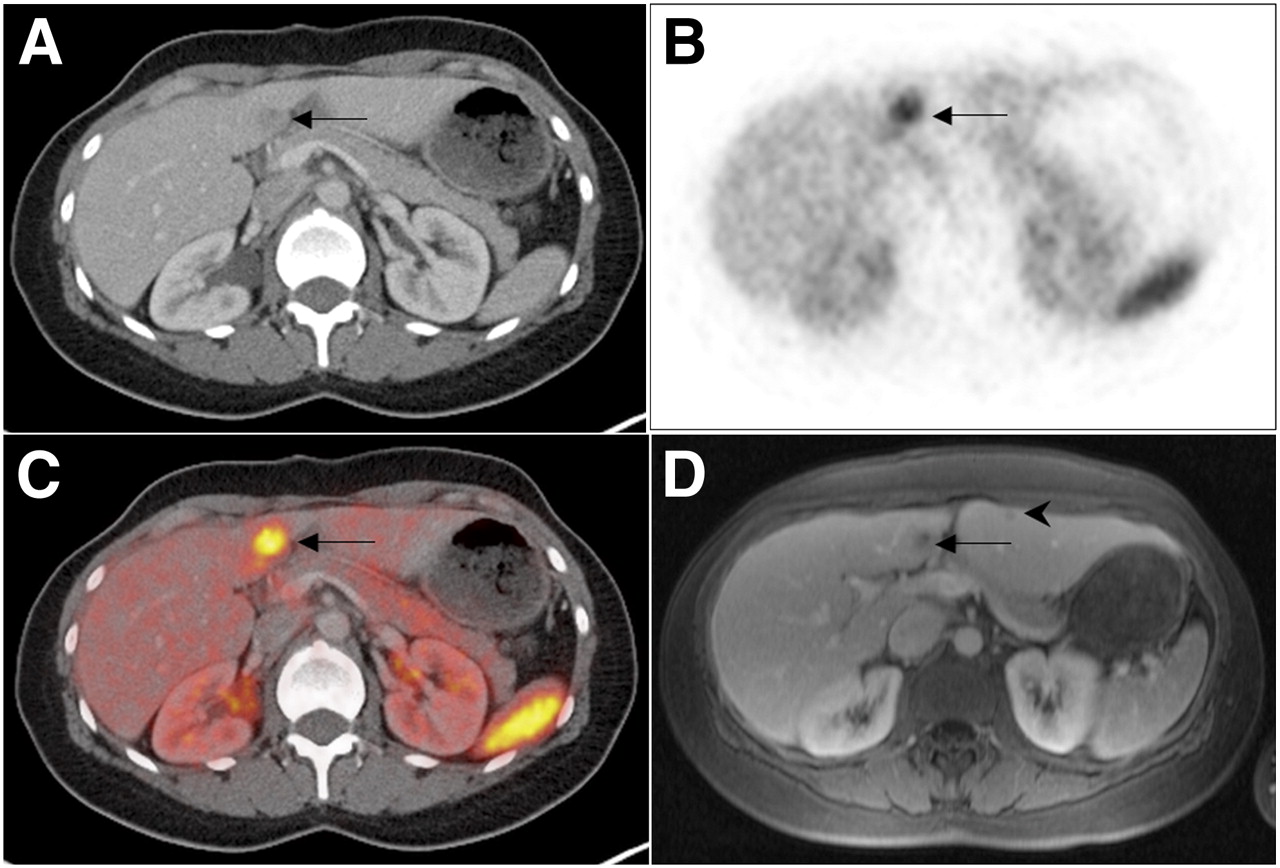
A 51-y-old patient with neuroendocrine tumor of small intestine. Axial contrast-enhanced CT (A) depicts metastasis to liver segment IV (arrow), which is strongly 68Ga-DOTATOC–avid on PET (B) and PET/CT (C). (D) Axial contrast-enhanced fat-suppressed T1-weighted MRI shows additional hypointense lesion in liver segment III (arrowhead) that was confirmed to be metastasis on follow-up.
Colorectal Cancer
Initial Diagnosis and T-Staging.
Software-based PET/MR images have been reported to provide no significant additional value in the preoperative staging of patients with rectal cancer, compared with pelvic MRI in conjunction with abdominal CT and chest radiography (69). The MRI component detected 100% of all rectal tumors (n = 23) but was inaccurate for the determination of tumor stage, as 11 of 23 patients were over-staged. The sensitivity and specificity of MRI for the T category of rectal cancer is 87% and 75%, respectively, based on the results of a recent metaanalysis (70). Besides endorectal ultrasonography, MRI is 1 of the 2 currently favorable preoperative imaging methods for assessment of the bowel wall and potential mesorectal infiltration (71) (Table 1). 18F-FDG PET cannot relevantly add to the accuracy of T-staging, as we learned from the application of 18F-FDG PET or 18F-FDG PET/CT to whole-body staging in colorectal cancer patients over the past few years (72). Despite the lack of reliable data, we assume that PET/MRI will not be better than MRI alone in the assessment of local tumor extent in colorectal cancer patients.
Indications in Which PET/MRI May Be Favorable over PET/CT, Depending on Tumor Entity
N-Staging.
The reported sensitivity of PET/MRI images for the detection of lymph node metastases in preoperative rectal carcinoma patients is only 44% (69). In the same retrospective analysis, a specificity and PPV of 100% and a NPV of 74% were reported. The authors reported that PET was never positive in the absence of positive lymph nodes on MRI; the pathologically determined size of metastases within lymph nodes rated positively on MRI ranged from 8 to 17 mm in that study (69). In a metaanalysis on the diagnostic performance of MRI for the detection of lymph node metastases, a sensitivity of up to 77% and a specificity of 71% were reported (70). Interestingly, the overall diagnostic accuracy for lymph node metastasis detection could be raised to 90% if 18F-FDG PET/CT and MRI were combined; the sensitivity, specificity, PPV, and NPV of combined MRI and 18F-FDG PET/CT were 94%, 83%, 89%, 91%, respectively (73). These initial experiences with PET/MRI reflect the general problem of lymph node micrometastasis detection with any imaging modality.
Restaging and Response to Therapy.
PET/MRI combines the advantages of MRI, functional MRI, and 18F-FDG PET for the assessment of therapeutic response and tumor relapse. MRI provides relevant prognostic information on colorectal cancer patients. In a retrospective evaluation, the tumor-free margin on preoperative MRI has been shown to be predictive of tumor recurrence and patient survival (74). For the assessment of this tumor-free distance to the mesorectal fascia, a recent metaanalysis showed MRI to be reliable, with a sensitivity and specificity of 77% and 94%, respectively (70). In locally advanced rectal cancer, a combination of morphologic and MR DWI could also predict the tumor clearance of the mesorectal fascia yielded by neoadjuvant radiochemotherapy (75). Furthermore, MR DWI has been reported to provide an imaging biomarker for tumor invasiveness. Lower apparent diffusion coefficient values correlated significantly with more aggressive tumor profiles, including high grades, high frequency of lymph node metastases, and invasion of the mesorectal fascia (76).
In patients with clinically suspected local recurrence, sensitivity ranged from 84% to 100% and specificity from 74% to 83% for conventional MRI, and an increase of diagnostic performance by adding functional MRI information (DWI) has been reported (77). Because of local changes after surgery or radiochemotherapy such as scar tissue or desmoplastic reactions, residual or locally recurrent tumors can be difficult to identify on the basis of morphologic criteria (78). In this setting, one would consider additional metabolic information desirable for a correct restaging. Tissue regeneration and inflammation, however, lead to increased 18F-FDG uptake on 18F-FDG PET. Because of this limitation, 18F-FDG PET/CT was not able to predict histopathologic tumor response after radiochemotherapy when scanning was performed shortly after therapy (79). The reported sensitivity, specificity, accuracy, PPV, and NPV of 18F-FDG PET/CT for the detection of local colorectal cancer recurrence were 84%, 88%, 87%, 76%, and 92%, respectively (80). In patients with suspected nonlocal recurrence, whole-body imaging is favorable for a complete restaging. PET/MRI integrates the advantages of MRI and 18F-FDG PET and thus may evolve as the first-line restaging modality in colorectal cancer patients with suspected tumor relapse or newly developed metastases.
CONCLUSION
Literature on truly integrated PET/MRI in oncologic applications is limited. The first experiences with this imaging technique report what may have been expected when the available data on whole-body MRI and PET/CT in oncology were considered. PET/MRI seems to be highly accurate in T-staging of those tumor entities for which MRI has traditionally been favored, such as SCCs of the head and neck. Thus, coupling PET with MRI will be clinically relevant in cases in which the soft-tissue contrast of MRI outperforms that of CT. With regard to N-staging, PET/MRI does not seem to provide a considerable benefit as compared with PET/CT but provides similar N-staging accuracy when applied as a whole-body staging approach. M-staging will benefit from MRI accuracy in the brain and the liver. The currently available literature focuses on 18F-FDG–based PET investigations. Specific radiotracers will have to be addressed in the future. Furthermore, the use of morphologic MRI techniques for the mere anatomic correlation of PET findings seems unlikely to tap the full potential of integrated PET/MRI. The true value of this new modality rather lies in the simultaneous acquisition of functional MRI parameters (e.g., DWI, dynamic contrast-enhanced MRI, and MR spectroscopy) and metabolic PET information. For this reason, the development of disease- and organ-specific PET/MRI protocols is a focus of the ongoing process of implementing this technique clinically. In summary, oncologic indications for PET/MRI will be defined by the soft-tissue contrast of MRI. All other indications will probably remain the domain of PET/CT.
Footnotes
Published online May 11, 2012.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the advantages and disadvantages of PET/MRI in oncologic applications in comparison to conventional imaging methods and PET/CT; (2) the limitations of PET/MRI compared with invasive staging procedures (biopsy); and (3) the metabolic–anatomic imaging procedure of choice (PET/MRI vs. PET/CT) based on tumor entity and location.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through June 2013.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- Received for publication March 19, 2012.
- Accepted for publication May 2, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET/MRI Versus PET/CT for Whole-Body Staging: Results from a Single-Center Observational Study on 1,003 Sequential Examinations
- MR/PET Imaging of the Cardiovascular System
- Prospective Evaluation of the Clinical Implications of the Tumor Metabolism and Chemotherapy-Related Changes in Advanced Biliary Tract Cancer
- Feasibility of Multiparametric Imaging with PET/MR in Head and Neck Squamous Cell Carcinoma
- Comparative Performance of 18F-FDG PET/MRI and 18F-FDG PET/CT in Detection and Characterization of Pulmonary Lesions in 121 Oncologic Patients
- Evaluation of the Outcome of Lung Nodules Missed on 18F-FDG PET/MRI Compared with 18F-FDG PET/CT in Patients with Known Malignancies
- Hybrid 18F-labeled Fluoride Positron Emission Tomography/Magnetic Resonance (MR) Imaging of the Sacroiliac Joints and the Spine in Patients with Axial Spondyloarthritis: A Pilot Study Exploring the Link of MR Bone Pathologies and Increased Osteoblastic Activity
- Qualitative and Quantitative Performance of 18F-FDG-PET/MRI versus 18F-FDG-PET/CT in Patients with Head and Neck Cancer
- Potential Pediatric Applications of PET/MR
- Application of FDG-PET in Cervical Cancer and Endometrial Cancer: Utility and Future Prospects
- Combination of 18F-FDG PET/CT and Diffusion-Weighted MR Imaging as a Predictor of Histologic Response to Neoadjuvant Chemotherapy: Preliminary Results in Osteosarcoma