


Abstract
Compliance with radiobiologic principles of radionuclide internal dosimetry is fundamental to the success of 90Y radioembolization. The artery-specific SPECT/CT partition model is an image-guided personalized predictive dosimetric technique developed by our institution, integrating catheter-directed CT hepatic angiography (CTHA), 99mTc-macroaggregated albumin SPECT/CT, and partition modeling for unified dosimetry. Catheter-directed CTHA accurately delineates planning target volumes. SPECT/CT tomographically evaluates 99mTc-macroaggregated albumin hepatic biodistribution. The partition model is validated for 90Y resin microspheres based on MIRD macrodosimetry. Methods: This was a retrospective analysis of our early clinical outcomes for inoperable hepatocellular carcinoma. Mapping hepatic angiography was performed according to standard technique with the addition of catheter-directed CTHA. 99mTc-MAA planar scintigraphy was used for liver-to-lung shunt estimation, and SPECT/CT was used for liver dosimetry. Artery-specific SPECT/CT partition modeling was planned by experienced nuclear medicine physicians. Results: From January to May 2011, 20 arterial territories were treated in 10 hepatocellular carcinoma patients. Median follow-up was 21 wk (95% confidence interval [CI], 12–50 wk). When analyzed strictly as brachytherapy, 90Y radioembolization planned by predictive dosimetry achieved index tumor regression in 8 of 8 patients, with a median size decrease of 58% (95% CI, 40%–72%). Tumor thrombosis regressed or remained stable in 3 of 4 patients with baseline involvement. The best α-fetoprotein reduction ranged from 32% to 95%. Clinical success was achieved in 7 of 8 patients, including 2 by sublesional dosimetry, in 1 of whom there was radioembolization lobectomy intent. Median predicted mean radiation absorbed doses were 106 Gy (95% CI, 105–146 Gy) to tumor, 27 Gy (95% CI, 22–33 Gy) to nontumorous liver, and 2 Gy (95% CI, 1.3–7.3 Gy) to lungs. Across all patients, tumor, nontumorous liver, and lungs received predicted ≥91 Gy, ≤51 Gy, and ≤16 Gy, respectively, via at least 1 target arterial territory. No patients developed significant toxicities within 3 mo after radioembolization. The median time to best imaging response was 76 d (95% CI, 55–114 d). Median time to progression and overall survival were not reached. SPECT/CT-derived mean tumor–to–normal liver ratios varied widely across all planning target volumes (median, 5.4; 95% CI, 4.1–6.7), even within the same patient. Conclusion: Image-guided personalized predictive dosimetry by artery-specific SPECT/CT partition modeling achieves high clinical success rates for safe and effective 90Y radioembolization.
- 90Y radioembolization
- 90Y selective internal radiation therapy
- catheter-directed CT hepatic angiography
- 99mTc-macroaggregated albumin SPECT/CT
- partition model MIRD macrodosimetry
As a form of arterial territory–specific point-source brachytherapy, 90Y radioembolization is always effective when delivered at the right location, in the right dose, and with the right intent. 90Y radioembolization failure is invariably due to one or a combination of these 3 factors being incorrectly addressed. Responsibility for this triad of factors is shared among the interventional radiologist, the nuclear medicine physician, and the referring clinician. 90Y radioembolization is complex, and a lack of coordinated care risks suboptimum outcomes.
Contemporary techniques, outcomes, and safety data of 90Y radioembolization are well described in recent literature (1–8). Disregard for radiobiologic principles of arterial territory–specific 90Y radionuclide internal dosimetry risks toxicity and fatality (9,10). Since the 1980s, sectional imaging (e.g., CT) has revolutionized the planning and delivery of external-beam radiation therapy. However, to date, radiation planning for 90Y radioembolization has yet to embrace modern imaging modalities such as catheter-directed CT hepatic angiography (CTHA) and SPECT with integrated low-dose CT (SPECT/CT).
Catheter-directed CTHA delineates hepatic arterial territorial margins more accurately than digital subtraction angiography (1,11). SPECT/CT is superior to both planar scintigraphy and SPECT for assessing intrahepatic biodistribution of 99mTc-macroaggregated albumin (99mTc-MAA), and for estimating the tumor-to-normal liver (T/N) ratio (12–14). The partition model is a validated dosimetric method for 90Y resin microspheres, scientifically superior to the body surface area (BSA) method (5,10).
Accurate assessment of target liver volumes is critical because it directly affects radiation absorbed dose estimates. This is especially important when planning for selective (lobar) or superselective (segmental or subsegmental) 90Y radioembolization. Catheter-directed CTHA refers to the acquisition of CT with direct intraarterial injection of dilute contrast medium through an angiographic catheter or microcatheter introduced into a hepatic lobar, segmental, or subsegmental artery via a percutaneous transfemoral arterial puncture (1,11). This technique provides superior delineation of arterial territories compared with digital subtraction angiography, enabling accurate estimation of artery-specific perfused liver volumes (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org) (1,11). Conventional 90Y radioembolization is planned on the interventional radiologists’ assessment of each patient's vascular anatomy (15). However, estimation of the perfused liver volume can be challenging. Hepatic vascular anatomy has many variations (13,15,16). A main hepatic artery may supply several liver segments via its branches; conversely, a single segment may be supplied by more than a single arterial branch. Couinaud segments may be distorted by large tumors, previous liver surgery, or locoregional therapy—for example, ablation cavities. Aberrant arteries due to neoplastic recruitment from extrahepatic sources further complicate hepatic vascular anatomy. These factors make it difficult to reliably estimate the target volume of a diseased liver on the basis of digital subtraction angiography alone.
This problem may be overcome by catheter-directed CTHA. With the catheter tip placed in the target artery, CT performed at the time of intraarterial contrast injection provides superior delineation of the perfused liver volume, as compared with that shown under digital subtraction angiography. Each run of catheter-directed CTHA is specific for its catheter tip position. The use of catheter-directed CTHA shifts the planning emphasis away from a conventional lobe- or segment-based approach to a more patient-specific arterial territory–based approach. Catheter-directed CTHA accurately delineates each target arterial territory regardless of arterial anatomy, variant vasculature, or tissue distortion by tumor, surgery, or locally ablative treatments.
The role of SPECT/CT in diagnostic imaging and internal dosimetry is well established in nuclear medicine (17,18). In the context of 90Y radioembolization, 99mTc-MAA SPECT/CT for preradioembolization assessment has a higher detection rate for extrahepatic radiotracer activity and has greater impact on therapy planning than does planar scintigraphy (14,19,20). Hepatic intraarterial 99mTc-MAA scintigraphy is a validated means of simulating the 90Y radioembolization therapy field (13,14). SPECT/CT-based dosimetry is superior to planar scintigraphy by tomographically resolving overlapping radiotracer activity, evaluating heterogeneous radiotracer uptake, and detecting activity in small lesions (12,14,17). Phantom studies have shown that 99mTc-MAA SPECT/CT volume measurements are accurate and reproducible (13). To date, no standardized technique exists for the calculation of SPECT/CT-based T/N ratios, although several methods have been described (21–23).
The partition model was developed and validated for 90Y resin microspheres by Ho et al. in the 1990s (24,25). It is one of several methods recommended by the manufacturer of 90Y resin microspheres to calculate the desired 90Y activity (26). Based on MIRD macrodosimetry, it partitions the lungs, tumor, and nontumorous liver into separate compartments for radiation dose modeling (24,26). This model surpasses the commonly used BSA method by incorporating absolute tissue masses and patient-specific mean T/N ratios for personalized and scientifically sound estimates of mean radiation absorbed doses to each tissue compartment (5,10,27). Technical differences between BSA methodology and partition modeling are discussed elsewhere, along with limitations and clinical implications (10).
The artery-specific SPECT/CT partition model is a unified technique of personalized predictive dosimetry developed by our institution for 90Y radioembolization using resin microspheres. It integrates catheter-directed CTHA, 99mTc-MAA SPECT/CT, and partition modeling for improved predictive radionuclide dosimetry (supplemental data). Its fundamental premise is to derive more accurate estimates of tissue masses and mean T/N ratios to optimize partition modeling. The underlying principles and limitations of MIRD macrodosimetry remain unchanged. Through the use of artery-specific SPECT/CT partition modeling, predicted mean radiation absorbed doses specific to target arterial territories are independently calculated and physician-adjusted according to patient-specific circumstances (e.g., mean T/N ratio, liver-to-lung shunt, liver reserve, prognosis, treatment intent, and potential treatment benefit). The overall process yields a personalized image-guided predictive radiation plan for safe and effective 90Y radioembolization. This report provides a technical overview of this integrated dosimetric technique and details our early clinical outcomes in patients with inoperable hepatocellular carcinoma (HCC).
MATERIALS AND METHODS
The institutional review board waived the need to obtain informed consent for this retrospective analysis. The technique for using artery-specific SPECT/CT partition modeling to plan 90Y radioembolization was implemented at our institution as a routine clinical service in January 2011. Five months after implementation, we had treated 22 patients with inoperable HCC. Of these, 10 were embargoed under an ongoing clinical trial. The treatment of 2 patients was planned by BSA methodology because of morphologically diffuse and infiltrative tumors that were below the resolution of 99mTc-MAA SPECT/CT, thus precluding reliable region-of-interest contouring. Both these patients were excluded (10). Treatment of the remaining 10 consecutive patients was planned by artery-specific SPECT/CT partition modeling, and these patients were eligible for inclusion into this report. Retrospective review of hospital medical records was performed for these 10 patients until August 2011, the time at which the manuscript was prepared.
Patient and baseline disease characteristics were highly heterogeneous (Supplemental Tables 1 and 2). Median age was 59 y (range, 48–65 y). There were 8 men and 2 women. Seven patients had chronic viral hepatitis. Five patients received prior therapy for HCC, including 2 with previous 90Y radioembolization planned by conventional planar partition modeling. Eight patients were Child–Pugh A; the remainder were Child–Pugh B. Tumor extent varied widely across all patients and was mostly bilobar and multifocal. Eight patients had T4 disease according to the staging system of the United Network for Organ Sharing; none had nodal or distant metastases. Classification by the staging system of the Barcelona Clinic Liver Cancer was stage A for 1 patient, stage B for 3, stage C for 5, and stage D for 1. Five patients had tumor vascular involvement.
Technique Overview
Mapping hepatic angiography and 99mTc-MAA injection were performed according to standard technique (1,15). Prophylactic coil embolization of vessels at risk was performed either at mapping hepatic angiography or at 90Y radioembolization, at the discretion of the interventional radiologist. The catheter tip position for 99mTc-MAA injection was decided by consensus between the interventional radiologist and nuclear medicine physician during mapping hepatic angiography. 99mTc-MAA was slowly hand-injected nonselectively (whole liver), selectively (lobar), or superselectively (segmental or subsegmental), depending on patient-specific circumstances (supplemental data). Patients were immediately transferred to the γ-camera suite for planar liver-to-lung shunt scintigraphy and SPECT/CT of the abdomen.
Technical aspects of artery-specific SPECT/CT partition modeling are detailed in the supplemental data. In essence, catheter-directed CTHA guides volume-of-interest delineation on 99mTc-MAA SPECT/CT to obtain arterial territory–specific tissue volumes and SPECT/CT-based mean T/N ratio estimates for improved partition modeling. The phrase planning target volume is introduced, adapted from external-beam radiation therapy. All treatments were planned by a team of experienced nuclear medicine physicians, and the final prescribed mean radiation absorbed doses were guided by published dose–response relationships (5). By partition modeling, the nuclear medicine physician had full control over predicted radiation absorbed dose estimates to tumor, nontumorous liver, and lungs within each planning target volume. The overall dosimetric aim was to balance the desired mean tumor radiation absorbed dose with collateral radiation injury, in accordance with the treatment intent. Illustrated online resources and worked examples are freely downloadable from our Web site to aid in understanding this dosimetric technique (supplemental data).
90Y radioembolization was performed using resin microspheres (SIR-Spheres; Sirtex Medical Ltd.) within 2 wk of mapping hepatic angiography. Catheter tip placement was the same as that for the 99mTc-MAA injections. All patients received prophylactic omeprazole, 20 mg, twice daily before 90Y radioembolization, and this treatment continued for at least 6 wk after radioembolization. In accord with our institutional protocol, after 90Y radioembolization all patients were observed overnight and discharged after bremsstrahlung planar scintigraphy of the lung and SPECT/CT of the abdomen the following day.
Terms and Definitions
Postradioembolization bremsstrahlung SPECT/CT of the abdomen was used to determine technical success. Our bremsstrahlung scan protocol is detailed in the supplemental data. Technical success was achieved when all targeted tumors within planning target volumes showed satisfactory bremsstrahlung activity by visual assessment, in keeping with the radiation plan (28). The success of the technique was considered indeterminate when planning target volumes included subcentimeter tumors or tumors with ill-defined margins (e.g., infiltrative HCC), below bremsstrahlung SPECT/CT spatial resolution. A technical failure occurred when targeted tumors did not exhibit visually detectable focal bremsstrahlung activity, analogous to a geographic miss in the context of external-beam radiation therapy.
Clinical and biochemical toxicities within 3 mo after radioembolization were classified according to Common Terminology Criteria for Adverse Events (version 4.03) (28,29). The nadir in serum α-fetoprotein at any time after radioembolization indicated the best biochemical response.
To evaluate the effectiveness of 90Y radioembolization strictly as a form of brachytherapy delivered at a single time point, the best imaging response was defined as the greatest change in size of the targeted index (largest) tumor between baseline and follow-up diagnostic sectional imaging. Clinical success was defined as any degree of regression of targeted tumors on follow-up diagnostic sectional imaging within planning target volumes, regardless of new tumors appearing within or outside planning target volumes (28).
Overall response according to the Response Evaluation Criteria in Solid Tumors (version 1.1), the criteria of the World Health Organization, and the 2-dimensional criteria of the European Association for the Study of the Liver were used to evaluate 90Y radioembolization as a part of comprehensive multimodality therapy for inoperable HCC, without regard to planning target volumes (28,30).
Statistical Methods
Data are presented as median and 95% confidence intervals (CI), where applicable. Using Bland–Altman analysis, the total desired 90Y activities calculated by artery-specific SPECT/CT partition modeling were compared with those hypothetically derived by BSA methodology. The intraclass correlation coefficient was calculated, with values 0.8 or more considered excellent; 0.6–0.8, good; 0.4–0.6, moderate; and less than 0.4, poor. Statistical analysis was performed on Office Excel 2003 software (Microsoft Corp.) and SPSS software (version 17.0; SPSS Inc.).
RESULTS
The artery-specific SPECT/CT dosimetric plans of all 10 patients are summarized in Supplemental Table 10. There were a total of 20 radiation plans across 10 patients, that is, a single planning target volume per target arterial territory. Two patients underwent 90Y radioembolization in a single arterial territory (Supplemental Fig. 2), 6 patients in 2 arterial territories, and 2 patients in 3 arterial territories (Fig. 1). Sublesional dosimetry was performed for 2 patients (Supplemental Figs. 3 and 4), in 1 of whom there was radioembolization lobectomy intent (Figs. 2 and 3). Four patients underwent prophylactic coil embolization of arteries at risk: 3 gastroduodenal, 2 accessory left gastric, 2 right gastric, 1 right inferior phrenic, 1 falciform, and 1 pancreaticoduodenal arcade. Technical success was achieved in 2 of 10 patients, indeterminate success in 7, and technical failure in 1. Patient 8 was classified as a technical failure because of the absence of visually detectable focal bremsstrahlung activity in a targeted caudate tumor.

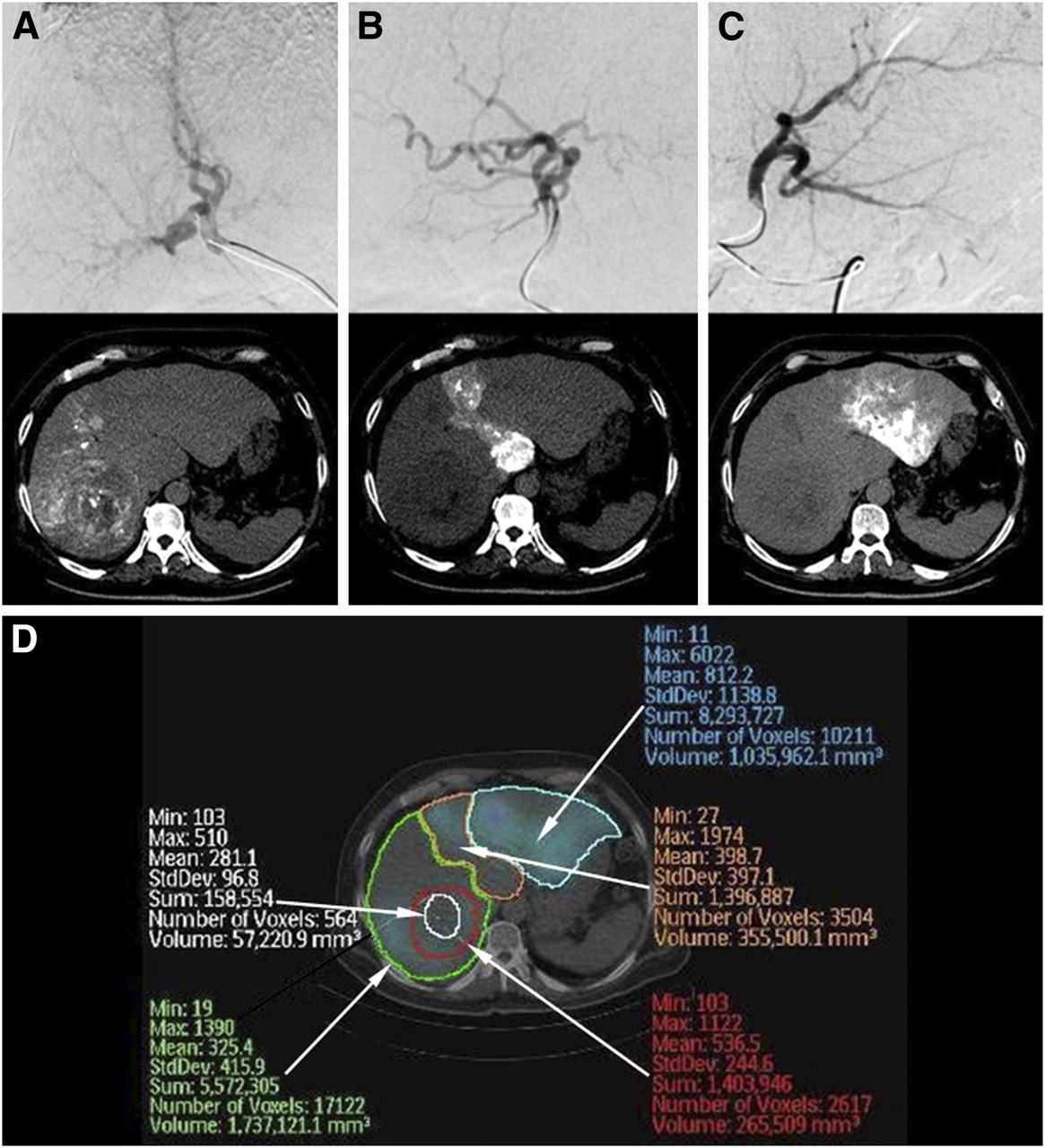
Example of artery-specific SPECT/CT partition modeling of 3 arterial territories. (A–C) Liver with multifocal HCC supplied by right (A), middle (B), and left (C) hepatic arteries is depicted in digital subtraction angiography (top) and catheter-directed CTHA (bottom). (D) Regions of interest (ROI) are drawn on 99mTc-MAA SPECT/CT transaxial slices representing left (blue ROI), middle (orange ROI), and right (green ROI) hepatic artery planning target volumes, implanted tumor (red ROI), and necrotic tumor (white ROI).

Example of sublesional dosimetry with left radioembolization lobectomy intent. Patient 2 had recurrent HCC at segment IV resection margin. Tumor was supplied by right and left hepatic arteries. (A and B) Catheter-directed CTHA depicts planning target volumes of right (A) and left (B) hepatic arteries, dividing dosimetric plan into 2 independent halves for sublesional dosimetry. Left lobe hypodensity is cyst. (C) 99mTc-MAA SPECT/CT shows good T/N ratio (6.1) of lateral tumor portion supplied by right hepatic artery but poor T/N ratio (1.4) of medial tumor portion supplied by left hepatic artery. Dosimetric plan of left hepatic artery planning target volume was deliberately escalated beyond safe limits to achieve predicted mean radiation absorbed dose of 133 Gy to tumor and 93 Gy to nontumorous liver, where progressive atrophy of left lobe was the anticipated collateral effect, that is, left radioembolization lobectomy intent. (D) Postradioembolization bremsstrahlung SPECT/CT shows good tumoral activity in both lateral and medial tumor portions, indicating technical success. C = cyst; L = left hepatic artery; Lat = lateral; Med = medial; R = right hepatic artery.
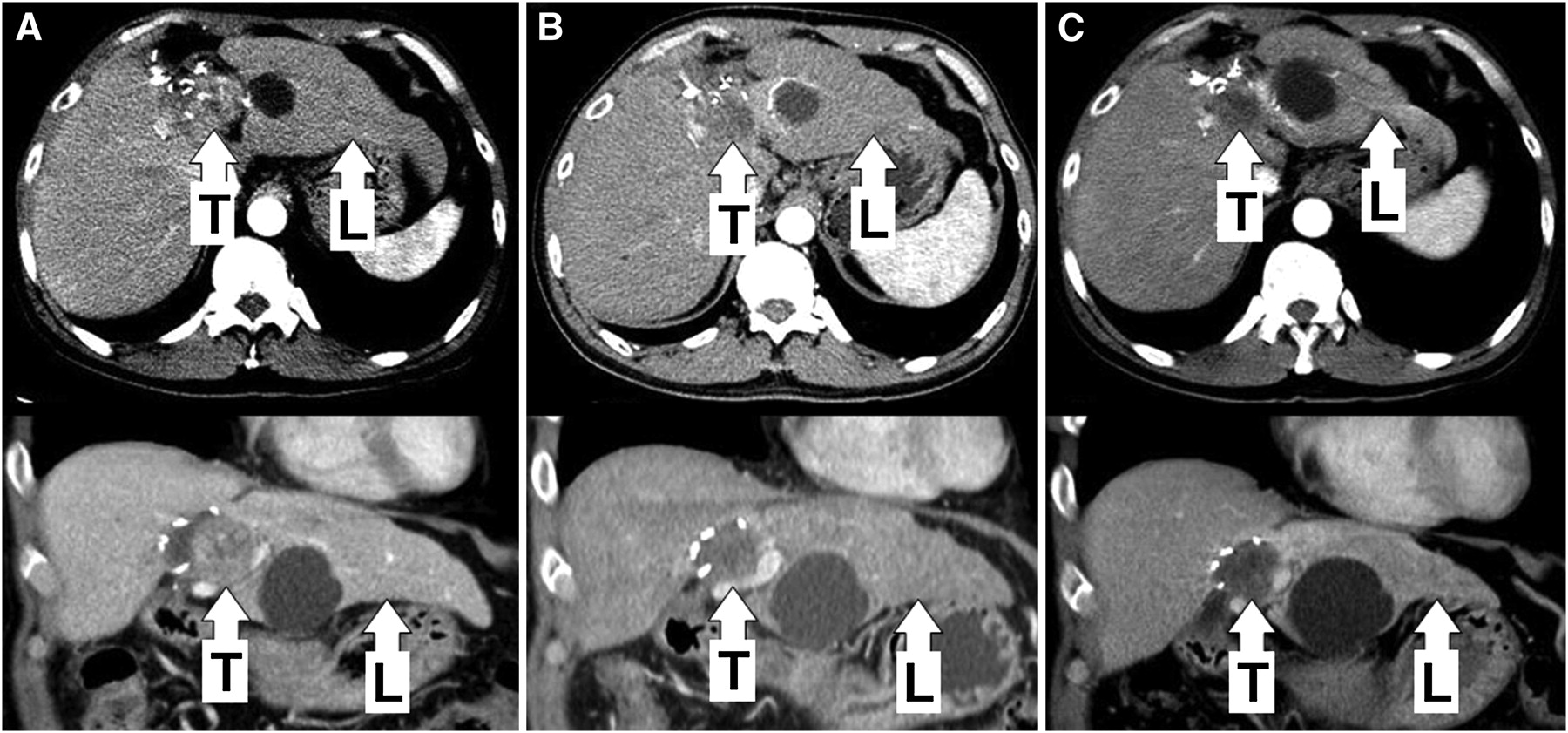
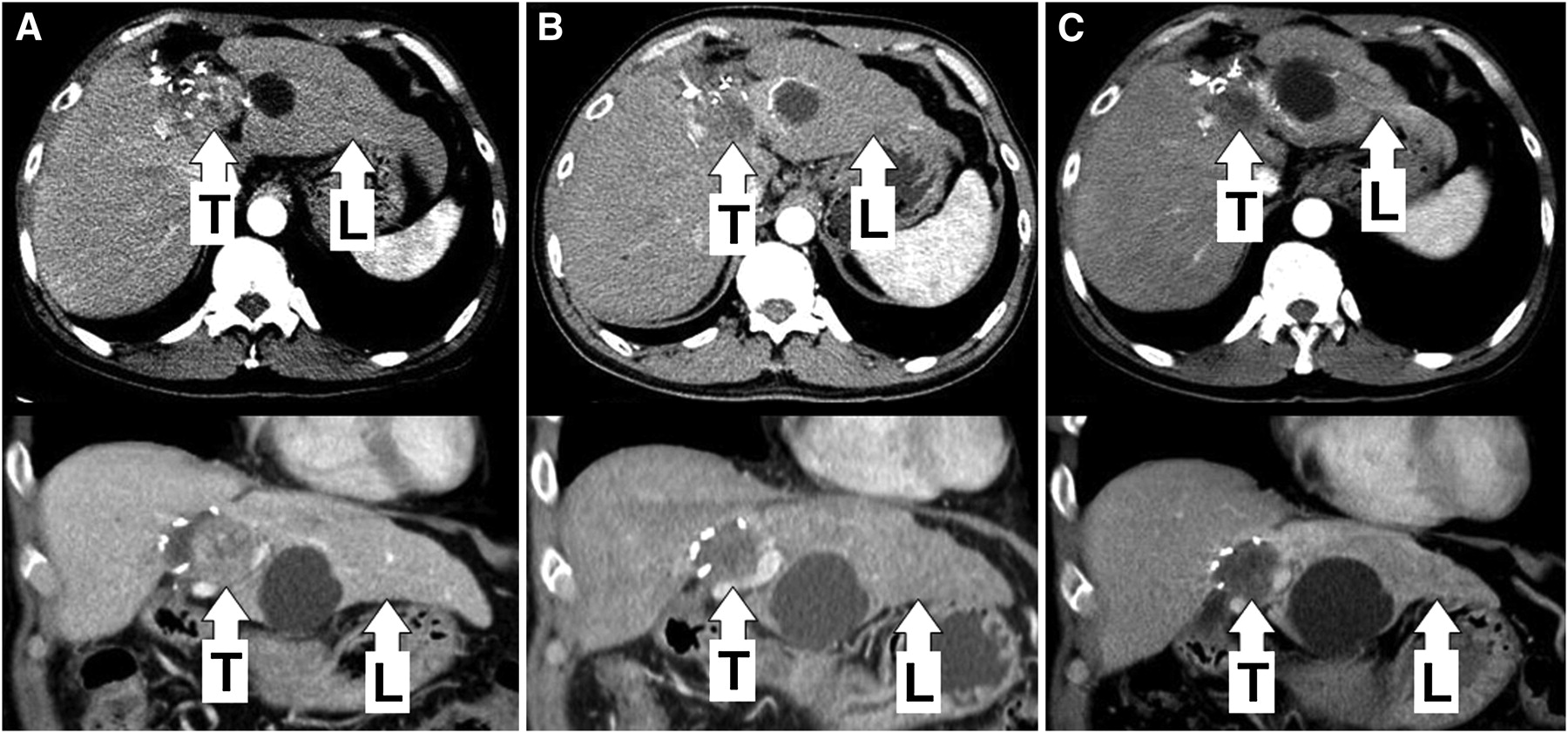
(A) Baseline triphasic CT scan of patient 2 shows recurrent HCC at segment IV resection margin. (B and C) Follow-up triphasic scans at 3 (B) and 6 (C) months after radioembolization show good tumor response (133 Gy), with progressive atrophy of left lobe (93 Gy), in keeping with left radioembolization lobectomy intent. Right lobe volume (27 Gy) remained stable. L = left lobe; T = tumor.
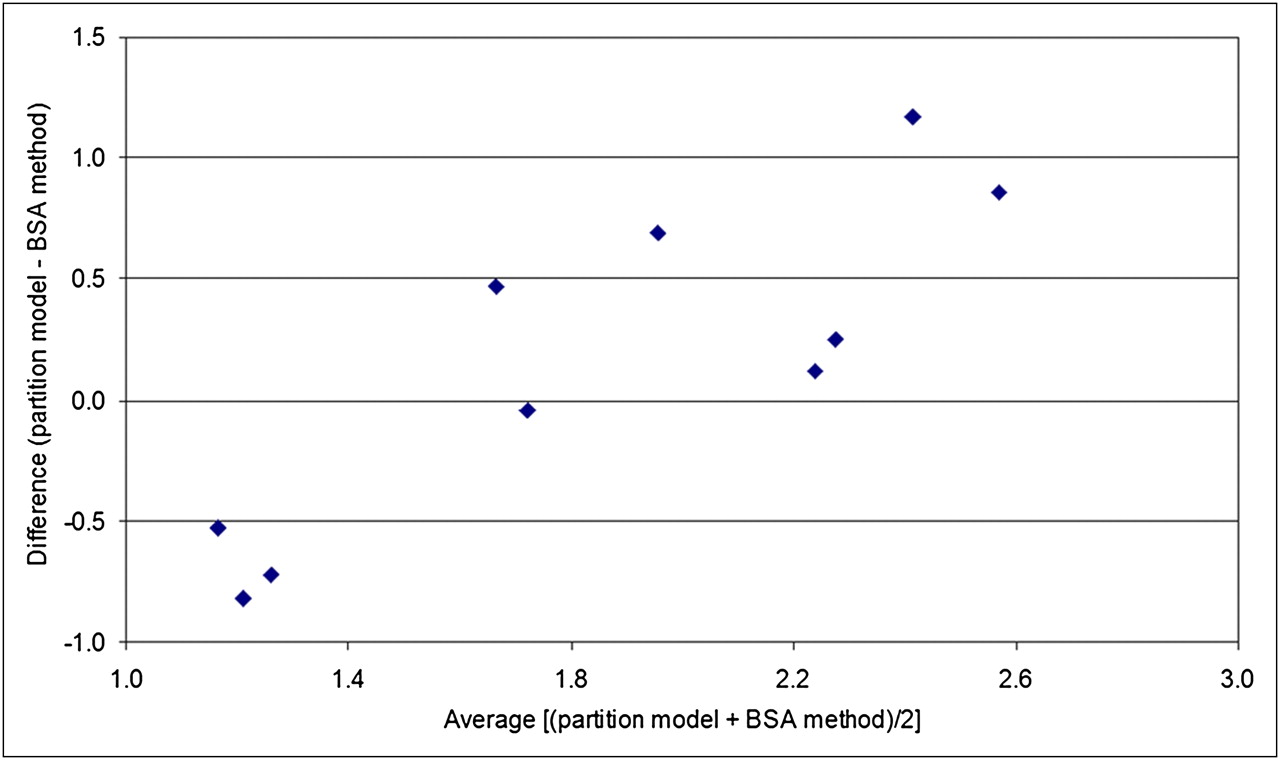
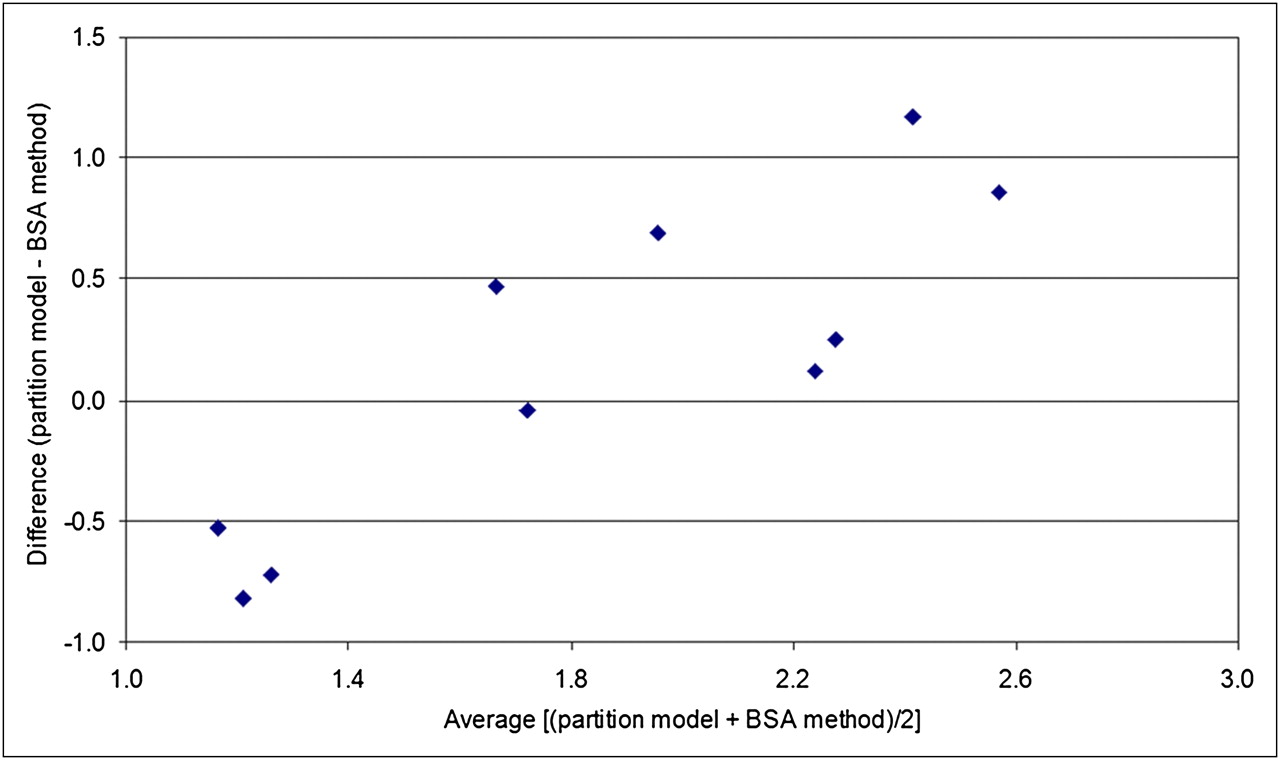
Bland–Altman plot of 90Y activities derived by artery-specific SPECT/CT partition modeling vs. that hypothetically derived by BSA methodology.
Median predicted mean radiation absorbed doses by artery-specific SPECT/CT partition modeling were 106 Gy (95% CI, 105–146 Gy) to tumor, 27 Gy (95% CI, 22–33 Gy) to nontumorous liver, and 2 Gy (95% CI, 1.3–7.3 Gy) to lungs. Across all patients, tumor, nontumorous liver, and lungs were predicted to have received ≥91 Gy, ≤51 Gy, and ≤16 Gy, respectively, to at least 1 target arterial territory. The median artery-specific tumor and nontumorous liver masses were 156 g (95% CI, 117–436 g) and 752 g (95% CI, 513–833 g), respectively. The median liver-to-lung shunt estimated by planar 99mTc-MAA scintigraphy was 5.4% (95% CI, 4.3%–9.0%). The median 90Y activity injected into an arterial territory was 0.6 GBq (95% CI, 0.7–1.3 GBq). Patient 2 received a mean radiation absorbed dose of 93 Gy to the left lobe nontumorous liver for 90Y radioembolization lobectomy (Supplemental Table 10; Fig. 2). There was good tumor response together with slow, progressive atrophy of the left lobe 6 mo after radioembolization, in keeping with the dosimetric intent. The right lobe volume, which received a mean radiation absorbed dose of 27 Gy to nontumorous liver, remained stable over time (Fig. 3).
SPECT/CT-based mean T/N ratios varied widely across all planning target volumes (median 5.4; 95% CI, 4.1–6.7) and even within the same patient (median intrapatient difference, 1.9; 95% CI, 1.1–2.5). We could not find any predictive relationship between mean T/N ratios and liver tissue masses. In a subanalysis, the total desired 90Y activities calculated by artery-specific SPECT/CT partition modeling were compared with those hypothetically derived by BSA methodology. Bland–Altman analysis (Fig. 4) showed a wide 95% limit of agreement ranging from −1.12 to +1.41, with only moderate correlation (intraclass correlation coefficient, 0.59; 95% CI, −0.71 to 0.90).
90Y radioembolization was well tolerated by all patients. None developed postradioembolization syndrome. All patients were ambulating freely by the next day and were discharged within 24 h after radioembolization. In 8 patients, serum bilirubin, albumin, and alanine transaminase were measured within 24 h after radioembolization; none developed significant biochemical toxicities. The results are summarized in Supplemental Table 3.
At the time of this report, follow-up data were available for 8 patients. The median follow-up duration was 21 wk (95% CI, 12–50 wk). The other 2 patients were nonresidents, returned to their home country, and were lost to follow-up. Patient 3 was excluded from biochemical and survival analysis because of confounding medical issues (supplemental data) but was included in imaging analysis.
With the exception of patient 3, all 7 of the other patients remained clinically well. None developed gastrointestinal complications or radiation pneumonitis. For 3 mo after radioembolization, there were no biochemical toxicities beyond grade 2 of the Common Terminology Criteria for Adverse Events (Supplemental Table 4). Postradioembolization serum α-fetoprotein was available in 5 patients. There was an interval decrease in α-fetoprotein in 3 patients, ranging from 32% to 95% (Supplemental Table 5). The remaining 2 patients had normal baseline α-fetoprotein levels, which remained unelevated on follow-up.
The postradioembolization best imaging response was available for 8 patients (Supplemental Table 6). The median time to the best imaging response was 76 d (11 wk; 95% CI, 55–114 d). When 90Y radioembolization was analyzed strictly as a brachytherapy, all 8 of 8 patients showed regression of the index tumor, with a median size decrease of 58% (95% CI, 40%–72%). None developed new tumors within planning target volumes. Seven of 8 patients achieved clinical success at the time of best imaging response. Patient 1, who had infiltrative HCC, was classified as a clinical failure because of progression of existing portal vein tumor thrombosis despite significant regression of the index tumor (Supplemental Fig. 5). Otherwise, tumor thrombosis regressed or remained stable in 3 of 4 patients with baseline tumor vascular involvement.
At the time of best imaging response, extrahepatic metastases were discovered in 3 of 8 patients, involving the lungs and adrenal gland. When 90Y radioembolization was analyzed as part of a comprehensive multimodality treatment plan, partial response was achieved in 3 of 8, stable disease in 1 of 8, and progressive disease in 4 of 8 patients (Supplemental Table 6)—consistent across all 3 classifications (Response Evaluation Criteria in Solid Tumors, World Health Organization criteria, and 2-dimensional criteria of the European Association for the Study of the Liver). Median imaging time to progression and median overall survival were not reached at the time of this report (Supplemental Table 7). Patient 1 died 13 wk after radioembolization and had an overall survival of 95 wk (22 mo) under comprehensive multimodality care; all 7 of the other patients are still alive.
DISCUSSION
The aim of personalized predictive dosimetry is to guide decisions on radionuclide therapy in order to avoid the use of futile therapy and achieve the maximum tumor radiation absorbed dose while minimizing collateral radiation injury to normal tissue.
Precise predictive dosimetry has the potential to yield many benefits for cancer therapy, and the need for further research into internal dosimetry has recently been emphasized (31). To our knowledge, the artery-specific SPECT/CT partition model is the first to integrate catheter-directed CTHA, 99mTc-MAA SPECT/CT, and partition modeling (MIRD) into a unified, accurate, and practical form of image-guided personalized predictive dosimetry for 90Y radioembolization.
Our results show that a 100% tumor response rate could be achieved when the predicted mean tumor radiation absorbed dose was at least 91 Gy to a planning target volume. There were no significant toxicities, with predicted mean radiation absorbed doses to nontumorous liver and lungs of ≤51 Gy and ≤16 Gy, respectively. This finding highlights the power of predictive radionuclide dosimetry to achieve desired outcomes when planned in accordance with dose–response relationships. The capability of artery-specific SPECT/CT partition modeling is best exemplified by patient 2, in whom sublesional dosimetry was successfully planned with 90Y radioembolization lobectomy intent (Figs. 2 and 3).
90Y radioembolization is a point-source, continuous low–dose-rate brachytherapy delivered at a single time point. Hence, its true therapeutic efficacy can be revealed only by analyzing outcomes in the context of planning target volumes and technical success. Therefore, the postradioembolization appearance of new tumors within a planning target volume should not be misconstrued as a clinical failure. Such lesions may represent new metastases, preexisting micrometastases that have enlarged, or de novo tumors arising from cirrhotic liver, all of which have little or no bearing on 90Y radioembolization as brachytherapy delivered at a single time point. It follows that when applying standard response evaluation criteria (e.g., Response Evaluation Criteria in Solid Tumors), which take into account new tumors and distant metastases, one should analyze 90Y radioembolization brachytherapy as part of comprehensive multimodality care and not in isolation.
The application of 90Y radioembolization without due regard for radiobiologic principles is akin to flying an aircraft without guidance from air traffic control. Since most patients with inoperable HCC have a limited prognosis, 90Y radioembolization should be carefully planned using scientifically sound methods (e.g., MIRD) to achieve the maximum desired effect for optimal, personalized cancer therapy. Our dosimetric data showed wide inter- and intrapatient variations in SPECT/CT-based mean T/N ratios (Supplemental Table 10), emphasizing the importance of having a personalized dosimetric approach to 90Y radioembolization. The assumption of a standard T/N ratio for the sake of dosimetric simplification may result in over- or undertreatment and confounds data analyses because reliable dose–response relationships cannot be established or verified (10). Despite its popularity, the BSA method has a questionable radiobiologic basis and is scientifically inferior to MIRD methodology (5,10). One must be cognizant that the BSA method was first published by van Hazel et al. for whole-liver 90Y radioembolization to previously untreated colorectal liver metastasis, not HCC (32). These patients did not have chronic liver disease, prior liver resection, local ablation, or selective or superselective 90Y radioembolization. Furthermore, colorectal liver metastases are rarely bulky enough to distort liver anatomy. These features are often present in HCC, and therefore they cast doubt on the validity, safety, and efficacy of the use of BSA methodology for HCC. The fact that our data show a lack of agreement in total 90Y activities derived by artery-specific SPECT/CT partition modeling versus the BSA method is further evidence against the routine use of BSA methodology (Fig. 4).
In this report, postradioembolization bremsstrahlung SPECT/CT was used to determine technical success. Success was indeterminate in 7 of 10 patients, all of whom had either subcentimeter tumors or tumors with ill-defined margins. This finding highlights the low spatial resolution of bremsstrahlung SPECT/CT as a technical limitation by indirectly imaging 90Y biodistribution using scatter radiation. It may be possible for PET to overcome this limitation by coincidence imaging of 90Y internal pair production (33). This possibility is currently under investigation at our institution.
90Y microspheres, once implanted, remain permanently in place and decay to infinity in situ. This simplifies the dosimetric process because time–activity curves need not be obtained, unlike in systemic radionuclide therapy. Future 90Y radioembolization dosimetric techniques must improve accuracy in several areas: delineation of arterial territory target volumes, microparticle simulation and biodistribution assessment, and predictive radiation dose–response modeling. For example, future development of positron-labeled microspheres in place of 99mTc-MAA may increase the accuracy of liver-to-lung shunt calculation and of simulation of hepatic microsphere biodistribution and improve predictive radiation modeling by voxel- or Monte-Carlo–based techniques (34,35). 90Y radioembolization will also benefit from a wealth of experience if radiobiologic models based on external-beam radiation therapy (e.g., linear quadratic model and normal tissue complication probability model) and radiation-planning techniques (e.g., dose–volume histogram) can be meaningfully translated into radionuclide dosimetry models (e.g., MIRD) and vice versa. Application of the concept of biologically effective dose (BED) into 90Y radioembolization dosimetry may achieve this aim (36).
CONCLUSION
Compliance with radiobiologic principles of radionuclide internal dosimetry is fundamental to 90Y radioembolization success. Image-guided personalized predictive dosimetry by artery-specific SPECT/CT partition modeling achieves high clinical success rates for safe and effective 90Y radioembolization.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Stephanie M.C. Fook, biostatistician, Division of Clinical Research, Singapore General Hospital, for assisting with the statistical analysis. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 17, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication August 25, 2011.
- Accepted for publication November 8, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Indirect Lung Absorbed Dose Verification by 90Y PET/CT and Complete Lung Protection by Hepatic Vein Balloon Occlusion: Proof of Concept
- The Impact of Radiobiologically Informed Dose Prescription on the Clinical Benefit of 90Y SIRT in Colorectal Cancer Patients
- Resin Versus Glass Microspheres for 90Y Transarterial Radioembolization: Comparing Survival in Unresectable Hepatocellular Carcinoma Using Pretreatment Partition Model Dosimetry
- Partition Model-Based 99mTc-MAA SPECT/CT Predictive Dosimetry Compared with 90Y TOF PET/CT Posttreatment Dosimetry in Radioembolization of Hepatocellular Carcinoma: A Quantitative Agreement Comparison
- Insights into the Dose-Response Relationship of Radioembolization with Resin 90Y-Microspheres: A Prospective Cohort Study in Patients with Colorectal Cancer Liver Metastases
- 90Y Hepatic Radioembolization: An Update on Current Practice and Recent Developments
- Systematic Evaluation of Tumoral 99mTc-MAA Uptake Using SPECT and SPECT/CT in 502 Patients Before 90Y Radioembolization
- A Gelatin Liver Phantom of Suspended 90Y Resin Microspheres to Simulate the Physiologic Microsphere Biodistribution of a Postradioembolization Liver
- 99mTc-MAA-Based Dosimetry for Liver Cancer Treated Using 90Y-Loaded Microspheres: Known Proof of Effectiveness
- Pretreatment Dosimetry in HCC Radioembolization with 90Y Glass Microspheres Cannot Be Invalidated with a Bare Visual Evaluation of 99mTc-MAA Uptake of Colorectal Metastases Treated with Resin Microspheres
- Three-Dimensional Personalized Monte Carlo Dosimetry in 90Y Resin Microspheres Therapy of Hepatic Metastases: Nontumoral Liver and Lungs Radiation Protection Considerations and Treatment Planning Optimization
- A Clinical Dosimetric Perspective Uncovers New Evidence and Offers New Insight in Favor of 99mTc-Macroaggregated Albumin for Predictive Dosimetry in 90Y Resin Microsphere Radioembolization
- Prognostic Utility of 90Y Radioembolization Dosimetry Based on Fusion 99mTc-Macroaggregated Albumin-99mTc-Sulfur Colloid SPECT
- Reply: Results Confounded by a Disregard for Basic Dose-Response Radiobiology
- Results Confounded by a Disregard for Basic Dose-Response Radiobiology
- Value of 99mTc-Macroaggregated Albumin SPECT for Radioembolization Treatment Planning
- 99mTc-Macroaggregated Albumin Poorly Predicts the Intrahepatic Distribution of 90Y Resin Microspheres in Hepatic Radioembolization
- Radiodosimetric Estimates for Radioembolic Therapy of Liver Tumors: Challenges and Opportunities