


Abstract
We evaluated potential associations between maximum standardized uptake value (SUVmax) on 18F-FDG PET before and after radiation therapy (RT) and survival outcomes for patients with locally advanced non–small cell lung cancer. Methods: Patients with stage III non–small cell lung cancer (n = 49) who had undergone 18F-FDG PET at the M.D. Anderson Cancer Center both before and up to 3.5 mo after undergoing radiochemotherapy were studied; exclusion criteria were patients with a history of thoracic surgery, RT, or other cancer or those who had received a total radiation dose less than 60 Gy. We assessed associations between overall survival (OS) or disease-free survival (DFS) and post-RT SUVmax and the extent of decrease in SUVmax in the primary tumor (PT) and regional lymph nodes (LNs). SUVmax was assessed as a continuous variable by Cox proportional hazards regression analysis. Results: Univariate and multivariate analyses showed that having a high post-RT SUVmax (either PT or LNs) was associated with a higher risk of death (univariate analyses: hazard ratio [HR] for PT SUVmax, 1.27, P < 0.0001; HR for LN SUVmax, 1.32, P = 0.004) and disease recurrence (univariate analyses: HR for PT SUVmax, 1.16, P = 0.004; HR for LN SUVmax, 1.32, P = 0.001). Moreover, after definitive RT, the greater the decrease in SUVmax in the lesion that had the highest SUVmax at diagnosis, the longer the OS (HR, 0.06; P = 0.002), DFS (HR, 0.03; P = 0.001), local–regional control (HR, 0.04; P = 0.002), and distant metastasis-free survival (HR, 0.07; P = 0.028). Conclusion: The post-RT SUVmax in both the PT and the LNs was a predictor of survival—specifically, the higher the residual SUVmax after RT, the poorer the OS and DFS; and the greater the decrease in SUVmax in the lesion with the highest SUVmax at diagnosis, the longer the OS and DFS. This information should help to identify patients who are at high risk of recurrence and for whom additional treatments can be designed accordingly.
- non–small cell lung cancer
- radiation therapy
- standardized uptake value
- chemoradiation therapy
- positron emission tomography
The current standard of care for patients with unresectable clinical stage III non–small cell lung carcinoma (NSCLC) is combined chemoradiation therapy. The median survival time after such treatment is approximately 17 mo (1)—a significant improvement over historical treatment with radiation therapy (RT) or surgery alone but still quite poor. New treatment strategies for this disease are thus still urgently needed.
PET has had an increasing role in the initial staging and posttreatment evaluation of various types of cancer, including breast cancer, lymphoma, head and neck cancer, and NSCLC (2–8). The uptake of the glucose analog 18F-FDG by NSCLC tumor cells has been found to be useful for restaging at recurrence and for delineating radiotherapeutic targets (9–11). The standardized uptake value (SUV) in 18F-FDG PET before initial curative treatment has also been shown by some (12,13), but not all (14), to be a prognostic factor for survival outcomes. Therefore, the potential value of 18F-FDG PET for predicting prognosis in advanced NSCLC before and after treatment still needs to be established.
A decline in 18F-FDG uptake in the primary tumor or lymph nodes (LNs) after chemotherapy, RT, or both treatments for NSCLC is thought to reflect a reduction in the metabolic activity of the tumor and thus can be used to assess tumor response to therapy. The evaluation of the metabolic change after RT would be of considerable benefit given the difficulty of assessing whether the therapy worked with other imaging techniques (15). However, whether reductions in SUV in the primary tumor or LNs from before to after RT are linked with survival in patients with NSCLC remains uncertain. Also unclear is whether reductions in SUV could be associated with the likelihood of either local relapse or distant metastasis in such patients.
Hence, we undertook this study to assess potential associations between survival outcomes and the maximum SUV (SUVmax) measured by 18F-FDG PET before and after therapy as well as the percentage of change in SUVmax in the primary tumor, regional LN with the highest SUVmax, SUVmax sum of all regional LNs, target lesion (either primary tumor or LN) with the highest SUVmax, and SUVmax sum of the primary tumor and all regional LNs in patients with inoperable stage III NSCLC who were candidates for curative therapy.
MATERIALS AND METHODS
Patients
This retrospective analysis was approved by the institutional review board of The University of Texas M.D. Anderson Cancer Center. Subjects were identified by a database search of patients with lung cancer treated with definitive radiochemotherapy in the Department of Radiation Oncology at M.D. Anderson Cancer Center between January 2007 and December 2008. Patients who were included in this study were those who had undergone an 18F-FDG PET study done at M.D. Anderson both before and up to 3.5 mo after completing RT, who had no history of thoracic surgery or radiation therapy, who had no prior other cancer, and who had received a total radiation dose of 60 Gy or more. Ultimately, 49 patients met the selection criteria for this study. Disease had been staged according to the 2002 edition of the American Joint Committee on Cancer staging system (16). CT or 18F-FDG PET scans were obtained every 3 mo for the first 2 y after treatment, then every 6 mo for 5 y, and then annually thereafter to check for evidence of recurrence.
18F-FDG PET Technique
Baseline (pretreatment) 18F-FDG PET scans were obtained a median of 26 d before the start of RT. For patients who had received induction chemotherapy, we used the SUVmax and clinical disease stages that had been assigned at initial diagnosis for our analysis. The median lag time between the end of the RT and the time of the 18F-FDG PET evaluation was 2.5 mo (range, 1–3.5 mo). For patients who had received adjuvant chemotherapy, the posttreatment scan was obtained after the chemotherapy. Scans were begun after a 6-h fast, with an intravenous injection of 370–555 MBq of 18F-FDG, and emission and transmission scans were obtained 60 min afterward. All patients were required to have had a blood sugar level of 150 mg/dL or less before 18F-FDG injection. Scans were obtained with a Discovery ST PET/CT scanner (GE Healthcare).
SUV Measurements
One experienced radiologist reviewed all 18F-FDG PET images and obtained the SUVmax for all patients. The SUVmax in the gross primary tumor and in each LN was calculated and recorded from scans obtained before and after RT. Changes in SUV (ΔSUV) after treatment were calculated with the following equation: ΔSUV = ([SUVpre − SUVpost]/SUVpre) × 100, where SUVpre and SUVpost denote pre- and posttreatment SUV, respectively. The primary tumor and LNs were manually drawn on the transaxial images around the focal 18F-FDG uptake zone by referring to CT images before and after RT. For those cases considered to represent complete metabolic response (i.e., areas with 18F-FDG uptake ≤ that in the aortic arch) or complete radiologic response (i.e., LN having a short axis of <10 mm), the SUVmax of the anatomic area corresponding to the pretreatment lesion was taken (Fig. 1). The SUVs of the primary tumor and LNs were calculated as SUV = activity concentration (kBq [μCi]/mL)/(injected dose [MBq (mCi)]/body weight [kg]). We used the maximum SUVmax to avoid partial-volume effects (17). The SUVmax is defined as the SUV of a 1-pixel region of interest corresponding to the maximum value in the primary tumor or LN; thus, SUVmax represents the value least affected by the partial-volume effect.

PET/CT scans of 18F-FDG uptake by primary tumor and lymph nodes at diagnosis (A) and after radiation therapy (B). SUVaorta = SUV in aorta.
Statistical Analysis
Data were analyzed using Stata/SE 11.1 software (Stata Corp LP). Our goal was to investigate associations between the SUVmax in the primary tumor or LNs and survival outcomes. For that purpose, we analyzed the SUVmax before and after RT and the percentage of the change after RT in the following categories: the primary tumor, regional LN with the highest SUVmax, SUVmax sum of all regional LNs, target lesion with the highest SUVmax, and SUVmax sum of primary tumor and all the regional LNs. Target lesions were defined as the primary tumor and any involved LNs. The Kaplan–Meier method was used to estimate the probability of overall survival (OS) and disease-free survival (DFS). Potential associations between the SUVmax and survival outcomes were assessed in univariate analyses using the Cox proportional hazards model, and SUVmax was evaluated as a continuous variable. Because of the possible confounding effect of clinical factors on survival, associations found to be significant in the univariate analysis were adjusted by patient factors (age, sex, race, Karnofsky performance status, weight loss, and smoking habits), tumor factors (histology, stage), and treatment factors (type of chemotherapy, RT technique, and dose). Multivariate analyses were performed using a logistic regression model, with a stepwise backward elimination procedure. A P value of 0.05 or less was considered statistically significant. Survival time was measured from the end of RT to the first occurrence of the considered event (death, local–regional recurrence [inside the radiation field, or both inside and outside the radiation field], or distant metastasis).
RESULTS
Patients, Treatments, and Follow-up
Patient characteristics are listed in Table 1. The median follow-up time for all patients was 25.5 mo (range, 3.9–49.4 mo). All patients had good performance status (Karnofsky performance score ≥ 70) and underwent RT 5 d a week to a total dose of 63–74 Gy (median, 66 Gy) over 6–7 wk at 1.8–2.0 Gy per day. Forty-eight patients received platinum and taxane-based chemotherapy, 47 concurrent with RT and 1 sequentially. Of the 22 local–regional relapses, 16 occurred inside the radiation field; of the 18 distant metastases, 5 were in the brain.
Patient Characteristics
Survival Analyses
SUVmax for Primary Tumor
In 8 patients, distinguishing the 18F-FDG accumulation of the primary tumor from that of the LNs was difficult because the primary tumor extended to the hilar or subcarinal station. In those cases, the 18F-FDG accumulation was regarded as the SUV for the primary tumor. We observed that the higher the SUVmax was after RT (Table 2), the shorter was the OS time (P < 0.0001; Fig. 2) and DFS time (P = 0.004; Fig. 3). Figures 4 and 5 illustrate the effect of SUVmax on OS and DFS, respectively, with the cut-off point of the SUVmax after RT set at 3.7 (the 50th percentile for primary tumors); patients with an SUVmax less than 3.7 had better OS and DFS than did those with an SUVmax of 3.7 or greater (OS, P = 0.0008; DFS, P = 0.0112). We then investigated whether the interval between the end of RT and the PET scan had any influence on tumor response. For that purpose, we compared the SUVmax after RT in those patients who underwent PET 2.5 mo or less after RT (the median time between RT end date and PET scan date) and those who had the evaluation more than 2.5 mo after RT. We found no significant difference in the SUVmax after RT between both subgroups (P = 0.201). However, we did find that for the subgroup with the PET scan more than 2.5 mo after RT, the SUVmax after RT was associated with OS time (P = 0.021). To clarify the patterns of relapse, we evaluated local–regional control (LRC) and distant metastasis-free survival (DMFS) rates in terms of SUVmax and found that the higher the SUVmax was after RT, the higher was the risk of local–regional recurrence inside (P = 0.002) and both inside and outside (P = 0.002) the radiation field. However, no significant associations with DMFS were found. All results that were statistically significant in the univariate analysis retained significance in the multivariate analysis (Table 3). Finally, for the primary tumor, the SUVmax at diagnosis was not associated with any of the outcomes that were assessed.
Univariate Analyses of SUVs and Survival
Multivariate Analyses of SUVs and Survival

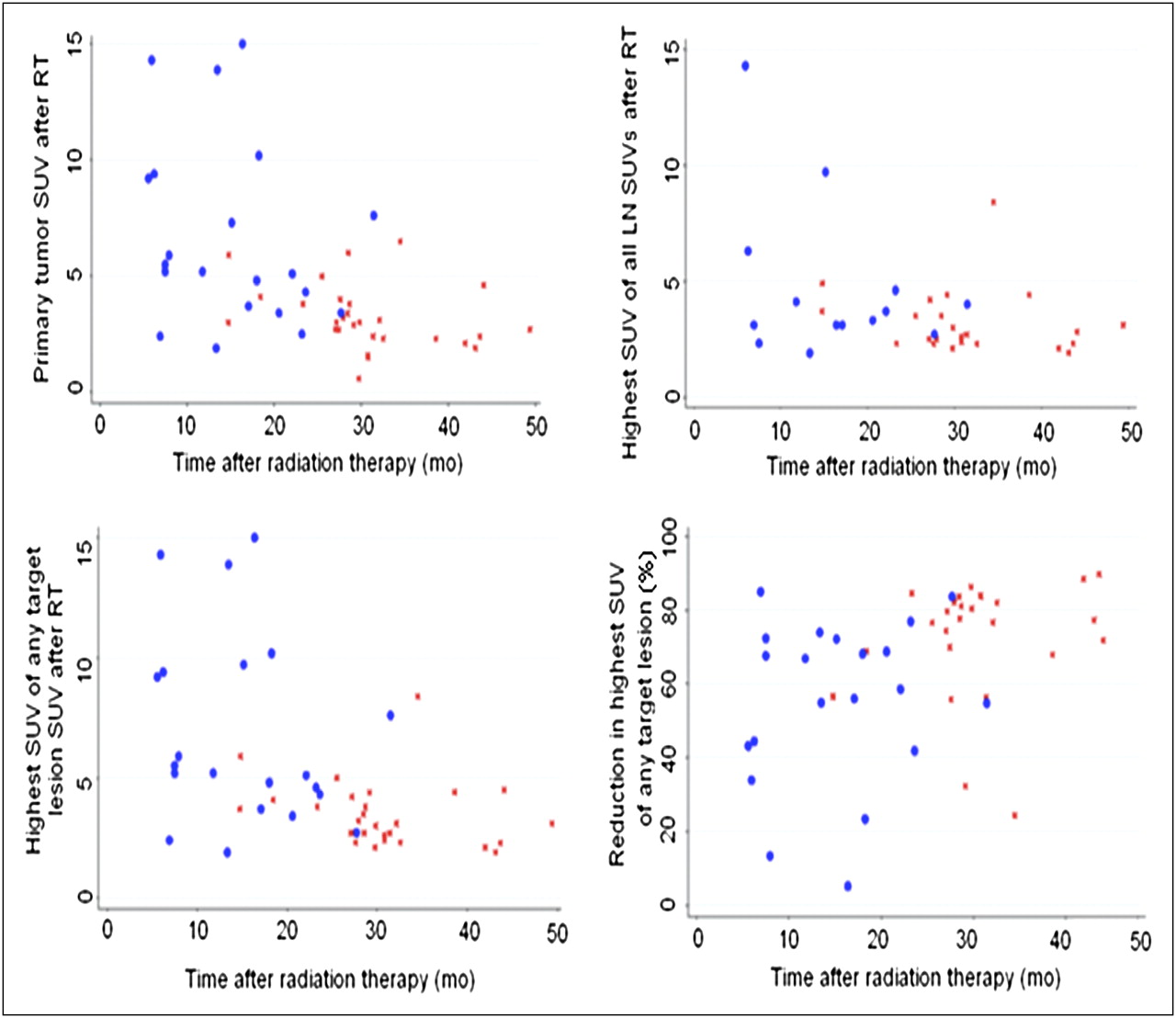
Scatterplot of OS time (x-axis) vs. SUVmax after radiotherapy for patients alive (red symbols) and or dead (blue symbols).

Scatterplot of DFS time (x-axis) vs. SUVmax after radiotherapy for patients with (red symbols) and without (blue symbols) recurrent disease.

OS according to 50th percentile of SUVmax after radiotherapy. *Total number of patients differs from other figures because 4 patients were stage N0 disease, and in 8 N-positive stage cases, it was difficult to distinguish each primary tumor accumulation of 18F-FDG from its LN accumulation. Thus, 18F-FDG accumulation was regarded as SUVmax for primary tumor.

DFS according to 50th percentile of SUVmax after radiotherapy. *Total number of patients differs from other figures because 4 patients were stage N0 disease, and in 8 N-positive stage cases, it was difficult to distinguish each primary tumor accumulation of 18F-FDG from its LN accumulation. Thus, 18F-FDG accumulation was regarded as SUVmax for primary tumor.
SUVmax for Regional LNs
Because some patients had more than one positive LN, we considered the single regional LN with the highest SUVmax and the SUVmax sum of all PET-positive LNs separately for these analyses. No significant difference was found in the extent of SUVmax reduction between the primary tumor (median, 70%) and the regional LN with the highest SUVmax after RT (median, 64%; P = 0.384). We found that, after RT, the higher the uptake was in the single LN with the highest post-RT SUVmax, the shorter were the OS time (P = 0.004; Fig. 2), the LRC inside the radiation field (P = 0.001), the LRC both inside and outside the radiation field (P = 0.002), and the DFS time (P = 0.001; Fig. 4). Figures 4 and 5 illustrate the effect of SUVmax on OS and DFS, respectively, with the cut-off point of the SUVmax after RT set at 3.1 (the 50th percentile for LNs); patients with an SUVmax of less than 3.1 also had better OS and DFS than did those with an SUVmax of 3.1 or more (OS, P = 0.0143; DFS, P = 0.0028). For the summed SUVmax of all PET-positive LNs, only the uptake after RT was significantly associated with LRC inside and outside the radiation field (P = 0.007). The results also indicated that the higher the summed SUVmax was after RT, the shorter was the LRC. These associations all retained significance in multivariate analysis (Table 3). Again, the SUVmax at diagnosis did not correlate with any of the measured outcomes.
SUVmax for Target Lesion (Either Primary Tumor or Regional LNs)
The target lesion with the highest SUVmax at diagnosis was the primary tumor in 67% of cases and the LNs in 33%. Similar results were observed after RT, when the highest SUVmax was the primary tumor in 63% of cases and the LNs in 37% of cases. The higher the post-RT SUVmax of the single target lesion with the highest post-RT SUVmax was, the shorter were the OS (P < 0.0001), DFS (P = 0.003), LRC inside the radiation field (P = 0.004), LRC both inside and outside the radiation field (P = 0.004), and DMFS (P = 0.044; Table 2). Findings were similar for the extent of SUVmax reduction after RT; specifically, the greater the SUVmax reduction was after RT in the single target lesion with the highest SUVmax at diagnosis, the longer were the OS (P = 0.002; Fig. 2), DFS (P = 0.001; Fig. 3), LRC inside the radiation field (P = 0.007), LRC both inside and outside the radiation field (P = 0.002), and DMFS (P = 0.028; Table 2). Figures 4 and 5 illustrate the effect of the post-RT SUVmax of the single target lesion with the highest post-RT SUVmax and the extent of SUVmax reduction after RT on OS and DFS when dichotomized according to the 50th percentile of the corresponding variable. Patients with a post-RT SUVmax of less than 3.8 or an SUVmax reduction of 72% or more had better OS and DFS than did those with a post-RT SUVmax of 3.1 or more (OS, P = 0.0006; DFS, P = 0.0045) or an SUVmax reduction of less than 72% (OS, P = 0.0074; DFS, P = 0.0603). However, the pretreatment SUVmax was not associated with any survival outcome. When analyzing the summed SUVmax of the primary tumor plus all PET-positive LNs, we observed that the higher the values were after RT, the shorter were the LRC both inside and outside the radiation field (P = 0.001) and the DFS (P = 0.001). Finally, we found that the greater the reduction was in the summed SUVmax of the primary tumor plus all PET-positive LNs, the longer were the OS (P = 0.004), LRC inside and outside the field (P = 0.021), and DFS (P = 0.033; Table 2). All of these results, except for the association between the reduction in the summed SUVmax of the primary tumor plus all PET-positive LNs and OS, retained significance in multivariate analyses (Table 3).
DISCUSSION
PET/CT images provide functional information about cancer by assessing the uptake of a radioactive glucose analog by a tumor—a process that most likely reflects the biologic behavior of a particular case of cancer in terms of proliferation, metastatic potential, sensitivity to therapy, and more (18,19). The key findings of the current study were that the regional LN with the highest SUVmax after RT was significantly associated with OS: the lower the post-RT SUVmax was, the longer the OS was. Our results also showed that the extent of reduction in SUVmax was associated with disease control after curative RT for locally advanced NSCLC: the greater the decrease in SUVmax was in the lesion (primary tumor or LN) that had the highest SUVmax at diagnosis, the longer was the OS. We further found that the lower the post-RT SUVmax was in the primary tumor or the regional LN with the highest SUVmax after RT, the longer were the DFS and LRC times. Finally, the greater the decline in SUVmax was after RT of the lesion with the highest SUVmax at diagnosis, the longer was the DMFS time.
It is well established that patients with inoperable NSCLC showing residual metabolic activity within the primary tumor after radiochemotherapy have worse OS than patients without such residual activity (18). Our results are consistent with data published by others. Several investigators have explored the usefulness of pretreatment 18F-FDG PET for predicting outcome for patients with NSCLC, and several cut-off SUV levels have been proposed (13,19,20). However, other recent studies (14,21) have shown that pretreatment 18F-FDG uptake of the primary tumor in patients with newly diagnosed advanced-stage NSCLC was not related to survival. For instance, Ikushima et al. (21) evaluated the relationship between the SUVmax and clinical tumor features in 149 patients with NSCLC who underwent pretreatment PET (n = 67) or PET/CT (n = 82) and definitive RT. A high SUVmax was a negative factor for LRC, DMFS, and OS on univariate analysis in the PET group, but the significance decreased when tumor size was included in the analysis. In addition, a high SUVmax was not a negative factor for LRC, DMFS, or OS in the PET/CT group, suggesting that the evidence was not sufficient to conclude that pretreatment 18F-FDG uptake in a primary NSCLC tumor provides prognostic information. Consistent with these findings, we did not observe a significant relationship between SUVmax before RT and survival.
Therefore, the post-RT SUVmax or the extent of reduction in 18F-FDG PET SUVmax after treatment may be a better method of predicting survival than the pretreatment values. This supposition is supported by several recent reports (22,23). For instance, Aerts et al. (22) found that patients with residual metabolically active areas within the primary tumor after RT had significantly worse survival than did individuals whose tumors showed a complete metabolic response. In our study, we found that higher post-RT SUVmax not only in the primary tumor but also in the regional LN with the highest residual SUVmax after RT were strong negative prognostic factors for survival. This finding in the regional LN was a novel discovery. In addition, the association found between the post-RT SUVmax and OS noted for patients who had PET scans more than 2.5 mo after the end of RT (but not for those who had earlier PET scans) suggests that scans done sooner than 2.5 mo after RT may not reflect much of the effect of the RT.
The utility of the SUV for disease staging or its role after neoadjuvant chemotherapy for NSCLC has been described before (3,24–27). However, the usefulness of the extent of reduction in SUV after definitive RT, particularly in LNs, for assessing prognosis remains uncertain. In our analysis, neither the reduction in SUVmax in the primary tumor nor the reduction in the LNs was associated with any survival outcome assessed. However, when evaluating the percentage of SUVmax reduction after RT in the target lesion (either primary tumor or LN) with the highest SUVmax at diagnosis, we found a significant association with OS. This result highlights the role of the most 18F-FDG–avid lesion, regardless of whether that lesion is the primary tumor or the LNs, in predicting outcome after treatment of locally advanced NSCLC.
Greene et al. (16) proposed that a complete response after high-dose RT or concurrent chemoradiotherapy is defined as the complete disappearance of all evidence of malignant disease or residual radiographic abnormalities at 3 and 6 mo after completion of RT that then remains stable for an additional 6 mo or more. A recent Dutch study (18) confirmed the validity of metabolic response assessment up to 6 mo after RT as a surrogate of survival. To predict survival and obtain this information to help identify patients who are at high risk of recurrence and to design additional salvage treatment early, we decided to evaluate the first PET scan done after RT, which usually took place 1–3 mo after treatment, and found that we could indeed obtain this information as early as 3 mo after RT. Whether patients with residual 18F-FDG uptake after RT should be offered additional treatment is still uncertain, and this question should be prospectively evaluated in protocols to evaluate further management strategies such as new targeted therapies or adjuvant chemotherapy for such patients. Currently, the American College of Radiology Imaging Network 6668/RTOG 0235 trial is prospectively evaluating whether the primary tumor 18F-FDG SUVmax shortly after definitive chemoradiation can predict long-term survival in inoperable stage II or III NSCLC. This multiinstitutional study will clarify whether our findings are also observed in a larger sample.
On the basis of our findings and others (13,18,23), we could speculate that tumor glucose metabolism is related to the metastatic potential of the tumor. Increased 18F-FDG uptake on PET images may correlate with conventional tissue markers of tumor aggressiveness, markers of hypoxia or angiogenesis, or molecular markers of proliferation, such as Ki-67 (28,29). The overexpression of various molecular markers of tumor biology in common solid tumors such as NSCLC may be associated with PET findings, clinical outcome, or both, which would provide a new avenue for targeted therapies (30).
CONCLUSION
We found that the post-RT SUVmax for the primary tumor and LNs, as well as the extent of reduction after RT in the target lesion that had the highest SUVmax at diagnosis, were associated with OS and DFS in patients with NSCLC. These findings indicate that the post-RT SUVmax and the extent of reduction may become a routinely used, quantifiable, and analytic indicator of disease activity and treatment efficacy.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Tinsu Pan, Lawrence Levy, and Christine Wogan for their contributions to this report. Financial support for this research was provided by M.D. Anderson Cancer Center. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication July 29, 2011.
- Accepted for publication September 26, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}