


Abstract
This study compared the utility of 3′-deoxy-3′-18F-fluorothymidine PET (18F-FLT PET) with that of 18F-FDG PET for assessment of the early locoregional clinical outcomes of chemoradiotherapy for head and neck squamous cell carcinomas. Methods: From May 2006 to September 2010, 28 patients with head and neck squamous cell carcinomas underwent 18F-FLT and 18F-FDG PET before radiation therapy (RT), 4 wk after the initiation of RT, and 5 wk after completion of RT. PET images were evaluated qualitatively for regions of focally increased metabolism and were analyzed in relation to residual accumulation and local disease control. Results: During RT, 18F-FLT uptake decreased more significantly than 18F-FDG uptake. 18F-FLT accumulations disappeared in 34 of 54 lesions (63%), and negative predictive value was 97%. 18F-FDG PET during RT also had a high negative predictive value (100%), but only 9 lesions (16%) showed complete absence of accumulation. The specificity and overall accuracy of 18F-FLT PET were significantly higher than those of 18F-FDG PET both during and after RT. In particular, high significance was attributable to the results of the evaluations of primary lesions. There were significant differences in 3-y local control between the residual-accumulation and no-accumulation groups on both posttreatment 18F-FLT PET (P < 0.0001) and posttreatment 18F-FDG PET (P = 0.0081). Conclusion: 18F-FLT PET during RT and early follow-up facilitates the selection of optimal further therapy and the prediction of outcomes.
Radiation therapy (RT) plays an important role in the management of locally advanced head and neck squamous cell carcinomas (HNSCCs). To preserve organ function, concurrent chemoradiotherapy is now widely applied as the definitive treatment for locoregionally advanced HNSCCs (1). If persistent or recurrent tumors can be detected accurately, salvage surgery may be offered.
The current method for assessing the response of a solid tumor to RT is assessment of tumor size change by anatomic imaging modalities (2). However, the size of a tumor after treatment is not directly related to the viability of tumor cells because morphologic changes can include scarring due to either therapy or inflammation. Thus, these imaging techniques have limitations for assessing therapeutic effects.
Several studies have suggested that 18F-FDG PET might be useful for assessment of therapeutic responses (3–6). However, 18F-FDG is also metabolized at sites of inflammation and in other reactive states, so that false-positive results may be obtained because of inflammatory changes remaining within the first few posttreatment months.
Recently, a thymidine analog, 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), was introduced as a stable cell proliferation imaging agent (7). This tracer is trapped within the cytosol after being monophosphorylated by thymidine kinase-1, a principal enzyme in the salvage pathway of DNA synthesis (8). 18F-FLT accumulation is dependent on the presence of thymidine kinase-1, which is closely associated with cellular proliferation (8). 18F-FLT has thus been found to be useful for noninvasive assessment of the proliferation rates of several types of cancer, including HNSCC (9–11). Moreover, 18F-FLT PET has been used for early response monitoring of chemotherapy and RT (12–14). Yue et al. (15) examined esophageal squamous cell cancer patients during RT and reported an almost complete absence of tumor proliferation after 30 Gy of irradiation and a complete absence after 40 Gy of irradiation. Recently, Troost et al. (16) studied oropharyngeal cancer patients before RT and then 2 and 4 wk after the initiation of RT. In primary lesions, the relative decrease in maximal standardized uptake value (SUV) was 55% when pretreatment and second scans were compared and there was a 34% difference between the second and third scans. As to lymph node metastases, similar patterns were observed. However, there are few studies comparing the accuracy of 18F-FLT PET and 18F-FDG PET in HNSCC at an early stage after RT.
In this study, patients with HNSCC underwent 3 consecutive 18F-FLT PET and 18F-FDG PET scans: once before, once during, and finally a few weeks after completion of RT. The aims of this study were to monitor early tumor responses based on visual inspection and to compare the accuracy of 18F-FLT PET and 18F-FDG PET in patients with HNSCC.
MATERIALS AND METHODS
Patients
From May 2006 to September 2010, 28 patients with newly diagnosed HNSCCs treated with concurrent chemoradiotherapy were studied. All tumors were staged according to the 2002 International Union Against Cancer TNM staging system (17). All 28 primary lesions were histopathologically confirmed. A total of 30 lesions of cervical lymph node involvement were radiologically assessed before RT. The study was approved by the local ethics committee, and written informed consent was obtained from all patients.
Treatment and Follow-up
RT was administered to primary and neck regions once a day using 4-MV photons with a pair of bilaterally opposed fields for the upper neck and an anterior port for the lower neck. Patients were irradiated with a total dose of 60–70 Gy in once-daily fractions of 2 Gy. After 40 Gy had been administered, the clinical target volume was reduced to encompass only the primary region and the involved neck nodes. Twenty-two patients received chemotherapy, which consisted of 1–2 courses of systemic chemotherapy. Five patients received chemotherapy with cisplatin (70 mg/m2) and 5-fluorouracil (1,000 mg/m2 continuous infusion for 5 d), and the other 17 patients underwent chemotherapy with nedaplatin (80 mg/m2) and S-1 (a novel oral anticancer drug consisting of a mixture of 1 M tegafur, 0.4 M 5-chloro-2,4-dehydroxypyrimidine, and 1 M potassium oxonate), administered orally twice a day for 14 d at the following doses on the basis of body surface area: <1.5 m2, 80 mg/d; ≥1.5 m2, 100 mg/d. Nedaplatin is a platinum derivative that was developed as a less nephrotoxic agent than cisplatin. Nedaplatin has been reported to be at least as effective as cisplatin for HNSCC (18,19). In S-1, tegafur is a prodrug of 5-fluorouracil, 5-chloro-2,4-dehydroxypyrimidine enhances the serum 5-fluorouracil concentrations, and potassium oxonate reduces adverse reactions in the digestive tract (20). Five patients with T2 laryngeal cancer and one with decreased renal function received weekly docetaxel (10 mg/m2) chemotherapy 4–6 times concomitantly with RT.
Patients were followed up every 1–2 mo for the first 2 y after RT and then every 3 mo. A physical examination including endoscopy was performed at each follow-up session. The assessments included repeated CT scans or MRI every 3–6 mo.
Responses to chemoradiotherapy were clinically evaluated on the basis of endoscopic, radiographic, and pathologic findings. When a residual or recurrent tumor was suspected in the primary region, biopsy was performed under local or general anesthesia.
Patients with positive CT or PET findings in lymph nodes were considered to have indications for the performance of neck dissection. Four patients were diagnosed as having persistent or recurrent disease in lymph nodes, and 5 lymph nodes were confirmed to have tumor involvement (3 patients had 1 metastatic lymph node, and 1 patient had 2 metastatic lymph nodes).
18F-FLT Synthesis
18F-FLT was synthesized using the method described by Machulla et al. (21) with a radiochemical purity of more than 95%.
PET Acquisition
Integrated PET and CT images were acquired using either dedicated PET and CT systems (19 patients) or a hybrid PET/CT system (9 patients). Patients were instructed to fast for at least 5 h before 18F-FLT and 18F-FDG PET examinations, although oral hydration with glucose-free water was allowed. For 18F-FDG PET, a normal peripheral blood glucose level was confirmed. Dedicated PET images were acquired using an ECAT EXACT HR+ scanner (Siemens/CTI). The imaging system allowed simultaneous acquisition of 63 transverse PET images per field of view, for a total axial field of view of 15.5 cm. PET scans were acquired 60 min after intravenous injection of 18F-FLT (3.5 MBq/kg) or 18F-FDG (3.5 MBq/kg), with 2 or 3 min per bed position in 3-dimensional mode. Transmission scans were obtained using a 68Ge rod source for the purpose of attenuation correction. PET images were reconstructed with ordered-subset expectation maximization using 2 iterations and 8 subsets. Starting in April of 2010, hybrid PET/CT acquisitions were performed with an integrated PET/CT system (Biograph mCT; Siemens Medical Solutions). Emission images were obtained 60 min after intravenous injection of 18F-FLT (3.5 MBq/kg) or 120 min after intravenous injection of 18F-FDG (3.5 MBq/kg) (2 min per bed position; scan length, 21.6 cm per bed position) from the neck to the pelvis (5–7 bed positions) and coregistered with an unenhanced CT scan of the same region (120 kV; quality reference mAs, 210 mAs [using CARE Dose4D; Siemens]; reconstructed slice thickness, 5 mm). The mean intervals between scans before RT, during RT and after RT, for both 18F-FLT PET and 18F-FDG PET, were 4, 2, and 2 d, respectively.
PET Image Analysis
PET images were reviewed on a Sun Microsystems workstation (Siemens/CTI) in transverse, coronal, and sagittal planes along with maximum-intensity-projection images. 18F-FLT and 18F-FDG PET images were read at random, with an interval of several days between interpretations. The observers were masked to all identifying information. Any differences in opinion were resolved by reaching a consensus. The PET images were evaluated qualitatively for regions of focally increased metabolism. Increased uptake to a level appreciably greater than that in the surrounding tissue was considered to indicate malignancy.
A finding was considered true-positive if a tumor was histopathologically proven at follow-up in an area with residual uptake. A finding was considered true-negative if no residual accumulation was shown and no tumor recurrence was found at follow-up. A finding was considered false-positive if it was not recurrent at follow-up in an area with residual uptake. A finding was considered false-negative if a tumor was histopathologically proven or the finding was recurrent at follow-up in an area with no uptake.
Data Analysis
Statistical analyses were performed using the Wilcoxon signed-rank test and the Mann–Whitney U test. Actual local control was estimated by the Kaplan–Meier method. Hazard ratios with 95% confidence intervals were calculated, with a P value of less than 0.05 considered to be statistically significant.
RESULTS
Patient and Tumor Characteristics
Patient and tumor characteristics are summarized in Table 1. In all patients with primary lesions of HNSCC, focally increased 18F-FLT and 18F-FDG uptake was visible. As to metastatic lymph nodes, only 1 metastatic node could not be detected by 18F-FLT PET, although 18F-FDG PET and CT yielded a positive diagnosis.
Patient Characteristics
The first PET scans were acquired within 3 wk before the start of RT. The second scans were acquired at the approximately 40-Gy point during RT (median, 42 Gy; range, 30–52 Gy, and median, 5 wk; range, 3–7 wk after the start of RT). The third scans were acquired after the completion of RT (median, 5 wk; range, 3–11 wk). Some of the second PET scans could not be obtained because of scheduling errors (18F-FLT PET in 2 patients and 18F-FDG PET in 1 patient). Some of the third 18F-FDG PET scans could not be obtained because of the condition of the patient (2 patients). The median follow-up time of surviving patients from the beginning of treatment was 39 mo (range, 12–65 mo). During the follow-up period, 4 primary sites and 5 lymph nodes showed residual or recurrent disease. At the last follow-up, 24 patients were alive and 4 had died. All deaths were tumor-related.
Changes in 18F-FLT and 18F-FDG Uptake with Irradiation
Figure 1 shows a typical case of hypopharyngeal cancer. The 18F-FLT accumulations in primary and metastatic lesions showed apparent decreases during RT, whereas 18F-FDG accumulations persisted.

PET images of patient with hypopharyngeal cancer (patient 14, Table 1) before RT (A and D), 3 wk after initiation of RT (B and E), and 4 wk after end of RT (C and F). Pretreatment 18F-FLT and 18F-FDG axial PET images showed increased metabolism in primary tumor and metastatic lymph node (18F-FLT SUVs, 9.16 and 6.06, respectively; 18F-FDG SUVs, 21.81 and 13.37, respectively). 18F-FLT and 18F-FDG SUVs decreased after 30 Gy of irradiation (18F-FLT SUVs, 2.86 and 2.14, respectively, and 18F-FDG SUVs, 11.44 and 6.39, respectively). 18F-FLT uptake in primary site and lymph nodes was same as in surrounding muscle (SUVs of 0.93, 0.9, and 0.9, respectively) at 4 wk after completion of treatment, whereas increased uptake of 18F-FDG persisted (SUV of 4.66 in primary lesion and 3.75 in lymph node). Patient was alive and without evidence of recurrent disease 19 mo after therapy.
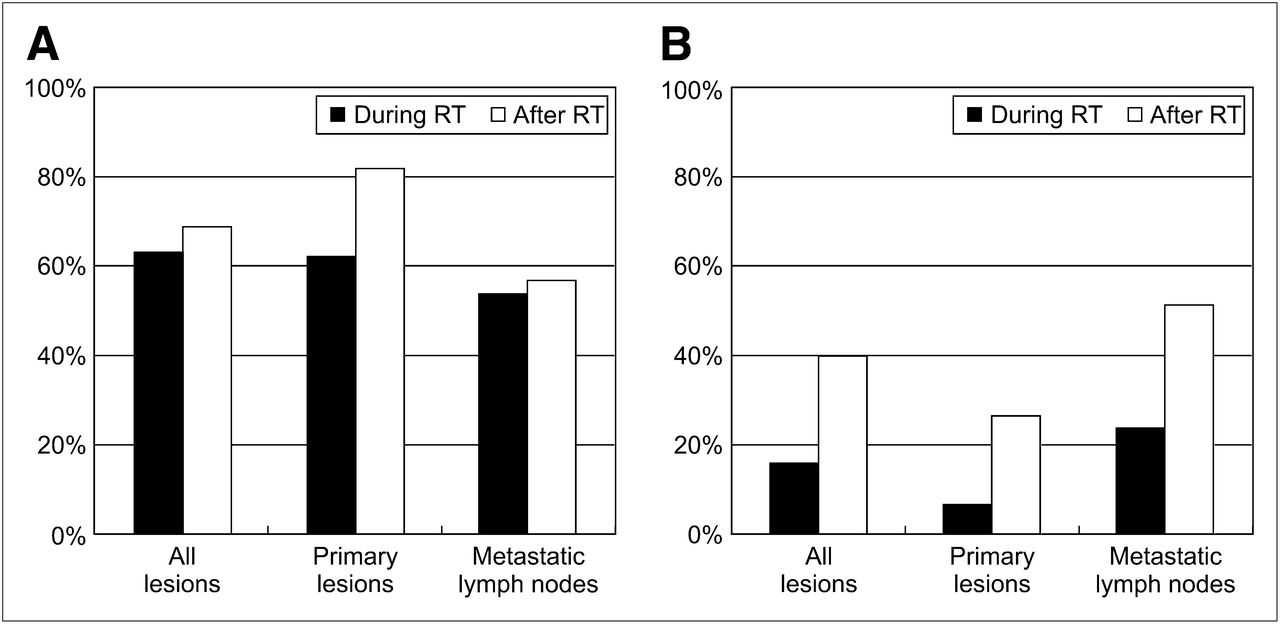
In the second 18F-FLT scan, 34 of 54 lesions (63%) demonstrated the absence of 18F-FLT accumulation whereas 18F-FDG accumulation disappeared in only 9 of 56 lesions (16%) during RT (P < 0.0001). The absence of 18F-FLT accumulation after RT slightly increased to 69% (40/58), and the absence of 18F-FDG accumulation after RT significantly increased to 40% during RT (21/53) (P = 0.0018). Although no significant difference was observed between primary lesions and lymph node metastases during treatment on 18F-FLT PET scans, the absence of 18F-FLT accumulation was significantly more common in the primary lesions than in lymph node metastases after treatment (P < 0.05). In contrast, the rate of disappearance of 18F-FDG accumulation on 18F-FDG PET was significantly higher in lymph node metastases than in primary lesions both during and after treatment (P < 0.05) (Fig. 2).

Rates at which accumulation of 18F-FLT (A) and 18F-FDG (B) disappeared during and after RT. In both primary lesions and lymph node metastases, rate during RT was significantly higher for 18F-FLT than for 18F-FDG (P < 0.001 and P < 0.01, respectively). After RT, no significant difference was found in lymph node metastases, whereas primary lesions differed significantly between 18F-FLT PET and 18F-FDG PET (P < 0.001).
Correlation Between Signal Change on PET and Local Control
The results of qualitative assessments are presented in Tables 2 and 3. During midtreatment imaging, 18F-FDG PET had high sensitivity (100%) and a high negative predictive value (100%) but low specificity (19%), a low positive predictive value (PPV) (17%), and low overall accuracy (30%). In contrast, midtreatment 18F-FLT PET showed significantly higher specificity (72%) and overall accuracy (74%) than 18F-FDG PET (P < 0.0001 and P < 0.0001, respectively). Only 1 primary lesion, in patient 9, showed a false-negative result with 18F-FLT PET both during and after RT. Compared with the results obtained during RT, the specificity and overall accuracy of posttreatment 18F-FDG PET were significantly improved (P = 0.003 and P = 0.007, respectively). Although all parameters on posttreatment 18F-FLT PET tended to improve in comparison to those during RT, the differences did not reach statistical significance. Specificity and overall accuracy for lymph node metastases with 18F-FLT PET were the same as those with 18F-FDG PET at 5 wk after RT.
Comparison of Qualitative (Visual) Analysis of PET During RT
Comparison of Qualitative (Visual) Analysis of PET After RT
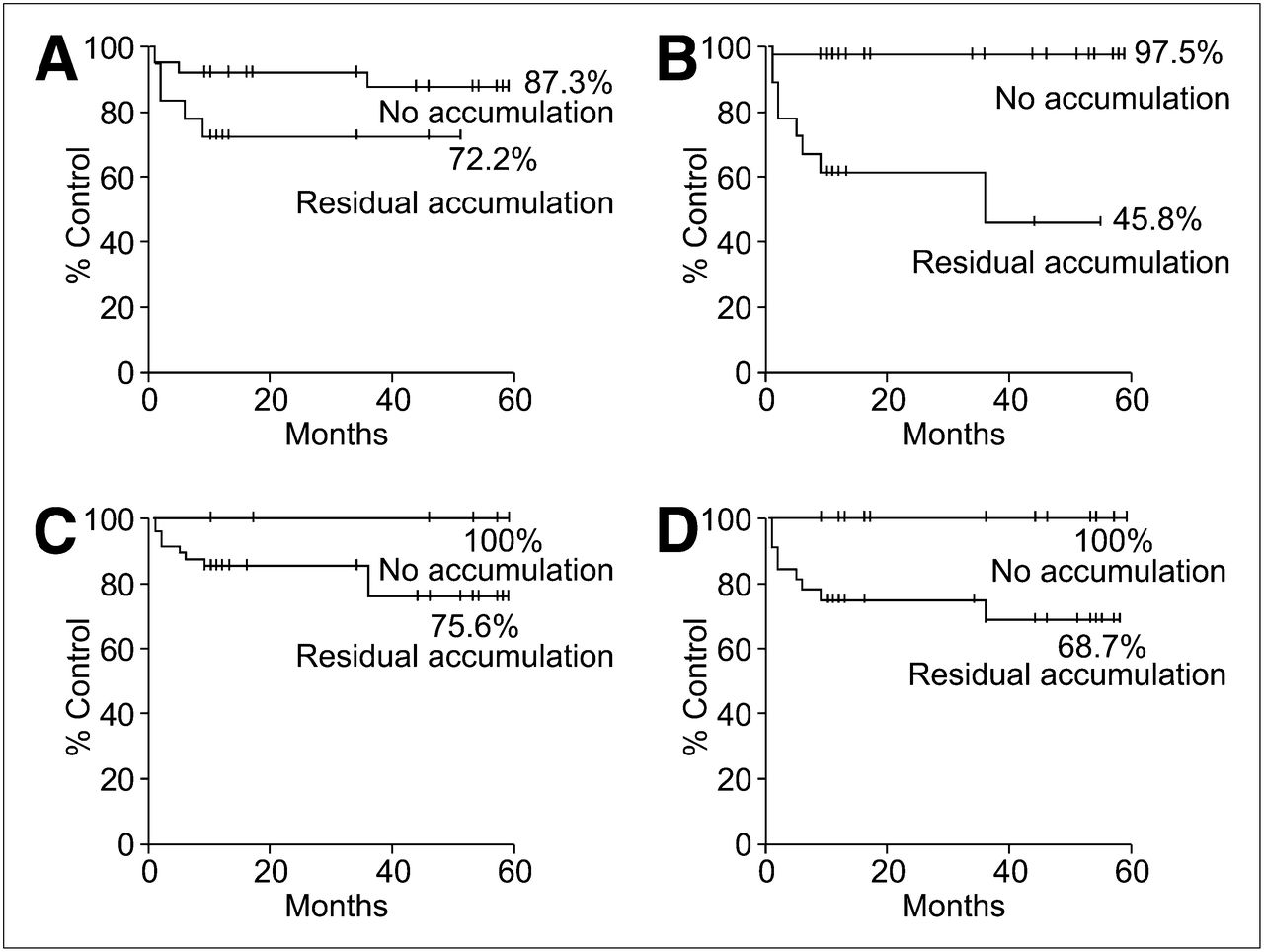
All lesions were divided into 2 groups: residual accumulation and no accumulation. The Kaplan–Meier method was used to identify significant differences in 3-y local control between the 2 groups based on posttreatment 18F-FLT PET (hazard ratio, 25.57; 95% confidence interval, 5.739–113.9; P < 0.0001) and posttreatment 18F-FDG PET (hazard ratio, 6.062; 95% confidence interval, 1.597–23.02; P = 0.0081). No significant differences were detected between 18F-FLT PET and 18F-FDG PET during treatment (Fig. 3).
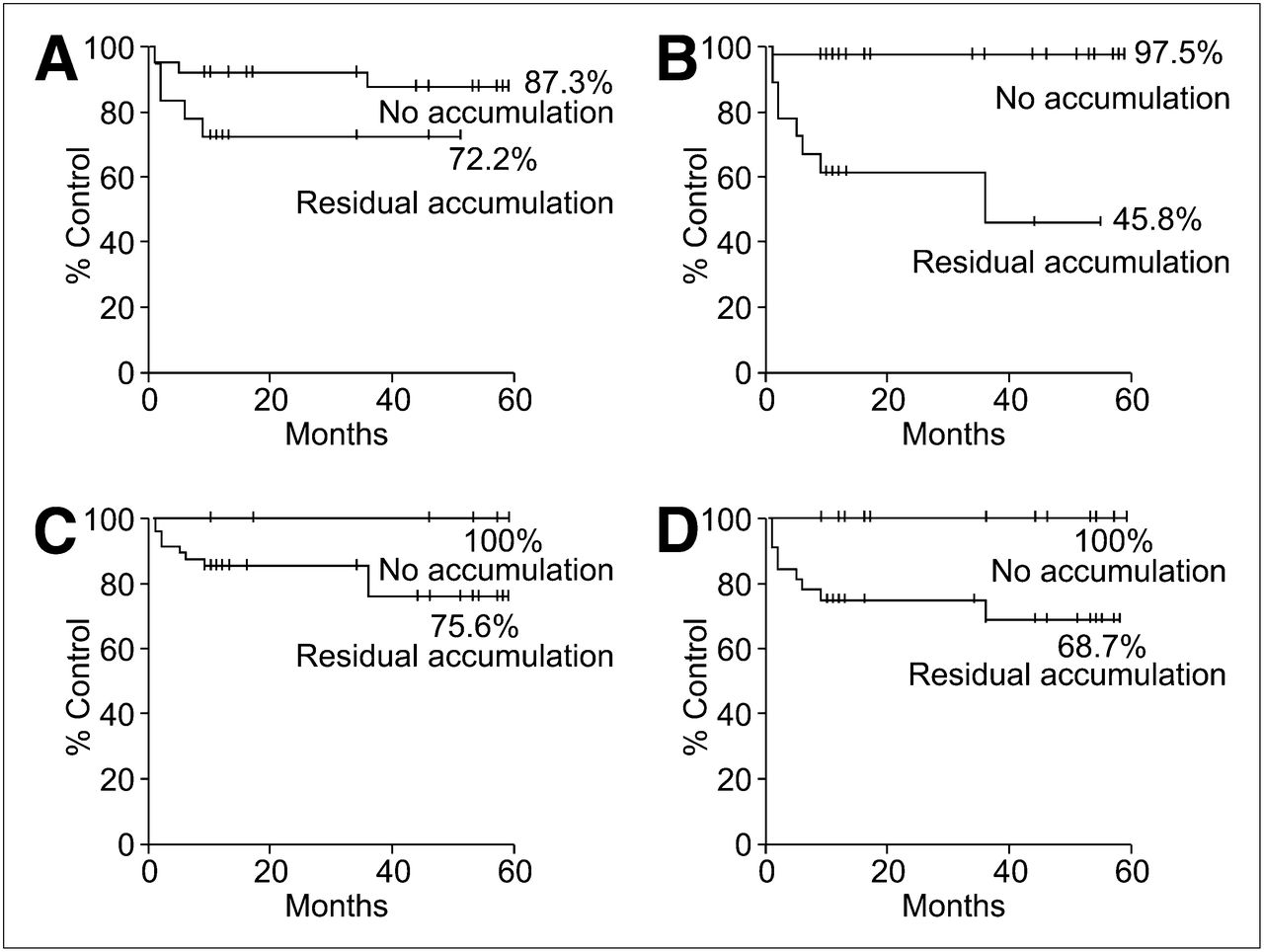
Local control in residual-accumulation and no-accumulation groups. Kaplan–Meier estimates are shown for local control on 18F-FLT PET during treatment (A), on 18F-FLT PET after treatment (B), on 18F-FDG PET during treatment (C), and on 18F-FDG PET after treatment (D). Differences in local control between 2 groups on posttreatment 18F-FLT PET (97.5% vs. 45.8%, P < 0.0001) and posttreatment 18F-FDG PET (100% vs. 68.7%, P = 0.0081) were significant.
DISCUSSION
18F-FLT retention has been shown to correlate with thymidine uptake and thymidine kinase-1 activity (8,22). Thymidine kinase-1 activity is extremely sensitive to ionizing radiation, and changes in 18F-FLT uptake are thought to reflect the direct biologic effect of RT (23,24). Yang et al. (25) showed 18F-FLT uptake by SCCVII tumor cells to be significantly reduced within 24 h after a single dose of irradiation, with no visible tumor shrinkage or morphologic change. In addition, the tumor uptake of 18F-FDG did not decrease 24 h after radiation, at a time when there was a significant reduction in 18F-FLT tumor uptake. They concluded that reduced 18F-FLT SUV preceded reduced 18F-FDG uptake, suggesting that decreased cell proliferation precedes changes in glucose metabolism.
In experimental models of esophageal carcinoma (26), 18F-FLT uptake after docetaxel plus irradiation declined by 75% compared with baseline by 2 d after chemoradiotherapy, whereas the decrease in 18F-FDG uptake was gradual and less pronounced.
In clinical practice, Herrmann et al. (12) found that 18F-FLT maximal SUV had already decreased significantly 2 d after the chemotherapy in non-Hodgkin lymphoma patients. Furthermore, the authors were able to detect a significant difference in the reduction of tumoral 18F-FLT uptake between patients reaching a partial response and patients reaching a complete response at the end of therapy. Kenny et al. (13) examined breast cancer patients before and 1 wk after neoadjuvant chemotherapy and found that the decrease in 18F-FLT SUV was significantly different between patients with clinical responses and patients with stable disease.
In head and neck cancer patients, Menda et al. (27) demonstrated a significant decrease in 18F-FLT uptake after 10 Gy of RT for HNSCCs. Troost et al. (16) examined oropharyngeal cancer patients before treatment and 2 and 4 wk after initiation of RT. The reduction in SUVs was more than 2-fold in the initial phase of treatment and a further 2-fold in the fourth week. They concluded that defining the tumor subvolume with 18F-FLT PET and dose escalation to these regions was feasible. On the basis of these findings, 18F-FLT PET is expected to assess the therapeutic response much earlier than currently used imaging modalities, including 18F-FDG PET.
However, few studies have examined whether changes in 18F-FLT PET correlate clinically with local control or survival. Only 1 report showed a correlation between 18F-FLT uptake and survival in head and neck tumor patients (28). The authors reported a significant correlation between pretreatment 18F-FLT SUVs and survival. However, their study had a small sample size (19 malignant and 1 benign tumor) and a short follow-up time (median, 18 mo).
The optimal timing of posttreatment 18F-FDG PET after chemoradiotherapy has yet to be defined. In general, the rate of false-positive cases declines with the interval between the end of therapy and PET. Several authors have suggested 10–12 wk after the end of treatment (29–32), but others showed that negative PET findings accurately determined a complete response to therapy within 8 wk (33–35). Previously, we examined the usefulness of early posttreatment 18F-FDG PET for assessing local control quantitatively and qualitatively (36). We found the combined analysis of posttreatment SUV and percentage change in SUV to be useful for predicting the therapeutic responses of metastatic lymph nodes. However, we still have the problem of how to handle the positive findings of both qualitative and quantitative analyses involving the primary site.
In the present study, to compare the utility of 18F-FLT PET with that of 18F-FDG PET for assessment of the early locoregional clinical outcomes of chemoradiotherapy for patients with HNSCCs, we performed 18F-FLT and 18F-FDG PET before RT, 4 wk after the initiation of RT, and 5 wk after completion of RT. We observed that 18F-FLT uptake was significantly decreased compared with that of 18F-FDG during and after RT. 18F-FLT accumulations during RT disappeared in 34 of 54 lesions (63%), and negative predictive value was 97%. 18F-FDG PET during RT also had a high negative predictive value (100%), but only 9 lesions showed absence of 18F-FDG. 18F-FLT PET yielded 1 false-negative result during and after RT. This patient had advanced oropharyngeal cancer, and progressive necrosis occurred during and after chemoradiotherapy. Although residual cancer cells were not detected by excisional biopsy, tumor persistence was suspected from clinical findings. In this case, a remarkable blood flow reduction due to necrosis might have accounted for the absence of 18F-FLT accumulation.
The appropriate timing of intratherapy PET scans is important. Everitt et al. (37) assessed patients with non–small cell lung cancer undergoing chemoradiotherapy. Arrest of tumor cell proliferation became apparent after 20 Gy in 2 patients. The authors suggested that measurement of 18F-FLT uptake in tumors after 40 Gy might possibly be used to determine whether accelerating RT administration to counteract accelerated proliferation was warranted.
In the present study, the disappearance of 18F-FLT accumulation was significantly more common in the primary lesions (from 62% to 82%) than in lymph node metastases (from 54% to 57%) 5 wk after RT. In addition, the specificity and overall accuracy of posttreatment 18F-FLT PET in the primary site was significantly higher than that of 18F-FDG PET (P < 0.001).
Our previous data (36) revealed that 18F-FDG PET was useful for predicting the therapeutic responses of metastatic lymph nodes 5 wk after the irradiation. In this study, the accuracy of 18F-FDG PET was the same as that of 18F-FLT PET in metastatic lymph nodes after the therapy. These results suggest that 18F-FLT PET was more useful for assessing early locoregional clinical outcomes in primary lesions and that 18F-FLT PET may discriminate tumors from posttreatment inflammation more effectively than 18F-FDG PET.
For the analysis of 18F-FDG uptake in the pathologic target volume, various approaches have been proposed. Semiquantitative analyses using maximal SUV are widely applied to assess the efficacy of treatments in various types of cancer. In the present study, we tried to predict early therapeutic responses with maximal SUV. However, no significant differences were found between the no-recurrence group and the recurrence group in the 18F-FLT and 18F-FDG PET study. Other semiquantitative analyses (e.g., change in SUV and tumor–to–normal-tissue ratio) or quantitative analysis (e.g., metabolic response) may make it challenging to understand the relationship between tracer uptake and tumor properties.
Our study population was heterogeneous with respect to tumor entities. Patient numbers were too small to allow analysis of the results by primary site location. Therefore, larger-population studies are needed to confirm the validity of these findings.
CONCLUSION
Concurrent chemoradiotherapy is widely used as the definitive treatment for advanced HNSCCs. 18F-FLT PET during treatment and early follow-up has the potential to predict therapeutic responses and identify patients needing close follow-up to detect persistent or recurrent disease. 18F-FLT PET assessment of therapeutic responses has potential for determining the optimal treatment course and predicting outcome.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jul. 7, 2012.
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 14, 2011.
- Accepted for publication May 2, 2012.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- FLT PET/CT imaging of metastatic prostate cancer patients treated with pTVG-HP DNA vaccine and pembrolizumab
- PET Imaging in Head and Neck Cancer Patients to Monitor Treatment Response: A Future Role for EGFR-Targeted Imaging
- 18F-FLT PET Evaluation of Radiation Response
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- PET Imaging of Proliferation with Pyrimidines
- PET Imaging During Radiotherapy of Head and Neck Cancer