


Abstract
The Fukushima Daiichi nuclear power facility, in the Futaba District of the Fukushima Prefecture in Japan, was severely damaged by the earthquake and ensuing tsunami that struck off the northern coast of the island of Honshu on March 11, 2011. The resulting structural damage to the plant disabled the reactor's cooling systems and led to significant, ongoing environmental releases of radioactivity, triggering a mandatory evacuation of a large area surrounding the plant. The status of the facility continues to change, and permanent control of its radioactive inventory has not yet been achieved. The purpose of this educational article is to summarize the short-term chronology, radiologic consequences, emergency responses, and long-term challenges associated with this event. Although there is ongoing debate on preparedness before the event and the candor of responsible entities in recognizing and disclosing its severity, it largely appears that appropriate key actions were taken by the Japanese authorities during the event that should mitigate any radiologic health impact. These actions include an organized evacuation of over 200,000 inhabitants from the vicinity of the site and areas early in the emergency; monitoring of food and water and placement of radiation limits on such foodstuffs; distribution of stable potassium iodide; and systematic scanning of evacuees. However, the risk of additional fuel damage and of further, perhaps substantial, releases persists. The situation at the Fukushima Daiichi nuclear facility remains fluid, and the long-term environmental and health impact will likely take years to fully delineate.
The Fukushima Daiichi (meaning “Fukushima 1” or “Fukushima the First”) power facility, constructed and operated by the Tokyo Electric Power Co. (TEPCO), is located on a 3.5-km2 (860-acre) site in the towns of Okuma and Futaba in the Futaba District of the Fukushima Prefecture in Japan. First commissioned in 1971, the facility consists of 6 boiling water reactors. When operational, it provided a total of 4.7 gigawatts electrical power, making this facility one of the 15 largest nuclear power installations in the world. The facility suffered major structural damage from a magnitude 9.0 earthquake (the Tōhoku earthquake) and ensuing tsunami that struck off the northern coast of the island of Honshu, Japan, on March 11, 2011 (1). These events triggered a major nuclear event that Japanese authorities have declared to be at level 7, the highest level on the International Nuclear Event Scale (2). Significant environmental releases of radioactivity required mandatory evacuations and other protective actions. The status of the Fukushima Daiichi nuclear facility continues to change, and as of the writing of this article, permanent containment of its radioactive inventory and the associated contaminated cooling water had not yet been achieved. Further substantial releases of radioactivity remain a possibility. TEPCO has developed a plan to bring all reactors under control and to reduce the possibility of release of radioactive materials within 6–9 mo (October–December 2011) (3,4).
Governments, various regulatory and advisory bodies, the news media, and professional societies have already begun to evaluate the preparation and response of TEPCO and the Japanese authorities (4–9). In addition, it is natural that comparisons of the Fukushima Daiichi event to Three Mile Island and Chernobyl have emerged. However, the ultimate health and economic impact of the damage to this facility—and the specific lessons associated with safety management, preparations, and response—are unclear at this time and will likely take years to delineate.
Nuclear medicine professionals are expected to assist in the response to nuclear emergencies. As such, an understanding of the chronology, radiologic consequences, and emergency response actions associated with such events is essential. This article is aimed at describing the Japanese tsunami and resulting nuclear emergency at the Fukushima Daiichi power facility and providing the nuclear professional with guidance and background information that can be useful for mitigating adverse public health outcomes during such a large-scale nuclear event. This continuing education article is directed at all nuclear medicine professionals and associated staff, including nuclear medicine physicians, technologists, nurses, residents, physicists, radiochemists, radiopharmacists, and researchers. The article specifically addresses the following learning objectives: describe the Fukushima nuclear reactor design and identify the multiple failures resulting from the earthquake and tsunami natural disasters; explain the sources and types of radioactive material available and released to the environment during the early weeks of the Fukushima nuclear reactor accident and recognize why specific public protective actions were necessary; and consider the appropriate use of potassium iodide (KI) as a countermeasure after nuclear reactor accidents.
FUKUSHIMA DAIICHI NUCLEAR REACTORS
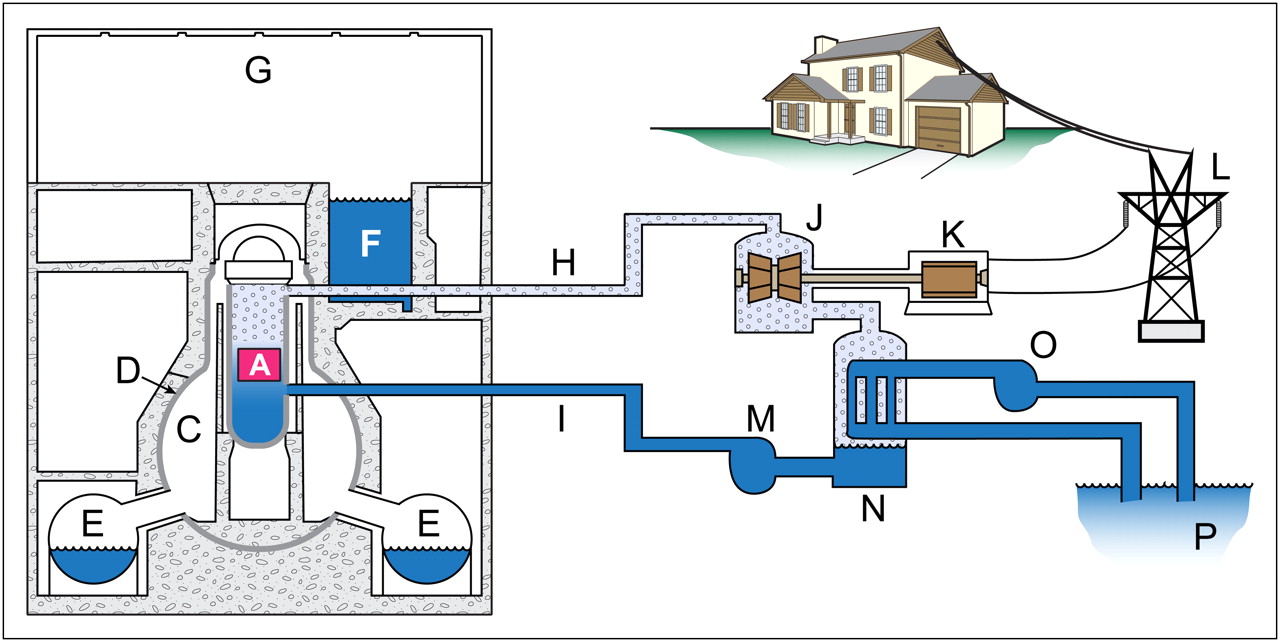
The Fukushima Daiichi nuclear power facility consists of 6 boiling water reactors (Fig. 1). Such reactors use the heat produced by nuclear fission to boil water (pressurized to ∼75 atm at a temperature of ∼285°C) to produce steam. The resulting steam directly drives an electric generator turbine and is cooled in a condenser, converting it back to the liquid phase, which is then subsequently pumped back to the reactor core to maintain core cooling and resume the cycle (Fig. 1). Therefore, water both removes heat from the core (maintaining fuel temperatures within operational range) and flashes to steam used to propel the turbines for the electrical generators. Fukushima Daiichi unit 1 is rated at about 1,380 megawatts thermal (MWt) heat generation; units 2, 3, 4, and 5 are rated at about 2,400 MWt; and unit 6 is rated at about 3,400 MWt (10).
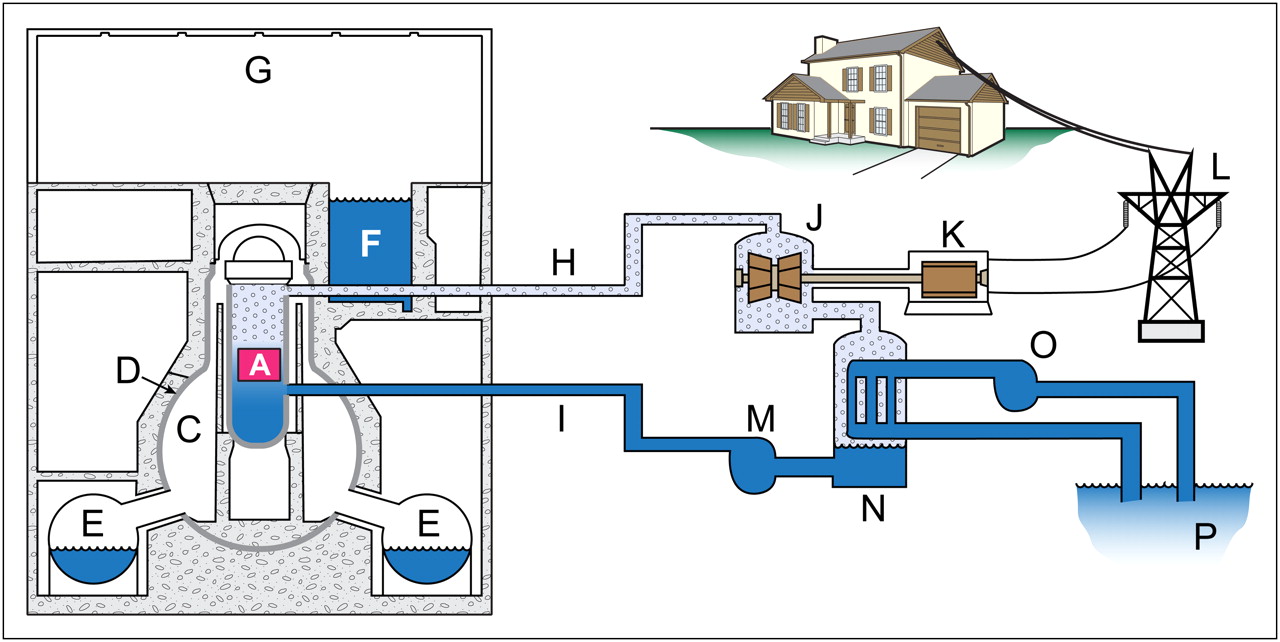
Typical boiling water reactor, containment, and cooling loop design: reactor pressure vessel and core (A), dry well (C), primary containment vessel (D), wet well torus (E), spent-fuel pool (F), reactor and refueling building (G), steam piping (H), steam turbine (J), electrical generator (K), power grid (L), cooling water (I), reactor coolant pump (M), condenser (N), secondary cooling loop (O), and Pacific Ocean (P).
The nuclear components of a boiling water reactor begin with the fuel pellets. These consist of solid ceramic pellets of 235U-enriched (∼3%–5%) uranium dioxide or of a mixed oxide of both uranium and plutonium isotopes. These pellets are stacked in long, thin tubes made of corrosion-resistant zirconium alloy. These fuel pellet–containing tubes are bundled to form a fuel assembly, which is about 4.5 m (14.5 ft) in length (11). The reactor cores at Fukushima Daiichi are designed to hold several hundred fuel assemblies. Spent-fuel assemblies are temporarily stored in a 14-m-deep pool of water, with electric pumps continually circulating water to dissipate heat from the still highly radioactive fuel rods. The thermal heat production of the spent-fuel rods is approximately 6% of that of the reactor immediately after shutdown, decreasing over several days to cold-shutdown temperatures; several years of additional cooling are then required before transfer to dry storage casks (12).
Most of the Fukushima Daiichi units are equipped with so-called Mark I containments (Fig. 1). The major components of the primary containment structure include the dry well, the wet well, and a venting network connecting the two. The dry well is a light-bulb–shaped, steel-lined pressure vessel backed over most of its surface with reinforced concrete that surrounds the cylindric steel reactor pressure vessel containing the fuel assemblies in the reactor core and the coolant loop piping. The wet well is situated beneath the dry well and is connected to it by a system of vent piping. The wet well is a steel or concrete toroidal (or donut-shaped) pressure vessel normally filled to about half its height with water.
There are several barriers limiting release of radioactive fission products from the nuclear fuel into the environment (13). The fuel-rod cladding and reactor pressure vessel and its piping form the reactor coolant-pressure boundary and the primary containment. In addition, the secondary containment surrounds the primary containment and houses emergency core cooling systems. Typically, a simple steel building encloses the top of the reactor floor to protect the refueling bay and spent-fuel pool and forms a minimal outermost barrier.
ISOTOPIC SOURCE TERMS AND POSSIBLE RELEASE MECHANISMS
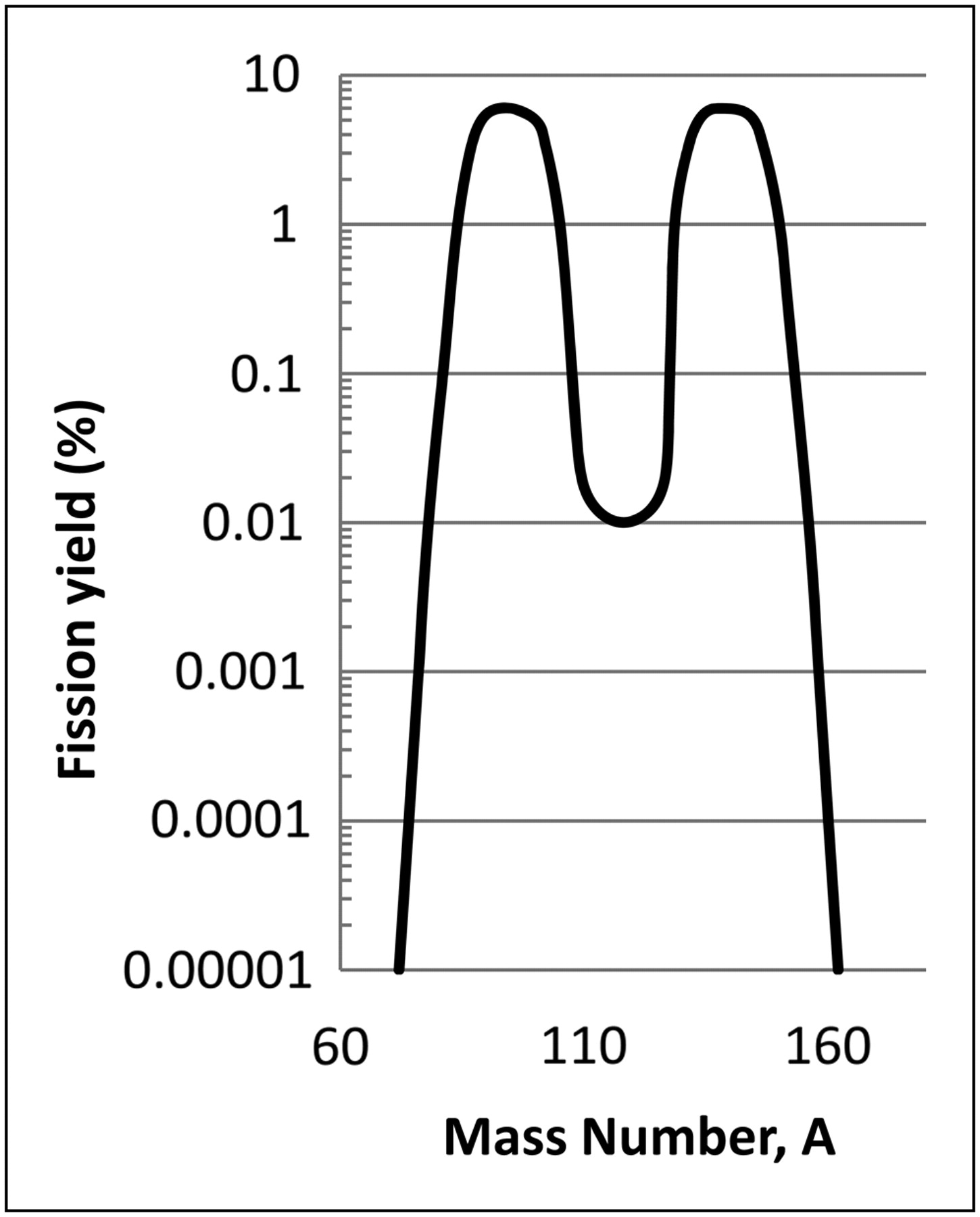
In the 235U fission process, a neutron is captured by the 235U nucleus, causing it to split (fission) into 2 smaller fragments as well as 2–3 neutrons, which may be captured by and split up to 3 additional fissionable nuclei and thus sustain the nuclear chain reaction. The energy released per 235U fission is about 200 MeV; together with the heat generated by decay of the fission product daughters, this is the primary contributor to heat production. The fission product yields vary as a function of their atomic numbers, following a bimodal distribution with atomic mass numbers in the range of 80–110 (krypton, strontium, molybdenum, etc.) and 120–155 (iodine, xenon, cesium, barium, lanthanum, cerium, etc.) (Fig. 2). During the reactor fission cycle, the noble gases and some volatilized forms of radioactive iodine will escape the ceramic fuel pellets and be captured in the space (fuel gap) between the fuel pellets and the wall of the zirconium alloy “can” of the fuel rods.

Bimodal distribution of 235U fission products.
If an operating reactor core or a spent-fuel pool (with recently burned fuel elements) undergoes severe and prolonged loss of coolant, several escalating release mechanisms can be initiated. In the first type of event, if the fuel-rod walls are damaged by mechanical means or undergo cracking during a slight overheat condition, the volatilized fission products can be released to the reactor coolant water. In the second type, if the fuel temperature continues to rise in the absence of core cooling, the fuel experiences a serious overheat condition, which can release approximately 10- to 20-fold more of the fission products. In the third and most severe type of event, damaged fuel rods can lose integrity, causing the oxide fuel pellets themselves to melt, releasing an additional 2- to 3-fold more of the fission products.
Table 1 presents estimates of the available total radioactive releases for these respective scenarios based on a 2,400-MWt reactor (14) and identifies the fuel temperatures needed for each such condition. The specific percentage of each fission product released from the core is estimated to be higher in fuel-melt than in fuel-overheat conditions (Table 2) (14). Although both conditions likely result in a significant release of noble gases, iodine, and cesium, there are differences among these conditions for the other fission products. In fuel melt, there is a significant amount of barium (140Ba) and strontium (89Sr, 90Sr), as well as other radioactive elements, including ruthenium, lanthanum, yttrium, neptunium, and molybdenum. Although radioactive products such as these were seen in weapons testing fallout (because they were created in a near-instantaneous large fission and were immediately available for release), in a nuclear reactor they are trapped in the fuel rods and are released in significant quantities only when the fuel melts. Also in reactor accidents, fission product releases can undergo other removal mechanisms such as deposition in the reactor pressure vessel, the primary containment, or filtration. The specific pathway to the environment will determine such reductions.
Sources for Release of Radioactivity Assuming ∼2,400-MWt Reactor at 7 Days After Shutdown
Percentage of Core Fission Products by Element Released in Fuel-Overheat or Fuel-Melt Conditions
Released noble gas fission products have relatively short half-lives and are typically a concern only as an external source. Longer-lived 134Cs (half-life, ∼2 y) and 137Cs (half-life, ∼30 y) can result in both external and internal exposures. Iodine fission products, especially longer-lived 131I (half-life, ∼8 d) can also be of concern for both external and internal exposures, with the latter occurring via the pasture deposition–cow milk–human thyroid pathway. Similarly, released strontium fission products can be of concern, especially for food deposition pathways.
CHRONOLOGY OF THE FUKUSHIMA DAIICHI NUCLEAR FACILITY ACCIDENTS
At 2:46 PM on Friday, March 11, 2011, a magnitude 9.0 earthquake occurred in the Pacific Ocean (the largest in Japan's recorded history), centered 130 km east of the city of Sendai on the eastern coast of the island of Honshu. The quake, which may have lasted as long as 3 min, set off a massive tsunami with devastating floods inundating an area as large as 561 km2 (4) and extreme damage and loss of life (∼30,000 or more fatalities) (15). The ground acceleration during the quake triggered automatic shutdowns of several nuclear power facilities (including Onagawa, Takai, Fukushima Daiichi, and Fukushima Daini) along the northeast coast of Honshu. The shutdown procedures include automatic insertion of control rods (comprising a mixture of materials with a high–neutron-capture cross-section, such as cadmium) into the reactor core to absorb fission neutrons and thus bring the fission reaction below criticality, thereby stopping the nuclear chain reaction. Although each of the nuclear facilities along the northeast coast of Honshu experienced some damage and perhaps pressure spikes, shutdown procedures were able to achieve and maintain a safe, cold-shutdown condition in all plants except for those at Fukushima Daiichi.
Fukushima Daiichi units 1–3 were operating at the time of the earthquake and tsunami. Units 4–6 were in an outage status during the event, having been previously taken off line for inspection and planned maintenance. The reactor vessel of unit 4 had also been completely defueled in December 2010, with all of its spent fuel moved to the unit 4 spent-fuel pool on the upper floor of the reactor building (16).
The plants had been modified in 2002 with a seawall designed to withstand a tsunami with a height of 5.7 m (based on an expected maximum tsunami height of 3.1 m). However, the March 2011 tsunami arriving 41–60 min after the earthquake was estimated to have an unprecedented maximum wave height of 14–15 m (4,17). The tsunami overwhelmed the seawall with massive flooding that disabled critical equipment, including all 6 external power supply sources (4) and on-site backup power emergency diesel generators (with some diesel fuel tanks perhaps even being swept out to sea). The operating reactor cores in units 1–3 required ongoing cooling to dissipate the significant heat they were producing because of decay of the fission products created before the shutdown; this thermal heat production amounts to about 6% of that when the reactor is operating (18).
The loss of electrical power resulted in loss of coolant to each of the reactors and associated spent-fuel pools. Plant personnel tried to maintain reactor-core and spent-fuel pool cooling and to perform shutdown activities with steam turbine–driven emergency core cooling systems, but these remained operational for a maximum of approximately only 8 h (19). Because of extensive damage to the infrastructure in the surrounding areas, it was impossible to deliver additional resources to the site quickly.
As the facility experienced a significant loss of cooling capabilities, the pressures within the primary containment vessels rose beyond design limits and plant personnel initiated primary containment venting to prevent extensive damage to the reactor vessel and a possible large-scale environmental release of radioactive material. Steam, radioactive gases (including 131I), and hydrogen (primarily produced by the oxidizing reaction of the hot zirconium fuel cladding with the boiling water and possibly some radiolysis of water) were therefore released into the refueling bay building above the containment structures. The likely continued reduction of the water levels in the core to levels below the top of the fuel rods resulted in significant additional overheating and cladding damage and some melting of the fuel cladding or of some fuel pellets. In the afternoon of March 12, a hydrogen explosion occurred at the top of the unit 1 reactor building, severely damaging the roof and walls of the top floor and injuring 4 workers. On March 14, unit 3 also experienced a large hydrogen explosion, damaging the upper portion of its building and injuring 11 people (20). Then, on March 15, unit 2 experienced an explosion, likely in the wet well torus under the primary containment (Fig. 1). In each of these events, as well as during required pressure-relieving steam-venting operations, significant radioactivity was released to the environment. These hydrogen explosions further impeded emergency work (21) and attempts to provide active cooling.
On March 17, one electrical generator at unit 6 was restored to operation, and external power was returned to units 5 and 6, allowing cooling equipment to be restarted at units 5 and 6, the least damaged at the facility. It appears that the facility was unable to maintain adequate cooling of spent-fuel pools in units 1–4, which are normally maintained at or below 50°C. As the fuel temperature continued to rise above the boiling point, it is likely that much (and possibly all) of the water in the pools evaporated and perhaps was also lost through leaks caused directly by the earthquake (22). In the case of the unit 4 fuel pool, the overheating may also have caused the generation of large quantities of hydrogen gas and a subsequent hydrogen explosion, although some believe the hydrogen blast at unit 4 may have originated from hydrogen generated in unit 3 (4,23). Regardless of the source, the explosion at unit 4 caused significant damage to the upper floors of the reactor building and the likely environmental release of additional radioactive fission products. To mitigate further hydrogen explosions, the plant staff removed panels from the roofs of units 5 and 6 to allow any hydrogen gas to escape (16).
During the first several days and weeks after the tsunami, attempts were made to pump seawater supplemented with boron (as a neutron absorber) into the reactor pressure vessels. In an operation known as “feed and bleed,” water was pumped into the reactor vessel and circulated within the damaged fuel rods and fuel pellets. Some of this water boiled to steam, causing a pressure buildup in the containment. To reduce this pressure, the containment system was vented to the atmosphere, releasing further radioactivity. After concerns that the sea salt may have been building up in the central components of the core and thereby preventing efficient cooling, a method to provide fresh water to the site was devised. Large quantities of the cooling water that did not flash to steam or that was later condensed were collected within the containment and turbine hall structures and apparently leaked to the sea from unit 2 and possibly from the other units. Although seawater releases are not as immediate a significant health hazard as are airborne releases, the difficulties managing this highly radioactive water are of concern. As of mid-April 2011, there were an estimated 50,000 tons of highly radioactive water present on site, with fresh water being pumped into the reactors at the rate of 6–7 m3/h (24). This is not sustainable long-term, and an alternate cooling mechanism must be implemented.
In heroic efforts to stabilize the reactors, the facility operators were able to restore some external power to the site, enabling the start of electrically driven pumps to inject cooling water into the core. Several damaged systems will need to be repaired or modified in order to continue to remove heat and to manage the large amounts of radioactively contaminated water at the site. Unresolved issues complicating the situation at the site include primary containment integrity, possible fuel overheating and melting, loss of fuel assembly integrity, and a series of aftershocks of up to 7 or more in magnitude.
To assess the possible types of early fuel events experienced at the Fukushima Daiichi facility, results of turbine hall water sample assays on March 25 and 26 were compared with expected release fractions. Table 3 lists the only nuclides consistently identified and the expected release fractions for different fuel events. It appears that there is more iodine and less cesium than expected for either event specified. The barium activity is consistent with fuel overheat and much lower than that expected for fuel melt. Strontium would also be expected, but the measurement of pure β-emitters requires a separate assay and these data were not available or reported by the time this article was prepared. Overall, the analysis of turbine water samples appears to identify a predominantly fuel-overheat event, with clear indications of some fuel melting as well. TEPCO had initially officially estimated that unit 1 had sustained damage to 55%–70% of the nuclear fuel, unit 2 to 30%–35%, and unit 3 to 25%–30% (10,25,26) and later acknowledged that most of the fuel rods likely melted and fell to the bottom of the reactor pressure vessel within the first 4 d of the earthquake (4,27,28).
Assessing Type of Fuel Damage at Fukushima Daiichi Nuclear Facility
A mix of the radionuclides similar to those listed in Table 3 (and others not yet identified) was therefore likely released to the atmosphere in gaseous (and possibly some particulate) form and to the sea in liquid (and possibly some particulate) form. As of mid-April, the quantity of radioactive iodine and cesium released to the environment was estimated by the Japanese government to have been as high as about 150 PBq (petabecquerel [1015 Bq]) (∼4 MCi) of 131I and about 12 PBq (∼0.3 MCi) of 137Cs (4,21,29). As of early June, the total amount of radioactive material estimated to have been released into the atmosphere during the first week of the crisis was raised to about 770 PBq (∼21 MCi), equivalent to about 10% of that released as a result of the accident at Chernobyl, which was estimated at approximately 5.2 EBq (exabecquerel [1018 Bq]) (∼140 MCi) (16,30,31). Airborne releases and ground deposition would be expected to disperse from the site in a gaussian plume pattern and would be transported out to the Pacific Ocean or inland over populated areas depending on the meteorologic conditions at the time of and immediately after the release. Any waterborne releases would be highly diluted and would follow sea currents, with particulates deposited more locally and soluble products dispersed more widely.
GUIDANCE ON EVACUATIONS AND EARLY SHORT-TERM PROTECTIVE ACTION
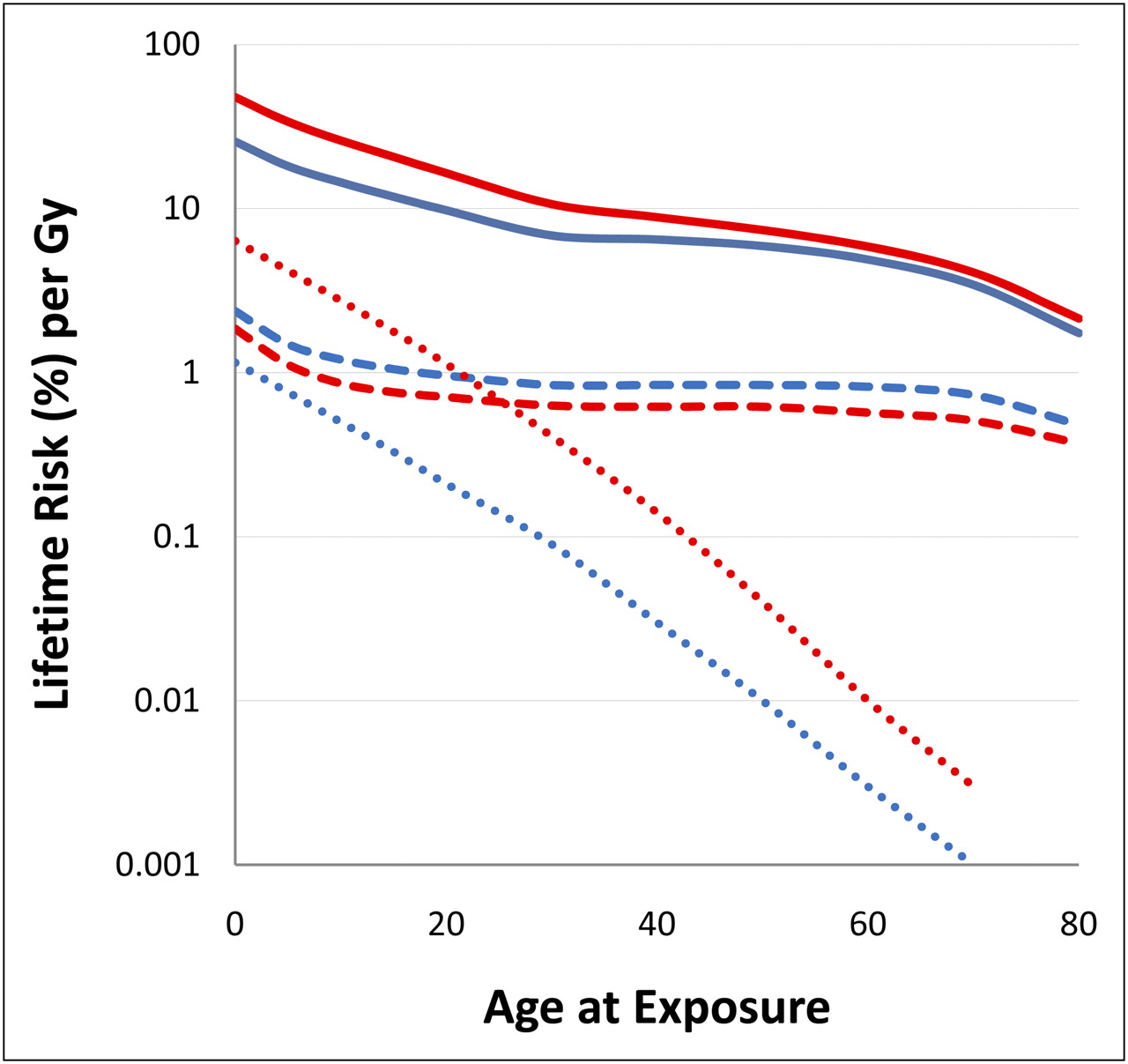
Protective-action guidelines and limits are typically implemented to reduce both deterministic and stochastic health effect risks (32). Figure 3 summarizes some of the most important stochastic risks based on susceptible tissues and organs (such as the thyroid and hematopoietic stem cells) and age at exposure (33). Importantly, the lifetime-attributable cancer risks in Figure 3 are normalized to an absorbed dose of 1 Gy, but there is no evidence to suggest that off-site population doses have even remotely approached 1 Gy. As indicated in Figure 3, children are generally at higher risk than adults from radiation exposure events. The specific public protective actions depend on the exposure pathways and the populations potentially exposed.
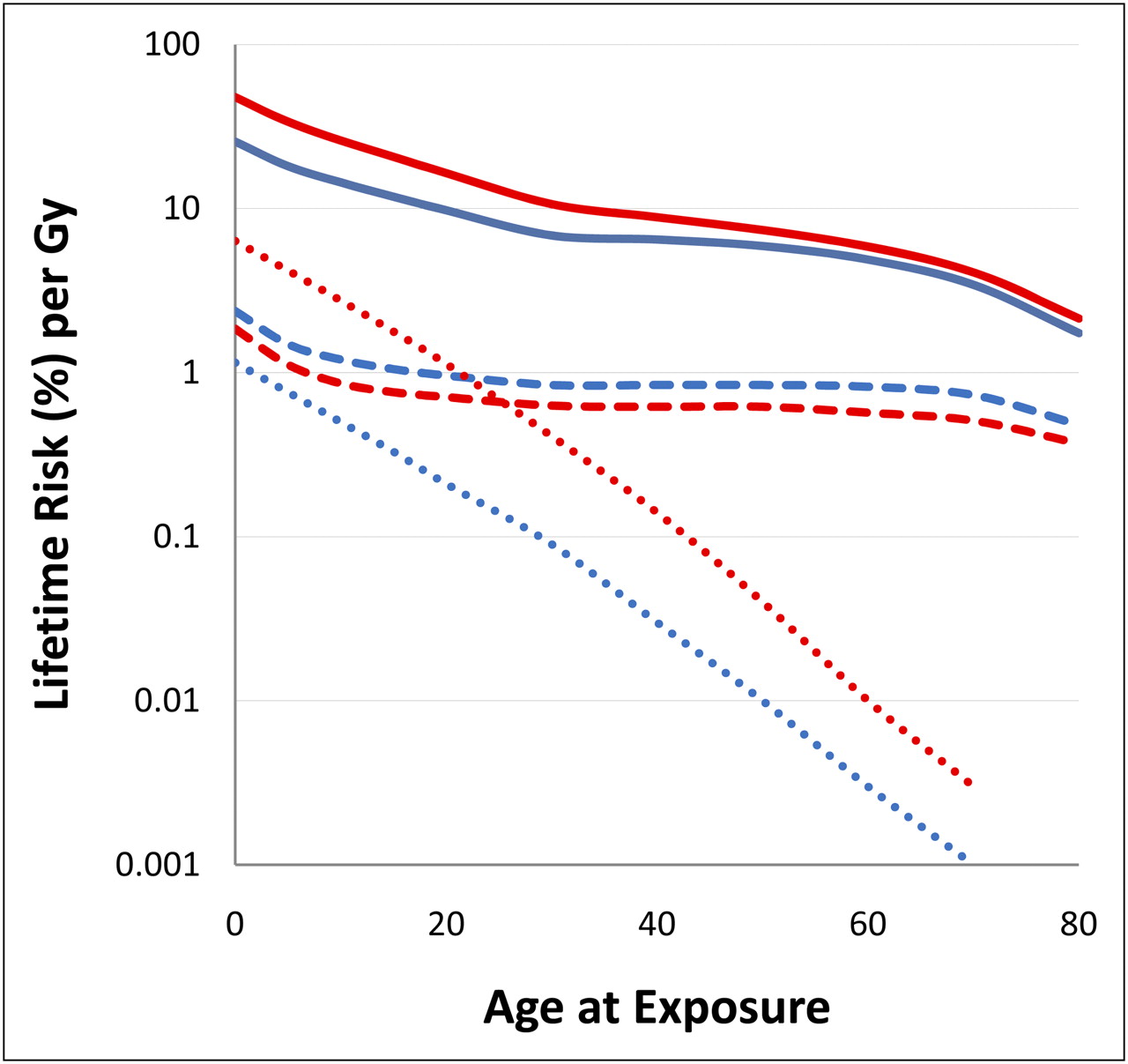
Estimates of lifetime-attributable radiation risks of cancer incidence for all cancers (solid lines), thyroid cancers (dotted lines), and leukemia (dashed lines) from single exposure based on age at exposure. Blue = male data; red = female data.
Several public exposure pathways, including external and internal (inhalation or ingestion) pathways, must be considered when responding to nuclear reactor accidents and ensuing environmental releases of radioactivity. External doses can result from x- and γ-irradiation emitted by radionuclides in the environment (i.e., in the radioactive plume or deposited on the ground, structures, and other locations) and β-particles deposited on skin. Based on the type of events at Fukushima Daiichi, early irradiation may have resulted primarily from radioactive xenon, krypton, iodine, and cesium. Deposited fission products measured and confirmed to date include particulate forms of iodine and cesium.
Initially, on the evening of March 11, the Japanese Prime Minister declared a state of nuclear emergency (4) and, in accordance with preexisting emergency plans to remove the public from the area most likely to be affected by a major release of radioactive material (21), evacuated an area within a 2-km radius and sheltered (in-house) residents between 3 and 10 km from the stricken facility. The evacuation zone was expanded as the event unfolded and the risk of a release of radioactive materials increased. On March 12, the evacuation radius was expanded to 10 km, and it was subsequently expanded further to 20 km after the initial hydrogen explosions and releases. On March 13, decontamination screening was started at the evacuation centers, and on March 15, sheltering inside buildings was ordered for those in the 20- to 30-km zone (34). In an effort to control external and inhalation doses to the public, the Japanese government instituted an evacuation zone of 20 km and a shelter-in-place (with evacuation suggested) zone of 30 km (35). Japanese authorities also distributed stable iodine (KI) tablets (or syrup for children) to the evacuation centers and instructed evacuees younger than 40 y to take the KI on March 16 (21,36).
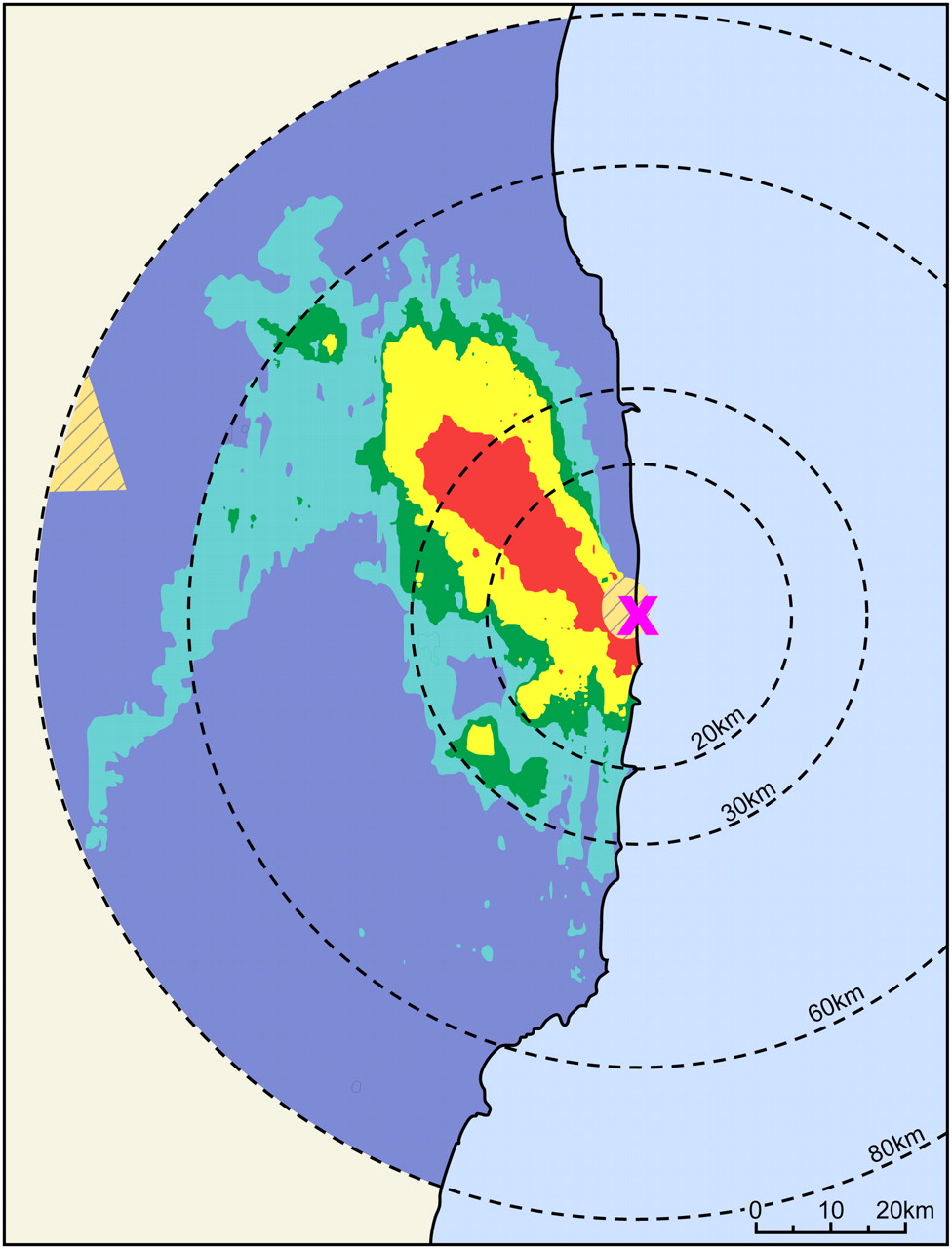
Figure 4 shows the results of aerial measurements of total cesium deposition after the Fukushima Daiichi nuclear facility event based on data compiled by the U.S. Department of Energy, the National Nuclear Security Agency, and the Japanese authorities (37,38). Although the prevailing wind in Japan was from the west and should have carried most of any airborne releases from the plant east out over the Pacific Ocean, deposition is clearly seen to the northwest, with external dose rates of approximately 20–120 μSv/h (2–12 mrem/h), and an additional smaller pathway is indicated to the southwest, with dose rates of approximately 2–12 μSv/h (0.2–1.2 mrem/h). Although some areas beyond 80 km have reported dose rates on the order of 10-fold higher than background exposure rates, most distant areas are currently reporting even lower exposure rates, that is, at background levels. Off-site environmental contamination with 131I, 134Cs, and 137Cs was fairly widespread within the 0- to 20-km radius, as well as in a northwestern plume extending to about 50 km. As of April 29, 2011, the longer-lived 134Cs and 137Cs deposited concentrations ranged from 3 to 30 MBq/m2 within the plume areas and below 300 kBq/m2 outside the plume areas (38).

Geographic distribution of radioactive cesium fission products after Fukushima Daiichi nuclear facility accident, based on aerial monitoring. X = Fukushima; hatched line = no aerial data; red = 3–30 MBq/m2; yellow = 1–3 MBq/m2; green = 0.6–1 MBq/m2; lighter blue-green = 0.3–0.6 MBq/m2; darker blue = <0.3 MBq/m2.
Within the higher-dose plume areas shown in Figure 4, it has been conservatively estimated that people who did not evacuate before the releases occurred (before March 16) would be expected to receive doses in excess of about 20 mSv (2 rem) if they were to remain in that area for 1 y after the release (39). Those who did evacuate before plant release would be expected to receive an approximate dose of less than 20 mSv (2 rem). In addition, for most areas within about 80 km and having lower levels of radionuclide deposition during the releases, it has been conservatively estimated that people who did not evacuate before the releases occurred would be expected to receive about 1 mSv (100 mrem) or less if they were to remain in that area for 1 y after the release (39). Although at least 200,000 people were likely evacuated (36), it is difficult to accurately estimate at this time the total potential number of people exposed in the contaminated areas.
To control external and inhalation doses to the public, the Japanese government instituted an evacuation zone of 20 km and a shelter-in-place (with evacuation suggested) zone of 30 km (35). In addition, on April 11, after the significant northwest deposition pathway had been noted, an additional designation of a “planned evacuation zone” was created: residents of areas with projected annual doses in excess of 20 mSv were directed to evacuate within 1 mo (15). This zone included parts of Minamisoma City, Namie, Kawamata Town, Katsuo, and Iitate villages (15).
To control ingestion exposures, Japanese officials instituted water and foodstuff countermeasures (Table 4) (40). These protective-action limits are lower than those recommended by the International Atomic Energy Agency (41), which are based on a 10-mSv (1-rem) annual dose limit to the most restrictive individual (generally, an infant) if consuming contaminated food for 1 y. In fact, in the latter days of March, several towns and villages did detect 131I in drinking water (e.g., up to ∼1,000 Bq/L recorded in the village of Iitate just beyond 30 km northwest of Fukushima) (42). Also, within several days after the initial releases, milk and leafy vegetables were apparently contaminated with 131I at levels exceeding the protective-action limits. Later, additional food sources were measured and other foods, in particular mushrooms and sand lances (small eellike fish), were also found to be contaminated with 131I, 134Cs, and 137Cs at levels exceeding their respective limits (15). However, the foodstuff and water protective-action limits were likely appropriately conservative.
Protective-Action Activity Concentration Limits (in Bq/L or Bq/kg) on Food and Drinking Water Imposed by Japanese Officials After Fukushima Daiichi Nuclear Facility Event
The International Commission on Radiological Protection has stated that the initial dose action levels for emergency exposure situations should be set in the range of 20–100 mSv to the public and that projected doses approaching 100 mSv will almost always justify protective measures (43). Despite some initial confusion and miscalculation, particularly on the part of TEPCO, of the initial severity of the environmental releases of radioactivity, early protective actions taken by Japanese authorities likely mitigated exposures of the public to released radioactive iodine and cesium. This result is in marked contrast to the Chernobyl nuclear reactor accident, for which protective actions were not implemented in a timely fashion and large public exposures, especially to the thyroid, resulted.
LONGER-TERM PROTECTIVE ACTIONS
Over time, there will be a transition from the current emergency-response situation to a chronic-exposure scenario, with a concomitant change in management from strategies driven mainly by urgency (i.e., to avoid potentially high levels of exposure) and predominantly centralized decision making to more decentralized strategies directed toward reducing exposures to as low as reasonably achievable given the circumstances.
Plans have been announced for a large-scale study of the environmental and health effects of radioactive contamination from the nuclear plant (44). Longer-term protective-action guidance around the Fukushima Daiichi nuclear facility will likely be needed to deal with 134Cs and 137Cs contamination from deposition onto soils, onto facilities, and in water (especially on-site water). Longer-term management strategies will need to address all relevant health, mental health, environmental, economic, social, psychologic, cultural, ethical, and political issues (45).
From the radiologic health perspective, the International Commission on Radiological Protection suggests that a reference level for the optimum protection of people living in contaminated areas should be selected in the lower part of the 1–20 mSv/y range (46), with past experience demonstrating that a suitable value in long-term postaccident situations is 1 mSv/y (45). Nonetheless, selection of levels of permissible exposures and public dose limits for the long-term radiation levels around Fukushima has proven to be difficult and has met with considerable criticism (47), particularly in the area of childhood protection (21). Dose reduction strategies in such a situation may include the relocation of individuals; decontamination of buildings and other infrastructure; remediation of soils and vegetation; changes in animal husbandry; monitoring of the environment and produce; provision of noncontaminated foodstuffs; management of waste; provision of information, guidance, instruction and equipment (e.g., for radioassay); health surveillance; and education (45).
THYROID RISKS AND KI
The scientific literature on radiation (including radioiodine) effects on the thyroid is extensive. Such effects can be classified as either stochastic or deterministic, with the former including low-dose effects such as induction of thyroid cancer and the latter including high-dose effects such as induction of hypothyroidism. (Although there is no rigorous distinction between “low” and “high” radiation doses, the former typically include doses in the diagnostic and occupational range on the order of 100 mSv [10 rad] or less whereas the former are in the therapeutic dose range on the order of 1 Gy [100 rad] or more.) Factors that affect the response of the thyroid to radiation include sex and age at the time of exposure (Fig. 3), with young children being at greatest risk (Fig. 3) (48). Epidemiologic studies have shown a statistically significant dose–response relationship between radiation exposure and thyroid cancer. It appears, however, that radioiodines (in particular 131I) are perhaps 2- to 3-fold less effective (on a per-rad basis) in inducing thyroid cancer than external radiation; this remains controversial, however (49). There is also a risk of benign thyroid nodules after radiation exposure, but the magnitude and dose dependence of that risk are less well known. Functional effects of radiation on the thyroid, such as the induction of hypothyroidism and other deterministic effects, likely do not follow a linear-nonthreshold dose–response model, since functional abnormalities are likely not stochastic. In any case, thyroidal effects offsite (i.e., to the general public) of a breach-of-containment nuclear reactor event are likely restricted to possible induction of benign or malignant neoplasms. This was the case even in a worst-case radioiodine-release scenario such as the Chernobyl nuclear reactor accident.
The Three Mile Island nuclear reactor accident resulted in low environmental releases of radioactivity (<1.1 TBq [< 30 Ci] of 131I), low radiation exposures (well under 1 cGy [1 rad]), and no demonstrable health effects among the surrounding general population (49). In marked contrast, the Chernobyl nuclear reactor accident in Ukraine released large amounts of radioactivity, including over 1.85 EBq (50 MCi) of 131I, with thyroidal doses among children in the surrounding general population as high as several grays (several hundred rads) (49). These occurred primarily through the pasture–cow milk–human pathway and in the absence of appropriate protective measures such as early embargoing of contaminated milk and other foodstuffs. In addition, there was widespread contamination from other radionuclides, principally 137Cs.
The first reports of increases in thyroid cancer risk in children thus exposed were published in 1992, only 6 y after the Chernobyl accident (49). These reports were initially received with skepticism because of the short latency period and the prevailing opinion that 131I was much less effective than external radiation in causing thyroid cancer. Since these early reports, however, there have been comprehensive ongoing efforts to improve thyroid dosimetry and to follow the exposed population to determine the effects of the exposure. There is now compelling evidence of an association between radioactive iodine exposure after childhood exposures and thyroid cancer, but risk estimates and the effects of modifying factors such as the amount of dietary iodine remain uncertain. Nonetheless, birth cohort studies, for example, have revealed a large increase in thyroid cancer incidence after the accident in young Ukrainian children exposed to the fallout from Chernobyl. In Belarus, for example, 1,342 adult and 7 childhood thyroid cancers were reported in the 10-y period before the Chernobyl nuclear reactor accident, compared with 4,006 adult and 508 childhood thyroid cancers reported during the 9-y period after the accident (49). Although the ultimate magnitude of environmental releases of radioactivity from the stricken Fukushima Daiichi nuclear facility and resulting health effects are uncertain, it currently appears unlikely that they will approach those associated with the Chernobyl nuclear reactor accident. Among other considerations, and in contrast to Chernobyl, Japanese officials instituted fairly rigorous radiation protection measures at an early stage. However, despite the rigor of recommendations, the infrastructure and transportation issues that immediately followed the tsunami disaster may have made it difficult to actually implement them efficiently.
In the scenario of a nuclear power plant that releases radioactive material to the environment, oral KI, taken in adequate quantities (65–135 mg in adults) and at the appropriate time, can almost completely block thyroidal uptake of radioiodine (48,50–52). Of course, KI is effective as a radiation countermeasure only for internal contamination with radioactive iodine; it has no effect on radiation exposure or its sequelae otherwise. The protective effect of KI blockade is affected by at least 2 highly variable factors, dietary levels of iodine (expected to be relatively high in the case of the Japanese population) and the time of administration relative to radioiodine internalization. KI taken up to 48 h before 131I exposure can almost completely block thyroid uptake and, therefore, greatly reduce the thyroid absorbed dose. KI taken 24 and 48 h before 131I exposure reduces the 24-h thyroid uptake by approximately 90% and 75%, respectively, with an iodine-sufficient diet (≥150 μg/d) and by 95% and 85%, respectively, for individuals on an iodine-deficient diet (<50 μg/d). KI taken 96 h or more before 131I exposure will have no protective effect. Further, the protective effect decreases rapidly with time after radioiodine exposure, with low overall effectiveness if KI is taken 6 h or longer after an acute exposure. However, if the exposure to radioiodine is protracted, even delayed administration may have a beneficial effect on decreasing the total radiation dose to the thyroid (52). In an event with a significant radioactive iodine release, therefore, KI administrations should be recommended for the duration of the release of radioactivity, with repeated doses given at 24-h intervals until the population is evacuated from the area or the releases cease. Importantly, in pregnant women, KI readily crosses the placenta and will block uptake of radioiodine by the fetal as well as the maternal thyroid and effectively reduce the potentially high doses to the fetal thyroid (53).
The International Atomic Energy Agency made available 230,000 doses of KI to Japanese officials (54), and additional KI was distributed to individuals in the vicinity of the Fukushima Daiichi nuclear facility and to emergency responders. The number and timing of KI doses actually taken by the Japanese population remain unclear. However, a survey of the thyroids of 1,080 children living in areas northwest of the plant, a region where some of the highest levels of terrestrial fallout have been seen, show minimal thyroid doses (4,55). Measurements revealed no dose rates in excess of 0.07 μSv h−1, suggesting that large intakes of 131I had not occurred in this group (21).
There were several reports of people outside the emergency protection zones in Japan and elsewhere (including the United States) who took KI in response to the radiation leaks from the Fukushima Daiichi nuclear facility although not specifically directed to do so by authorities. The World Health Organization cautioned against self-medicating with KI or with products containing iodide as a precaution against nuclear radiation (56). Several professional societies, including the Society of Nuclear Medicine, the American Association of Clinical Endocrinologists, the American Thyroid Association, and the Endocrine Society, emphasized that KI should not be taken in the absence of a clear risk of exposure to a potentially dangerous level of radioiodine (57). Appropriate use of KI is important, as KI can occasionally cause side effects such as inflammation of the salivary glands, nausea, rashes, intestinal upset, and, although rare, possible severe allergic reactions or hyperthyroidism or hypothyroidism. KI can also interact with other medications, especially certain types of cardiovascular medications such as angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and potassium-sparing diuretics. Therefore, KI administration should be reserved for specific radiation exposure situations in which the risk of radiation-induced damage to the thyroid exceeds the risk of side effects.
CONCLUDING REMARKS
The damage to the earthquake- and tsunami-stricken Fukushima Daiichi nuclear facility in Japan has resulted in fuel damage and substantial environmental releases of radioactivity—apparently far greater than those from the Three Mile Island accident but less than those from the Chernobyl accident—and exposure rates in excess of 10 μSv (1 mrem)/h generally extending to about 30 km from the facility, with some specific areas of higher exposure rates extending beyond 30 km. Although there is ongoing debate on preparedness before the event, it appears that appropriate key actions were taken by the Japanese authorities during the event to effectively mitigate the radiologic health impact. These actions include an organized evacuation of over 200,000 inhabitants from the vicinity of the site and potentially affected areas early in the emergency; monitoring of food and water and placement of radiation limits on such foodstuffs; distribution of stable KI; and scanning of over 190,000 persons (4,36). However, the risk of additional fuel damage and of further, perhaps substantial, releases persists. Even in the best-case scenario, a complete cold shut-down will likely require 6 or more months. With the infusion of corrosive sea water into the reactor core, the facility is no doubt permanently disabled, and permanent radiologic control of units 1–4 will likely take years. The situation at the Fukushima Daiichi nuclear facility thus remains fluid, and long-term environmental and health impacts (8,55) will similarly take years to fully delineate.
Footnotes
Published online Jul. 28, 2011.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the Fukushima nuclear reactor design and the multiple failures resulting from the earthquake and tsunami natural disasters; (2) the sources and types of radioactive material available and released to the environment during the early weeks of the Fukushima nuclear reactor accident and why specific public protective actions were necessary; and (3) the appropriate use of potassium iodide as a countermeasure after nuclear reactor accidents.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through September 2012.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 2, 2011.
- Accepted for publication June 22, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- FUKUSHIMA DAIICHI NUCLEAR REACTORS
- ISOTOPIC SOURCE TERMS AND POSSIBLE RELEASE MECHANISMS
- CHRONOLOGY OF THE FUKUSHIMA DAIICHI NUCLEAR FACILITY ACCIDENTS
- GUIDANCE ON EVACUATIONS AND EARLY SHORT-TERM PROTECTIVE ACTION
- LONGER-TERM PROTECTIVE ACTIONS
- THYROID RISKS AND KI
- CONCLUDING REMARKS
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics