


Abstract
The purpose of our study was to update the safety and efficacy results of radioimmunotherapy in relapsed or resistant indolent or transformed non-Hodgkin lymphoma. Methods: More than 9 y ago, we treated 12 indolent and 4 transformed, relapsed or refractory lymphoma patients with a single administration of nonmyeloablative therapy with tositumomab and 131I-tositumomab. The 16 patients had a mean of 3.1 (range, 1–6) previous chemotherapy and antibody treatments. Results: Six of 12 relapsed indolent lymphoma patients remain disease-free a mean of 9.8 y (range, 8.6–10.7 y) after radioimmunotherapy. Three of 4 transformed lymphoma patients progressed after radioimmunotherapy, and 1 patient had a partial response of 10 mo. Conclusion: Optimal patient benefit might be obtained in indolent lymphoma when administering radioimmunotherapy up-front in combination with chemotherapy and rituximab treatment. However, these results show that radioimmunotherapy alone achieved long-lasting remissions in 6 of 12 (50%) indolent lymphoma patients in relapse after 1 or multiple chemotherapies.
Advanced-stage indolent or follicular non-Hodgkin lymphoma (NHL) is considered incurable by conventional therapy. Only localized stage I or II follicular lymphoma may occasionally be cured with radiotherapy of involved sites (1). These authors stated: “patients who remain disease-free 10 years after [radiotherapy] are unlikely to relapse.”
Two commercial antibodies targeting the CD20 antigen, 131I-tositumomab and 90Y-ibritumomab, and other radiolabeled antibodies in research trials have been shown to lead to high percentages of complete remissions (CRs) (2,3) and long-lasting responses either up-front (4) or at recurrence after chemotherapy (5–9). Radioimmunotherapy is a combination of radiotherapy and antibody treatment. The use of a 131I-labeled antibody may have the clinical advantage that the low-energy electrons emitted by this radioisotope appear well adapted for treatment of minimal disease (10,11) and 131I therapy of thyroid cancer is well tolerated (12).
A high percentage of complete response was reported for 41 relapsed patients treated in England with tositumomab and 131I-tositumomab in the same protocol (5). As a second European center participating in this multicenter study, otherwise mainly conducted in the United States, we report the 10-y update from Switzerland for 16 patients who experienced a particularly high long-term efficacy of 131I-tositumomab.
MATERIALS AND METHODS
Sixteen patients (Table 1) were treated in Switzerland between August 1999 and November 2001 in the frame of this single-arm, open-label phase II study of Corixa Corp. and GlaxoSmithKline. The protocol aimed at establishing the response rate, duration of response, safety, and survival after 131I-tositumomab radioimmunotherapy in patients with indolent or transformed B-cell lymphoma after first or multiple recurrences or resistance to treatment. The study protocol was approved by the local Ethics Committees of the University Hospitals of Lausanne and Geneva, the Intercantonal Drug Control Office (later renamed Swissmedic), and the Swiss Federal Office of Public Health, Section of Radioprotection.
Characteristics of Patients with Indolent or Transformed Lymphoma at Radioimmunotherapy
Eligibility criteria were as described for patients having given written informed consent (13). The most salient criteria were an indolent, CD20-positive B-cell lymphoma confirmed by histology, in relapse or resistant after at least 1 full regimen of chemotherapy. Maximal acceptable lymphoma infiltration of bone marrow (trephine biopsy) was 25%. Patients having had high-dose chemotherapy or radiotherapy, including stem cell rescue, were excluded.
Dosimetry and Therapy
Tositumomab and 131I-tositumomab were provided by the study sponsor. Tositumomab 131I-labeling was performed centrally (MDS Nordion Inc.) and was shipped frozen. Patient preparation included thyroid blocking (2 × 100 mg of potassium iodide daily orally from 2 d before dosimetry to 14 d after radioimmunotherapy) and premedication with 500 mg of paracetamol and 2 mg of clemastine orally before antibody administration. For dosimetry, patients received 450 mg of unlabeled tositumomab followed by 35 mg of 131I-tositumomab (185 MBq). After repeated whole-body scintigraphy (14), the 131I-tositumomab therapeutic activity was calculated (14) to deliver a whole-body dose of 75 or 65 cGy for patients with normal or reduced platelet counts, respectively. Therapy, consisting of the infusion of 450 mg unlabeled tositumomab followed by 35 mg of 131I-tositumomab (2,867 ± 454 MBq), was performed within 2 wk from dosimetry.
Response and Evaluation of Side Effects
Responses were evaluated (including physical examination, CT, and bone marrow biopsy if bone marrow was involved before treatment) according to the 1999 International Working Group criteria, and evaluations were performed at weeks 13 and 26 and every 6 mo thereafter until disease progression. Progression-free survival (PFS) was defined as the time from treatment initiation to first documentation of progression or death and overall survival (OS) as the time from treatment start to death. Subjects were censored at the time of the last evaluation if they did not experience an event.
All adverse events from study entry through week 13 and adverse events after this period possibly or probably related to therapy were graded according to the National Cancer Institute Common Toxicity Criteria. Detailed blood analysis was performed weekly from study week 3 to 9 or until recovery and repeated at weeks 13 and 26 and every 6 mo thereafter. Other toxicity evaluations included blood chemistry and thyroid-stimulating hormone assays for all patients every 6 mo. The HAMA (human antimouse IgG antibody) assay (HAMA Elisa; Medac) performed for all patients had to be negative at inclusion. The HAMA assay was repeated at weeks 7, 13, and 26 after therapy and every 6 mo thereafter. Long-term evaluations after 2 y from treatment were performed every 6 mo.
Statistical Analysis
PFS and OS were analyzed using the Kaplan–Meier survival analysis, and differences among patient subgroups were tested with the log-rank test using Stata 11.1 (StataCorp). P values of less than 0.05 were considered significant.
RESULTS
Response to Radioimmunotherapy
All patients—8 with CR/unconfirmed complete response (CRu) and 4 with partial response (PR)—treated for relapsed indolent lymphoma responded. For PR patients, the duration of response was 0.5–1.4 y (Fig. 1A). Three PR patients survived 1.3–5.2 y, and 1 patient remains alive after 10 y.
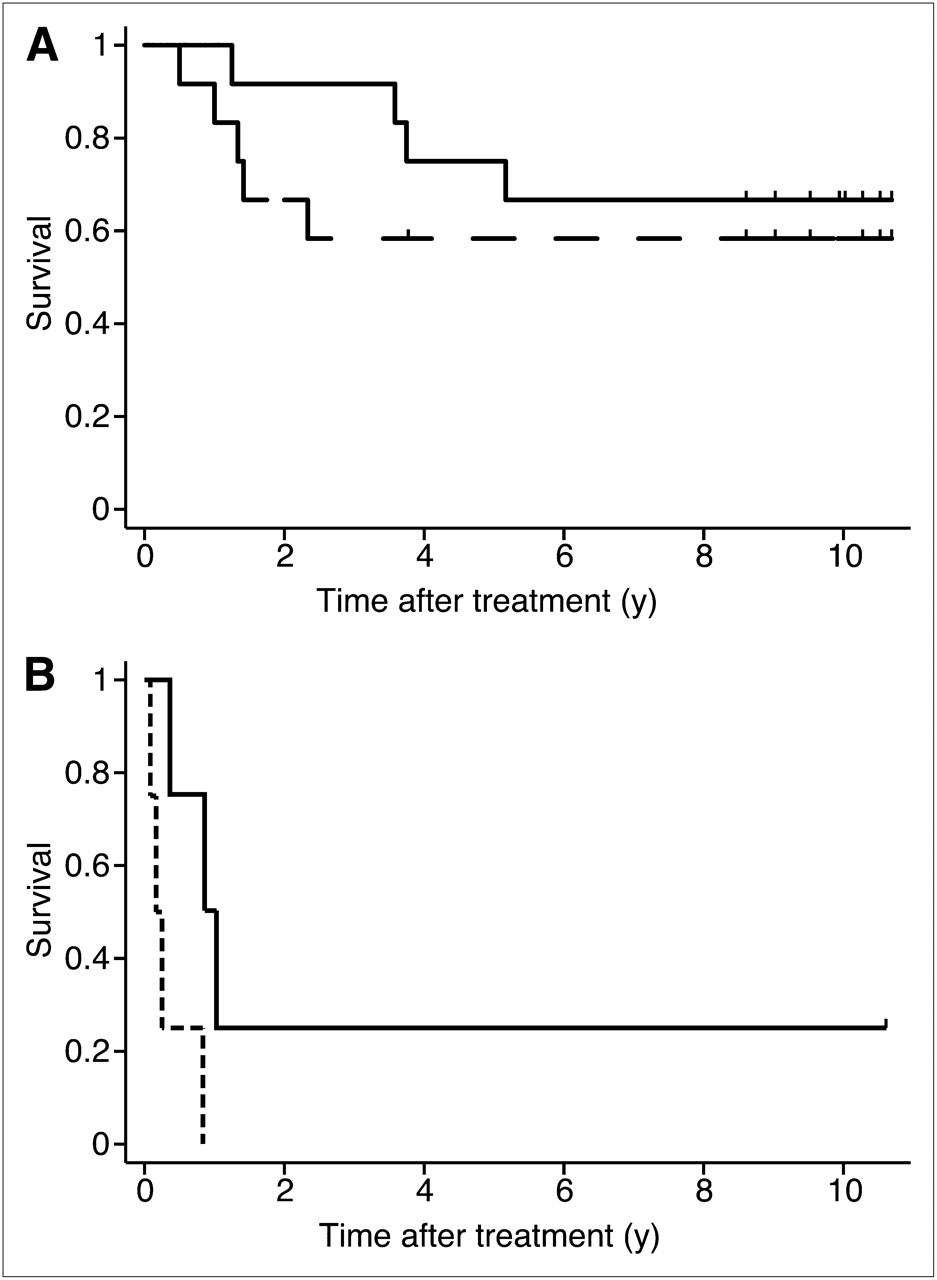
Kaplan–Meier plots in years showing OS (solid line) and PFS (dashed line) of patients who presented with relapsed indolent lymphoma (A) and 4 patients with transformed disease (B). Tics indicate censored data.
The 8 patients experiencing CR/CRu had a mean of 2.5 chemotherapy or rituximab treatments before radioimmunotherapy, 2 patients had radiotherapy, and 1 patient had interferon-α treatment (Table 1). More specifically, 7 patients (88%) had received anthracycline, 6 (75%) an alkylating agent, and 5 (63%) rituximab. Two patients (25%) had elevated lactate dehydrogenase, and 7 (88%) had bulky tumor.
One CR patient had a relapse after 28 mo, but OS has continued, lasting currently 10 y. Another CRu patient developed secondary myelodysplastic syndrome (MDS) and subsequent leukemia (acute myeloid leukemia [AML]) 2.8 y after radioimmunotherapy and 6.2 y after cyclophosphamide, hydroxydaunorubicin, Oncovin, and prednisone (CHOP). Today, 6 of 12 CR/CRu patients (50%) remain disease free, a mean of 9.8 y (range, 8.6–10.7 y) after radioimmunotherapy (Fig. 1A).
Among 4 patients with transformed lymphoma, disease progression after radioimmunotherapy was observed in 3 (Fig. 1B), whereas 1 patient responded with a PR that lasted 10 mo, OS being longer than 10.5 y.
PFS and OS differences between indolent and transformed disease were significant (P < 0.0001 and P < 0.03, respectively). Median PFS and OS for indolent lymphoma (n = 12) are 8.6 y or more and 8.8 y or more (50% events not reached), respectively, whereas for transformed disease (n = 4) they were 0.2 and 0.8 y, respectively. Given the small number of patients, these statistics must be considered cautiously.
Adverse Events
All treated patients experienced transient bone marrow depression. Bone marrow depression was grade 1 or 2 (minor) in 4 patients and grade 3 or 4 in 12 patients. Twenty-eight nonhematologic side effects, mostly mild (25 grade 1 or 2), were reported for 9 patients. These side effects included pain, fatigue, fever, chills, sweating, rash, arthralgia, erythema, and edema; 1 case of pneumonia, 1 of thyroiditis; and 1 of elevated TSH (without hormone replacement). Four patients developed HAMA. One case of febrile lymphadenitis during pancytopenia and 1 of febrile neutropenia, both grade 3, observed 7–8 wk after radioimmunotherapy, resolved rapidly after the administration of antibiotics.
One patient experienced an MDS 2.8 y after radioimmunotherapy, that is, 6.2 y after initial diagnosis and treatment with 5 cycles of CHOP. He died subsequently from leukemia.
DISCUSSION
In stage I or II follicular lymphoma treated with radiotherapy, a reduced probability of tumor recurrence was observed after 10 y of recurrence-free survival. Only 5 of 47 patients (11%) relapsed after 10 y (1). Radioimmunotherapy comprises systemic, targeted radiotherapy combined with immunotherapy. Thus, it is tempting to compare the situation of the 6 indolent lymphoma patients without recurrence 9.8 y after radioimmunotherapy with the low relapse probability that was observed after 10 y of recurrence-free survival after initial radiotherapy (1).
We observed a high percentage of long-lasting CR after radioimmunotherapy without concomitant chemotherapy or maintenance treatment. These results compare favorably with long-term observations after 131I-tositumomab treatment in the literature (9,15) and are similar to the results of combined chemotherapy and radioimmunotherapy in the initial treatment of follicular lymphoma (16). Combined up-front treatment including chemotherapy or rituximab–chemotherapy and radioimmunotherapy for consolidation (16,17) and further maintenance immunotherapy might provide optimal patient benefit. The South West Oncology Group (US) phase II trial (NCT00770224) is currently exploring this strategy. Radioimmunotherapy alone, however, was able to bring patients—even after multiple chemotherapy relapses—into particularly long-lasting CR.
One of our patients experienced MDS. As was shown by large cohort studies, the incidence of secondary MDS or AML was not increased after radioimmunotherapy, as compared with conventional therapies (3,18). Alkylating agents and doxorubicin (CHOP constituents) are, however, known to increase the risk for MDS or AML (19). Globally, an estimated 10% of treated lymphoma patients will develop secondary MDS or AML within 10 y (19).
A high efficacy of radioimmunotherapy with 90Y-ibritumomab has been reported repeatedly (3,8,17), including a report on 5-y relapse-free survival in close to 20% of patients with recurrent disease (20). However, 10-y observations after 90Y-ibritumomab radioimmunotherapy are not yet available. At our institution, one of the first patients treated has reached a current 9-y survival without objective recurrence after 90Y-ibritumomab radioimmunotherapy consolidation. Theoretically, the low-energy electrons emitted by 131I could be better adapted than the high-energy electrons of 90Y to eradicate minimal disease. Also, tositumomab is different from the chimeric antibody rituximab, the latter having been derived from the mouse antibody ibritumomab. In patients who have been or are treated with rituximab, the use of a different antibody in radioimmunotherapy could be an advantage. In the absence of a direct comparison between 90Y-ibritumomab and 131I-tositumomab, however, speculations on the advantages of one compared with the other radioimmunotherapy remain theoretic.
Our results could be the result of a favorable coincidence because we treated a small patient population. The 6 patients observed in continued CR close to 10 y after radioimmunotherapy alone, however, are remarkable. In another recent report on 60 patients, including 36 patients with relapsed or resistant low-grade lymphoma, 12 patients responded with CR and 5 remain in continued CR at 10 y or more after radioimmunotherapy (15). In a different interpretation, our small series of patients could reflect a better efficacy of 131I-tositumomab in a European subpopulation with disease characteristics different from those of U.S. patients or of patients who have had a different treatment history. The high CR rate reported for England for the same study (5) was also higher than what is generally reported for this therapy in the United States. The authors of that study reported a 53% CR/CRu rate for recurrent or resistant indolent lymphoma (5). These hypotheses cannot currently be confirmed because 131I-tositumomab has not been studied comparatively between Europe and the United States, and large patient groups overall have not yet been treated with 131I-tositumomab in Europe.
CONCLUSION
These results show a particularly high number of CR/CRu in recurrent indolent NHL. We observed exceptionally long-lasting PFS, with 6 ongoing CRs after a mean of 9.8 y after radioimmunotherapy, representing half of the indolent, relapsed lymphoma patients. Toxicity was mild or transient, except for 1 patient who developed a secondary MDS. Previous reports have shown that a significant number of indolent, relapsed NHL patients experience CR under radioimmunotherapy. Here, 6 of 12 patients treated with radioimmunotherapy alone reached a close to 10 y of relapse-free survival, and relapse probability in the next few years may expectedly be small for these patients.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We acknowledge support from the Swiss Cancer League KFS 991-02-2000. We express our gratitude to Frances Godson for reviewing the manuscript and to the referring physicians, Drs. Alfonso Zaccaria, Ravenna, Italy; Jean-Philippe Grob, Lausanne, Switzerland; Pierre Hösli, Yverdon-les-Bains, Switzerland; Christian De Pree, Geneva, Switzerland; and Christian Taverna and Alexander Knuth, Zurich, Switzerland. OWP declared an honorarium from Spectrum Pharmaceuticals.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication January 5, 2011.
- Accepted for publication February 18, 2011.





{kind=link}