


Abstract
Evaluation of nasopharyngeal carcinoma (NPC) using 18F-FDG PET/CT is limited by the intense physiologic uptake of 18F-FDG in the brain. We attempted to improve detection of intracranial tumor invasion (including better delineation of invasion near the skull base) in locally advanced NPC using11C-choline PET/CT. Methods: Fifteen patients with newly diagnosed or recurrent locally advanced NPC were enrolled in the study. 18F-FDG and 11C-choline PET/CT was performed on all patients. PET/CT images obtained using the 2 tracers were compared using both maximum standardized uptake value (SUVmax) and tumor-to-brain (T/B) ratios. All patients were followed up for more than 1 y. Results: The sensitivity of 18F-FDG PET/CT in detecting locally advanced NPC was 86.6%, compared with a 100% sensitivity for 11C-choline PET/CT (t = 2.143, P = 0.483). The SUVmax of lesions detected was higher using 18F-FDG than using 11C-choline (12.81 ± 5.00 vs. 6.84 ± 2.76, t = 6.416, P < 0.001), but the T/B ratio was much higher for 11C-choline than for 18F-FDG (18.62 ± 7.95 vs. 1.38 ± 0.59, t = 8.801, P < 0.001). Compared with 18F-FDG PET/CT, 11C-choline PET/CT improved the delineation of intracranial invasion in 6 of 12 patients (χ2 = 8.00, P = 0.014), skull base invasion in 4 of 14 patients, and orbital invasion in 3 of 3 patients. Conclusion: 11C-choline can improve the quality of PET/CT in the T staging of NPC.
Nasopharyngeal carcinoma (NPC) is a common malignancy in southern China, with intracranial as well as skull base invasion frequently seen in patients with locally advanced disease. The determination of the gross tumor volume and delineation of the extent of tumor invasion are critical for radiation treatment planning (1–3).
18F-FDG PET/CT has been shown to be more accurate than MRI for the detection of cervical nodal metastasis of NPC and to be more accurate than conventional work-up (chest radiography, liver ultrasound, skeletal scintigraphy, and CT of the thorax and abdomen) for detection of distant metastases (1,3–8). However, 18F-FDG PET/CT lacks sensitivity for T staging, especially in the delineation of skull base and intracranial invasion, because of the intense physiologic uptake of 18F-FDG in the brain (8,9). 11C-choline has been introduced as a complementary tumor imaging agent for gliomas and other brain tumors because its uptake in normal brain is minimal (10–12). In the present study, we investigated whether 11C-choline can improve the quality of PET/CT in T staging of NPC.
MATERIALS AND METHODS
Patients
The study was approved by our hospital's Institutional Review Board, and all subjects gave written informed consent before their participation in the study.
From December 2007 through May 2009, 15 patients (including 10 men and 5 women, with a mean age of 49 y [range, 36–76 y]) were enrolled in the study. Ten of the patients were newly diagnosed, and 5 had recurrent locally advanced NPC. The 15 cases of NPC, diagnosed by histopathology, included 14 cases of nonkeratinizing undifferentiated carcinoma and 1 case of well-differentiated squamous carcinoma. Intracranial and skull base invasion was diagnosed using contrast-enhanced MRI or CT combined with other clinical findings, such as the cranial nerve sign. The clinical data are listed in Table 1. All patients were treated with radical radiotherapy and chemotherapy and were followed up for a mean of 19 mo (range, 14–26 mo).
Clinical Data on NPC Patients
18F-FDG and 11C-Choline PET/CT Examination
All examinations were performed using a Discovery LS PET/CT scanner (GE Healthcare). The patients were instructed to fast for at least 6 h, and blood glucose was monitored immediately before the study to ensure a normal blood glucose level (<7 mmol/L). Approximately 60 min after the intravenous injection of 315–511 MBq (8.49–13.81 mCi, 150 μCi/kg) of 18F-FDG, whole-body PET/CT was performed, according to published guidelines for tumor imaging with 18F-FDG PET/CT (13). The patients also underwent regional PET/CT of the head and neck at approximately 10 min after the intravenous injection of 370–740 MBq (10.0–20.0 mCi) of 11C-choline during fasting. 11C-choline was produced by the method of Wilson et al. (14), and the radiochemical purity exceeded 99%.
Image acquisition using whole-body 18F-FDG PET/CT included 6–8 bed positions for each unenhanced CT and PET scan, covering the entire range from the vertex of the skull to the mid thigh using head fixation. If head movement was noted, then imaging was performed at an additional bed position covering the lesion. Image acquisition using 11C-choline PET/CT, performed on a different day, included 2 bed positions covering the head and neck. Each CT scan was performed with a scout view using 20 mA and 80 kVp, followed by a spiral CT scan with a 0.8-s rotation time, 80 mA, 140 kVp, a 5-mm section thickness, and a 4.25-mm interval in high-speed mode. After CT was completed, the scanner was returned to the landmark position and the PET scan was then acquired in the 2-dimensional acquisition mode at 4 min per 14.25-cm bed position. Among the 15 patients enrolled, a 3-dimensional acquisition brain scan was performed on 2 patients who were suspected to have intracranial recurrence but showed no abnormality on the 2-dimensional-mode 18F-FDG whole-body scan. 11C-choline PET/CT was performed using the same acquisition method as that used for the 18F-FDG PET/CT scans.
The PET images were reconstructed using a standard iterative algorithm (ordered-subset expectation maximization), with the CT data used for attenuation correction. The 2 PET/CT scans were performed on 2 different days, and all scans were completed within 1 wk. No treatment was performed during this period.
Image Analysis
The acquired PET and CT images were sent to the Xeleris workstation (GE Healthcare) for registration and fusion. The images from both 18F-FDG and 11C-choline PET/CT scans were reviewed separately on different days by 2 experienced nuclear medicine physicians, who were unaware of the results of contrast-enhanced MRI/CT. Each reviewer independently assessed each 18F-FDG and 11C-choline image. After visually examining all images on the workstation, the reviewers reached a final diagnosis based mainly on fusion images of PET and CT. Any initial difference of opinion was resolved by consensus. A lesion showing 11C-choline or 18F-FDG uptake that exceeded that of the surrounding normal tissue was considered positive. The border of each lesion was visually evaluated by comparing the radioactivity at the margin of the lesion with that of the surrounding normal tissue. If the radioactivity at the margin of the lesion was higher than that of the surrounding normal tissue, then the borders and the extent of invasion were determined. The syn-modality CT was used to determine morphologic location and degree of invasion. After separately interpreting each modality, 2 experienced nuclear medicine physicians comparatively analyzed the fused images of the 2 modalities frame by frame. The scope and border of each lesion were compared, and any discrepancy between the 2 modalities was recorded. The physiologic uptake of 18F-FDG in the ocular muscles was carefully analyzed to avoid a potential false-positive result.
For measurement of the maximum standardized uptake values (SUVmax), the region of interest was drawn along the margin of the lesion on the transverse PET image. For determination of uptake in normal brain tissue, a circular 2-cm region of interest was placed on the normal contralateral cerebellum. The tumor-to-brain (T/B) ratio was calculated by dividing the SUVmax of each lesion by that of the contralateral normal cerebellum. 11C-choline PET/CT images were selected for size measurements because they showed a clear tumor border. The longest major axis measured in any section that contained tumor was defined as the maximum diameter of the tumor.
Statistical Analysis
The SUVmax and T/B ratio were expressed as the mean ± the SD. Statistical Package for the Social Sciences, version 13.0 (SPSS Inc.), was used for statistical analysis, and the paired t test was used to compare the 2 paired samples. The rates were compared using the crosstabs χ2 test. a P value of less than 0.05 was considered statistically significant.
RESULTS
Semiquantitative Analysis of the 2 PET Studies
Ten of the 15 patients had newly diagnosed NPC, and 5 patients had recurrent NPC. 18F-FDG PET/CT was positive for tumor in all 10 newly diagnosed NPC patients and was positive in 3 of 5 cases of recurrent tumor. In 2 patients with insidious skull base involvement and intracranial recurrence, 18F-FDG PET/CT was negative. However, 11C-choline was positive in all 15 NPC patients. The sensitivity for the positive detection of tumor was 86.6% using 18F-FDG PET/CT, compared with 100% using 11C-choline PET/CT (t = 2.143, P = 0.483).
Overall uptake of radiotracer in lesions was higher for 18F-FDG than for 11C-choline (SUVmax, 12.81 ± 5.00 vs. 6.84 ± 2.76, t = 6.416, P < 0.000), but 11C-choline had a much higher T/B ratio than did 18F-FDG (18.62 ± 7.95 vs. 1.38 ± 0.59, t = 8.801, P < 0.001). This result is likely due to the lower uptake of 11C-choline than of 18F-FDG in normal brain (0.38 ± 0.09 vs. 10.01 ± 1.90, t = 19.68, P < 0.001). A significant correlation was found between the 2 tracers with regard to lesion uptake (r = 0.712, P = 0.003). In addition, there was also a significant correlation between lesion size and tracer uptake for both radiotracers (18F-FDG: r = 0.790, P < 0.001; 11C-choline: r = 0.759, P = 0.001).
Visual Evaluation of Tumor Delineation
Nasopharyngeal Invasion.
Twelve patients had lesions in the nasopharynx. Intense uptake was clearly seen in all lesions for both18F-FDG and 11C-choline, with each having a 100% positive detection rate. The borders and extent of invasion were clearly delineated by both modalities. The shape and size of the lesions were similar for both tracers (Table 2; Fig. 1).
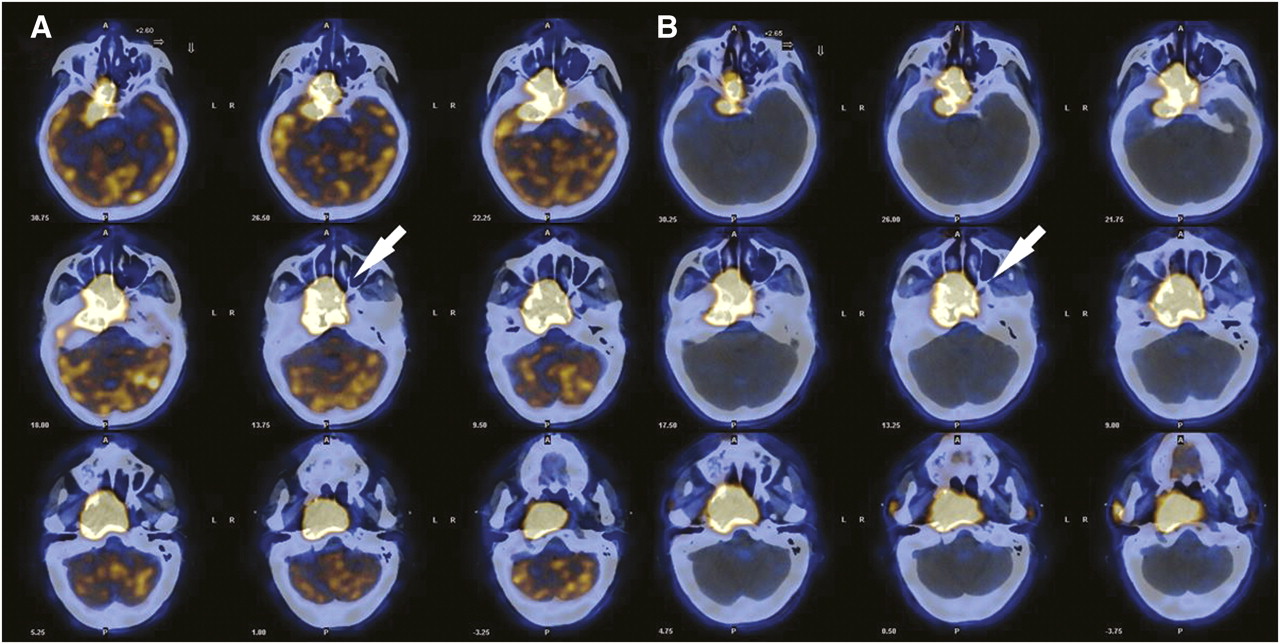
A 42-y-old woman with nonkeratinizing undifferentiated carcinoma of right nasopharynx. 18F-FDG PET/CT (A) and 11C-choline PET/CT (B) demonstrate intense uptake of both radiotracers in primary tumor (arrow), with clear and similar delineation of intracranial and skull base extension. SUVmax and T/B ratio of 18F-FDG were 17.82 and 2.48, respectively, and SUVmax and T/B ratio of 11C-choline were 6.17 and 23.7, respectively.
Visual Evaluation of Tumor Invasion Using the 2 Modalities
Skull Base Invasion.
Fourteen patients had skull base invasion. 11C-choline PET/CT and 18F-FDG PET/CT had a 100% (14/14) and 85.7% (12/14) positive rate of detection, respectively (χ2 = 2.154, P = 0.481). 11C-choline and 18F-FDG PET/CT showed a similar tumor extent and border delineation in 9 patients. However, visual findings were discordant in 5 patients. In 4 of 14 patients (28.5%), 11C-choline PET/CT showed a larger extent of tumor invasion and a clearer border with respect to skull base invasion than did 18F-FDG PET/CT (Figs. 2E and 2F). The tumor invasion primarily involved the sphenoidal sinus, foramen lacerum, clivus basilaris, and carotid foramen. In contrast, 18F-FDG PET/CT was superior to 11C-choline PET/CT in 1 patient (Table 2).
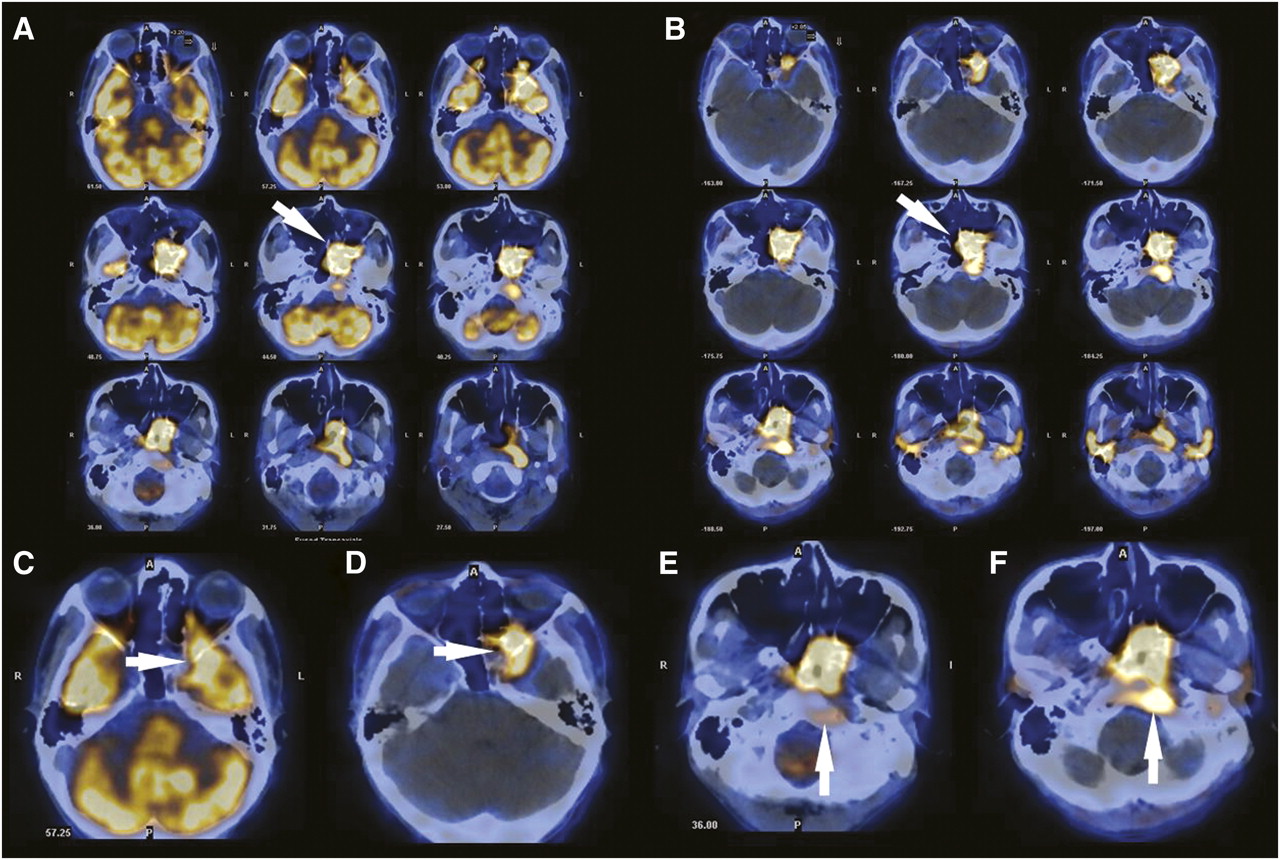
A 37-y-old man with nonkeratinizing undifferentiated carcinoma of left nasopharynx. 18F-FDG (A) and 11C-choline PET/CT (B) both demonstrate intense tracer uptake at primary site of NPC (arrow). SUVmax and T/B ratio of 18F-FDG in lesion were 11.21 and 1.05, respectively, and SUVmax and T/B ratio of 11C-choline were 7.86 and 25.3, respectively. Both modalities demonstrate invasion of nasopharynx, parapharyngeal region, skull base, and left temporal lobe. 11C-choline PET/CT (D) shows clearer border of invasion of left orbit and left temporal lobe (arrow) than does 18F-FDG PET/CT (C). Extent of clivus basilaris invasion (arrow) is also clearer and larger with 11C-choline PET/CT (F) than with 18F-FDG PET/CT (E).
Intracranial Invasion.
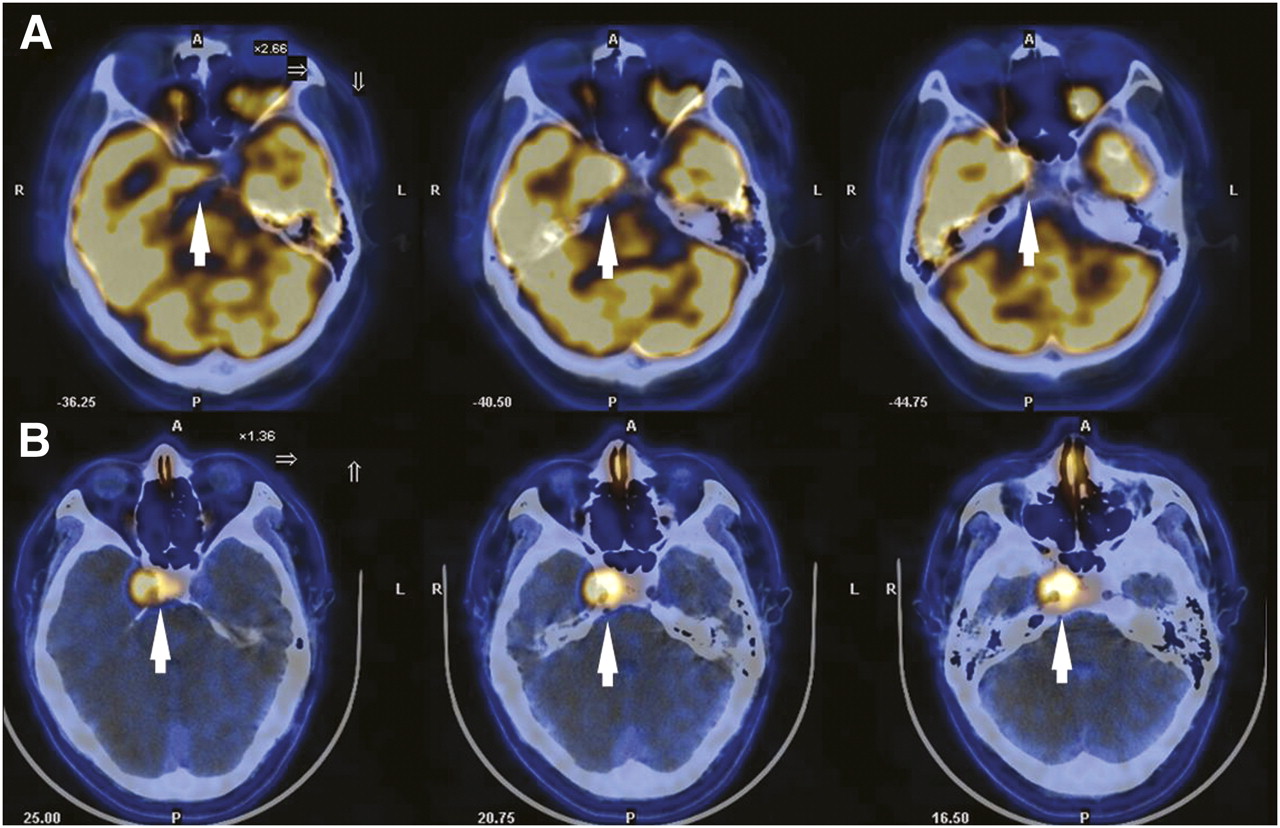
Twelve patients were known to have intracranial invasion. Intracranial invasion was detected in 100% of patients using 11C-choline and in 83.3% of patients using 18F-FDG PET/CT (χ2 = 1.104, P = 1.000). In 2 patients with insidious intracranial recurrent tumor, 18F-FDG PET/CT was negative. The extent of intracranial invasion was clearly delineated by 11C-choline PET/CT (Figs. 2 and 3) in all 12 patients and by 18F-FDG PET/CT in only 6 patients. Thus, 11C-choline PET/CT improved the visual determination of intracranial invasion in 50% (6/12) of patients (χ2 = 8.00, P = 0.014).

A 36-y-old man with recurrent NPC of right nasopharynx. 18F-FDG PET/CT (A) shows increased uptake of 18F-FDG in skull base and adjacent right temporal lobe (arrow, SUVmax = 13.66), with unclear border (T/B ratio = 1.04). Uptake of 11C-choline in skull base and left temporal lobe is intense (arrow, SUVmax = 6.00). Clearer border of intracranial invasion is seen with 11C-choline PET/CT (B) (T/B ratio = 10.71) than with 18F-FDG PET/CT.
DISCUSSION
Several articles have shown that 18F-FDG PET/CT plays an important role in the diagnosis and staging of NPC. 18F-FDG PET/CT was reported to be superior to MRI and conventional work-up (chest radiography, liver ultrasound, skeletal scintigraphy, and CT of the thorax and abdomen) for the detection of cervical lymph node metastasis and distant metastasis (4–8). 18F-FDG PET/CT was also reported to have a positive impact on radiotherapy planning and patient management (15–17). But for the T staging of locally advanced NPC, the studies of Ng et al. and King et al. have indicated that 18F-FDG PET/CT may underestimate the presence or extent of tumor invasion in the parapharyngeal space, skull base, intracranial area, sphenoid sinus, and retropharyngeal nodes, when compared with MRI (8,9).
Our results confirmed that 18F-FDG PET/CT is limited with regard to T staging for locally advanced NPC. 18F-FDG PET/CT underestimated invasion of the skull base, intracranial compartment, and orbit in 4 of 14, 6 of 12, and 3 of 3 patients, respectively, when compared with 11C-choline PET/CT. This discrepancy is likely due to the higher physiologic uptake of 18F-FDG in normal brain, which makes intracalvarial lesions or lesions near the skull base difficult to detect on 18F-FDG PET/CT. In addition, high physiologic uptake of 18F-FDG in the ocular muscles may also obscure orbital invasion.
Radiolabeled choline is a novel PET agent for tumor imaging. Radioactive choline can rapidly incorporate into tumor cells and then through phosphorylation become phosphorylcholine and finally integrate into a phospholipid—that is, phosphatidylcholine (18,19). High uptake of radioactive choline has been confirmed in many types of tumors, such as prostate carcinoma, brain tumors, hepatocellular carcinoma, and bone and soft-tissue sarcoma (20–29). To our knowledge, however, no one has evaluated the use of 11C-choline PET/CT for the diagnosis of NPC. In addition, uptake of 11C-choline in the normal brain was reported to be quite low, suggesting that 11C-choline PET/CT may be helpful for T staging of NPC, especially for the detection and delineation of intracranial invasion.
The present study demonstrated avid uptake of 11C-choline by NPC. The SUVmax of 11C-choline also correlated positively with NPC lesion size (P = 0.001). With a low level of background radioactivity in normal brain tissue, 11C-choline PET/CT had a much higher T/B ratio than did 18F-FDG PET/CT. As a result, 11C-choline PET/CT improved the detection of insidious intracranial recurrence in 2 patients and the visual delineation of skull base, intracranial, and orbital invasion in 4 of 14, 6 of 12, and 3 of 3 patients, respectively. This finding suggests that 11C-choline PET/CT may be superior to 18F-FDG PET/CT for determining gross tumor volume in patients with locally advanced NPC.
Although imaging plays an important role in NPC for both determining gross tumor volume and T staging, unfortunately, pathologic and radiologic findings cannot usually be correlated because few patients undergo surgical resection. Thus, evidence from the literature is scanty. MRI is known to be a highly sensitive technique for identifying tumor invasion and is currently the standard modality for T staging of NPC. However, MRI has problems with specificity that can lead, in some cases, to results that are positive due to edema and inflammation rather than to tumor infiltration (30). Daisne et al. reported that tumor volume in pharyngolaryngeal squamous cell carcinoma, as determined by 18F-FDG PET, was found to be more accurate than CT and MRI determinations, particularly when the volume was compared with the actual surgical specimen (31). If 11C-choline PET/CT were proven more accurate than MRI for tumor delineation, then 11C-choline PET/CT could play an important role in gross tumor volume determination, thus improving radiation treatment outcome. Future research should be undertaken to determine which technique is more accurate for tumor delineation and whether a complementary role exists between 11C-choline PET/CT and MRI. In addition, our study was limited by our relatively small and heterogeneous patient population. Future randomized, controlled studies, using a larger patient population, are needed to confirm our findings.
It has been reported that 11C-choline can also be taken up by the choroid plexus, the lateral ventricles, the plexus venosus caroticus internus, and the pituitary body, potentially limiting the detection of tumors such as glioma (11). In the present study, we found that this physiologic uptake had no influence on T staging of NPC because most of the tumors we studied were remote from all these structures except for the pituitary body. But because the uptake of 11C-choline was lower in the pituitary body than in tumor, the influence of 11C-choline PET/CT on T staging of NPC in our patients was also limited.
CONCLUSION
The present study has demonstrated that 11C-choline is avidly taken up by NPC. Because of its low background radioactivity in normal brain tissue, 11C-choline PET/CT had a higher T/B ratio than did 18F-FDG PET/CT, thus improving detection of intracranial, skull base, and orbital invasion. These findings suggest that 11C-choline PET/CT may be a useful modality for T staging of NPC in conjunction with 18F-FDG PET/CT.
Acknowledgments
We thank our colleagues in the Department of Radiotherapy, Nanfang Hospital, who provided the follow-up data.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication July 12, 2010.
- Accepted for publication December 1, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.