


Abstract
We hypothesized that 68Ga-DOTATATE uptake of neuroendocrine tumors is sensitive to therapy with a nonradioactive somatostatin analog. Methods: 68Ga-DOTATATE PET/CT was used to examine 105 patients, 35 of whom had been pretreated with long-acting octreotide. The maximum standardized uptake value (SUVmax) of target tissues, as well as metastases, was compared between the groups of patients with (group 1) and without (group 2) octreotide treatment. Results: The SUVmax of the spleen and liver was significantly lower in group 1 than in group 2 (both P < 0.001). There were no significant group differences in SUVmax for primary tumors (28.6 ± 6.8 vs. 32.9 ± 31.5) or metastases in the liver (27.2 ± 14.8 vs. 25.7 ± 10.7), lymph nodes (41.4 ± 19.5 vs. 25.0 ± 6.3), or skeleton (39.5 ± 22.0 vs. 15.4 ± 7.8). In 9 patients available for intraindividual comparison, tumor uptake was unaffected by treatment with somatostatin analogs (21.7 vs. 20.6; P = 0.93). Conclusion: Treatment with a long-acting somatostatin analog did not significantly reduce 68Ga-DOTATATE binding in neuroendocrine tumors but tended to improve the tumor-to-background ratio.
PET using 68Ga-labeled somatostatin analogs such as 68Ga-DOTATATE is increasingly applied for the diagnosis of neuroendocrine tumors (NETs). 68Ga-labeled somatostatin analogs are diagnostically more sensitive than 18F-3,4-dihydroxyphenylalanine (1), more accurate than conventional somatostatin receptor (SSTR) scintigraphy (2), useful in response assessment (3), and of considerable prognostic value in therapy monitoring (4). For all these reasons, PET with somatostatin analogs is now recommended by recent guidelines for the detection of NET (5), and procedure guidelines were recently published (6).
Medical treatment with unlabeled somatostatin analogs such as octreotide is an accepted option in symptomatic NET patients and has proven to delay the time to tumor progression in functionally active midgut NET (7). Like the PET tracer 68Ga-DOTATATE, octreotide binds to SSTR subtype 2, where it acts as an agonist. This common molecular target of the medication and the tracer could reduce the specific PET signal by simple competition or by evoking internalization of SSTR subtype 2 receptors, as is seen after treatment with octreotide in vitro (8–11). An additional potential confounding factor is suggested by the observation that SSTR expression was induced by incubation of pituitary cells in culture with a somatostatin analog (12). Indeed, scintigraphy with 111In-pentetreotide (OctreoScan; Covidien) has revealed some positive effects of octreotide pretreatment on tumor-to-background ratios in NET patients (13), but there are no corresponding reports using 68Ga-labeled somatostatin analogs.
Because of these partly conflicting results, it is generally recommended that treatment with long-acting somatostatin analogs be interrupted before SSTR imaging is performed (14), even if the treatment of proven antiproliferative effects has to be withdrawn before the diagnostic scan at the risk of causing discomfort and complications to patients by attenuating the inhibition of hormonal hypersecretion. To assess the extent of the potential confounding factors, we aimed in the present study to compare the 68Ga-DOTATATE PET standardized uptake values (SUVs) of different tumor sites and healthy organs in groups of patients with or without octreotide treatment at the time of scanning.
MATERIALS AND METHODS
Study Population
A total of 105 patients (50 women and 55 men; mean age ± SD, 58 ± 12 y; range, 20–81 y) with histologically proven well- to intermediately differentiated NET were investigated with 68Ga-DOTATATE PET/CT. Primary sites of the NET are shown in Table 1. Thirty-six of the 105 patients had no evidence of residual tumor or metastases.
Demographics and Tumor Sites for Treated and Untreated Patients
Patients were divided into 2 groups according to their treatment status with respect to somatostatin analogs, which was derived from patients’ charts and verified by telephone interviews with the patients. Group 1 consisted of 35 patients (all with metastases) under treatment with long-acting octreotide (Sandostatin LAR [Novartis] every 4 wk) at the time of the PET/CT investigation. Of these 35 patients, 33 had been treated with a dosage of 30 mg, 1 patient with 20 mg, and 1 with 50 mg. The mean interval between previous long-acting octreotide application and PET/CT was 14.5 ± 11.4 d. Group 2 consisted of 70 patients without a history of octreotide treatment. If patients underwent subsequent PET/CT scans, only the first investigation was included.
In a substudy, intraindividual comparison was performed in the 9 patients (3 women and 6 men, mean age, 60.6 ± 7.6 y) who had successive PET scans with and without long-acting octreotide treatment within a mean interval of 13.8 ± 15.6 wk. For these analyses, up to 5 metastases per organ and patient (in total, 42 lesions) were compared between the 2 scans.
PET/CT Scans
Written, informed consent was obtained from all patients before the examinations. 68Ga-DOTATATE was labeled as described elsewhere (15). Whole-body PET scans were acquired in 3-dimensional mode (3-min recordings per bed position) using a Gemini PET/CT scanner (Philips) 60 min after intravenous injection of 200 MBq of 68Ga-DOTATATE, corresponding to 36 ± 3 μg of DOTATATE (15). A diagnostic whole-body CT scan was obtained for all patients.
PET Image Evaluation
Images were analyzed using a dedicated software package (Hybrid Viewer; Hermes Medical Solutions). Maximum SUV (SUVmax) and mean SUV (SUVmean), with correction for body weight, were calculated for the liver, spleen, kidneys, adrenal glands, and pituitary gland, as well as the primary tumor and the most intense metastases of the liver, lymph nodes, bone, and lung (Fig. 1). In organs presenting metastases, at least 4 regions of interest were manually drawn, distal to all evident metastases, except for 9 cases with disseminated metastatic spread in the liver. SUV measurements were recorded only for those metastases with a diameter greater than 10 mm on CT, so as to minimize partial-volume effects. For each organ, the metastasis with the highest SUVmax was considered.

Axial views and multiple-intensity projections of 2 PET/CT scans from same patient: scan under treatment with long-acting octreotide (A) and scan without treatment (B). Although SUVmax of metastases was not different (32.9 and 31.6 with and without treatment, respectively), uptake of both spleen (20.2 and 25.3, respectively) and liver (9.5 and 11.5, respectively) was notably lower under long-acting octreotide treatment. Between the 2 examinations, no disease progression was evident and no treatment was performed.
Statistical Analysis
Statistical analyses were performed using the SPSS software package (version 15.0; SPSS, Inc.). The Friedman test (differences in SUVmax and SUVmean between the different organs and tumor sites), Mann–Whitney U test (differences in SUVs between the 2 treatment groups), Kruskal–Wallis test (SUVs of the 6 groups assigned by the site of the primary tumor), and Wilcoxon test (for intraindividual comparison) were used. All tests were 2-tailed, and P values of less than 0.05 were assumed to be statistically significant. All quantitative data are presented as mean ± SD.
RESULTS
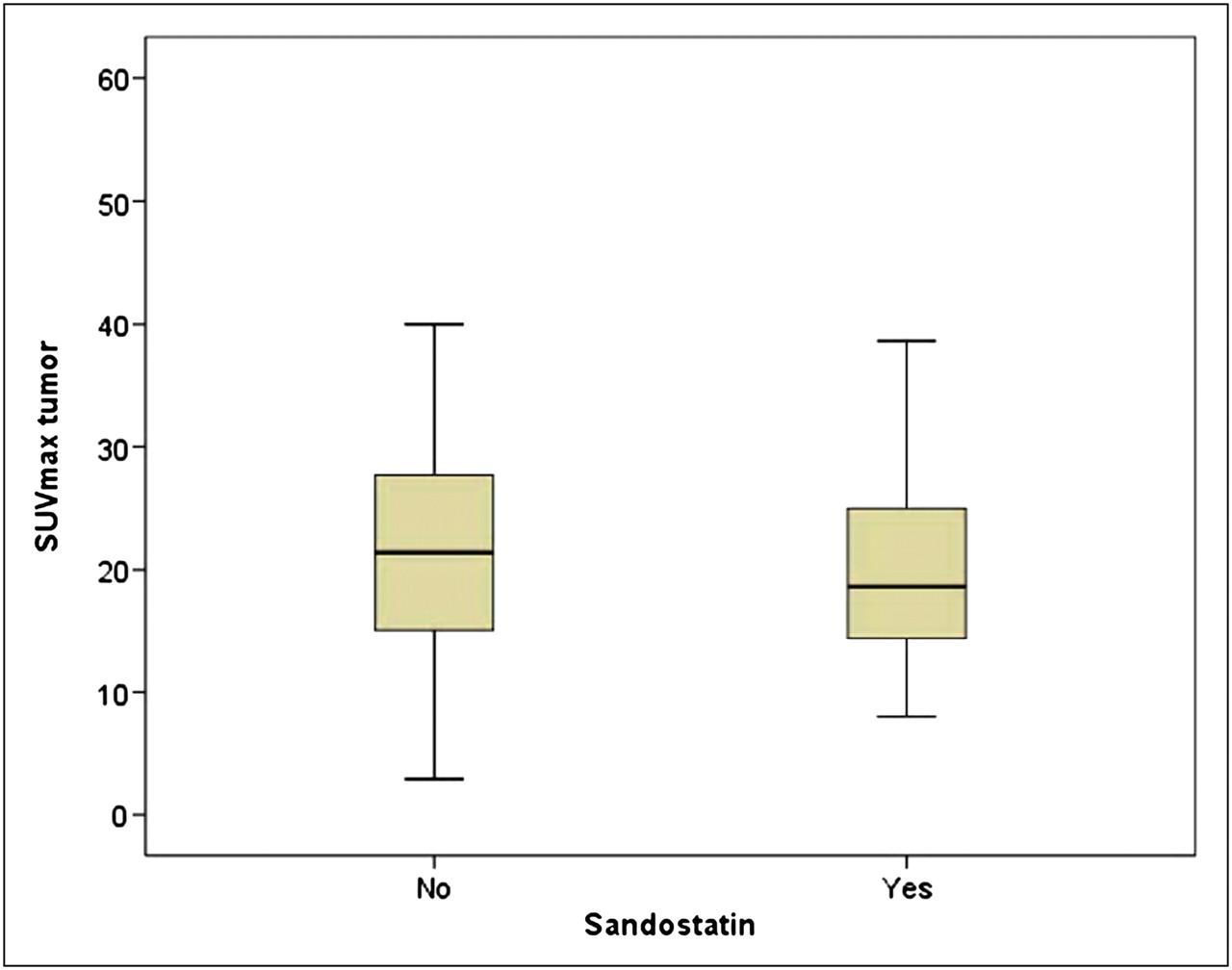
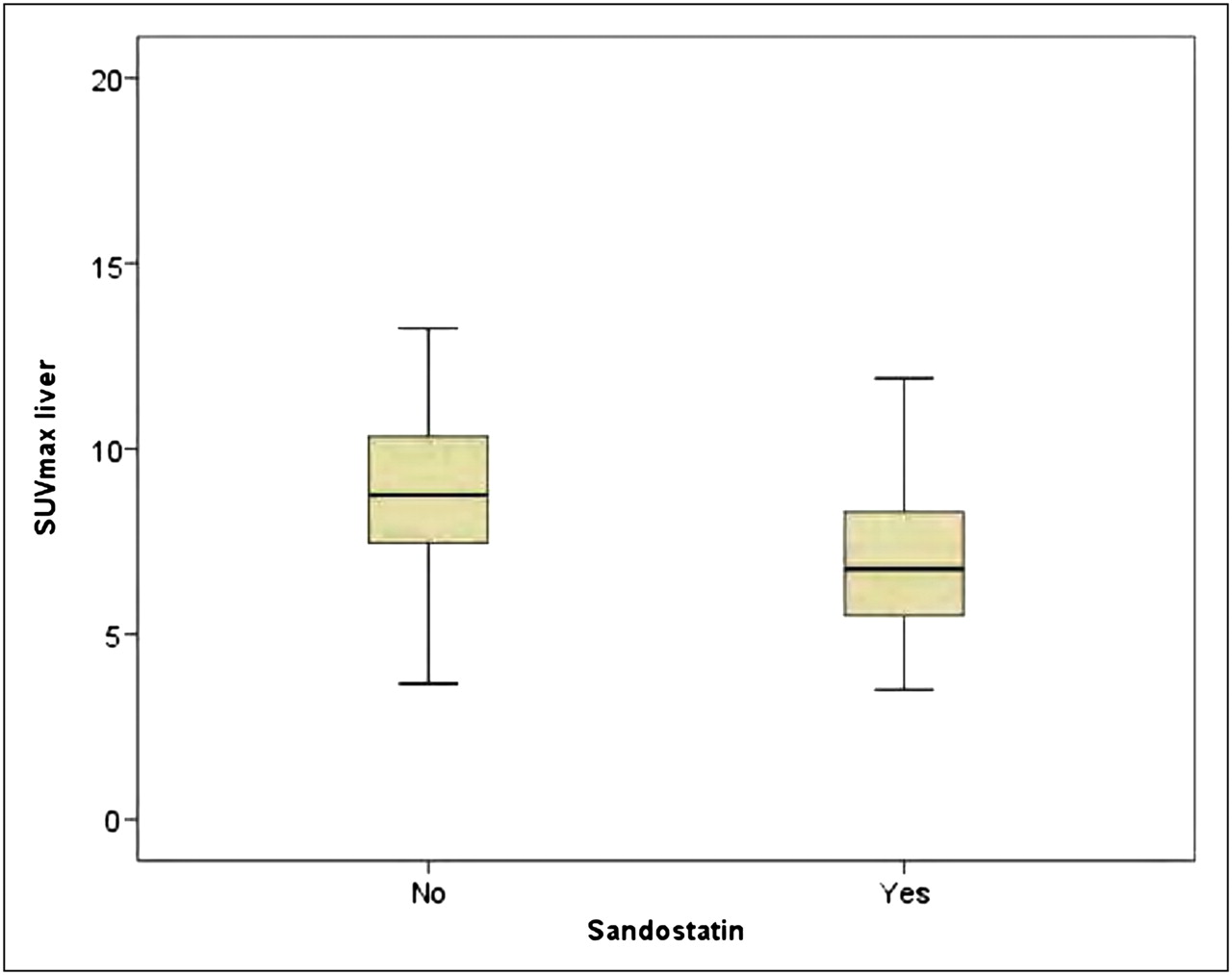
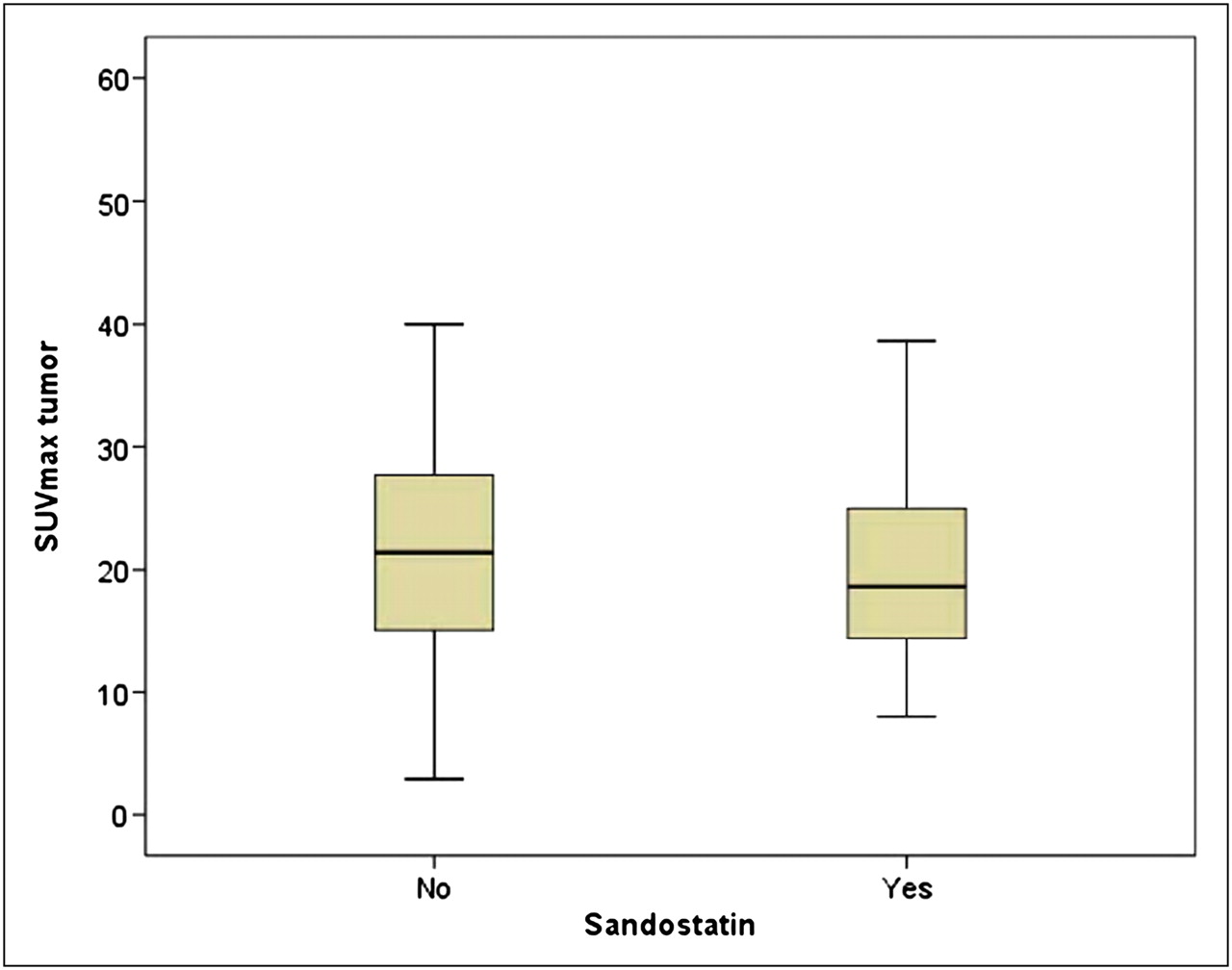
There were no significant differences in sex, age, and primary tumor location between the patient groups with and without octreotide treatment (Table 1). The proportion of patients with tumor metastases was significantly higher in the octreotide group than in the group without octreotide treatment (35/35 vs. 34/75; P < 0.001). However, neither the mean SUVmax nor the mean SUVmean of the primary tumor and the metastases differed significantly between the 2 groups (Table 2; Fig. 2). Nonetheless, the patient group under octreotide treatment presented with a lower average SUVmax and SUVmean for the spleen (P < 0.001) and the liver (P < 0.001; Fig. 3) than the nontreated patients, whereas uptake in the kidneys, pituitary gland, and adrenal gland did not differ (Table 2).
SUVmax and SUVmean of Organs, Primary Tumors, and Metastases in Treated and Untreated Patients

SUVmax measurements of tumor with highest value per patient. Mann–Whitney U test revealed no difference between groups with and without octreotide medication (P = 0.70).

SUVmax measurements of liver. Mann–Whitney U test revealed significantly lower SUVmax in group with octreotide treatment than in group without (P < 0.001).
Among the patients under octreotide treatment, those who had received an injection fewer than 14 d (n = 12) before the PET/CT scan did not present with lower SUVs in the healthy organs (liver, spleen, kidney, adrenal glands, or pituitary gland) than the subgroup that had received octreotide more than 14 d (n = 7) before the scan. The SUVmax of the most intense metastases per patient tended to be higher in the group with the longer interval between long-acting octreotide application and PET scan (45.3 ± 13.5 vs. 35.2 ± 14.2), although the difference was not statistically significant (P = 0.73). As only 1 patient of these 2 groups had a primary tumor, no comparison by tumor type was possible. No tumors were visible on CT, which lacked 68Ga-DOTATATE uptake in the patient group treated with long-acting octreotide.
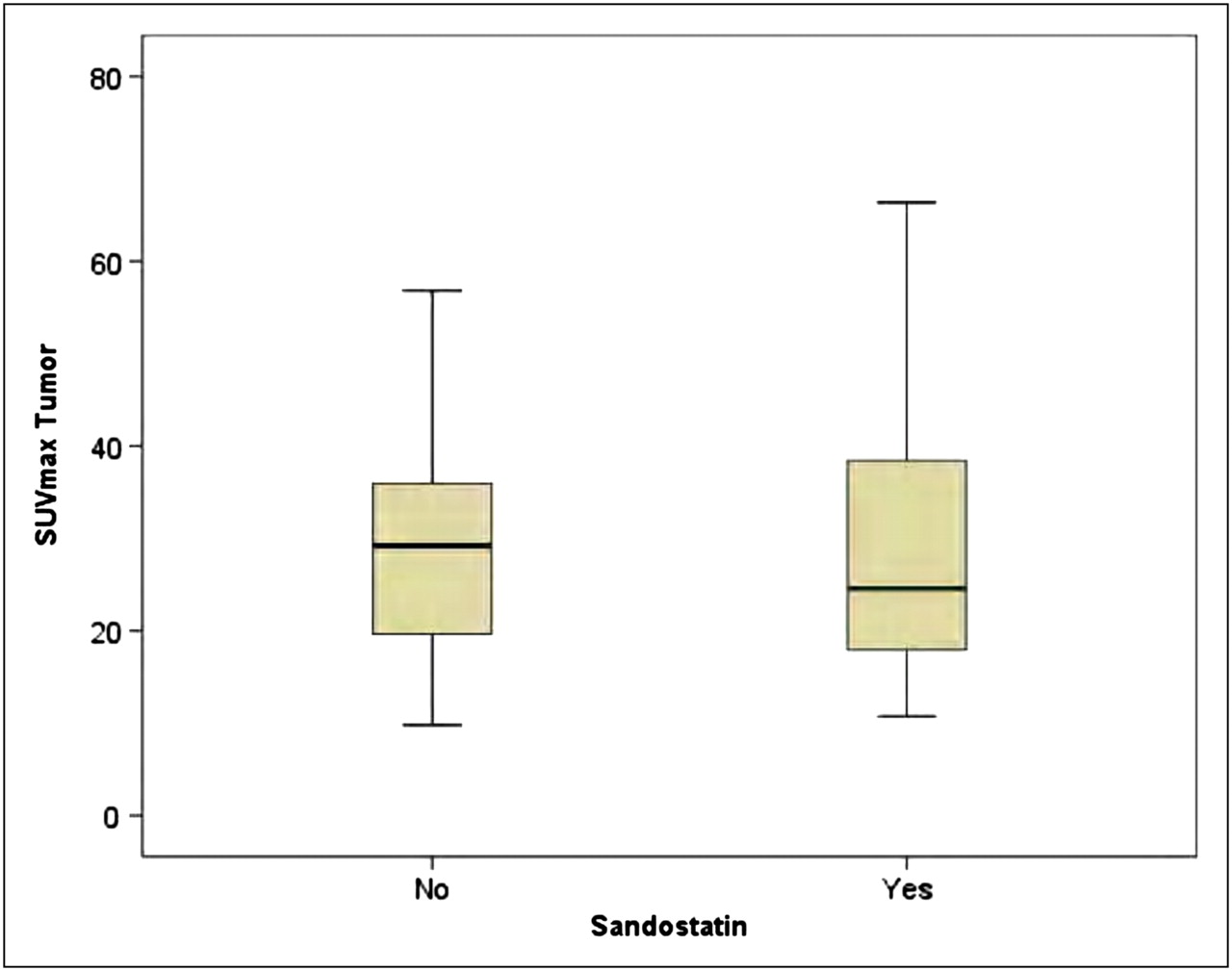
In the intraindividual comparison of 9 patients with follow-up PET/CT, liver uptake was significantly reduced on octreotide treatment (7.1 vs. 9.2; P < 0.05), whereas differences in uptake by the spleen (21.7 vs. 23.3; P = 0.58), kidneys (16.5 vs. 16.0; P = 0.95), adrenal glands (17.8 vs. 16.9; P = 0.48) and metastases (21.7 vs. 20.6; P = 0.93) were not significant (Fig. 4).
SUVmax measurements of up to 5 tumors per organ and patient in subgroup of 9 patients with successive PET scans with and without octreotide medication. Wilcoxon test revealed no statistical difference (P = 0.93).
DISCUSSION
The main finding of the present study was a significantly lower 68Ga-DOTATATE uptake by nontumorous spleen and liver in patients treated with somatostatin analogs. There were, however, no significant group differences in 68Ga-DOTATATE in tumors, and 68Ga-DOTATATE uptake showed no discernible time dependence on the interval since octreotide treatment. Detailed analysis of the small group of patients available for intraindividual comparison confirmed the finding of unaffected tumor uptake in the presence of significantly lower hepatic uptake on treatment.
In brief, high uptake of 68Ga-DOTATATE in NET was previously reported by Reubi et al. in patients treated with the SSTR subtype 2 agonist [Tyr3, Thr8]octreotide, based on SSTR autoradiography of resected tumors, indicating high SSTR expression despite octreotide medication (16). This finding was seen despite the concurrent observation of a variable rate of internalization of the SSTR. The dissociation between receptor expression and internalization might be explained by another animal study, in which octreotide medication induced rapid SSTR subtype 2 internalization within 2.5 min in vivo, followed by recovery of receptor expression within 24 h (17). With the long-acting octreotide, the serum concentration remains quite stable over 28 d (18), as might be expected to result in concomitant receptor internalization and overexpression. This stability, however, need not also hold true for other somatostatin analogs such as lanreotide, for which the serum concentration decreases over time (18).
The present finding of a greater tumor-to-background ratio for hepatic tumors in patients treated with octreotide agrees with the results of previous studies using conventional SSTR scintigraphy for the diagnosis of NET (13,19). Together, these findings provide increasing evidence that treatment with somatostatin analogs not only does not hamper but even may facilitate the diagnosis and detection of NET, although the mechanism by which this improvement is obtained is obscure. Because of the heterogeneity of NETs and their differing biologic behaviors, it remains uncertain if these findings can be generalized to all types of this tumor. In an earlier study, Dörr et al. (13) described in 5 patients improved visualization of carcinoid liver metastases by 111In-pentreotide after treatment with a somatostatin analog. In a study of 8 patients, Janson et al. (19) performed an intraindividual comparison of 111In-octreotide scans before and after 12 mo of treatment with high-dose lanreotide; the tumor-to-background ratio increased by an average of 50%, but the increase extended over a considerable range (−79% to 1,087%). Interpretation of this result is subject to the caveat that during 12 mo of follow-up, tumor progression itself may have increased the uptake values. The superior quantitation with SUV calculations afforded by the present PET/CT study, as compared with earlier SPECT studies, suggests that the consistent findings of a greater target-to-background ratio in patients treated with somatostatin analogs are driven by a decline in background binding rather than an increase in tumor binding. Given the finding of agonist-induced upregulation of SSTR in vitro (12), we speculate that the binding site density may likewise have been increased in the tumors and metastases of patients treated with octreotide, whereas the net effect on 68Ga-DOTATATE binding was masked because of partial occupancy of the receptors by the medication. Summing up, the treatment effects may lead to improved tumor delineation, especially in the liver, because of a higher tumor-to-nontumor ratio.
Despite the relatively large number of patients included in the present study for interindividual comparison, a still larger number of patients would have further strengthened our conclusions. However, even in such a setting, parameters such as plasma clearance and receptor expression of organs and tumors are hard to control and would likely have influenced the SUV of 68Ga-DOTATATE between the 2 examinations.
CONCLUSION
Treatment with a long-acting somatostatin analog does not reduce 68Ga-DOTATATE binding in the target tumor in any organ, as opposed to binding in the nontumorous spleen and liver, where a significant reduction (and thus improved signal-to-background ratio) was observed. This finding may support the approach of not interrupting octreotide medication before the PET/CT scan. Further studies including a larger number of intraindividual comparisons would be desirable for confirmation of this finding.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 5, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication March 2, 2011.
- Accepted for publication August 1, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Prospective Observational Study to Evaluate the Effects of Long-Acting Somatostatin Analogs on 68Ga-DOTATATE Uptake in Patients with Neuroendocrine Tumors
- Long-Acting Somatostatin Analog Therapy Differentially Alters 68Ga-DOTATATE Uptake in Normal Tissues Compared with Primary Tumors and Metastatic Lesions
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites
- Impact of 68Ga-DOTATATE PET/CT on the Management of Neuroendocrine Tumors: The Referring Physician's Perspective
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification
- Free Somatostatin Receptor Fraction Predicts the Antiproliferative Effect of Octreotide in a Neuroendocrine Tumor Model: Implications for Dose Optimization
- Neuroendocrine tumor disease: an evolving landscape