


Abstract
The dopamine transporter (DAT) is a transmembrane protein responsible for reuptake of dopamine from the synaptic cleft and termination of dopaminergic transmission. Several radioligands are available for DAT imaging with SPECT and PET. This review summarizes the main SPECT and PET radioligands and the main applications of DAT imaging in neuropsychiatric disorders.
The neurotransmitter dopamine is one of the main monoamine transmitters in the brain and is involved in the regulation of important brain functions such as locomotor activity, reward, and cognition. The dopamine transporter (DAT) is a plasma membrane protein expressed exclusively in dopamine neurons, where it acts by rapidly clearing dopamine released into the extracellular space, thus regulating the amplitude and duration of dopamine signaling (1). In mammalian brain, the DAT protein is distributed mainly in the mesencephalic dopamine neurons of the substantia nigra pars compacta and of the ventral tegmental area and is particularly enriched in the striatum and nucleus accumbens.
Radioligands for In Vivo Imaging of DAT
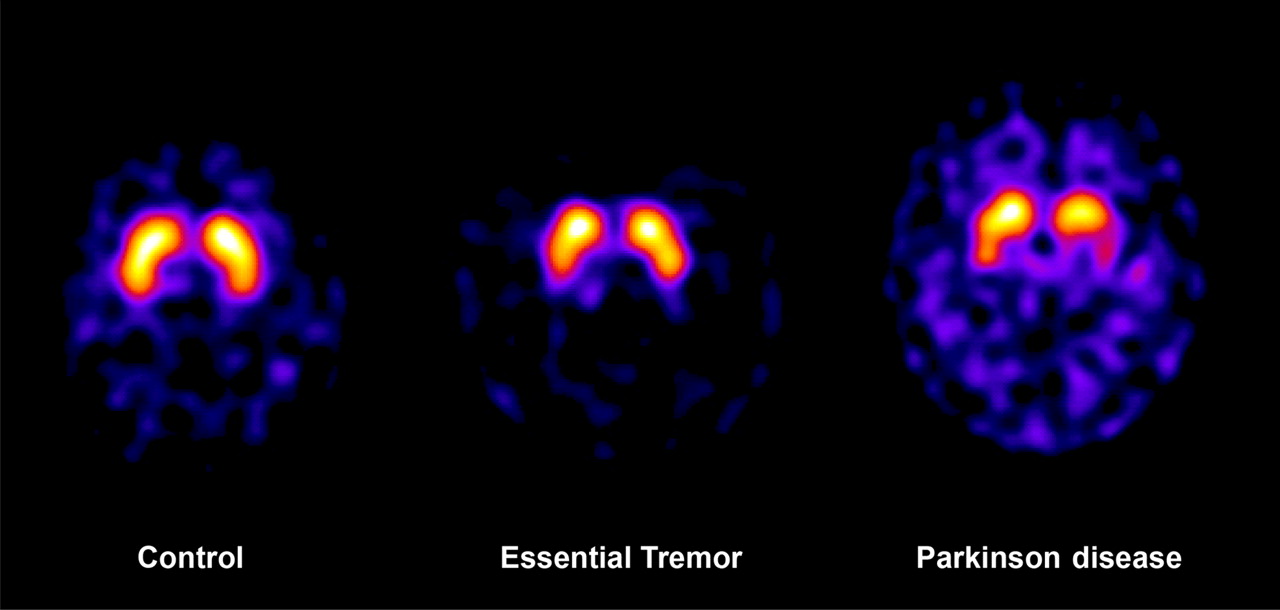
Several SPECT and PET radioligands for DAT are available. SPECT radioligands such as 123I-N-3-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane (123I-FP-CIT, also referred to as 123I-β-CIT-FP, 123I-ioflupane, and DaTSCAN [GE Healthcare]) and 123I-2β-carbomethoxy-3β-(4-iodophenyl)tropane (123I-β-CIT, also referred to as DOPASCAN [MAP Medical Techologies]) are commercially available. 123I-FP-CIT is widely used in Europe, and its approved indications are differential diagnosis between essential tremor and degenerative parkinsonism (Fig. 1) and differential diagnosis between dementia with Lewy bodies (DLB) and Alzheimer disease (AD) (2). 123I-β-CIT is one of the DAT tracers most frequently used. Other 123I-labeled DAT radioligands used in some imaging centers include 123I-2β-carbomethoxy-3β-(4-fluorophenyl)-N-(1-iodoprop-1-en-3-yl)nortropane (123IACFT, or 123I-Altropane [Alseres Pharmaceuticals, Inc.]), 123I-N-(3-iodopropen-2-yl)-2β-carbomethoxy-3β-(4-chlorophenyl)tropane (123I-IPT), and 123I-labeled N-(3-iodoprop-(2E)-enyl)-2β-carboxymethoxy-3β-(4-methylphenyl)nortropane (123I-PE2I). Among other SPECT radioligands, 99mTc-TRODAT-1 (99mTc-[2-[[2-[[[3-(4-chlorophenyl)-8-methyl-8-azabicyclo[3.2 0.1]oct-2-yl]methyl](2-mercaptoethyl)amino]ethyl]amino]ethanethiolato(3-)-N2,N2′,S2,S2′]oxo-[1R-(exo-exo)]) is the only available technetium-labeled radioligand and has drawn interest because of its potential for routine clinical use. However, despite the advantageous imaging properties of technetium, the target-to-background ratio is lower for 99mTc-TRODAT-1 than for other 123I-labeled radioligands, and the tracer might be less suitable for the follow-up of parkinsonian patients in whom there is a higher degree of specific signal loss in the striatum.
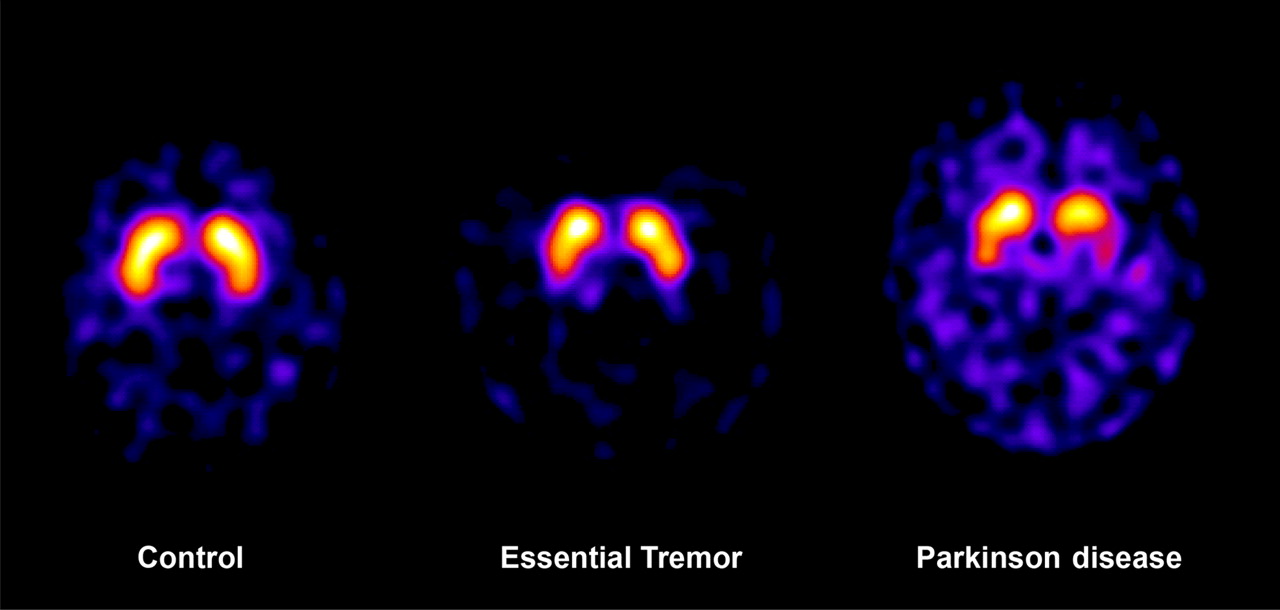
DAT SPECT with 123I-FP-CIT shows normal striatal DAT availability in patient with essential tremor, whereas asymmetric DAT loss is found in patient with PD. SPECT images were acquired at Biostructure and Bioimaging Institute, Naples, Italy.
The wider availability of PET and PET/CT systems could be an important motivation for the development of new PET radioligands for DAT. Radioligands labeled with 11C and applied in human studies include 11C-PE2I (3), 2β-carbomethoxy-3-β-(4-fluorophenyl)tropane (11C-β-CFT, also referred to as 11C-WIN 35,428), 11C-β-CIT, and N-(2-fluoroethyl)-2β-carbomethoxy-3β-(4-iodophenyl)nortropane (11C-β-CIT-FE) (4). Two properties of PET radioligands for DAT are desirable. The tracer should have high affinity and selectivity for DAT, yielding a high in vivo target-to-background ratio and also providing the opportunity to visualize DAT in the midbrain (Fig. 2). This property is of particular interest in Parkinson disease (PD), because the midbrain is the site at which the cell bodies of the dopamine neurons are located and the primary site of PD pathology.

DAT PET with 11C-PE2I in healthy control. Image was acquired on ECAT EXACT HR system (Siemens). Not only striatum but also midbrain can be visualized.
The other desirable property for new PET radioligands for DAT is labeling with 18F. 18F-labeled radioligands can be interesting for at least 2 reasons: the lower energy of the positron provides higher intrinsic resolution, resulting in better imaging quality, and labeling with 18F allows for distribution to centers without a cyclotron, resulting in widespread clinical application. Several 18F-labeled DAT radioligands have been reported, but only some have been applied to humans: 18F-β-CFT, 18F-2β-carbomethoxy-3β-(4-chlorophenyl)-8-(2-fluoroethyl)nortropane (18F-FECNT), and 18F-FP-CIT. Second-generation 18F-radioligands for DAT are (E)-N-(4-fluorobut-2-enyl)-2β-carbomethoxy-3β-(4′-tolyl)nortropane (LBT-999) and fluoroethyl-PE2I. The 11C analog of LBT-999 has been studied in baboons and seems to be a suitable DAT radioligand for in vivo quantification (5). 18F-fluoroethyl-PE2I has been evaluated only in preclinical studies and seems to be a promising DAT radioligand because of its fast kinetics and favorable metabolism (6).
Factors Influencing DAT Availability
The investigation of the effect of age on DAT availability has provided consistent results indicating a 6%–8% decline of DAT per decade, using various SPECT or PET radioligands. In addition, a PET study has demonstrated that the DAT decline is paralleled by deterioration in episodic memory and executive functioning with advancing age, suggesting that DAT binding is a powerful mediator of age-related cognitive changes as well as of cognitive functioning in general (4). DAT availability appears to be influenced also by sex, being higher in women than men. These findings should be taken under consideration when one is designing in vivo imaging studies aimed at assessing group differences in DAT availability.
Antidepressants and selective serotonin reuptake inhibitors can also induce changes in DAT availability. Preclinical and clinical studies have shown that clomipramine, citalopram, and paroxetine determine an increase in DAT availability (7). One possible explanation of such an increase is that inhibition of 5-hydroxytryptamine uptake could lead to a rapid regulation of DAT molecules to more efficiently remove dopamine from the synapse. These effects on striatal DAT should be considered, because patients often are treated with various drugs—including selective serotonin reuptake inhibitors—that can affect the quantitative outcome measures of the studies.
DAT Imaging as a Diagnostic Biomarker
DAT imaging has been successfully applied to several central nervous system disorders. Table 1 summarizes the main findings of DAT availability in movement disorders and other neurodegenerative disorders. The main application has been the quantification of the dopaminergic deficit in PD. The pathology of PD consists of the loss of dopamine neurons in the substantia nigra and the reduction of dopamine projections to the striatum. Both 123I-β-CIT and 123I-FP-CIT SPECT have high power to discriminate PD from normal aging, particularly when DAT availability in the putamen is evaluated. Similar results, with sensitivity and specificity between 95% and 100%, have been obtained with 99mTc-TRODAT-1, suggesting that the 3 radioligands are equally sensitive in detecting the dopamine deficit at an early stage of PD.
DAT Imaging in Parkinsonism, Related Movement Disorders, and Other Neurodegenerative Disorders
The main clinical application of DAT imaging is the differentiation of degenerative parkinsonism from conditions not associated with dopamine deficit, such as essential tremor and drug-induced, vascular, or psychogenic parkinsonism. Two SPECT studies—one conducted in the United States (using 123I-β-CIT) and one in Europe (using 123I-FP-CIT)—have reported respective sensitivities of 98% and 95% and respective specificities of 83% and 94% in the differentiation of essential tremor from PD. In the clinical setting, the utility of SPECT of DAT is to prove the presence of degenerative parkinsonism in conditions having an uncertain diagnosis and warranting appropriate treatment. A multicenter study with 123I-FP-CIT SPECT has shown that DAT imaging contributed to a change in diagnosis in 52% of patients and also prompted changes in clinical management in 72% of patients (8). In PD, DAT availability has also been found to correlate with prefrontal cognitive functions, particularly in the caudate region, whereas DAT availability in the putamen is correlated mainly with motor function (9). DAT imaging is not reliable for the differentiation of PD from atypical parkinsonian disorders such as multiple-system atrophy and progressive supranuclear palsy, disorders in which the degree and pattern of dopamine deficit are similar to PD.
DAT dysfunction is common to disorders characterized by Lewy-body pathology, including PD dementia and DLB. In DLB, dementia usually occurs before the development of parkinsonism, and early identification of dopamine deficit is important for the management of patients. Dopamine dysfunction is not a characteristic of AD pathology, and DAT imaging is an established tool for differential diagnosis between AD and DLB. A multicenter phase III clinical trial with 123I-FP-CIT SPECT in 94 patients with probable DLB, 57 patients with possible DLB, and 147 patients with non-DLB dementia reported a mean sensitivity of 77.7% for detecting clinically probable DLB, a specificity of 90.4% for excluding non-DLB dementia, and diagnostic accuracy and positive and negative predictive values of 85.7%, 82.4%, and 87.5%, respectively (10). The gold standard in this study, clinical diagnosis, is far from perfect and, compared with autopsy data, has shown a sensitivity not exceeding 85%. Therefore, a sensitivity of 78% is an accurate outcome for imaging studies.
DAT Imaging as a Biomarker of Dopamine Deficit in PD
The conventional understanding about dopamine deficit and PD is that parkinsonian symptoms develop when approximately 70%–80% of dopamine neurons are lost. However, PET and SPECT studies have shown that an approximately 50% loss of dopamine terminals is required for the onset of symptoms. In hemiparkinsonian patients, the striatum contralateral to the more affected side shows about a 50% DAT loss, but the “unaffected” striatum shows about a 30% DAT loss. This finding has drawn interest toward the use of DAT imaging in preclinical PD by studying either preclinical conditions or genetic mutations associated with parkinsonism. Hyposmia is a common sign that can be present years before the onset of PD. A study of a large cohort of healthy subjects has found that approximately 10% of hyposmic subjects show a DAT loss and develop parkinsonism within 2 y and that an additional 12% of hyposmic individuals show a decrease in DAT over a 2-y follow-up (11). These findings suggest that idiopathic hyposmia can be a preclinical sign of PD. Rapid-eye-movement sleep behavior disorder is another common condition that can precede the onset of PD, and some studies have shown that patients with idiopathic development of this disorder show an impairment of presynaptic dopaminergic function almost to the degree seen in PD patients (12).
Mutations in the Parkin gene are the cause of autosomal recessive early-onset PD. Heterozygous and homozygous carriers of Parkin mutations already show a dopaminergic deficit at a preclinical stage, and the severity of the dopaminergic deficit seems to be related to the number of mutated alleles. Taken together, these findings strengthen the observation that DAT imaging can be a sensitive marker for early and presymptomatic diagnosis of PD and that strategies combining dopaminergic imaging with early clinical signs or symptoms (i.e., olfactory loss or rapid-eye-movement sleep behavior disorder) and known genetic mutations for PD can be used to identify individuals at risk for PD before the onset of motor symptoms (13).
DAT Imaging as a Biomarker of Progression in PD
The decline of DAT as the disease progresses is an exponential process that can be followed by longitudinal DAT imaging (14). PET and SPECT studies have shown that the decrease in DAT is approximately 8%–10% per year; thus, the rate of decline of dopamine function is approximately 10 times faster in PD than in normal aging. The possibility of quantifying the progression of dopamine dysfunction has raised the question of whether imaging of dopamine function with DAT SPECT or 6-fluoro-l-dopa (FDOPA) PET could be used as a surrogate biomarker of disease progression to assess the effect of putative neuroprotective or disease-modifying drugs.
DAT Imaging as a Biomarker of Therapy Monitoring
DAT SPECT and FDOPA PET are imaging modalities that would satisfy the requirements for a biomarker of disease progression, because they correlate with the number of dopamine neurons and with the stage and severity of PD symptoms. Two independent clinical trials with 123I-β-CIT SPECT (Comparison of the Agonist Pramipexole with Levodopa on Motor Complications of Parkinson's Disease, or CALM-PD) and 18F-FDOPA PET (Requip [ropinirole; GlaxoSmithKline] as Early Therapy Versus l-Dopa-PET), or REAL-PET) have shown that PD patients treated with a D2 agonist, either pramipexole or ropinirole, have a slower progression of dopamine deficit than do patients treated with l-dopa. However, the findings of the 2 studies have raised several questions about interpretation of the results. Are D2 agonists neuroprotective? Is l-dopa neurotoxic? Is l-dopa interfering with DAT expression? Some of these questions remain unanswered. Preclinical and clinical studies on a small number of research subjects have shown that l-dopa or D2 agonists have small or insignificant effects on DAT. A subsequent randomized, double-blind, placebo-controlled trial (Earlier Versus Later Levodopa Therapy in Parkinson Disease, or ELLDOPA) in 361 PD patients assigned to receive different daily doses of l-dopa (150, 300, or 600 mg) or placebo showed a significant clinical benefit of l-dopa over placebo. In the 123I-β-CIT SPECT substudy of 142 patients from the same cohort, the DAT decline was more significant in the l-dopa groups than in the placebo group, with the difference being greatest in the group receiving the highest l-dopa dose. The discrepancy between the clinical effect of l-dopa and the results of the neuroimaging study questions the interpretation of 123I-β-CIT SPECT in the presence of dopaminergic agents (15).
Although many unresolved questions remain about the usefulness of DAT imaging or FDOPA PET as surrogate biomarkers of disease progression, these imaging modalities seem to be useful molecular biomarkers to assess the effects of restorative therapies on the primary pathologic dysfunction of PD. DAT imaging and FDOPA PET have been used in preclinical models of PD using either fetal mesencephalic cells or glial cell line–derived nerve factor or in applied studies on PD patients who have received transplanted mesencephalic cells (16) or were treated with glial cell line–derived nerve factor, to assess the integrity of the dopaminergic system before and after treatment. DAT imaging has also been used to evaluate longitudinally the effect of deep-brain stimulation of the subthalamic nucleus on DAT availability in PD patients with advanced disease (17).
DAT Imaging in ADHD
DAT imaging has also been applied to the study of neuropsychiatric disorders in which the dopaminergic system is implicated. Attention-deficit hyperactivity disorder (ADHD) is a pediatric psychiatric condition characterized by the presence of inattention, hyperactivity, and impulsivity. The disorder can also manifest in adults, with a prevalence of 2%–4%. Symptoms can be alleviated by treatment with methylphenidate. Imaging studies of DAT have found somewhat contradictory results, probably related to differences in patient populations, imaging modalities, or radioligands used. Some studies on children and adults with ADHD have reported increased striatal DAT availability (18), whereas other studies have indicated no changes or, rather, decreased DAT availability in adults with ADHD (19). A PET study with 11C-PE2I in adolescents with ADHD has reported a decrease in DAT availability in the midbrain, suggesting that the substantia nigra is also involved in the dopamine dysfunction associated with ADHD (3). More recently, Volkow et al., in studying 55 unmedicated adults with ADHD, reported decreased DAT availability in the caudate and other brain areas (such as the nucleus accumbens and the midbrain) involved in reward and motivation, suggesting a specific impairment of the dopamine reward pathway in ADHD (20). Although partially controversial, these studies suggest that the dopamine system is implicated in the pathophysiology of ADHD and that DAT imaging can be used to examine the functional status of the system and to monitor the effect of methylphenidate treatment.
CONCLUSION
DAT is a transmembrane protein involved in the regulation of extracellular levels of dopamine. Currently, SPECT radioligands for DAT, such as 123I-FP-CIT, 123I-β-CIT, and 99mTc-TRODAT-1, represent molecular imaging tools available for daily practice. The development of 18F-radioligands for DAT may provide new opportunities for more widespread use of PET or PET/CT in the diagnostic work-up of patients with PD or related movement disorders.
Acknowledgments
Part of this work has been supported by FP6-project DiMI, LSHB-CT-2005-512146.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication December 4, 2009.
- Accepted for publication March 31, 2010.





{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Radioligands for In Vivo Imaging of DAT
- Factors Influencing DAT Availability
- DAT Imaging as a Diagnostic Biomarker
- DAT Imaging as a Biomarker of Dopamine Deficit in PD
- DAT Imaging as a Biomarker of Progression in PD
- DAT Imaging as a Biomarker of Therapy Monitoring
- DAT Imaging in ADHD
- CONCLUSION
- Acknowledgments
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Optimal Acquisition Time Window and Simplified Quantification of Dopamine Transporter Availability Using 18F-FE-PE2I in Healthy Controls and Parkinson Disease Patients
- A New Era of Clinical Dopamine Transporter Imaging Using 123I-FP-CIT
- Authors' response
- Imaging of the Striatal and Extrastriatal Dopamine Transporter with 18F-LBT-999: Quantification, Biodistribution, and Radiation Dosimetry in Nonhuman Primates