


Abstract
Diabetes mellitus (DM) is a common metabolic disorder. Hyperglycemia occurs in a significant proportion of patients with uncontrolled DM but can also be found in patients without diabetes. Although the relationship between 18F-FDG uptake in malignant tumors and blood glucose levels has been previously addressed, it has not been investigated in cases of infection and inflammation, despite the high incidence of these entities in diabetic patients. The current study assessed whether hyperglycemia and DM affect the detectability rate of disease in 18F-FDG PET/CT studies performed for patients with suspected infectious and inflammatory processes, as compared with a group of patients with malignant tumors. Methods: 18F-FDG PET/CT studies of 123 consecutive patients investigated for suspected infection or inflammation and 320 patients evaluated for malignancy were retrospectively analyzed. The presence of DM and the level of glucose at the time of the study were recorded. Differences between the 2 study populations in false-negative (FN) rates in patients with and without hyperglycemia and DM were compared and analyzed for statistical significance. Results: In the infection or inflammation group, 19 of 123 patients (15%) had serum glucose levels greater than 180 mg/dL and 43 of 123 (35%) had DM. There were no FN studies in patients with hyperglycemia and 4 FN studies in patients with normal glucose levels. There were 2 FN studies each in patients with and without DM. Neither glucose levels nor DM affects the detection rate of infection or inflammation with 18F-FDG PET/CT. In the oncology group, 84 of 320 patients (26%) had serum glucose levels greater than 180 mg/dL and 183 of 320 (57%) had DM. There were 6 FN studies in cancer patients with hyperglycemia and 7 in patients with normal glucose levels. There were 8 FN studies in cancer patients with DM and 5 FN studies in patients without DM. Higher glucose levels but not DM affected the detection rate of malignancy with 18F-FDG PET/CT. Conclusion: High glucose levels at the time of the study but not DM may reduce the sensitivity of 18F-FDG PET/CT in the assessment of malignancy. No significant impact on the FN rate was found in patients with infection and inflammatory processes with either DM or hyperglycemia.
PET after the administration of 18F-FDG is widely used in the assessment of many malignancies. 18F-FDG imaging of cancer relies on a molecular shift in glucose transporters in malignant cells, resulting in increased uptake of glucose within the tumor. The relationship between the presence of diabetes mellitus (DM) or elevated glucose serum levels and the sensitivity of 18F-FDG studies is still a controversial issue. Although the biodistribution of 18F-FDG is adequate in patients (with or without diabetes) with blood glucose levels less than 180 mg/dL at the time of the study (1), guidelines for 18F-FDG PET/CT in cancer patients recommend that attempts should be made not to inject 18F-FDG when blood glucose levels exceed 200 mg/dL (2,3). The impact of hyperglycemia or DM has been investigated in cancer patients in a few specific malignancies, with mixed results. Although hyperglycemia was found to decrease the detection rate of pancreatic cancer by 18F-FDG PET (4), it did not affect the sensitivity of this modality in cervical cancer (5). Results in lung cancer were controversial, showing either no change (6) or a decrease in 18F-FDG uptake (7).
18F-FDG, an indicator of increased intracellular glucose metabolism, is taken up by infectious and inflammatory processes as well, and several studies have demonstrated the value of 18F-FDG PET/CT in this specific clinical setting (8–12). Many infectious processes are more common in diabetic patients, whereas other processes exhibit increased severity and a higher risk of complications in association with DM (13). To the best of our knowledge, no data are currently available regarding the detectability rate of 18F-FDG PET/CT for infection and inflammation in patients with DM or hyperglycemia at the time of imaging. The current study investigated whether these factors affect the diagnostic accuracy of 18F-FDG PET/CT for the detection of infectious processes, as compared with the assessment of malignancy, in a retrospective data analysis of 443 patients.
MATERIALS AND METHODS
Patient Population
18F-FDG PET/CT studies of 123 consecutive patients investigated for suspected infection or inflammation and 320 randomly selected patients evaluated for malignancy (for a total of 443 files) were retrospectively analyzed.
The infection group included 87 men and 36 women, with a mean age of 61 y (range, 23–87 y). Inclusion in the study was based on fever of unknown origin (FUO) (n = 46), assessment of diabetic foot (n = 26), and suspected vascular graft infection (n = 51). The oncologic group included 186 men and 134 women, with a mean age of 63 y (range, 18–90 y). Studies were performed for assessment of a single pulmonary nodule (n = 42), Hodgkin and non-Hodgkin lymphoma (n = 95), lung cancer (n = 72), colon cancer (n = 43), malignant melanoma (n = 15), gynecologic malignancies (n = 14), head and neck cancer (n = 8), breast cancer (n = 8), and other tumors (n = 23).
The presence or absence of DM was recorded in all patients. Glucose serum levels were measured in all patients before the injection of 18F-FDG PET. Hyperglycemia was defined as values above 180 mg/dL. The hospital Institutional Review Board approved the study.
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 296–444 MBq (8–12 mCi) of 18F-FDG. The patients were instructed to keep their regular drug schedule. No additional glucose-control drugs were used in patients with high blood glucose levels. Insulin-dependent diabetic patients were scheduled to undergo their studies in the late morning or at noon and instructed to inject the normal amount of insulin before the start of the fasting period. No insulin was administered concurrent with or after 18F-FDG injection. Oral contrast was administered to the patients during the uptake time. No intravenous contrast material was used for the CT scan.
All patients in the oncologic group underwent head to mid-thigh acquisition. Lower limb scanning was added when clinically indicated. Patients in the infection or inflammation group were scanned according to the area of the suspected infection (diabetic foot, vascular graft) or using the routine head–to–mid-thigh acquisition protocol (FUO). PET and CT images were acquired consecutively 90 min after the injection of 18F-FDG, using a PET/CT system (Discovery LS; GE Healthcare). CT data were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET data were reconstructed iteratively using ordered-subset expectation maximization software. PET, CT, and fused PET/CT images were available for review and displayed in axial, coronal, and sagittal planes.
Interpretation and Analysis of PET/CT Images
All studies were reviewed by a combined team of nuclear medicine physicians and radiologists with knowledge of the patient's clinical history and the results of previous imaging studies. Studies showing at least 1 focus of increased 18F-FDG PET uptake with intensity higher than that of surrounding tissues, localized by PET/CT to an area that did not correspond to the physiologic biodistribution of the radiotracer, were defined as positive. Studies showing 18F-FDG PET activity only in areas of the physiologic tracer biodistribution or no sites of increased uptake were considered negative. An abnormal 18F-FDG PET/CT result, further confirmed as representing active malignancy or infection or inflammation, was defined as true-positive (TP). A normal 18F-FDG PET/CT study with further evidence of active disease was defined as false-negative (FN). The FN rate was calculated as the proportion of FN studies among all patients with disease (FN/TP + FN). The difference in FN rates between patients with and without DM and hyperglycemia and in patients with infection or inflammation and cancer was assessed for statistical significance using the χ2 test for homogeneity of proportions (a P value ≤ 0.05 was considered to be significant).
RESULTS
Records for 443 patients who underwent 18F-FDG PET/CT for the assessment of infection or inflammation (n = 123) and cancer (n = 320) were reviewed. There were a total of 285 TP studies—61 in the infection or inflammation group and 224 in the oncology group. Seventeen studies were determined to be FN—4 in the infection or inflammation group and 13 in the oncology group. No statistically significant difference in the FN rates was observed between the 2 groups (4/65 vs. 13/237, P = not significant). Overall, 226 of 443 patients (51%) had DM, and hyperglycemia was measured in 103 patients (23%).
In the infection or inflammation group, 43 of 123 patients (35%) had DM and 19 of 123 patients (15%) had serum glucose levels greater than 180 mg/dL (range, 189–330 mg/dL). Nineteen of 43 diabetic patients (44%) had high blood glucose levels at the time of the study, and all 19 hyperglycemic patients had DM. There were 60 TP studies in this group, including 24 in patients with DM, 11 with hyperglycemia at the time of the study, 36 without diabetes, and 49 with normal glycemia levels. The 4 FN studies included 2 patients with DM and 2 patients without diabetes, all with normal blood glucose levels (Table 1). Two of these 4 patients presented with suspected vascular graft infection. An infected pus-secreting wound was found in the medial aspect of the left thigh of one patient (Fig. 1), and an infected vascular graft was diagnosed in the second patient. Two additional FN studies occurred in patients assessed for FUO, further diagnosed as granulomatous hepatitis and low-grade non-Hodgkin lymphoma. In the assessment of patients with infectious or inflammatory processes, no statistically significant difference was found in the FN rates of 18F-FDG PET/CT for either DM (2/26 vs. 2/38, P = not significant) or high blood glucose levels (0/11 vs. 4/53, P = not significant) (Table 2; Fig. 2).

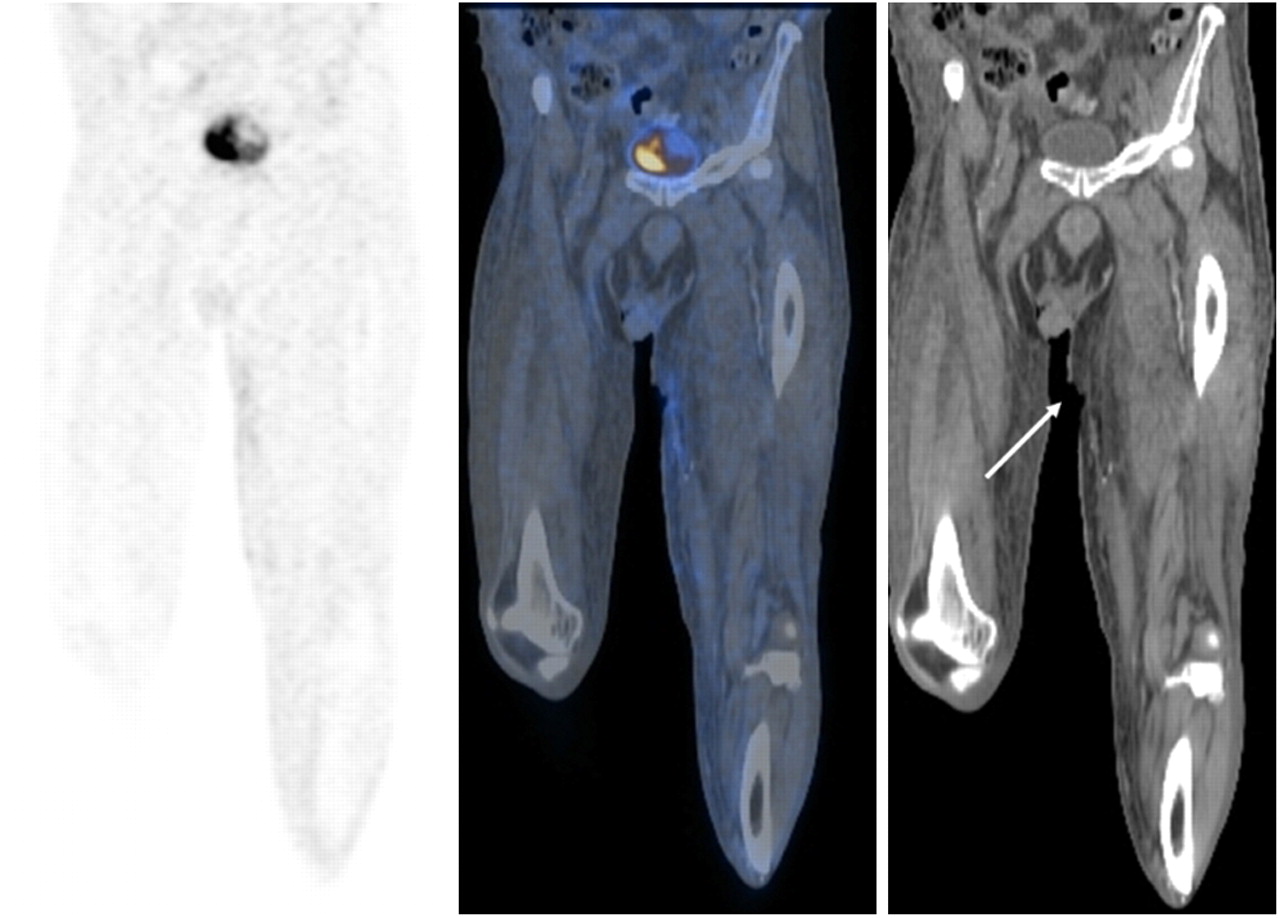
A 66-y-old diabetic man who had received left femoropopliteal bypass graft insertion 18 mo before current investigation. Patient was admitted with clinical suspicion of infection due to fever and tenderness at medial aspect of proximal thigh. Serum glucose level at time of study was 84 mg/dL. Coronal 18F-FDG PET (left), PET/CT (center), and CT (right) slices show no 18F-FDG uptake in deep soft-tissue wound demonstrated on CT at medial aspect of left thigh (arrow). Final diagnosis by microbial assay indicated bacterial soft-tissue infection, and antibiotic therapy was instituted with good response.

A 64-y-old diabetic man who presented with fever and swollen, tender right foot. 18F-FDG PET/CT was performed because of clinical suspicion of diabetic foot osteomyelitis. Serum glucose level at time of study was 290 mg/dL. Transaxial 18F-FDG PET (left), PET/CT (center), and CT (right) slices show 18F-FDG uptake at medial aspect of right forefoot, involving only soft tissues with sparing of metatarsal bones (arrow). Extensive soft-tissue infection involving muscles and planter fascia and no osteomyelitis were found at surgery.
Clinical Characteristics of 17 Patients with FN 18F-FDG PET/CT Results
FN Rate* of 18F-FDG PET/CT in Patients with Infection or Inflammation and Cancer
In the oncology group, 183 of 320 patients (57%) had DM and 84 of 320 (26%) had serum glucose levels greater than 180 mg/dL (range, 181–379 mg/dL). Sixty-eight of 183 diabetic patients (37%) had high blood glucose levels at the time of the study, and 68 of 84 hyperglycemic patients (81%) had DM. There were 224 TP studies in this group, including 114 in patients with DM, 50 with hyperglycemia, 110 without diabetes, and 174 with normal glycemia levels. The 13 FN studies included 8 patients with DM and 5 patients without diabetes (Table 1). There were 6 FN studies in cancer patients with hyperglycemia and 7 in patients with normal glucose levels. Four of the 13 patients were investigated for a single pulmonary nodule and had a final diagnosis of bronchoalveolar carcinoma (n = 2), squamous cell carcinoma (n = 1), and lung metastasis of renal cell carcinoma origin (n = 1). Three patients had recurrent non-Hodgkin lymphoma (diffuse large cell, n = 2; follicular, n = 1), 3 patients had liver metastases, 1 patient had melanoma metastatic to the lungs, 1 had recurrent mesothelioma, and 1 had cancer of the pancreas (histologic and morphologic characteristics are detailed in Table 1). The FN rate was found to be statistically significantly higher in cancer patients with hyperglycemia than in those with blood glucose levels less than 180 mg/dL (6/56 vs. 7/181, P < 0.05). DM had no statistically significant impact on the FN rate of malignancy with 18F-FDG PET/CT (8/122 vs. 5/115, P = not significant) (Table 2).
DISCUSSION
18F-FDG PET/CT is a well-accepted tool for the clinical assessment of a wide range of malignancies and has also been shown to play a promising role in the evaluation of infection and inflammation. 18F-FDG, in a manner similar to glucose, enters the cells by active passage through the cell membrane, mediated by the glucose transporters 1–7 and sodium-glucose–linked transporters 1–2, which exchange sodium for glucose. Intracellular 18F-FDG is phosphorylated by hexokinase to FDG-6-P, which—unlike phosphorylated glucose—is not a suitable substrate for the glucose-6-P-isomerase and is therefore unable to exit the cells. In the presence of an active disease process characterized by an accelerated metabolic rate, malignant and inflammatory cells have increased 18F-FDG uptake, which is mediated by different cytokines and growth factors (14). The increased 18F-FDG uptake is due to an increased number of glucose transporters with increased affinity for deoxyglucose.
DM affects 18% of the population over the age of 65 and has risen in incidence over the past decade. Among other factors, the incidence of DM is expected to increase even more in the future because of more people who are obese and the drop in physical exercise. Hyperglycemia in DM is due to insulin deficiency related to the destruction of pancreatic β-cells. Hyperglycemia can also occur during stress, because of an increase in adrenergic neurotransmitters and other factors that encourage hepatic glycogenolysis and gluconeogenesis.
There is a paucity of data regarding the influence of DM or hyperglycemia on the diagnostic capabilities of 18F-FDG PET/CT; this topic has been previously addressed only in several specific malignancies. 18F-FDG uptake, measured by standardized uptake value, decreased significantly after glucose loading in patients with bronchogenic carcinoma (15) and in head and neck malignancies and was associated with increased muscular uptake that resulted in image-quality degradation (16). Hyperglycemia, unrelated to the presence of DM, has been reported to decrease the intensity of 18F-FDG uptake, resulting in a poorer detectability rate of pancreatic cancer (4). These findings were further supported by an in vitro study on cancer cells that demonstrated that acute hyperglycemia at the time of the test affects 18F-FDG uptake, probably because of a decrease in glucose transporter 1 (which potentially aims to maintain the normal glucose intake of malignant cells, even in the presence of hyperglycemia) (17). However, although 18F-FDG activity was found by some authors to be lower in diabetic patients with primary lung cancer (7), a recent report indicated that the standardized uptake value of malignant lung tumors in 40 diabetic patients did not differ significantly from values measured in patients without diabetes (6). Furthermore, 18F-FDG uptake of lung cancer in patients with DM was not significantly different between patients with and patients without hyperglycemia at the time of the study. These authors hypothesized that their findings were related to an overexpression of glucose transporters 1 and 3—which cannot be saturated even in the presence of high blood glucose levels—in non–small cell lung cancer (6).
The use of 18F-FDG PET/CT in infectious and inflammatory processes has been implemented only in recent years, and data regarding the effect of hyperglycemia and DM on 18F-FDG uptake in these entities are therefore sparse. Activated inflammatory cells are characterized by an increased metabolic rate, with high glucose consumption—thus the high performance of 18F-FDG imaging, with a positive predictive value of 91% and a negative predictive value of 100% in this particular clinical indication (18). A study investigating the relationship between blood glucose levels and the degree and intensity of 18F-FDG activity as measured by standardized uptake value in malignant and infectious processes indicated that hyperglycemia induced a slight decrease in tracer uptake in malignant tumors but, in contrast, had only a slight and positive effect on 18F-FDG uptake in inflammatory and infectious lesions (19). The reason for the different response to hyperglycemia of inflammatory and malignant cells is unclear and could be related to multiple factors. One potential explanation for the less significant effect of glucose levels on 18F-FDG uptake in infectious and inflammatory processes, as compared with malignancy, could rely on their different intracellular glycogen storage. Although tumor cells exhibit an increased glycolytic activity, have low glycogen storage capabilities, and fully depend on extracellular glucose supply, inflammatory cells are capable of mobilizing intracellular glycogen during periods of low plasma glucose (19).
The present study examines, for the first time to the best of our knowledge, whether altered glucose metabolism affects the diagnostic accuracy of 18F-FDG PET/CT in patients with cancer and infection or inflammation. As demonstrated by the present data, the detectability rate of active disease in the group of patients with a suspected infectious or inflammatory process was not affected by elevated glucose levels or DM. The 4 FN studies found in this patient population could not be characterized by any particular clinical features. This low FN rate is in concordance with other studies that reported a high diagnostic accuracy of 18F-FDG PET/CT in infection and inflammation in heterogeneous study populations, unrelated to the presence of hyperglycemia and DM (9,10,18).
The present data also indicate, however, that hyperglycemia statistically significantly affected the diagnostic accuracy of 18F-FDG PET/CT in the group of patients assessed for the presence of an active malignant tumor, in agreement with some previously published reports (4,17). Thirteen FN studies were found in this patient population. Five of these patients had tumors with a histology known to be overall less 18F-FDG–avid. DM did not represent an interfering factor in the 18F-FDG PET/CT assessment of cancer. However, these results, in addition to those in several previously published reports regarding the effect of hyperglycemia on 18F-FDG uptake in cancer (1,4,7,19), are in disagreement with the results of an experimental study in a rat model. That model suggested that 18F-FDG uptake in inflammatory lesions was significantly impaired with hyperglycemia, and tumor uptake of 18F-FDG was not significantly affected (20). These discrepancies may be related to the differences in the metabolic state of the investigated subjects. Although acute, controlled hyperglycemia was induced in the rat model in healthy subjects, hyperglycemia in patients with or without DM represents in most cases a chronic systemic condition.
A limitation of this study may be the relatively high proportion of diabetic patients in the randomly selected oncology group, as compared with the general population. This high proportion may be potentially related—at least in part—to steroid treatment, commonly administered in oncologic patients, which may lead to a higher rate of DM and to the higher prevalence of this condition in elderly individuals who were represented in significant numbers in the present study population. A strong association between hyperglycemia and DM was found in both the oncology and the infection or inflammation groups. Of patients with DM, 44% in the infection or inflammation and 37% in the oncology group had high glucose levels at the time of the study, and 100% and 81% of hyperglycemic patients, respectively, had DM.
CONCLUSION
DM did not significantly affect the diagnostic accuracy of 18F-FDG PET/CT for the assessment of malignancy or infectious and inflammatory processes. However, hyperglycemia at the time of the study can lead to a higher FN rate in the oncology group, and imaging in the presence of high blood glucose levels should be avoided in cancer patients. In contrast, high blood glucose levels at the time of the 18F-FDG PET/CT study did not significantly affect the detectability rate of infectious and inflammatory processes and had no statistically significant impact on the number of FN studies in this patient population. On the basis of the results of the present study, hyperglycemia—which is frequently detected in acute and chronically ill patients—and DM—which is often an underlying condition in patients presenting with a suspected infectious process—should not be considered as potential contraindications for performing 18F-FDG PET/CT studies.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication December 30, 2009.
- Accepted for publication March 19, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Importance of Blood Glucose Management Before 18F-FDG PET/CT in 322 Patients with Bacteremia of Unknown Origin
- Role of 18F-FDG PET/CT in Large Vessel Vasculitis and Polymyalgia Rheumatica
- Assessing the Effect of Various Blood Glucose Levels on 18F-FDG Activity in the Brain, Liver, and Blood Pool
- Metformin Targets Mitochondrial Glycerophosphate Dehydrogenase to Control Rate of Oxidative Phosphorylation and Growth of Thyroid Cancer In Vitro and In Vivo
- Does Antibiotic Treatment Affect the Diagnostic Accuracy of 18F-FDG PET/CT Studies in Patients with Suspected Infectious Processes?
- Detection of Osteomyelitis in the Diabetic Foot by Imaging Techniques: A Systematic Review and Meta-analysis Comparing MRI, White Blood Cell Scintigraphy, and FDG-PET
- The Reverse Warburg Effect and 18F-FDG Uptake in Non-Small Cell Lung Cancer A549 in Mice: A Pilot Study
- Positron Emission Tomography/Computed Tomography for Diagnosis of Prosthetic Valve Endocarditis: Suggestions to Increase Diagnostic Accuracy
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Could Different Hydration Protocols Affect the Quality of 18F-FDG PET/CT Images?