


Abstract
The purpose of this study was to determine whether dual-phase 18F-FDG PET could be a prognostic factor for adenocarcinoma of the lung. Methods: One hundred patients with histologically proven adenocarcinoma of the lung were included in this retrospective analysis. All patients underwent dual-phase pretherapy 18F-FDG PET for which, after the intravenous administration of 18F-FDG, both early (∼60 min) and delayed (∼90 min) PET were acquired. The percentage change in the maximal standardized uptake values (SUVmax) of the cancer between the early and the delayed images was calculated. Overall survival of the SUVmax change over time together with the known prognostic factors were calculated by the Kaplan–Meier method and evaluated with the log-rank test. The prognostic significance was assessed by univariate and multivariate analyses. Results: Statistical analysis showed that SUVmax change over time between the early and the delayed PET was a strong independent predictor of outcome for lung adenocarcinoma. A cutoff of 25% change for SUVmax over time showed the best discriminative value. Patients with more than 25% increase in SUVmax had a median survival of 15 mo, compared with 39 mo for those with less than 25% increase in SUVmax. Conclusion: Dual-phase 18F-FDG PET reflects the dynamics of glucose metabolism. Our findings suggest that the percentage SUVmax change over time is a strong prognostic factor in patients with lung adenocarcinoma and can be complementary to the other well-known factors.
Lung cancer is one of the most common malignancies in the world and a leading cause of death in Western countries. It is estimated that 215,020 patients in the United States received the diagnosis of lung cancer during 2008 and that 161,840 deaths were attributed to the disease (1). The 5-y survival rate is poor and is related to the low cure rate (6%–15%), which in turn is associated with the lack of adequate screening measures, few patients diagnosed at an early stage of disease, and poor treatment efficacy in advanced disease (2). In recent years, the frequency of lung adenocarcinoma has increased (1). The major prognostic factors in lung cancer include tumor stage, clinical factors, pathologic indices, and genetic markers (3). Although the TNM staging system is the most common tool used by oncologists to estimate prognosis and to choose the suitable combination of therapy, it does not always give a satisfactory explanation for differences in survival. Recent advances in molecular biology explain more about different patterns of survival (4).
Lung cancer is characterized by carbohydrate metabolic derangements, which also have been identified as independent prognostic factors correlated with poor treatment response (5). These glucose metabolism derangements can be measured quantitatively in vivo by PET after the administration of 18F-FDG. 18F-FDG uptake in lung cancer cells has been correlated with growth rate and proliferation (6). Standardized uptake value (SUV) is the commonly used measure of 18F-FDG uptake in tumors. It provides a semiquantitative and static index of 18F-FDG uptake and is conceptualized as the ratio of 18F-FDG uptake in the tumor to the injection dose normalized to the patient's body weight (7).
Although malignant lesions may have higher levels of SUV, various benign conditions, such as inflammation cells or granulation tissues, may also have a high SUV (8). Because of the longer time required for levels of 18F-FDG to plateau in cancer cells than in inflammatory cells in cell line studies, some investigators performed dual-phase 18F-FDG PET, which includes delayed scanning, to differentiate benign from malignant lesions in various cancers. The results from most investigators showed that this delayed scan is valuable (9,10). This finding probably is related to the upregulation of glucose consumption, demonstrated by the malignant cells, to obtain more energy for proliferation. This leads to graded concentration of 18F-FDG in tumor cells. In contrast, such a prolonged period of 18F-FDG uptake is less common in inflammatory lesions or normal tissues (10).
Although some studies correlated the SUV to survival (11,12), to the best of our knowledge, the prognostic role of dual-phase 18F-FDG PET in primary lung cancer has not been evaluated previously. The purpose of this study was to determine whether dual-phase 18F-FDG PET can predict the outcome in patients with primary lung adenocarcinoma.
MATERIALS AND METHODS
Patients
The medical records of 100 consecutive patients with newly diagnosed lung adenocarcinoma who underwent 18F-FDG PET at our institution from January 2000 to January 2004 were retrospectively reviewed. Follow-up was completed and closed by the death of the last patient in August 2008. Eligibility requirements included the presence of histologic proof of adenocarcinoma and contrast-enhanced chest CT and PET performed within 30 d. Exclusion criteria were the following: known diabetes, age younger than 18 y, prior lung surgery, and chemotherapy or radiation therapy. After reviewing the available clinical information including the surgical pathology reports, initial staging was assigned according to the guidelines of the American Society of Clinical Oncology (13). This study was performed after approval had been obtained from the Institutional Review Board. Patient and tumor characteristics are listed in Table 1.
Patient and Tumor Characteristics
18F-FDG PET
PET was performed as a part of the initial workup of patients within 14 d after pathologic diagnosis of the lung cancer. All patients fasted for at least 6 h before examination to ensure standardized glucose metabolism. At the time of 18F-FDG administration, fasting plasma glucose values were lower than 150 mg/dL in all patients. Depending on the patients' weight, an activity of 2.51 MBq/kg of 18F-FDG was injected through an indwelling catheter inserted into an antecubital vein. PET scans were acquired using a dedicated full-ring scanner (CPET PET scanner; Philips/ADAC) equipped with lutetium oxyorthosilicate crystals, with a 162-mm axial field of view.
Dual-phase 18F-FDG PET was performed for all patients, for whom an early (∼60 min) and delayed (∼90 min) PET study was acquired, after 18F-FDG administration. The early scan was obtained from the skull base to mid thigh, whereas the second scan was acquired from the neck to the upper abdomen. Patients were instructed not to move or leave the scanner between the two 18F-FDG PET scans. Imaging was performed, using sequential overlapping scans, by acquiring 6–8 bed positions, depending on patients' heights. The acquisition time for scanning was 2 min for emission and 1 min for transmission per bed position. The transmission scan was acquired using a 137Cs single-event source of 662 to correct for nonuniform attenuation. Patients were examined supine, with their arms above their head. The PET scanner was working in a fully 3-dimensional mode. Image reconstruction was performed using an iterative reconstruction algorithm based on the row action maximum likelihood algorithm. The reconstructed volume image had the same number of slices and slice separation as the raw sinogram data and an image pixel size of 4.0 mm. Resolution was 5.5 mm in full at half maximum at the center of the field of view. Slice thickness and the slice interval were both 4 mm. The reconstructed images were displayed in axial, coronal, and sagittal planes and were interpreted by 2 nuclear medicine physicians. Quantitative analysis was applied to the attenuation-corrected images by calculating the SUV of areas of abnormal 18F-FDG uptake, corrected for the injected dose of 18F-FDG, and adjusted for the patient's weight, as previously described (14). Tumor mass was identified by areas of pathologically increased 18F-FDG uptake, avoiding physiologic uptake. SUV was independently measured by using regions of interest drawn on the area of maximal metabolic activity on every axial slice of tumor-related increased 18F-FDG uptake. SUVmax was defined as the highest pixel value related to the neoplasm burden in each study and was computed using the following formula: SUVmax = maximum activity concentration in the neoplasm (kBq/mL)/[injected dose (MBq)/body weight (kg)].
SUVmax was calculated for both the early (SUVmax1) and the delayed (SUVmax2) 18F-FDG PET scans, for which identical transaxial slices were identified by using the bed position number together with the anatomic landmarks. The percentage change of SUVmax of neoplasm between the early and delayed images was calculated as follows: percentage change SUVmax = [(SUVmax2 – SUVmax1)/SUVmax1] × 100%.
CT
CT images were obtained with multislice CT scanners: the LightSpeed QX/i (GE Healthcare) or SOMATOM Sensation 4 (Siemens AG Medical). Scanning was done supine in the craniocaudal direction during the inspiration phase, from lung apices to below the level of the adrenal glands. Contrast enhancement with 100 mL of iopromide (Ultravist 300; Schering AG) was used, and volumetric CT examination of the chest was obtained. Images were reviewed using lung, mediastinal, and bone windowing.
Survival Analysis
Overall survival was the endpoint of this study. Overall survival time was calculated from the date of pathologic diagnosis of lung cancer to the date of death as a result of any cause. Details of the verification of dates of death have been described previously (15).
Statistical Analysis
Frequency distributions of selected variables were compared by Fisher exact tests. Cut points were established by means of exploring martingale residual plots and the minimum P value approach.
Actuarial survival curves and probabilities were generated using the method of Kaplan and Meier. Significance of the difference between groups was assessed using the log-rank test. A multivariate model was built using Cox proportional hazards regression.
All tests were 2-sided and were performed at the 5% level of significance by using PASW for Windows, version 18.0 (SPSS Inc.).
RESULTS
Patients and Treatment
Detailed demographic and clinical information are presented in Table 1. Patients had a median age of 71 y (range, 32–92 y). There were 58 men and 42 women. The histologic type was adenocarcinoma in all cases. Although histology results were available for all patients, the lack of some clinical data or an inconclusive pathology report regarding the surgical margin and nodal involvement for some patients would not allow confident clinical staging. Appropriate clinical staging was achieved for 64 patients.
Surgery was performed in 42 (42%) patients. The breakdown by the extent of resection was as follows: pneumonectomy, 2 patients; lobectomy, 24 patients; and wedge resection, 16 patients. Mediastinal lymph node dissection was performed in 35 (83.3%) of the 42 patients. An additional component of rib resection was performed in 4 patients. Of the 42 patients with surgery, adjuvant therapy was administered postoperatively in 13 patients: 11 patients received radiation therapy, and 2 patients received concurrent radiation–chemotherapy. Forty-one patients received radiation therapy; 33 (80.5%) of those patients underwent concurrent chemotherapy. Seventeen patients were treated with chemotherapy alone.
At the end of this investigation, there was no patient alive. The 12-, 24-, 36-, 48-, and 60-mo survival rates were 84%, 69%, 60%, 57%, and 52.1%, respectively.
Tumor Characteristics
The median size of the lung neoplasm as measured on CT images or during examination of the surgically resected specimens (if available) was 2.7 cm (range, 1–5.4 cm). Regional lymph node involvement was pathologically investigated in 64 patients and proved to be involved in 36 patients (56.3%) of the 64. The presence of distant metastases was diagnosed in 10 patients (15.6%).
18F-FDG PET
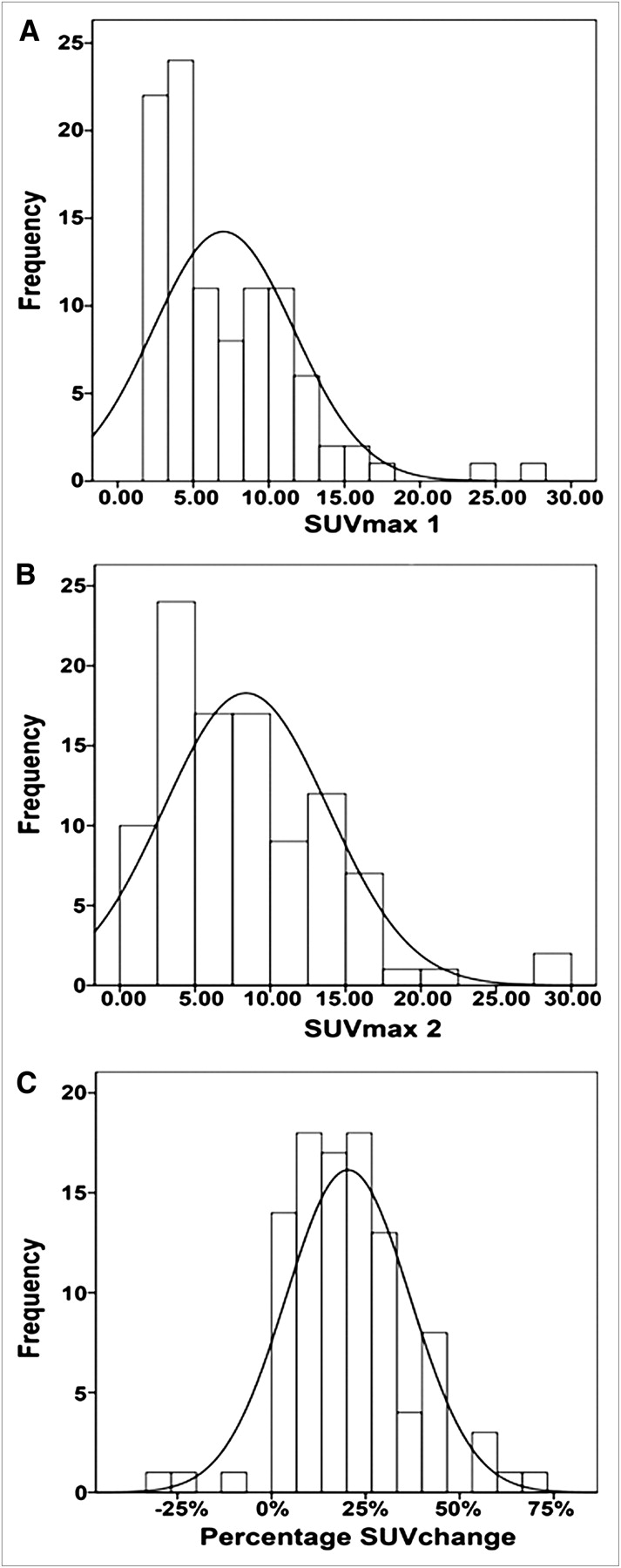
Patients had a median SUVmax1 of 5.5 (range, 1.7–27.1) and SUVmax2 of 7.2 (range, 1.8–29.9). When both values were compared, an increase in SUVmax over time was demonstrated in 90 (90%) patients, with no change in 7 (7%) and a decrease in 3 (3%) patients. The median of percentage change of SUVmax was 18.8% (range, −28.6%−66.7%). The distribution of SUVmax1 and SUVmax2 and the percentage change of SUVmax over time are shown in Figure 1.
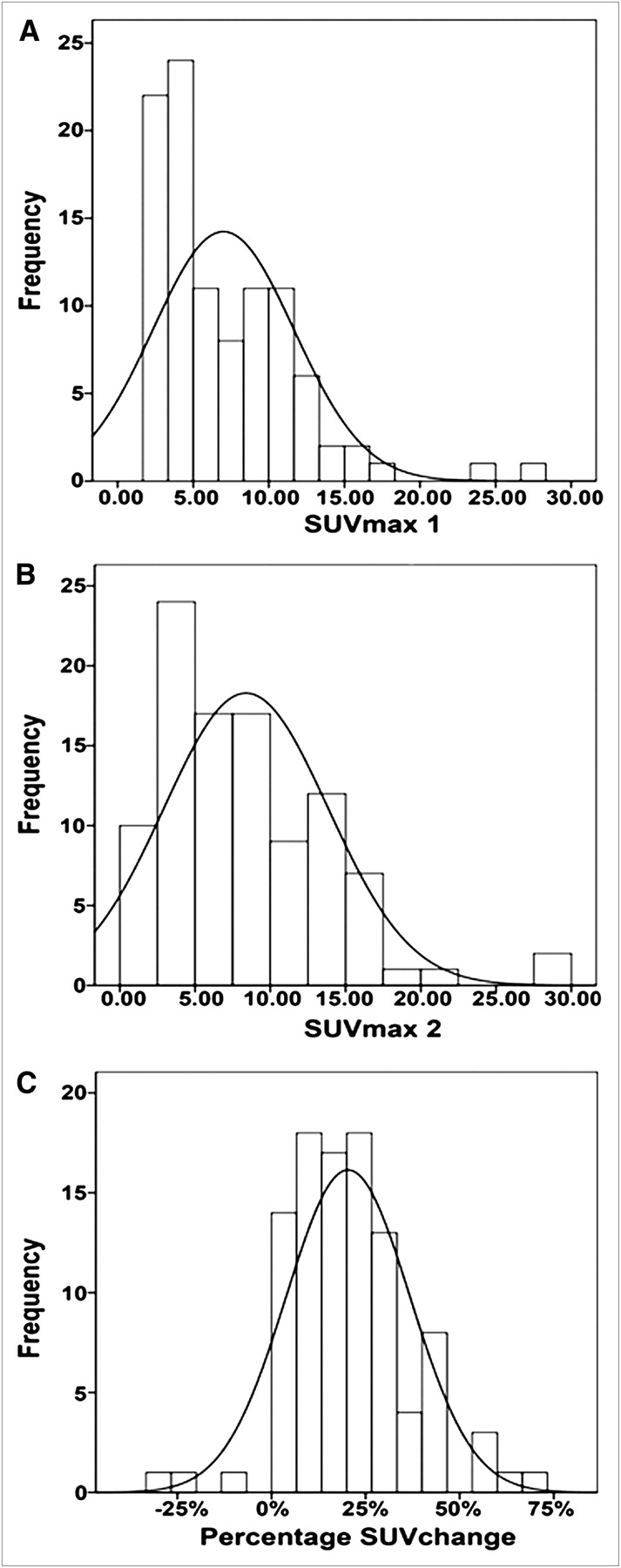
Histograms of distribution of SUVmax of tumor site on early images (A), SUVmax on delayed images (B), and percentage SUVmax change between early and delayed scans (C). Line represents gaussian fit to distribution.
Percentage Change of 18F-FDG Uptake
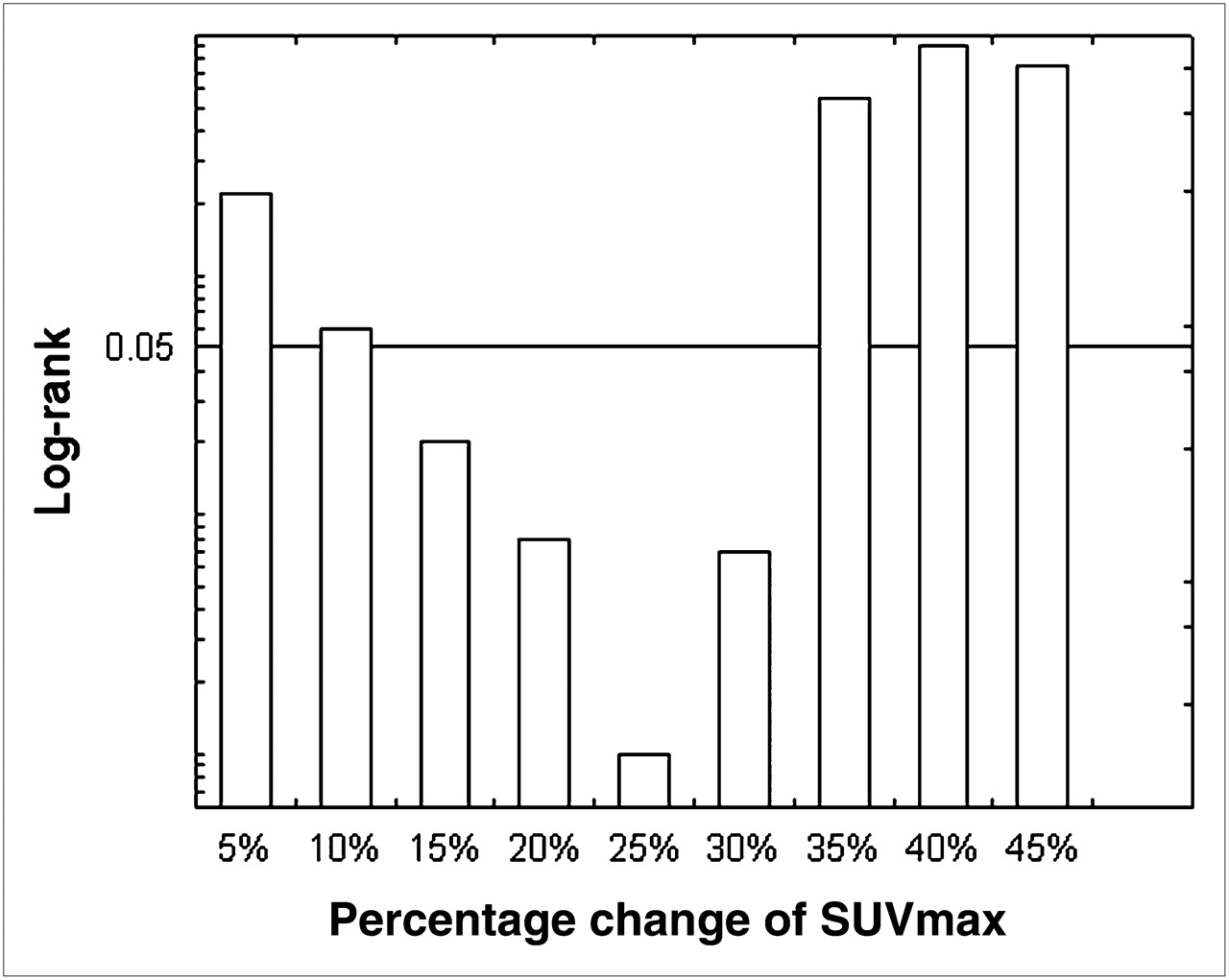
The discriminative value of various cutoff percentage changes of SUVmax for the 18F-FDG uptake by the primary neoplasm was analyzed (Fig. 2). In the analysis, cutoffs at 15%, 20%, 25%, and 30% showed significance, but 25% change was the most discriminative and yielded the minimum P value in the log-rank test. Therefore, 25% change was used as the cutoff in this analysis.

Relationship between various cutoff of percentage changes of SUVmax and their discriminative value for overall survival, as assessed by log-rank test.
Factors Associated with Prognosis in Univariate and Multivariate Analyses
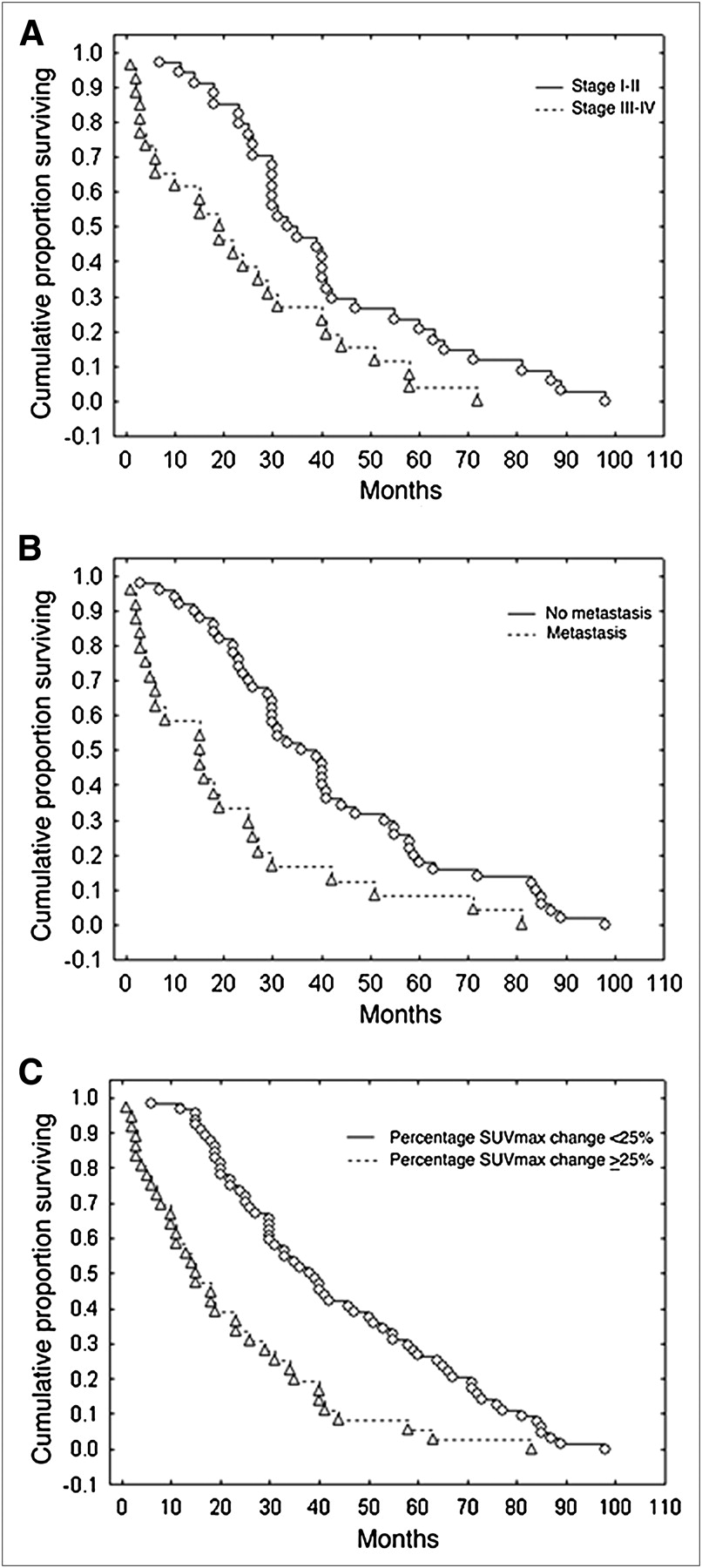
In the univariate analysis using the Kaplan–Meier method, for which each variable was treated as a categoric variable, all factors were associated with a statistically significant correlation to the overall survival (Table 2). Clinical stage, presence of metastasis, and percentage SUVmax change (Fig. 3) showed the most significant values (log-rank overall P = 0.001, 0.0005, and 0.0002, respectively [Fig. 4]).

Transaxial PET images of 2 patients at early (left) and delayed (right) scans. Histopathology, in both cases, was moderately differentiated adenocarcinoma. Percentage change of SUVmax, between early and delayed scans, measures 4.3% for patient in A and 36.4% for patient in B. Survival for patient in A was 28 mo, and for patient in B it was 12 mo.

Kaplan–Meier survival plots of patients with adenocarcinoma of lung by clinical stage (stages I–II, compared with stages III–IV, P = 0.001) (A), presence of metastasis (P = 0.0005) (B), and percentage change of SUVmax (dichotomized using value of 25%, P = 0.0002) (C).
Univariate Kaplan–Meier Analysis of Overall Survival in Patients with Lung Adenocarcinoma
Multivariable Regression Model
All prognostic factors with significance in the univariate analysis were included in the multivariate model to evaluate their interaction and joint effect on the overall survival. The adjusted Cox proportional hazards regression model revealed 4 factors to be independently correlated with the overall survival including platelet count, staging, metastatic state, and percentage SUVmax change over time. Table 3 presents the parameters and the significance of the obtained estimators.
Multivariate Cox Regression Analysis of Overall Survival in Patients with Lung Adenocarcinoma
DISCUSSION
Lung cancer remains the leading cause of cancer-related death. Validating new prognostic factors may be of value in the clinical course and management. PET quantitative methods as prognostic factors have been discussed before (16–18). However, the dynamic change in 18F-FDG uptake with time, to the best of our knowledge, has not been evaluated in lung cancer as a prognostic factor. The data obtained in this study show that more than a 25% increase in SUVmax over time in primary lung cancer is a strong marker of poor prognosis in patients with lung adenocarcinoma. Patients with more than a 25% increase in SUVmax had a median survival of 15 mo, compared with 39 mo for those with less than a 25% increase in SUVmax.
We selected a percentage increase of SUVmax of 25% as the cutoff point for the analysis of prognosis because it yielded the minimum P value on the log-rank test.
A variety of clinical and pathologic factors has been reported to be associated with prognosis for patients with lung cancer, such as age, sex, tumor size, lymph node and metastatic status, tumor differentiation, disease stage, and serum levels of calcium, albumin, hemoglobin, platelet and white blood cells (19–21). A univariate analysis of our data showed these factors to be, together with the percentage SUVmax change over time, significantly related to survival. However, multivariate analysis showed that, of these clinicopathologic factors, only disease stage, tumor differentiation, percentage SUVmax change over time, and platelet count were associated with survival. The clinicopathologic results are in agreement with other studies (22–24).
The point estimates in the multivariable Cox proportional hazards model suggest that percentage change in SUVmax over time may be as significant as common clinical parameters, including staging, metastatic status, and platelet count.
In our study, analyzing SUVmax and exact executions of the protocols revealed high reproducibility. Furthermore, the current analysis of SUVmax uptake in the initial diagnosis and its change over time could be associated with the neoplasm aggressiveness. Malignant tumors are characterized by progressive growth (25). Haberkorn et al. studied 2 groups with low and high 18F-FDG uptake. In the group with high 18F-FDG uptake, the degree of 18F-FDG accumulation was correlated significantly with the proliferation rate (26). A positive correlation seen between 18F-FDG uptake and the fraction of proliferating cells in human neoplasms more likely reflects the aggressiveness of tumors, which is correlated secondarily with the proliferative activity (27).
Dual-phase 18F-FDG PET has been used to improve the diagnostic efficacy and to differentiate benign from malignant lesions (28–30). Although many theories have explained the mechanism of 18F-FDG uptake by tumors and its accumulation over time, the molecular basis of 18F-FDG uptake is still under investigation. These theories include high glycolytic enzyme activities in both the transmembrane glucose transporter protein (particularly glucose transporter protein-1) and the cytosol (particularly hexokinase-II) and also by underexpression of glucose-6-phosphatase (31). Higashi et al. suggested that 18F-FDG accumulation on delayed PET is related to hexokinase-II expression and could indicate the phosphorylation rate (9). Demura et al. reported a positive correlation in dual-time-point change with the degree of cellular differentiation in patients with lung cancers (32). A stable or decrease in 18F-FDG uptake over time has been noted in 10 patients in this study. In theory, this can be due to degree of tumor differentiation and the cellular composition of neoplasms.
The significance of assessing SUVmax in a single time point in primary lesions has been wildly debated. Hoang et al. showed no correlation between survival and SUVmax. However, their study group was limited to patients with advanced non–small cell lung cancer (33). Vesselle et al. in another study revealed no prognostic information of 18F-FDG uptake by lung cancer. Vesselle et al. included patients with non–small cell lung cancer of different histology (34). On the other hand, several studies reported a significant correlation between 18F-FDG uptake and prognosis (12,35). However, these studies have been criticized with overestimation in the statistical significance due to the failure to account for the effects of multiple testing (36). We believe that measuring percentage change in SUVmax overcomes many of factors limiting SUV measurements. These limitations include blood glucose levels, body weight, and partial-volume effect (37). Furthermore, differences in the 18F-FDG dose, time of scanning, reconstruction algorithms, filters, scanner characteristics, sinogram noise, and quantification methods might lead to (structural) interinstitutional SUV differences when depending on single SUV measurements (38). Thus, we proposed that measuring SUVmax change over time is more feasible and reproducible than depending on single SUV detection.
The known 18F-FDG PET limitations in lung cancer including false-negative results due to small-sized tumors and bronchoalveolar type of lung cancer (39) were not encountered in our study.
Several investigators have speculated that SUV is correlated with cellular proliferation or biologic factors and may be related to the metastatic potential of the tumor (9,40). Our analysis indicated that patients with metastases showed slightly higher percentage SUVmax changes over time than patients without metastases. The differences did not reach a significant level in our study, maybe because of the small number of cases with metastases. Further studies with larger number of patients may clear up this point.
A limitation in our study was maintaining the exact time interval for rescanning the lung. However, taking into consideration that the average time was 30 min with ±6 min variability and our focus on the percentage change in SUVmax, we believe that the effect was limited. Moreover, the patient selection was based on a 18F-FDG PET database; therefore, prognostic factors not directly related to 18F-FDG PET may suffer from selection bias. Another limitation was the fact that some patients did not undergo extensive surgical sampling. In addition, the survival data were calculated on the basis of date of death as a result of any cause, which inevitably included a few patients who died of other reasons. It is conceivable that the result would be even better if the cause of death could have been limited to the lung cancer, and such analysis should be performed in future analyses, if possible. Finally, because this was a retrospective investigation, we could analyze only the data from previous studies, which were all done with the 60- and 90-min protocols. The 60- and 90-min protocols were initially used simply because we tried to reduce the possible patient movement between the scans as much as possible so that early and delayed images could be easily compared. However, because we never had the chance to try other protocols, the results obtained from time points other than the 60 and 90 min of PET might be slightly different from our results. A prospective study on a larger scale should be conducted to ensure better control of all the factors and to avoid possible overestimation of the prognostic factors.
CONCLUSION
Percentage SUVmax change over time in a pretherapy 18F-FDG PET scan is a strong predictor of mortality in patients with lung adenocarcinoma. This predictor proved to be powerful on univariate analysis and independent on the Cox regression model. Therefore, we anticipate that dual-phase 18F-FDG PET with measurement of the percentage SUVmax change may significantly affect the management of patients with lung adenocarcinoma and could be complementary to other well-known factors. These results remain to be confirmed in a larger prospective study.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 21, 2009.
- Accepted for publication January 5, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prediction of Survival by [18F]Fluorodeoxyglucose Positron Emission Tomography in Patients With Locally Advanced Non-Small-Cell Lung Cancer Undergoing Definitive Chemoradiation Therapy: Results of the ACRIN 6668/RTOG 0235 Trial
- Underestimated Role of 18F-FDG PET for HCC Evaluation and Promise of 18F-FDG PET/MR Imaging in This Setting