


Abstract
The objective of this study was to evaluate the in vivo assay of folate receptors in nonfunctional pituitary adenomas using preoperative 99mTc-folate SPECT/CT and Western blot analysis (WBA) of surgical specimens as the standard. Methods: Fifty-six patients (29 men, 27 women; age range, 29–82 y) with clinically nonfunctional pituitary adenomas on MRI underwent preoperative imaging using 666 MBq (18 mCi) of 99mTc-folate. SPECT/CT images and whole-body and lateral head planar images were acquired approximately 2 h after injection. Surgical resection took place within a week. WBA on a portion of the excised specimens assessed folate receptor expression in 49 patients. Attenuation-corrected 99mTc-folate SPECT/CT images were assessed qualitatively and quantitatively (maximal adenoma counts to background), with WBA as a standard. Results: Integrated CT was useful for uptake localization and assisted region-of-interest placement. Qualitative interpretation of planar imaging yielded a sensitivity of 81% and specificity of 72%. Qualitative SPECT/CT yielded a sensitivity of 94% and specificity of 61%. Receiver-operating-characteristic curve analysis of quantitative uptake yielded a tumor-to-background cutoff ratio of 3.5, with a sensitivity of 81% and specificity of 83%. Scalp uptake yielded consistent results (over the brain, neck, and choroid plexus) for background when SPECT/CT misalignment artifacts were avoided. Detection of pituitary uptake on anterior–posterior and lateral images was hampered by facial uptake, which varied between patients. Conclusion: SPECT/CT of 99mTc-folate is an accurate method of assaying folate receptors in vivo and may provide a quantitative marker for identifying folate receptor–positive tumors. This method may also prove beneficial in selecting patients for folate-targeted therapy of clinically nonfunctional pituitary adenomas, for which there is currently no medical therapy.
Pituitary adenomas are frequently occurring intracranial tumors that can cause significant morbidity (1–3). Functional pituitary adenomas produce specific hormones and cause life-threatening diseases, infertility, and impotence. Nonfunctional pituitary adenomas, the most common pituitary tumors, do not secrete hormones and cause damage through compression of regional structures. Unlike functional pituitary adenomas, there is no available effective medical therapy for nonfunctional adenomas. Though initial diagnosis of the adenoma may be delayed because of lack of symptoms, nonfunctional adenomas are easily detected by MRI and are enhanced with MRI contrast. Surgery to remove these adenomas is the treatment of choice but can be challenging because of their proximity to the carotid artery and optic nerve and their invasiveness. Some residual adenoma may remain after surgery, and patients are at risk of recurrence for several years after surgery (4).
Investigation of the molecular changes that contribute to the development of pituitary adenomas has shown that the folate receptor α (FRα), a high-affinity folate transporter, is significantly overexpressed in clinically nonfunctional adenomas but not in functional adenomas (5). It was also found that FRα expression in nonfunctional pituitary adenomas was uniform throughout the adenoma and varies significantly between patients (5). Elevated levels of FRα promote folate acid uptake, alter signal transduction (6–9), and facilitate growth of nonfunctional pituitary adenomas in vitro (10,11). The ability to assay folate receptors noninvasively may be valuable as a prognostic measure of tumor aggressiveness and provide a tool for the selection of nonfunctional pituitary adenomas that may respond to folate-targeted therapy. Without such a diagnostic test, obtaining this information would require immunohistologic or molecular examination of specimens obtained at surgery.
Radiopharmaceuticals have been investigated as scintigraphic imaging agents for the in vivo assay of folate receptors in clinical studies. 111In-diethylenetriaminepentaacetic acid–folate scintigraphy has been investigated as a tool for differentiating between malignant and benign ovarian masses (12). Scintigraphy with 99mTc-EC20 (FolateScan; Endocyte, Inc.) has been investigated in various tumors that are folate receptor–positive (FR+). Preclinical studies in a rodent model indicated that 99mTc-EC20 uptake was specific and proportional to folate receptor expression levels in tumor cells, linear with tumor size, and independent of tumor location (13). In a clinical study, tumors with 99mTc-EC20 uptake were identified in 68% of the 154 patients studied with proven or suspected cancer (14).
The objective of this study was to evaluate the in vivo assay of folate receptors in nonfunctional pituitary adenomas using preoperative 99mTc-EC20 planar scintigraphy and SPECT/CT. Western blot analysis (WBA) using a polyclonal antihuman antibody of surgical specimens was used as the reference for comparison. The sensitivity and specificity of each diagnostic modality has been determined on the basis of a qualitative interpretation of results as compared with those from Western blot. Quantitative analysis based on tumor-to-scalp count ratios extracted from the SPECT/CT scans was also examined, and a receiver-operating-characteristic (ROC) curve was created to examine the optimal cutoff ratio.
MATERIALS AND METHODS
Patient Population
Fifty-six patients (age range, 29–82 y; mean age, 55 y; 29 men, 27 women) with clinically nonfunctional pituitary adenomas were evaluated. Each patient presented with a visual deficit and a hormone profile consistent with clinically nonfunctional pituitary adenoma, and the presence of tumor was confirmed by MRI. After a medical evaluation and pregnancy test (if applicable), the patients were scheduled for surgery to remove the tumor, with 99mTc-EC20 scintigraphy before surgery. After surgery, WBA was performed on a portion of the excised surgical specimens of 49 patients to detect folate receptor expression (WBA could not be obtained for 7 patients). The first 6 patients were also included in another, multisite study of various tumor types (14). The study protocol was approved by the Emory University Institutional Review Board, and all patients gave written informed consent before participation.
Radiopharmaceutical Preparation and Injection
Folate-labeled 99mTc-EC20 for injection was packaged as a sterile lyophilized powder in a single-reagent vial containing the components EC20 (100 μg), sodium α-D-glucoheptonate dihydrate (80 μg), and tin (II) chloride dihydrate (80 μg). 99mTc-EC20 was prepared in the hospital radiopharmacy by adding up to 1,850 MBq of 99mTc-sodium pertechnetate into the vial and heating the vial in a boiling water bath for approximately 18 min. The radiochemical purity of 99mTc-EC20 was determined by thin-layer chromatography at the time of preparation and was required to be 90% for administration (13–15).
Patients were asked to discontinue taking folic acid supplements 2 d before the imaging study. The patients underwent 2 injections via a free-flowing intravenous catheter in an upper extremity vein. The first injection contained 0.5–1 mg of folic acid. The second contained 1–2 mL of folate (0.1 mg) labeled with 666 MBq of 99mTc (99mTc-EC20). The purpose of the first injection was to saturate the folate receptors in normal tissues, thus reducing the extratumor uptake of 99mTc-EC20. The time delay between the first and second injections was 3 min for the first 7 patients and 30 min for the remainder of patients. These changes in protocol were suggested by the manufacturer, but this study does not provide sufficient data to evaluate the optimal time between injections or the dosage of nonlabeled folic acid.
Imaging
Imaging began approximately 2.5 h after injection, with each patient undergoing whole-body imaging and SPECT/CT (average time for SPECT/CT, 2.8 h after injection). Lateral static images of the head were obtained for all but the first 6 patients. Twenty-three patients underwent a second SPECT/CT study (average time, 4.7 h after injection) before completion of their evaluation to determine whether changes in the distribution of 99mTc-EC20 would affect uptake ratios or study interpretation between early and late scans. All images were acquired on a dual-detector, large-field-of-view SPECT/CT system equipped with low-energy high-resolution parallel-hole collimation and using a 140-keV, 20% energy window (VG/Hawkeye; GE Healthcare). Images were reconstructed, displayed, and evaluated on a clinical nuclear medicine workstation (Xeleris 2.0; GE Healthcare).
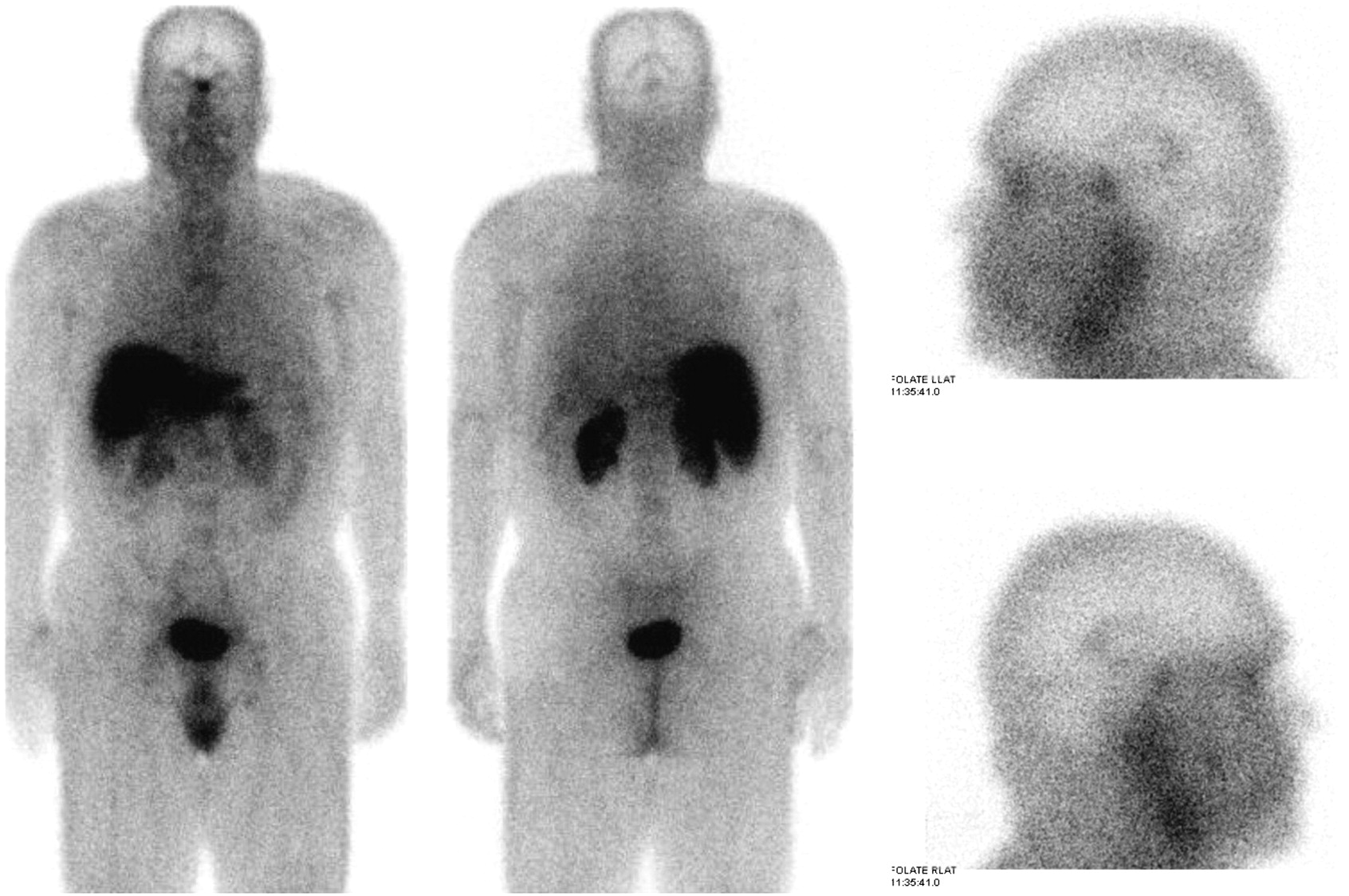
Whole-body images were acquired in a 1,024 × 256 matrix (2.4 mm/pixel) from head to mid thigh using continuous motion at 15.5 cm/min (giving an effective exposure time of 131 s). Lateral head static images were acquired in a 256 × 256 matrix, with a 2.0 zoom (1.1 mm/pixel) for 5 min. Planar images of a FR+ patient are shown in Figure 1.

Whole-body and lateral head static images of patient with FR+ nonfunctional pituitary adenoma. Pituitary adenoma, which had estimated volume of 2.7 mL, is clearly visible in most images. Uptake is also seen in liver, kidneys, bladder, and choroid plexus. LLAT = left lateral; RLAT = right lateral.
For SPECT/CT, CT images were acquired first using a slow-rotation low-radiation dose that took 5–7 min (1-cm-thick slices, 256 × 256 matrix, 1.7 mm/pixel), from the top of the head to the patient's shoulders. SPECT images were acquired immediately on completion of the CT, with a 1.28 zoom (128 × 128 matrix, 3.4 mm/pixel) using a continuous orbit with 120 projections (15 min total acquisition time). SPECT images were reconstructed with and without attenuation correction using ordered-subset expectation maximization (6 iterations, 10 subsets). A 3-dimensional Butterworth filter (critical frequency of 0.6 1/cm, power factor of 10.0) was applied after reconstruction. SPECT/CT images of a FR+ and folate receptor–negative (FR−) patients are shown in Figure 2.

SPECT/CT images and registered contrast-enhanced MR images of 2 patients with nonfunctional pituitary adenomas: FR+ tumor (A) with estimated volume of 6.0 mL and FR− tumor (B) with estimated volume of 3.9 mL. Imaging times were 2.9 and 2.5 h, respectively, after injection. From top to bottom, panels show SPECT, SPECT/CT fusion with low-dose integrated CT, and contrast-enhanced MR images. Tumor location is indicated with arrow on MR images.
Surgical Resection and Tumor Evaluation
Transsphenoidal surgical resection took place within a week in all but 2 of the patients, who had delays of 2 and 6 wk. After surgery, WBA was performed on a portion of the excised surgical specimens of 49 patients to detect folate receptor expression (WBA could not be obtained for 7 patients). The WBA was performed as follows. Thirty milligrams of the excised tissue (each tumor is excised in several pieces weighing 100–1,000 mg) were homogenized and the protein concentration measured. Equal portions of the homogenized samples (20 μg) were loaded onto a 15% acrylamide–sodium dodecylsulfate gel, and proteins were resolved by electrophoresis. The proteins were then transferred into nitrocellulose, and FRα was detected using a polyclonal antihuman FRα antibody. The antibody was produced by rabbits immunized with a recombinant FRα-glutathione S-transferase fusion protein (16). The FRα protein was visualized using a horseradish peroxidase–conjugated antirabbit IgG as the secondary antibody (catalog no. A-4914; Sigma/Aldrich) and the enhanced chemiluminescence WBA system (catalog no. RPN2132; GE Healthcare) on Biomax ML film (Kodak). The films were scanned with a densitometer, and the absorbance of the FRα protein bands was measured using UN-SCAN-IT Gel Analysis Software (Silk Scientific, Inc.). The software subtracts the background for each film and normalizes it to a standard with known high folate receptor expression (included with each measurement). The Western blot scored the presence of FRα in the tumors as 1 (absent: 0.1%–25% of the density of the standard), 2 (moderate: 26%–70%), or 3 (marked: 71%–100%). These cutoff percentages were derived from our experience with Western blotting. WBA films of the patients whose images were shown in Figure 2 are shown in Figure 3. The absorbance value of each tumor sample indicated the FRα protein expression per 20 μg of total protein.

Western blot correlation for the 2 patients in Figure 2: FR+ tumor (A) and FR− tumor (B). Western blot of markedly positive standard is shown on left and that of sample taken from excised tumor is on right.
Image Analysis
Planar images (whole-body and lateral head static) were read by an experienced nuclear medicine physician who documented areas of uptake, with particular note of the pituitary area. SPECT/CT images were read using an integrated display that showed the attenuation-corrected and noncorrected SPECT, CT, and fused images. The same grading scale (absent, moderate, and marked) as was used for the Western blot was used to note tumor uptake. For sensitivity and specificity analysis, the absent category was considered to be a negative result, whereas moderate and marked assessments were considered a positive result representing the presence of FRα expression.
Quantitative analysis was applied as a count ratio of tumor-to-background counts in the attenuation-corrected SPECT images. Tumor counts were measured by locating the SPECT slice with the greatest tumor uptake and extracting maximal counts from a small region of interest (ROI) drawn over the tumor. Where tumor uptake could not be noted, the CT image was used to locate the tumor or to estimate the tumor location, and an ROI was placed there. The CT image on this system, however, suffered from slices that were too thick at 1 cm to allow the CT image to be used to outline the tumor completely. Scalp uptake was evaluated by extracting maximal counts from an ROI drawn over a lateral or inferior area of the scalp (chosen to avoid attenuation-correction artifacts caused by misalignment of the SPECT and CT images). The choroid plexus, cortex, and neck were investigated but proved to be too variable (choroid plexus and neck) or too low in counts (cortex) for use as background.
RESULTS
Planar Images
Although many tumors were clearly visible in the whole-body and lateral head static images (Fig. 1, for example), the 99mTc-EC20 uptake was often obscured by extratumor uptake, primarily from the sinus area. This made determination of tumor uptake difficult in several patients. Other areas of uptake included the liver, kidneys, and choroid plexus in all patients. Incidental areas of uptake in some patients included the bone marrow and inguinal lymph nodes. Extratumor uptake prevented accurate measurement of counts in the planar images. Comparison of the physician's interpretation of the tumor uptake from the planar images with the WBA is shown in Tables 1 and 2. The qualitative assessment of the static whole-body and lateral head images yielded a sensitivity of 81% and a specificity of 72% using the WBA as a standard.
Qualitative Interpretation of Planar Scintigraphy
Planar Scintigraphy Sensitivity and Specificity
SPECT Images
Qualitative analysis of the SPECT/CT images by the experienced nuclear medicine physician noted that the CT image helped with localization of the tumor, particularly in patients with little tumor uptake. Attenuation correction made the tumor much more readily visible, as might be expected because it is an interior structure, particularly important in patients with marked facial or sinus uptake. Comparison of the physician's interpretation of the tumor uptake from the SPECT/CT image with the WBA is shown in Tables 3 and 4. The qualitative assessment of the SPECT/CT images yielded a sensitivity of 94% and a specificity of 61% using the WBA as a standard.
Qualitative Interpretation of SPECT/CT
SPECT/CT Sensitivity and Specificity
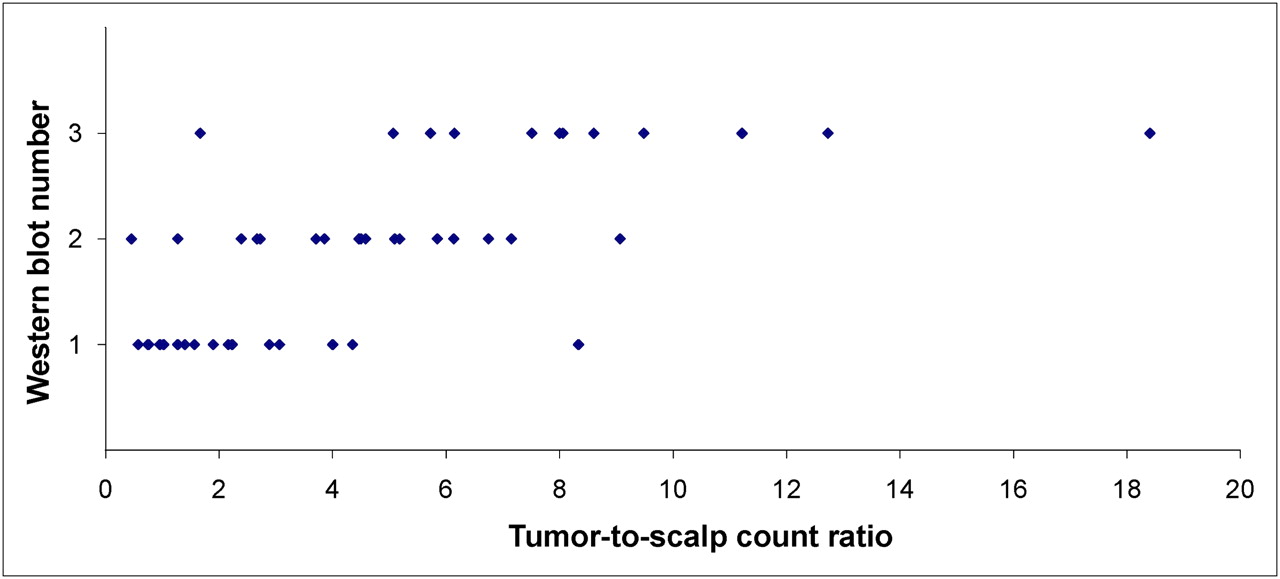
Comparison of the tumor-to-scalp (tumor-to-background) count ratios with the qualitative assessment (Fig. 4) showed little overlap of the count ratios of patients noted as having a marked or moderate tumor uptake. There was more overlap of count ratios between the patients noted with absent (1 on the y-axis) tumor uptake. Comparison of the same ratios to the Western blot results showed that the count ratios were not as delineated by category as they were in the qualitative assessment (Fig. 5). This result is to be expected because the qualitative assessment did not agree with the WBA in all cases (Tables 1 and 3).
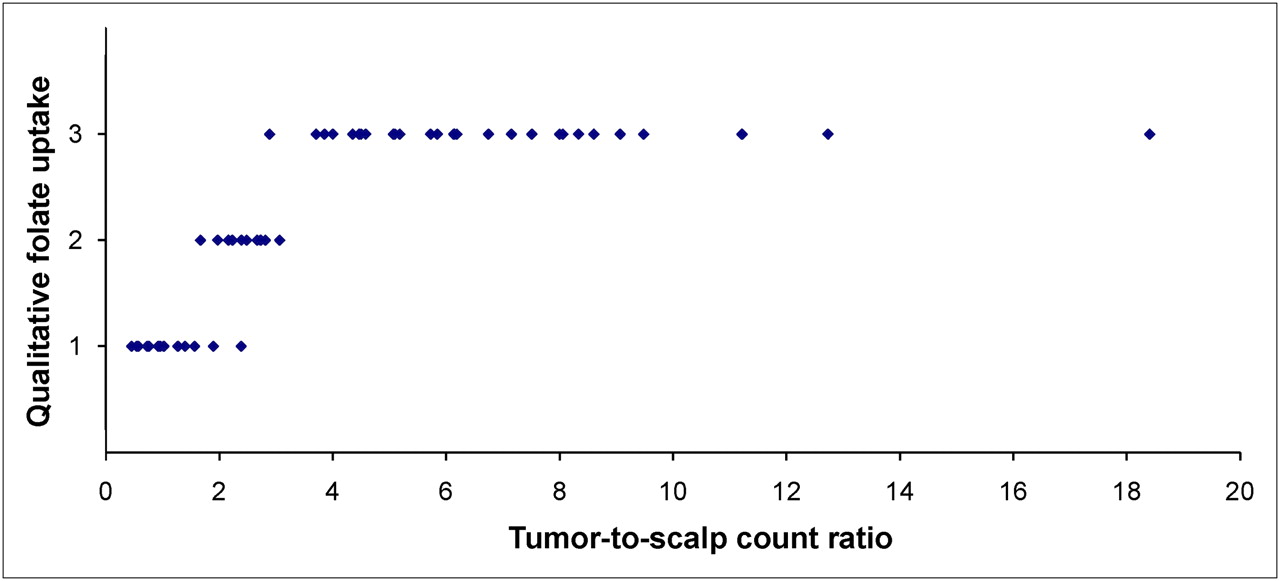
Qualitative assessment of tumor uptake of 99mTc-EC20 (as scored by physician on 3-point scale), compared with tumor-to-scalp count ratio. Little overlap of in count ratios is seen in patients with uptake that was noted as moderate (2) and marked (3), but the delineation of the absent (1) and moderate groups is not as striking.

Western blot versus quantitative assessment of tumor uptake. FRα assessment by WBA is compared with tumor-to-scalp ratio. Count ratios are not as well delineated by category as they were in qualitative assessment.
Early and late SPECT/CT images (23 patients) were scored exactly the same by the reviewer, with 2 exceptions. Both exceptions were for patients whose images were scored as “moderate uptake” on the early but changed to “absent uptake” on the late images. Comparison of tumor-to-scalp ratios from the early and late images showed that tumor-to-background tended to decrease slightly over time, with an average decrease in the ratio of 10% (SD of 17%) in 15 (of the 23) patients that the reviewer scored with moderate or marked tumor uptake.
Use of the tumor-to-scalp ratio of 99mTc-EC20 as a quantitative marker of the presence of folate receptors was investigated with ROC curve analysis, varying the tumor-to-scalp count ratio threshold for a positive result and subsequently calculating the corresponding sensitivity and specificity. The ROC curve is shown in Figure 6. A tumor-to-scalp cutoff ratio of 3.5 resulted in a sensitivity of 81% and specificity of 83% (Table 5).

Tumor-to-scalp count ratio ROC curve. ROC curve was produced by varying the tumor-to-scalp count ratio as a threshold for determining whether tumor was positive for FRα. Ratios are given in red next to corresponding point on curve.
Quantitative SPECT/CT Sensitivity and Specificity
DISCUSSION
The in vivo diagnosis of tumor receptor expression allows selection of tumors that may be treatable by targeted therapy, such as a folate drug conjugate or folate-based radionuclide therapy (17–20). Normal tissues, lacking in folate receptors, could be spared toxicity associated with nontargeted drug delivery. Folate-based imaging agents, including radiopharmaceuticals, may provide novel diagnostic testing by locating and assessing the receptor density of FR+ tumors (21–23). Identification of tumors by imaging before surgery could be clinically significant should the FR+ lesions have a different natural history than the FR− lesions or should effective medical therapy become available for FR+ lesions (17–20).
Several labeled folate conjugates have been investigated for scintigraphic imaging; 67Ga (24) and 111In-diethylenetriaminepentaacetic acid (12,25,26) have been used but are costly and have long half-lives. 99mTc, with its 6-h half-life and optimal γ-energy, is well suited for delivering the counting rates desired for same-day SPECT. Different chelators have been used to label 99mTc with folate (15,27–31). 99mTc-EC20 is the only 99mTc-based agent that has been used in a clinical study to date (14). This is a second clinical report with99mTc-EC20 and the first in which it has been exclusively used to evaluate nonfunctional pituitary adenomas–benign brain tumors.
The purpose of receptor imaging in the management of pituitary tumors is not to localize or diagnose them (both investigations can be better performed with other imaging tools) but to identify the tumors that express the receptors—such that targeted therapy can be applied to that subset—allowing personalized medicine that decreases toxicity and increases efficacy. Hence, receptor imaging is less important in tumors that always express receptors.
Whereas a previous clinical report with 99mTc-EC20 noted uptake in the choroid plexus in only 4 of 155 patients (14), uptake was noted in varying degrees in the SPECT/CT images of all the patients in this study. The apparent discrepancy is probably due to the fact that in the previous study (14) SPECT or lateral images of the head were obtained for only a few of the patients (the study dealt with different tumor types and SPECT was targeted at the known or suspected tumor). As with the pituitary adenomas, the choroid plexus was more easily visualized on the attenuation-corrected SPECT images than on the planar images. The finding of 99mTc-EC20 in the choroid plexus is in agreement with a preclinical study of 99mTc-His-folate, which also reported the presence of 99mTc-EC20 in the choroid plexus (32). In addition, the choroid plexus is known to express folate receptors (33). The uptake in the choroid plexus is probably not due to a small amount of free 99mTc-pertechnetate, as was speculated in an earlier study (14), because uptake was not noted in the stomach or thyroid (as would be expected with free 99mTc-pertechnetate).
Planar scintigraphy, evaluated by an experienced physician, yielded a sensitivity of 81% and a specificity of 72% and was hampered by the presence of facial and sinus uptake in some patients, lowering the confidence in the interpretation. The addition of SPECT/CT dramatically raised the sensitivity (94%) of a qualitative interpretation but also lowered specificity to 61%. Quantitative evaluation of SPECT/CT tumor-to-scalp count ratios after selecting a tumor-to-scalp cutoff ratio of 3.5 based on ROC curve analysis substantially improved the specificity of SPECT/CT to 83%, with a sensitivity of 81%.
Although the gain in quantitative evaluation of SPECT/CT was modest, it is possible that it would be useful in planning for treatment by giving a more accurate assessment of the receptor density. The work described here was done on a first-generation SPECT/CT scanner. Use of a system with higher quality CT might improve the accuracy of the quantitation by making the ROI placement and selection of background areas less subjective. Correlation of the SPECT images with an MR image designed to complement the SPECT study would likely improve the quantitation by more accurately defining the tumor site.
An important factor that limits the accuracy of this study is that the SPECT images of the tumors are subject to partial-volume effects and, therefore, larger tumors may appear brighter in the images, simply because of their size (34). Compensation for partial-volume effects will likely require anatomic images that clearly delineate the tumor (35–38). Volumetric MRI with contrast may prove to be ideal for this, but unfortunately, all of the MR images cited in this work were obtained before the patient entered the study. Many of the scans were acquired at other institutions and were not available for a detailed review. To investigate the bias of the results in favor of higher counts in larger tumors due to partial-volume effect, MR images of a subset of the patients (n = 17) were used to estimate the size of the tumor by outlining the tumor in 3 dimensions (MIMVista Contouring; MIMVista Corp.). There was no correlation between the size of the tumor and any of the uptake measurements.
A delayed SPECT/CT acquisition, approximately 2 h after the initial, or early, acquisition, did not result in different qualitative diagnostic results. The late scans, as compared with the early SPECT/CT images, proved to have slightly decreased tumor-to-scalp count ratios. The administration of cold folate before administration of 99mTc-EC20 in this work followed the manufacturer's recommendations. The effects of this administration have been documented in preclinical studies with other folate-based radiopharmaceuticals (24,26), but a study designed to test the hypothesis behind giving the cold folate (that it will reduce the uptake in normal tissue, increasing tumor–to–soft-tissue contrast) for 99mTc-EC20 would be beneficial.
Understanding the molecular basis of disease processes is essential to increase the efficacy and decrease the side effects of therapy through customization for individual patients. At present, the standard for assessing tumors is the histologic evaluation of excised tumor tissue. Histologic sampling, however, suffers when the sample contains material other than active tumor cells. This sampling bias could cause a reduction in the correlation between WBA and imaging. Another factor that may decrease the correlation is that 99mTc-EC20 will bind to both FRα and FRβ receptors (39), whereas WBA detects only FRα. This will also cause a decrease in the correlation by reducing the specificity calculated for the scan results in this study (without affecting the sensitivity). Because FRα and FRβ are both active in folate transport, an in vivo assay with 99mTc-EC20 scintigraphy may be better than immunohistochemistry (14,40) or even WBA for assessing real-time functioning activity of tissue-related folate receptors.
CONCLUSION
Molecular imaging, specifically 3-dimensional molecular imaging, has the bright prospect of assessing tumors in vivo. To our knowledge, this is the first study focusing on the use of 99mTc-labeled folates for imaging nonfunctional pituitary adenomas. Planar imaging of 99mTc-folate had good sensitivity and specificity (81% and 72%, respectively), with a positive predictive value of 83%. The addition of SPECT/CT improved the sensitivity (94%), at some loss of specificity (61%), by qualitative assessment. SPECT/CT improved the clinician's confidence in the location of any uptake noted and, consequently, the confidence of diagnoses. Quantitative analysis of the SPECT/CT image showed similar sensitivity to planar imaging (81%) but higher specificity (83%). Though the gain was modest, the higher specificity given by quantitative analysis of SPECT/CT images may prove useful when a diagnostic scan is used as a gateway to folate-based therapy by preventing the use of the therapy when it would not be beneficial. Improved quantitation through the use of a higher-quality CT scan or by the use of image fusion with MRI may further improve the utility of quantitation.
The data demonstrate that 99mTc-EC20 can successfully target FR+ pituitary adenomas and support the possibility that folate receptor imaging might be useful in selecting patients who would benefit from folate receptor–targeted therapy. SPECT allowed for definite separation of pituitary uptake from facial or glandular uptake that sometimes overlies the tumor on planar scintigrams. Integrated CT was valuable for tumor localization, and corrections based on the CT may prove valuable for quantification of the SPECT tracer uptake, and, in turn, for therapy planning and dosimetry calculations.
Acknowledgments
This work was funded in part by the National Institutes of Health grant Molecular Targeting and Imaging of Pituitary Adenomas (NIH NS051439-03). The radiopharmaceutical (99mTc-folate [EC20; FolateScan]) was provided by Endocyte, Inc.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 5, 2009.
- Accepted for publication August 13, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}