


Abstract
Although the diagnostic effectiveness of integrated PET/CT for staging of non–small cell lung cancer (NSCLC) has already been proven, it remains to be determined if tumor staging with combined metabolic and anatomic imaging is also cost-effective. The objective of this study was to evaluate from a payers’ perspective the cost-effectiveness of staging NSCLC with CT alone (representing the mainstay diagnostic test) and with integrated PET/CT. Methods: The study is based on 172 NSCLC patients from a prospective clinical study who underwent diagnostic, contrast-enhanced helical CT and integrated PET/CT. Imaging was performed at the University Hospital Ulm between May 2002 and December 2004. To calculate treatment costs, we differentiated among cost for diagnosis, cost for nonsurgical treatment according to the clinical diagnosis, and cost for surgical procedures according to the clinical tumor stage. Results: The diagnostic effectiveness in terms of correct TNM staging was 40% (31/77) for CT alone and 60% (46/77) for PET/CT. For the assessment of resectability (tumor stages Ia–IIIa vs. IIIb–IV), 65 of 77 patients (84%) were staged correctly by PET/CT (CT alone, 70% [54/77]). The incremental cost-effectiveness ratios per correctly staged patient were $3,508 for PET/CT versus CT alone. The incremental cost-effectiveness ratios per quality-adjusted life year gained were $79,878 for PET/CT vs. CT alone, decreasing to $69,563 assuming a reduced loss of utility (0.10 quality-adjusted life years) due to surgical morbidity. Conclusion: Cost-effectiveness analyses showed that costs for PET/CT are within the commonly accepted range for diagnostic tests or therapies. Therefore, reimbursement of PET/CT for NSCLC staging can be also recommended from an economic point of view.
Non–small cell lung cancer (NSCLC) represents one of the most common cancers. In Europe and the United States, NSCLC is the leading cause of cancer-related deaths in both men and women and is, therefore, a major economic issue for health care systems (1). Patients with limited disease (stages I and II) are candidates for curative surgery, followed by adjuvant chemotherapy in patients with stage II NSCLC. Patients presenting with stage IIIA disease usually receive chemo- or radiotherapy before resection of the primary tumor. Locally advanced (stage IIIB) or metastatic disease (stage IV) is considered to be incurable. Palliative treatment options for these patients include chemotherapy, radiotherapy, combined therapy approaches (stage IIIB), and epidermal and vascular epidermal growth factor receptor–directed drug regimens (2).
As treatment is determined predominantly by the initial stage of NSCLC, the accuracy of the diagnostic work-up is crucial for adequate therapeutic planning. If the diagnostic algorithm indicates advanced disease (stages IIIB or IV), unnecessary surgical procedures performed with a curative intent can be avoided, thereby increasing patients’ quality of life and reducing costs for futile therapeutic procedures (3,4). The standard diagnostic work-up is based on imaging with CT, but numerous studies have indicated that the addition of PET using the glucose analog 18F-FDG as the radiotracer exhibits higher diagnostic accuracy than CT alone and is also cost-effective when implemented into the diagnostic algorithm (5–9). Although reimbursement for PET has been provided in the United States since the early 1990s, the German Federal Joint Committee did not approve the use of PET for staging of NSCLC in the inpatient sector until December 20, 2005. On April 1, 2007, the approval was extended also to the outpatient sector (10).
The combination of the 2 imaging procedures provided by hybrid PET/CT scanners is relatively new, having been introduced in 2001 (11). The method combines the advantages of morphologic and functional imaging (12). Although new-scanner acquisitions in hospitals in European countries and the United States are now integrated PET/CT units, the decision-making process on the reimbursement of PET/CT has not yet been completed by the German Federal Joint Committee and other members of the European Union (13).
To provide input into the ongoing decision-making process on the reimbursement of PET/CT, this study evaluates from the payer's perspective the cost-effectiveness of integrated PET/CT versus CT alone.
MATERIALS AND METHODS
Study Design
Data were derived from a prospective clinical trial performed at the University Hospital of Ulm. The study protocol was approved by the ethics committee of the Medical Faculty of the University of Ulm, and all patients gave written informed consent to participate in this study. The patients were followed up until January 2007. Follow-up consisted of regular visits every 2–3 months within the first year after initial diagnosis of NSCLC.
Between May 2002 and December 2004, patients with suspected or histologically proven NSCLC were enrolled for pretherapeutic staging. The results of CT and PET/CT scans were made available to referring physicians. Therapeutic decisions were made by a tumor board consisting of at least 1 thoracic surgeon, 1 internal medicine physician, 1 oncologist, 1 chest radiologist, 1 radiation oncology specialist, 1 pathologist, and 1 nuclear medicine physician. Before a decision was made, all imaging findings (e.g., chest radiography, chest CT, abdominal CT, PET/CT, MRI, or ultrasound), along with histopathologic data on the primary tumor or metastatic sites and clinical condition (judgment of resectability or nonresectability based on cardiopulmonary function, comorbidity, and other factors), were reviewed.
Ultrasound-guided endoscopic biopsy or mediastinoscopy was performed in a limited number of patients to verify PET/CT findings that would preclude curative surgery (15). In the remaining patients, advanced disease (stages IIIb and IV) was confirmed by other means, including repetitive imaging with CT, MRI, or ultrasound and clinical follow-up. Stage IV disease was not further validated by histologic work-up in the case of severe comorbidity preventing resective surgery, such as significant reduction of cardiac or pulmonary function.
PET/CT was performed for each patient using a first-generation hybrid scanner installed in April 2002. For the purpose of this study, CT alone was analyzed separately. The cost, effectiveness, and cost-effectiveness of the 2 diagnostic modalities were compared. The economic analysis was performed from the payer's perspective; the analysis relied on a piggyback study design, which is common in health economic research. Piggyback health economic evaluations collect data on resource use and outcomes along clinical trials. This design has several advantages; for example, it increases the internal validity of studies but also requires careful sensitivity analyses, and appropriate analytic methods must be applied to obtain rigorous results (14–16).
Integrated PET/CT and Image Analysis
PET/CT was performed using a first-generation hybrid scanner (Discovery LS; GE Healthcare). Diagnostic multislice CT and PET emission data were acquired from the skull to the mid thigh in all patients. Image acquisition started 60 min after intravenous injection of 370–550 MBq of 18F-FDG. CT (140 kV; 160 mAs; slice thickness, 5 mm; increment, 4.25 mm; pitch, 1.5; and rotation time, 0.5 s) was performed after intravenous injection of 120 mL of contrast medium (Ultravist; Schering). An 80-mL bolus (flow, 3 mL/s) was injected, and the scan was started with a delay of 60 s. During the scan, an additional 40 mL were administered. CT was acquired in a middle respiratory position. Directly after CT, the PET acquisition was started. The acquisition time was 4.5 min per bed position (5–8 bed positions per patient). During imaging of the chest, patients were instructed to breathe shallowly. Each position had 35 scanning planes, with a 14.6-cm longitudinal field of view and a 1-slice overlap between scanning positions. PET images were reconstructed using CT attenuation correction and an ordered-subset expectation maximization algorithm.
All images were analyzed using an Entegra workstation (GE Healthcare). Scans were evaluated separately for CT alone and combined PET/CT. Readers were unaware of patient history and histologic diagnosis. CT scans were analyzed by 2 experienced radiologists, and PET/CT scans were analyzed by 1 radiologist and 2 nuclear medicine physicians using standard criteria for the evaluation of CT and PET/CT.
Data Collection
Data on CT alone, PET/CT, age, sex, choice of treatment, and time of death were recorded. In the case of a surgical intervention, pathologic results were also obtained. Costs for surgical and nonsurgical treatment according to the clinical diagnosis were based on the base rate of the University Hospital Ulm, which is close to the average in Germany and other European countries, and on the national frequencies of the relevant diagnosis-related groups (DRGs) in 2006 (17).
Calculation of Treatment Costs
To calculate treatment costs, we differentiated among cost for diagnosis, cost for nonsurgical treatment, and cost for surgical procedures. Diagnostic costs were based on the reimbursements of CT alone and PET/CT at the University Hospital Ulm. Costs of nonsurgical treatment were based on the reimbursement of the DRG for nonoperative treatment with radiotherapy (E08B) and 2 other DRGs for the treatment of malignant growth (E71A and E71B). Costs of surgical treatment consisted of different DRGs for surgical intervention, for example, lobectomy, thoracotomy, lung resection, and surgery combined with radiotherapy (E01A, E01B, E05A, E05B, E06A, E06B, and E08A, respectively). To estimate costs for surgical and nonsurgical treatment, the average reimbursement for surgical and nonsurgical treatment was calculated. Each DRG was weighted with the national frequency of the DRG in 2006 (17). Costs of additional treatment after an initial hospital stay were not included. For currency conversion between Euros and U.S. dollars, we used the official annual average exchange rate for 2006 (€1 = $1.2556).
Evaluation of Cost per Correctly Staged Patient
Cost-effectiveness analysis based on correctly staged patients was conducted for the subgroup of patients who underwent surgery, because histologic proof of the tumor stage could be obtained only for this group (77 patients). Effectiveness was assessed for each imaging procedure as the percentage of correctly staged patients. It was measured in 2 ways; first, according to the correct tumor stage (Ia/Ib, IIa/IIb, IIIa, IIIb, or IV), and second, according to the differentiation of resectable and unresectable tumors. For differential analysis, stages Ia/Ib, IIa/IIb, and IIIa were considered resectable, whereas stages IIIb and IV were considered nonresectable. A patient was considered as correctly staged by any diagnostic procedure if the clinical stage could be confirmed by pathologic results obtained from resected primary tumors and mediastinal lymph node sampling. In doing so, we followed the procedure of Klose et al., who used the same methodologic approach—that is, correctly staged patients as outcome measure (7).
To compare the diagnostic accuracy of the 2 imaging modalities, a McNemar test was performed (18). A P value below 0.05 was considered statistically significant. Incremental cost-effectiveness ratios (ICER) were calculated for PET/CT versus CT alone. To calculate ICERs, the difference in the diagnostic costs of the 2 strategies was divided by the difference in their effectiveness (19). The ICER reveals the cost per unit of benefit (here per correctly staged patient) of switching from one technology that is already reimbursed to another technology.
As a sensitivity analysis, we included an additional 38 patients with benign lesions, increasing the subsample to 115 patients. For the purpose of this sensitivity analysis, a “no malignancy” tumor stage was added to our cost-effectiveness analyses. We also performed another sensitivity analysis including those patients who did not undergo surgery. Patients with stage IIIB or IV had been staged correctly if they died within 1 y after staging, and patients with stage IIIA or below had been staged correctly if they survived 1 y after staging. For this sensitivity analysis, we included 156 patients of the full sample of 172 patients. Sixteen patients lost to follow-up were excluded.
Evaluation of Cost per Quality-Adjusted Life Year (QALY)
We also performed a different cost-effectiveness analysis (also known as cost-utility analysis outside the United States), which measures the benefit or health outcome in quality-of-life improvement, defined by the QALY. Thus, we measured costs per additional QALY gained. As a measure for quality of life, QALYs were used. In the absence of information on quality of life after surgery, we relied on a modeling approach that is commonly accepted in health economic research (20). We followed an approach from a study on NSCLC by the Centre for Health Economics Research and Evaluation at the Sydney University of Technology to determine quality of life after surgery. Accordingly, quality of life was defined as 1 for patients alive and 0 in the case of death. To account for surgical morbidity, we assumed a loss in quality of life of 0.15 QALYs for patients who underwent surgery (4).
To adjust for censoring due to the patients who were lost to follow-up, a Cox proportional hazards model was estimated (20). h0(t) is the unspecified baseline hazard for each individual. The model included the covariates age and gender. It also differentiated between patients with and without operative treatment (OP):
Initially, we also tried to stratify patients with operative treatment according to the pathologic results. However, this approach was dropped because of the low number of observations in each stage, especially in stages IIIB and IV. To test whether the influence of the covariates was significantly different from zero, a χ2 test was used. With this model, it was possible to correct survival times for censored observations (21). QALYs were then calculated for the average patients with and without surgical treatment. To take a conservative approach and to allow for a robust estimation, the calculation of QALYs has been limited to a time of 3 y, because several patients were lost to follow up after 3 y and the sample size was reduced substantially. However, we performed a sensitivity analysis for other periods, too.
For each diagnostic method, CT alone and integrated PET/CT, it was assumed in our model that treatment was chosen strictly according to the respective diagnostic result. A patient with stage I, II, or IIIa was thus assumed to undergo surgical treatment, whereas a patient with stage IIIb or IV was assumed to undergo nonsurgical treatment. For example, CT staging may suggest curative resection with its subsequent costs and outcomes, and PET/CT staging may suggest palliative care with its subsequent costs and outcomes. The total QALYs generated by each diagnostic method were calculated by multiplying the number of patients with stage I, II, or IIIa by the QALYs derived from the Cox proportional hazards model for surgical treatment and by multiplying the number of patients with stages IIIb and IV by the QALYs derived for nonsurgical treatment. Thus, we used actual survival from our study cohort for patients who underwent surgery and those who did not undergo surgery to estimate survival for each treatment decision. The cost calculation for each diagnostic method was based on the diagnostic costs for CT alone or PET/CT and on the cost for surgical or nonsurgical treatment multiplied by the number of patients with surgical or nonsurgical treatment, respectively. The ICERs were assessed as the incremental costs of PET/CT versus CT alone divided by their incremental QALYs (19). The resulting values are thus additional costs per QALY gained of a diagnostic method, compared with another.
Sensitivity Analysis
The robustness of the assumption that the utility for patients who underwent surgical treatment decreased by 0.15 (surgical morbidity rate) had to be tested by sensitivity analysis. Depending on the course of disease for each patient, and on the method of surgery, the loss in QALYs may differ from patient to patient. As a result, a sensitivity analysis was conducted by varying the decrease in utility to 0.1 and 0.2. We also varied the follow-up years (for calculated QALYs) from 3 to 4.
In addition, cost-effectiveness acceptability curves were constructed for PET/CT versus CT. To do so, we ran a Monte Carlo simulation of model parameters with 10,000 iterations. Cost-effectiveness acceptability curves were then calculated as the proportion of simulation results that were cost-effective (16). As recommended by Briggs et al. (20) for distributional assumptions in Monte Carlo simulations that cannot be derived from empiric data, the decrease in QALYs due to surgical treatment was assumed to be β-distributed (mean, 0.15; SD, 0.05). The β-distribution has the advantage that it can take only positive values in an interval between 0 and 1. As derived from our sample, QALYs for patients who underwent surgery and QALYs for patients without surgical treatment were assumed to be normally distributed. Distributional parameters were obtained from the data using the method of moment estimators. Costs with and without surgical treatment were assumed to follow a discrete distribution that resembled the calculation of surgical and nonsurgical costs from weighted average costs of surgical and nonsurgical DRGs, respectively.
RESULTS
Study Collective
From 240 patients prospectively recruited at the study site, 68 patients had to be excluded because of benign histology (38) or malignancies other than non–small cell lung cancer (small cell lung cancer, 14 patients; mesothelioma, 11 patients; soft-tissue sarcoma, 3 patients; and not further classified, 2 patients). The final study population consisted of 172 patients (132 men and 40 women) with non–small cell lung cancer, and the mean age was 65.6 y (age range, 33–88 y). Although 77 patients underwent open resective surgery, 95 patients had been treated nonsurgically. Table 1 gives an overview of the study population. None of the patients had chemo- or radiotherapy before surgery. Ninety-five patients (55.2%) died during the course of the study. Survival times of the remaining 77 patients (44.8%) were right-censored—that is, 25 of the patients were lost to follow-up, and 52 were alive at the end of the study (January 2007). For cost-effectiveness analysis with QALYs as outcomes, we included the full study population of 172 patients, and for cost-effectiveness analysis using correctly staged patients as outcome, only those patients undergoing surgery were included (77/172). The reason for this approach was that effectiveness is measured by comparing staging results with pathology results, which are available only in patients who underwent surgery including complete resection of the primary tumor and full mediastinal lymph node sampling (Fig. 1). The results for each patient, under consideration of data protection laws, are displayed in the Supplemental Table 1 (supplemental materials are available online only at http://jnm.snmjournals.org).
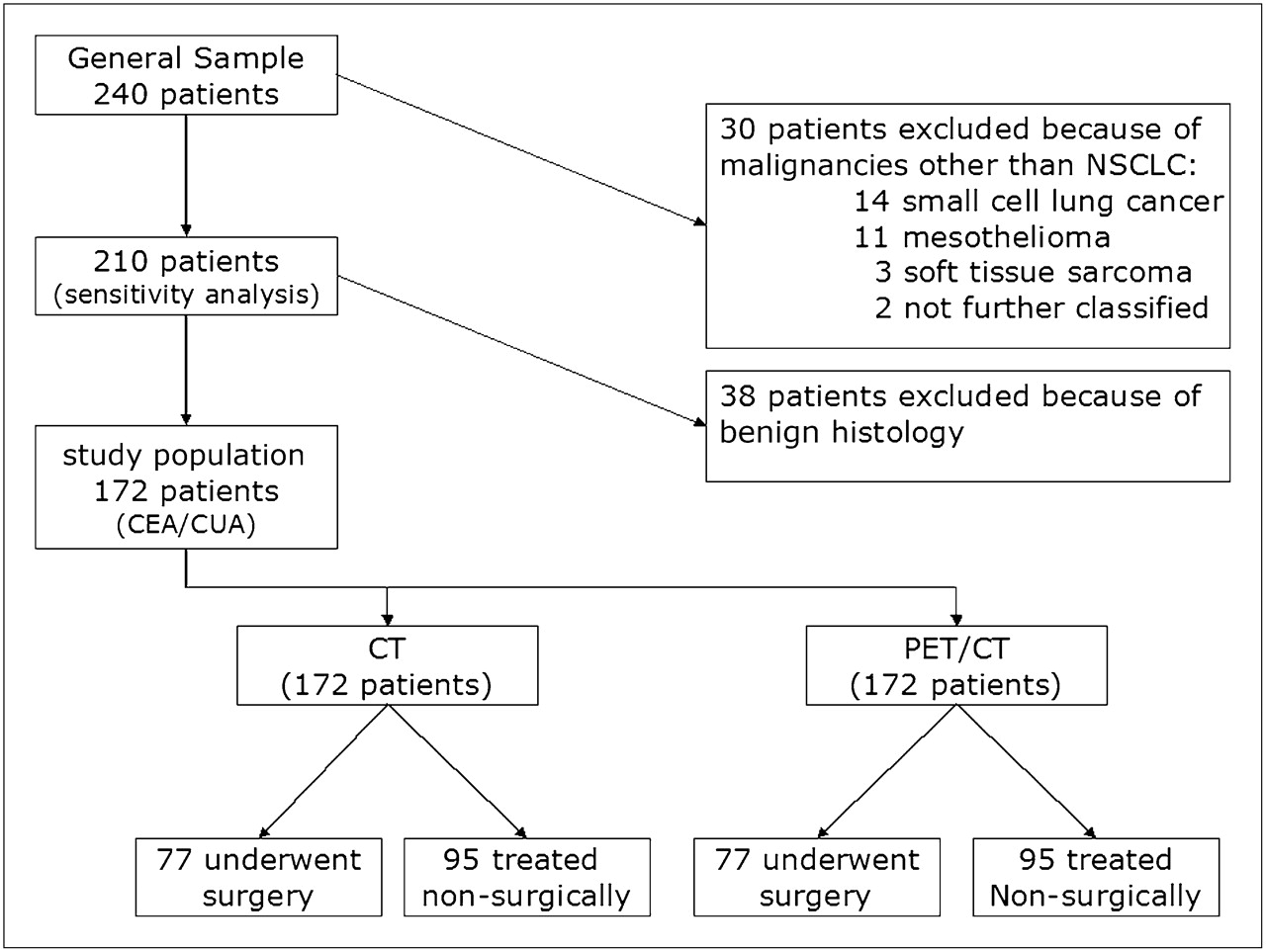
Standards for reporting of diagnostic accuracy diagram showing subsets of patient population used in different analyses. CUA = cost-utility analysis.
Costs for Imaging NSCLC
The cost of diagnosis was $783 per patient for PET/CT and $100 per patient for CT alone. The cost of surgical treatment amounted to $10,226 per patient, and the cost of nonsurgical treatment amounted to $2,881 per patient (Table 2).
Full List of Patients, with Staging Results
Overview of Costs for Treatment
Diagnostic Effectiveness of CT and PET/CT Regarding TNM Staging and Differential Diagnosis of Pulmonary Nodules
According to the histologic stage, PET/CT correctly classified patients significantly more often than did CT alone. Sixty percent of patients (46/77) were correctly staged with PET/CT, compared with 40% with CT alone (31/77). The difference between the performance of PET/CT and CT alone was statistically significant (P < 0.01). Also, PET/CT was significantly more correct in differentiating benign from malignant pulmonary nodules. The accuracy of CT was 86% (206/240) and that of PET/CT was 94% (226/240) (P < 0.001). Thirty-eight patients were classified as having benign pulmonary disease. In 13 patients, a benign histology was proven by histologic examination (resection of the complete tumor), and in 10 patients, fine-needle aspiration served as the reference for benign disease. Fifteen patients did not undergo tissue sampling but were followed by repetitive CT indicating benign disease. Eleven patients were also classified as having benign disease at CT, and 26 patients were classified as having indeterminate or malignant disease. PET/CT classified 16 patients with suspected lesions at CT as having benign disease and 10 as having indeterminate or malignant disease.
Diagnostic Effectiveness of CT and PET/CT Regarding Tumor Resectability
According to CT, 69 patients were classified as having stages Ia–IIIa disease, resulting in 54 surgical interventions performed with a curative intent. CT indicated stages IIIb–IV in 103 patients, suggesting palliative care. PET/CT staged 75 patients as having stages I–IIIa disease and 97 patients as having stages IIIb–IV disease. When assessing the effectiveness with regard to correct tumor staging and, thus, adequate differentiation of patients with resectable disease (stages I–IIIa) and patients with incurable cancer (IIIb–IV), PET/CT staged 65 of 77 patients correctly (84%), and CT alone staged 54 of 77 patients correctly (70%). PET/CT indicated metastatic disease in 35% of the patients (60), compared with 28% (48) by CT. Compared with CT alone, staging with PET/CT was significantly more accurate (P < 0.05).
The number of curative surgeries was significantly influenced by downstaging, which occurred in 16 patients (9%), and upstaging, which occurred in 12 patients (7%), predominantly by detecting metastatic disease not evident at CT. Regarding the frequency of futile surgeries and inappropriately canceled surgeries, recommendations based on PET/CT and CT alone would have led to 2 unnecessary surgeries. PET/CT would have led to 10 inappropriately canceled surgeries, whereas with CT alone, 21 patients would have undergone inappropriate surgeries.
Cost per Correctly Staged Patient
The cost-effectiveness of the 2 imaging procedures was measured with respect to costs per correctly staged patient. In the first step, the cost-effectiveness of correct staging according to each stage (Ia/Ib, IIa/IIb, IIIa, IIIb, and IV) was assessed. When PET/CT was compared with CT alone, the ICER was $3,508 per correctly staged patient (Table 3). The ICER increased to $5,805 per correctly staged patient when patients with benign histology were included.
ICERs for Correct Staging According to Stage (Ia/b, IIa/b, IIIa, IIIb, and IV)
In the second step, the cost-effectiveness of correct staging according to the resectability of NSCLC was assessed. The ICER of PET/CT versus CT alone increased to $4,784 (Table 4). The ICER increased to $7,591 per correctly staged patient when patients with benign histology were included.
ICERs for Correct Staging According to Resectability (I–IIIa)
In the third step, the cost-effectiveness of including those patients who did not undergo surgery was assessed. In this analysis, the ICER increased to $14,874 per correctly staged patient.
Estimated Survival: Cox Proportional Hazards
The results of the model used for this evaluation show a strong prognostic effect of surgical intervention on patient survival (P = 0.0007). The hazard ratio was 0.56 for patients who underwent surgery—that is, the risk of mortality was 44% lower for patients who underwent surgery than for those who did not undergo surgery. There was a weak trend for survival to decrease with age (P = 0.0824). Sex did not significantly affect survival (P = 0.6023), after accounting for the prognostic effects of the 2 other variables.
Cost per QALY
With incremental costs of $939 per patient and incremental QALYs of 0.01 per patient for PET/CT, compared with CT alone, the ICER of PET/CT versus CT alone was $79,878 per QALY (Table 5).
ICERs for Evaluation of Cost Per QALY
Sensitivity Analysis
By assuming the loss of utility due to surgical morbidity (estimated to be 0.10 QALYs), the ICER decreased from $79,878 to $69,563 per QALY for PET/CT versus CT alone. A larger loss of utility from surgical intervention (0.20 QALYs) consequently increased ICERs to $93,782 per QALY for PET/CT versus CT alone. The increase in the time frame for the calculation of QALYs from 3 to 4 y led to an increase of 0.14 QALYs for patients who underwent surgery and an increase of 0.03 QALYs for patients who were treated palliatively. ICERs decreased to $60,899 per QALY for PET/CT versus CT alone (Table 6). We also calculated results for a 5-y period, but the sample size was too small to generate robust results; results, however, were similar to the model, assuming a 4-y period. Figure 2 shows ICER depending on difference in diagnostic cost between PET/CT and CT. Results from Monte Carlo simulation show that, at a threshold of $62,780, the probability of PET/CT, compared with CT, to be cost-effective was 35.7%.
Sensitivity Analysis of PET/CT Versus CT, with Different Surgical Morbidity Rate and Time Period

ICER depending on difference in diagnostic cost between PET/CT and CT.
DISCUSSION
The objective of this study was to evaluate the cost-effectiveness of 2 imaging procedures, PET/CT and CT alone, in the clinical scenario of NSCLC staging from the payer's perspective.
This study demonstrated the cost-effectiveness of integrated PET/CT for primary staging of NSCLC, with an ICER of $3,508 for PET/CT versus CT alone. A gain in diagnostic accuracy of PET/CT, compared with CT alone, in staging NSCLC has been demonstrated by Lardinois et al. (22), Halpern et al. (23), and Shim et al. (24) and was also observed in our study. Cost-effectiveness analysis (CEA), however, has not been conducted so far. PET/CT had higher costs than did CT alone but is associated with a gain in effectiveness—that is, 15 additional patients were correctly staged using the integrated modality than using the CT-based approach. This increase in effectiveness is confirmed by results from other studies. Whereas this is the first study indicating that integrated imaging with PET/CT is cost-effective, similar advantages of functional imaging with PET alone, compared with CT alone, have been demonstrated. A study performed in Canada concluded that PET for staging NSCLC without CT coregistration, compared with CT alone, led to a cost savings of $1,455 combined with an increase in life expectancy of 3.1 d (25). In France, nearly the same conclusions were drawn, with costs decreasing by $96.68 (€77) per patient and an observed gain in life expectancy of 0.1 y per patient for PET, when compared with CT alone (26). However, our sensitivity analyses show that the ICER increases substantially if patients are included who did not undergo surgery. Thus, the superiority of PET/CT, compared with CT alone, is reduced if patients with an intermediate pretest likelihood for the presence of metastases are staged too, because CT is likely to result in a similar staging accuracy.
There is strong evidence from more recent studies that PET/CT usually performs better than PET alone (12,22,23,27). Cerfolio et al. (12) showed that integrated PET/CT predicts stages I and II, and the T (tumor) and N (node) status, significantly more accurately than PET alone. In their study, for stage I, the tumor stage was predicted correctly in 52% of patients with PET/CT versus 33% of patients with PET alone. For stage II, PET/CT was correct in 70% of patients and PET was correct in 36%. The values were 70% versus 47% for T staging and 78% versus 56% for N staging. Antoch et al. (27) showed similar results. The sensitivity of PET/CT was 89%, equal to the sensitivity of PET alone, versus the 70% for CT alone. The specificity, however, was 94% for PET/CT versus 89% for PET alone and only 59% for CT alone. Although no other CEA studies on PET/CT have been conducted so far, these findings help to assess the reliability of the ICERs in this study, which heavily depend on the staging results. In addition, according to Antoch et al., the number of patients correctly staged increases with the number of studies performed with PET/CT (27). Because the PET/CT scanner used in this study was established only 1 month before the start of patient recruitment, it can be assumed that for trained physicians the true sensitivity (and in consequence the costs) will be lower than the sensitivity obtained here.
With regard to the cost per QALY, in this study PET/CT proved to be slightly above an accepted threshold of $62,780 for implementation in the clinic (3,6,19). However, when a lower surgical morbidity is assumed—that is, the loss of utility due to surgical intervention is decreased—or when the time frame for the calculation of QALYs is increased, the ICER of PET/CT versus CT alone moves below the assumed threshold of $62,780. In the present study, consecutive patients with clinical suspicion of or histologically proven NSCLC were included. Focusing on patients with an intermediate pretest likelihood for the presence of metastases would further reduce the ICER of PET/CT versus CT.
So far, only a few CEAs have evaluated the cost per QALY of PET alone versus CT alone. The results of the study of Bird et al. are in line with those already published concerning the accuracy and cost-effectiveness of PET alone, compared with CT alone (4). In the Centre for Health Economics Research and Evaluation study, ICERs of PET alone versus CT alone were $18,308. In the study of Dietlein et al. (6), the ICERs of PET alone versus CT alone were $13,927 per life year saved. The sensitivity analysis presented in Table 6 showed the substantial effects that varying QALY outcomes can have on the ICERs—that is, the additional costs per QALY gained using PET/CT, compared with other technologies, varied largely when we assumed different surgical morbidity rates or longer follow-up periods after initial staging. As a result, the evaluation of cost per QALY has to be interpreted with caution.
The strength of this study is related to a relatively large sample size, compared with that in previous series (Klose et al. (7), 22 patients; Lardinois et al. (22), 49 patients; and Antoch et al. (27), 27 patients). Furthermore, the study had a rather long follow-up of up to 4 y. In addition, no CEAs of PET/CT have been conducted for NSCLC until now. Also, cost data did not have to be estimated from the literature but could be obtained from a hospital's administrative department. Another strength of the study is that 2 different measures for outcomes in our cost-effectiveness analyses were used to increase the generalizability and transferability of our findings. Some evaluation committees prefer clinical endpoints such as correctly staged patients, whereas others prefer utility measures such as QALYs.
Limitations apply to the fact that the surgical morbidity rate is estimated, and costs for treatment (surgery vs. nonsurgical therapy) are based on the payer's perspective. It would have been preferable to obtain costs from the societal perspective too. Thus, our costs may not be representative for Germany or other European countries, although the base rate used is close to the average hospital base rate in Germany. In this study collective, none of the patients received chemo- or radiotherapy before surgery. However, the validity of our reference standard (histology) to assess the utility of PET/CT may be altered if radio- or chemotherapy is administered in a neoadjuvant setting. It is also likely that some bias resulted from the interpretation of images, because the experience of the evaluating physicians may improve over time. Because of a lack of information on patient comorbidities and surgical complications, survival analysis could adjust only for age and sex. Also, the economic evaluation was not assessed using detailed information on separate T, N, and M staging but simply on the overall TNM stages. Mediastinoscopy is considered the gold standard for N staging of the mediastinum but was not mandatory for participation in our study. Finally, it would have been preferable to use data from a randomized controlled trial, but because of ethical reasons it was not possible in this study. However, in the absence of randomized controlled trials, modeling approaches are widely accepted among reimbursement evaluation committees.
CONCLUSION
This study demonstrates that PET/CT, in comparison to the standard CT-based approach, is more accurate and represents a cost-effective imaging modality for staging NSCLC. With an ICER of $4,784 per additional patient correctly staged regarding resectability and $79,878 per QALY gained, costs only slightly exceed the accepted threshold of $62,780 (∼€50,000) for reimbursement acceptance. This amount is, for instance, set by the British National Institute for Health and Clinical Excellence, which is frequently used by evaluation agencies in other countries as a reference. Thus, the results of cost-effectiveness analyses suggest that PET/CT for staging of NSCLC should be reimbursed by public schemes in industrialized countries, especially when considering the current improved performance due to better-trained physicians and higher-sensitivity state-of-the-art PET/CT scanners.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication October 28, 2009.
- Accepted for publication May 19, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriate Use Criteria for 18F-FDG PET/CT in Restaging and Treatment Response Assessment of Malignant Disease
- Effect of PET/CT on Management of Patients with Non-Small Cell Lung Cancer: Results of a Prospective Study with 5-Year Survival Data
- Large Decreases in Standardized Uptake Values After Definitive Radiation Are Associated with Better Survival of Patients with Locally Advanced Non-Small Cell Lung Cancer
- Contribution of Imaging to Cancer Care Costs
- 18F-FDG PET/CT for Monitoring Treatment Responses to the Epidermal Growth Factor Receptor Inhibitor Erlotinib
- Are Health Economics Making Us Sick?