


Abstract
The purpose of this study was to test the hypothesis that the level of baseline 18F-FDG uptake in the primary tumor adds value to its relative change in 18F-FDG uptake in serial PET scans in predicting the histopathologic response to systemic cytotoxic neoadjuvant treatment of patients with solid extracerebral tumors. Methods: We performed a literature search from January 1995 through November 2008 using PubMed and Embase. Two reviewers independently selected eligible studies for possible inclusion in the meta-analysis by reviewing titles and abstracts. Inclusion criteria were at least 10 patients, 18F-FDG PET before and after therapy, 18F-FDG PET performed with the intention of monitoring the response of solid extracerebral tumors in humans to cytotoxic neoadjuvant systemic therapy, attenuation-corrected 18F-FDG PET studies, and studies presenting individual patient data (PET results and histopathologic reference test after treatment). Multilevel logistic regression was used to assess the effect of relative change of 18F-FDG uptake ([baseline – end]/baseline) and baseline 18F-FDG uptake value with type of tumor and type of treatment as level 1 covariates. Results: Nineteen studies (all observational; a total of 438 patients [median, 23 patients per study; range, 10–40]) were included, aiming at the accuracy of PET versus histopathology. To quantify PET, maximum standardized uptake value (SUV) was used in 6 studies, mean SUV in 7, SUV (subtype unclear) in 1, tumor-to-background ratio in 3, and dose uptake ratio in 1. The average overall histopathologic response rate was 0.47 (median, 0.50), ranging from 0.17 to 0.88. The relative change in 18F-FDG uptake was the strongest indicator (P < 0.0001) for tumor response. Baseline 18F-FDG was not significantly associated as a main factor; however, a significant interaction of baseline uptake and relative change after therapy was observed (P < 0.001). Conclusion: Relative change in 18F-FDG uptake was the strongest indicator for tumor response, but the level of baseline 18F-FDG uptake in the primary tumor provided additional information about prediction of response to therapy. These data corroborate and extend the need for standardization, quality assurance, and control of PET studies quantifying 18F-FDG in oncologic treatment monitoring.
During the last decade, 18F-FDG PET has become important for the diagnosis, staging, prognosis, and evaluation of treatment response in oncology (1). In the neoadjuvant setting, 18F-FDG PET examinations before, during, or after therapy have been investigated to evaluate and monitor therapy response, predict prognosis, and guide decisions on postsurgical treatment. The need for quantitative assessment of metabolic response increases, and it is expected that PET will be incorporated in the response evaluation criteria of solid tumors.
In the context of response evaluation, most studies focus on the relative change of 18F-FDG uptake as an index for metabolic response. Additionally, the level of baseline 18F-FDG uptake may have prognostic value (2). Relative change does not account for this potential effect modifier. The aim of this meta-analysis was to qualitatively test the hypothesis that the level of baseline 18F-FDG uptake in the primary tumor has added value to relative change in 18F-FDG uptake in serial PET scans in evaluating response to systemic cytotoxic neoadjuvant treatment of patients with solid extracerebral tumors.
MATERIALS AND METHODS
Literature Search
A formal computer-assisted search was performed in the medical databases PubMed (Medline included) and Embase from January 1995 through November 2008. Both text words and medical subject headings were used. The full-search algorithm can be obtained in Supplemental Table 1 (supplemental materials are available online only at http://jnm.snmjournals.org). In addition, a manual cross-reference search of eligible and review papers was performed to identify additional possible articles.
Study Selection
Three reviewers independently selected studies for possible inclusion in the meta-analysis by reviewing titles and abstracts. Differences were resolved by consensus. To be eligible for the meta-analysis, a study had to fulfill the following inclusion criteria: at least 10 patients, 18F-FDG PET before and after therapy, 18F-FDG PET performed with the intention of monitoring the response of solid extracerebral tumors in humans to cytotoxic neoadjuvant systemic therapy, attenuation-corrected 18F-FDG PET studies, and studies presenting individual patient data (PET results and histopathologic reference test after treatment). Duplicate studies on the same patients, studies using only γ-camera coincidence imaging, studies written in a language other than English or German, and reviews and abstracts were excluded. The last 2 categories were used for cross-referencing. No unpublished data or data from abstracts were used.
Data Abstraction and Quality Assessment
Two reviewers independently extracted the following items from the studies: study design (prospective, retrospective but consecutive, retrospective inclusion), patient characteristics, PET characteristics (qualitative and quantitative), and reference test or histopathologic evaluation system.
We considered the description of PET as adequate if the publication reported details on the scanner type, the timing of scanning after injection, a clear description of quantitative procedures including region-of-interest (ROI) methodology, and the performance of attenuation correction.
Statistical Analysis
Dichotomized histopathologic response (response or no response) was the primary endpoint. Individual patient data consisted of baseline and relative change of 18F-FDG uptake. Baseline PET data were missing for 6 individuals (1%) in different studies and missing for the second PET measurement for 38 individuals (8.7%). For overall consistency, these missing values were imputed by regression (3).
Multilevel logistic regression was used to assess the effect of relative change of 18F-FDG uptake ([baseline – end]/baseline), baseline 18F-FDG uptake value, type of tumor (sarcoma, esophageal carcinoma, or other), type of treatment (chemotherapy or chemoradiotherapy), and type of measurement (standardized uptake value [SUV], tumor-to-background ratio, or dose uptake ratio) as level 1 covariates. All sarcomas were treated exclusively by chemoradiotherapy, and they served as the reference group. Studies were included as random factors (level 2), allowing for random intercepts and random slopes for the differences in relative decrease at level 2. Level 1 factors and interactions were investigated by a backward stepwise procedure in which nonsignificant interactions were excluded in order of largest P value (exclusion at P > 0.05).
To quantify the heterogeneity between studies, the median odds ratio (MOR) was calculated (4). The MOR quantifies the variation between studies (the second-level variation) by comparing 2 persons from 2 randomly chosen, different studies. The MOR is always greater than or equal to 1. If there is considerable between-study variation, the MOR will be large (the measure is comparable with fixed-effects odds ratio). To quantify the effect of study-level covariates (therapy, tumor type), interval odds ratios were calculated. If the interval contained 1, the (fixed) effect of the study-level variable was large in comparison with the unexplained between-study variation (4).
RESULTS
Study Characteristics
Our initial search identified 1,749 studies: the PubMed search identified 917 and the EMBASE search (after exclusion of duplicates) 832 studies. On the basis of title and abstract, 1,632 studies did not meet the inclusion criteria. After reviewing the full text of the remaining 117 studies, we included 19 studies (5–23). All were observational studies, aiming at the accuracy of PET versus histopathology. The detailed process by which the articles were selected can be found in the Supplemental Appendix 1.
The 19 studies included data on 438 patients, with a median of 23 patients per study (range, 10–40). Of these studies, 6 were on esophageal cancer (46% of patients), 7 on sarcoma (27% of patients), and 6 on other malignancies (breast cancer, head and neck carcinoma, non–small cell lung cancer, gynecologic cancer, and locally advanced rectal cancer; 27% of patients). In 8 studies, each patient received chemotherapy (51% of patients); in the other studies (49% of patients), chemotherapy was combined with radiotherapy in several patients. Radiotherapy was always given concurrently with chemotherapy. Table 1 provides further details of the patient characteristics per study. In all studies, surgical resection of the tumor was scheduled within weeks after completion of the neoadjuvant treatment. The pathologic definition of response differed per malignancy and is displayed in Table 2 (24–27). Because studies were performed over a period of almost a decade (1999–2008), no standardized PET protocol was used, and variable scanners, scan modes, 18F-FDG doses, time intervals (between injection of 18F-FDG and the PET scan, between the completion of the induction therapy and the posttreatment PET, and between the posttreatment PET and surgery), and image-reconstruction methods were used. These PET characteristics are listed in Table 3, and in Table 4 the PET data-analysis characteristics are displayed in more detail. Furthermore, the fasting period differed per study. However, all studies reported a fasting period of at least 4 h before PET, except the study of Huang et al., in which this period was at least 2 h (17). All but 4 studies (17,19,20,22) reported that glucose levels were measured before PET examination. No study, except for the study of Chen et al. (13), described when or how the PET or PET/CT scanners were calibrated. Different methods to quantify 18F-FDG uptake were used: the SUV approach was used in 15 studies (maximum standardized uptake value in 7 studies; mean standardized uptake value in 8 studies), tumor-to-background (or nontumor-to-background) ratios in 3 studies, and a dose uptake ratio in 1 study. Different ROI methodologies were used in the analysis (manual; irregular isocontour, based on a fixed percentage of the maximal pixel in the tumor, on a fixed SUV threshold, or on a background-level threshold; or small fixed-dimension ROI centered over the highest-uptake part of the tumor; Table 4).
Patient Characteristics of 19 Studies Reviewed
Definition of Response Differs According to Tumor Type: Histopathologic Evaluation System
18F-FDG PET Characteristics in 19 Studies Reviewed
PET Data Analysis Characteristics of 19 Studies Reviewed
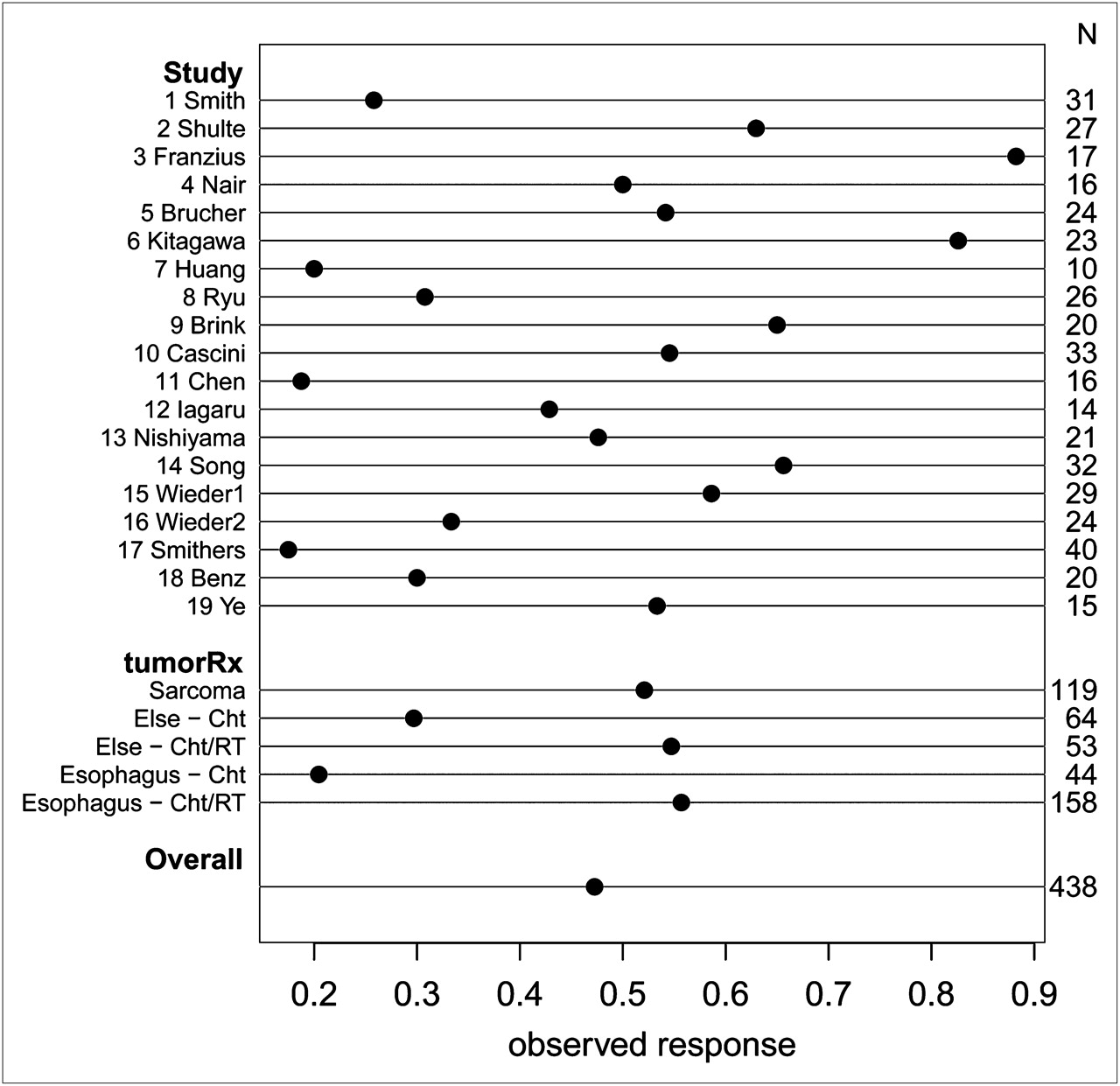
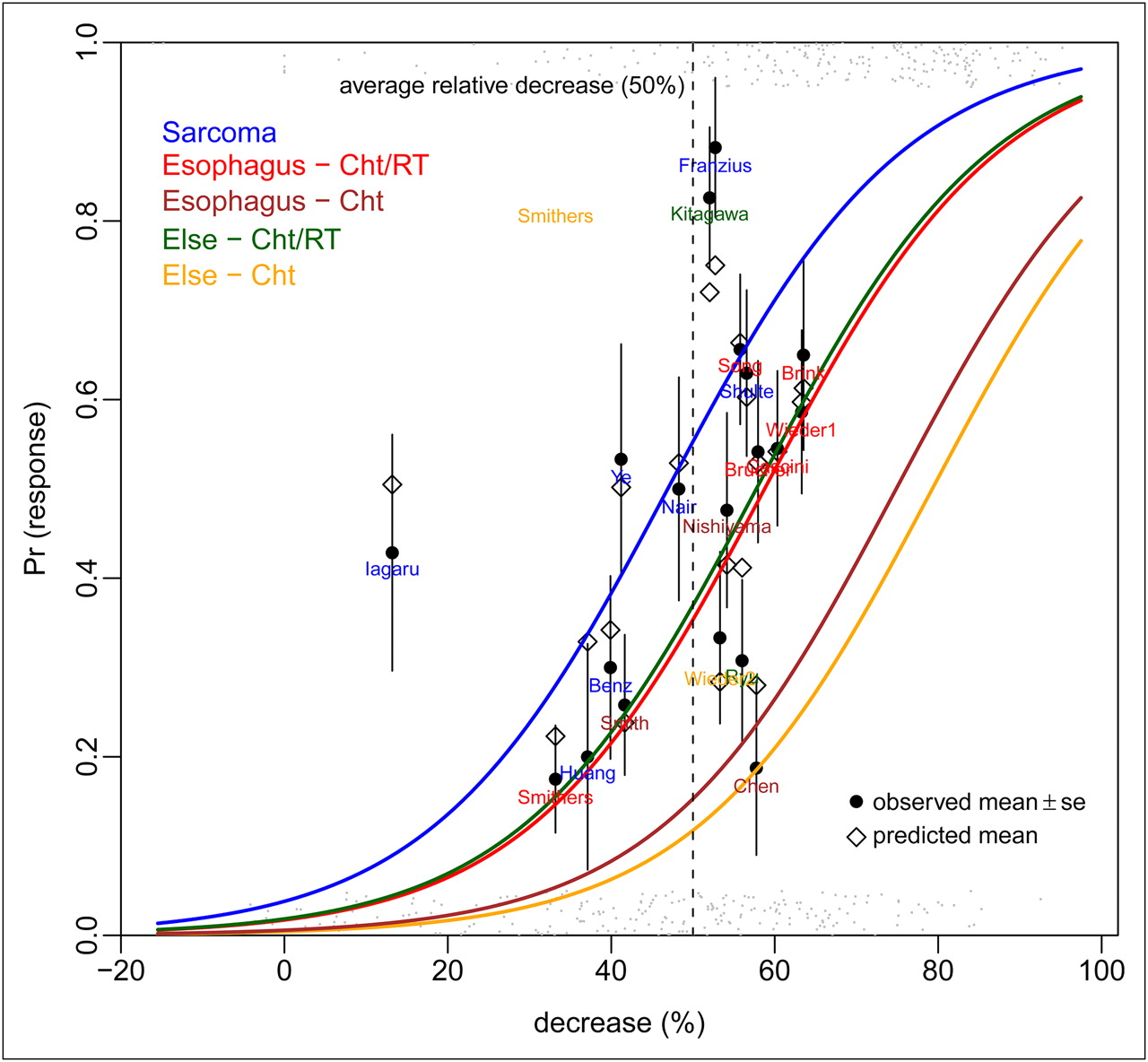
For all patients, the average overall histopathologic response rate was 0.47 (median, 0.50), ranging from 0.17 to 0.88 among the studies (Fig. 1). Logistic regression estimated the histopathologic response rate as a function of the linear predictor decrease in 18F-FDG uptake, tumor type, and therapy. As illustrated in Figure 2, this model suggests that each 10% relative difference in 18F-FDG uptake corresponded to a 17% positive change in pathologic response rate at the mean level of baseline 18F-FDG uptake (for each tumor-therapy group). Figure 3 illustrates the predicted response according to the multilevel model versus the observed response rate according to histopathology of all 19 studies.

Overview of response rates in 19 eligible studies. TumorRx indicates combination of tumor type (sarcoma, esophagus, or other types) and therapy (chemotherapy [ChT] or chemoradiotherapy [ChT/RT]). Sarcoma was exclusively treated by chemoradiotherapy. Tumor-treatment combination mostly explains heterogeneity between studies with respect to factors explaining response.
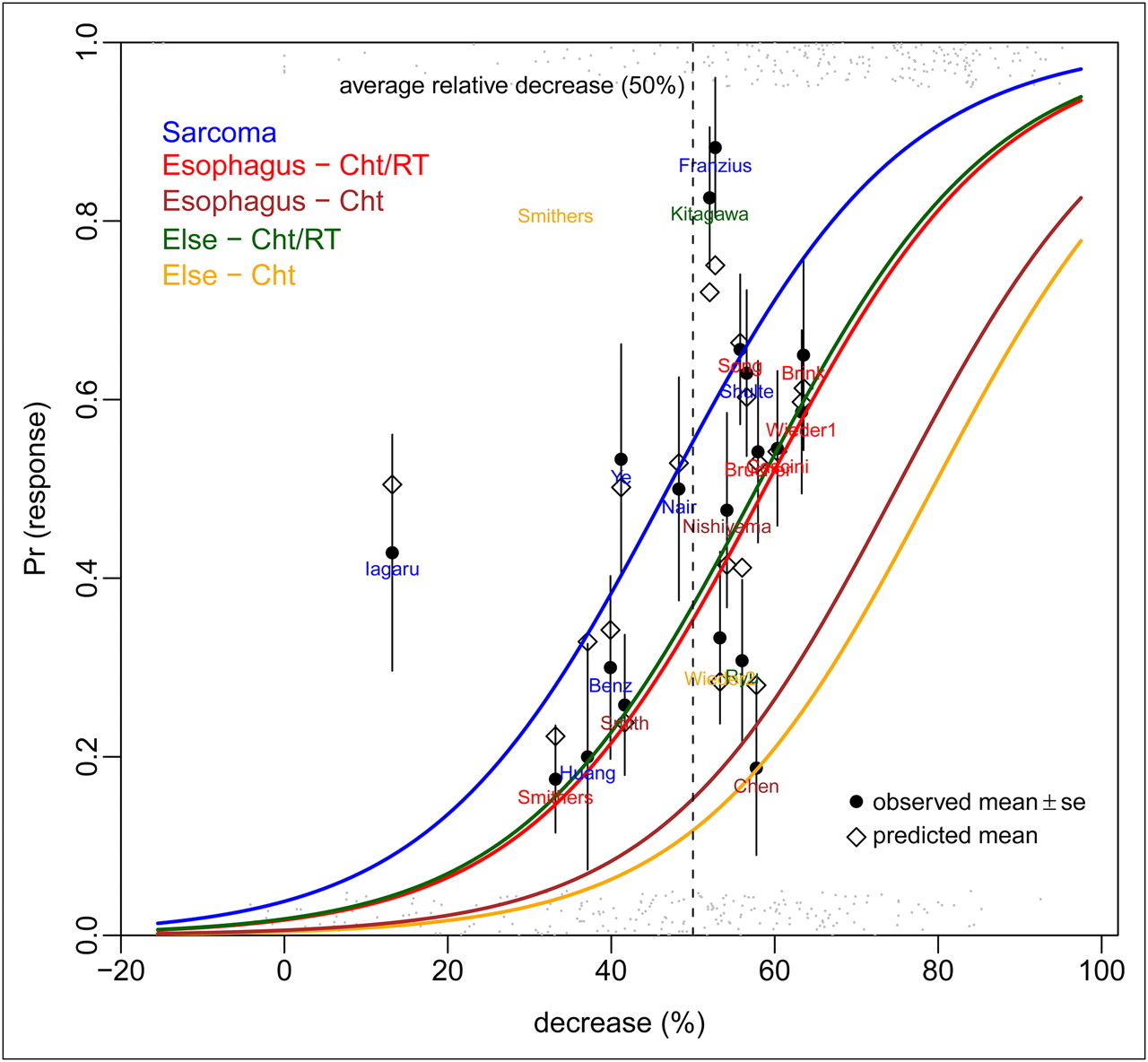
Logistic regression estimating histopathologic response rate (Pr [response]) as function of linear predictor of decrease in 18F-FDG uptake (decrease [%]), tumor type, and therapy (indicated by colored lines). Black circles indicate actual average histopathologic response rates per study, whereas open diamonds represent point estimates of response rate. Gray dots at bottom (no response) and top (response) show actual individual patient data. At mean level of baseline (for each tumor-therapy group), model suggests that 10% decrease in relative difference corresponds to 17% increase in pathologic response rate. Cht = chemotherapy; ChT/RT = chemoradiotherapy.
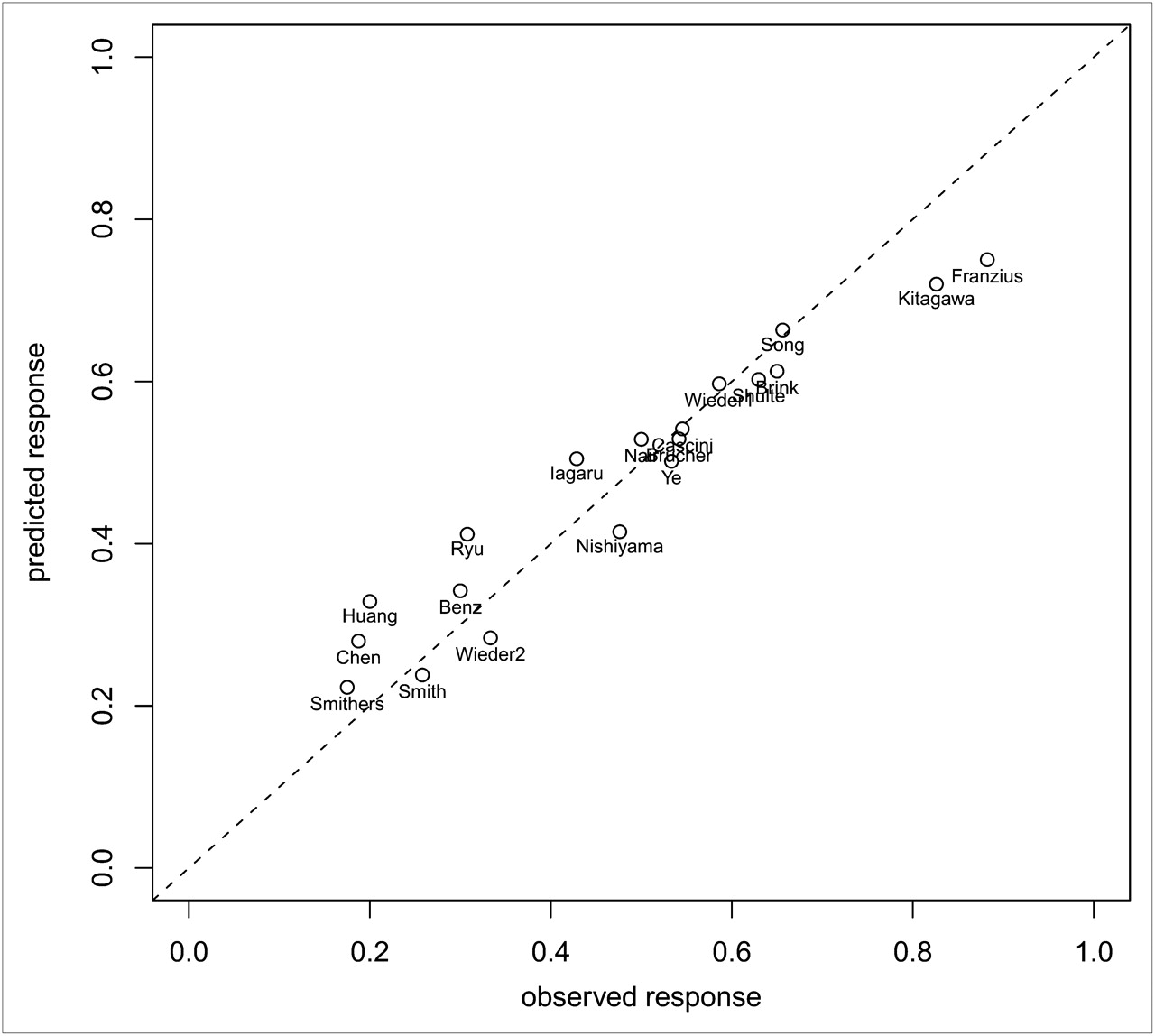
Predicted and observed response rate of all 19 studies based on multilevel model with change in 18F-FDG uptake, baseline 18F-FDG uptake, tumor type, and treatment.
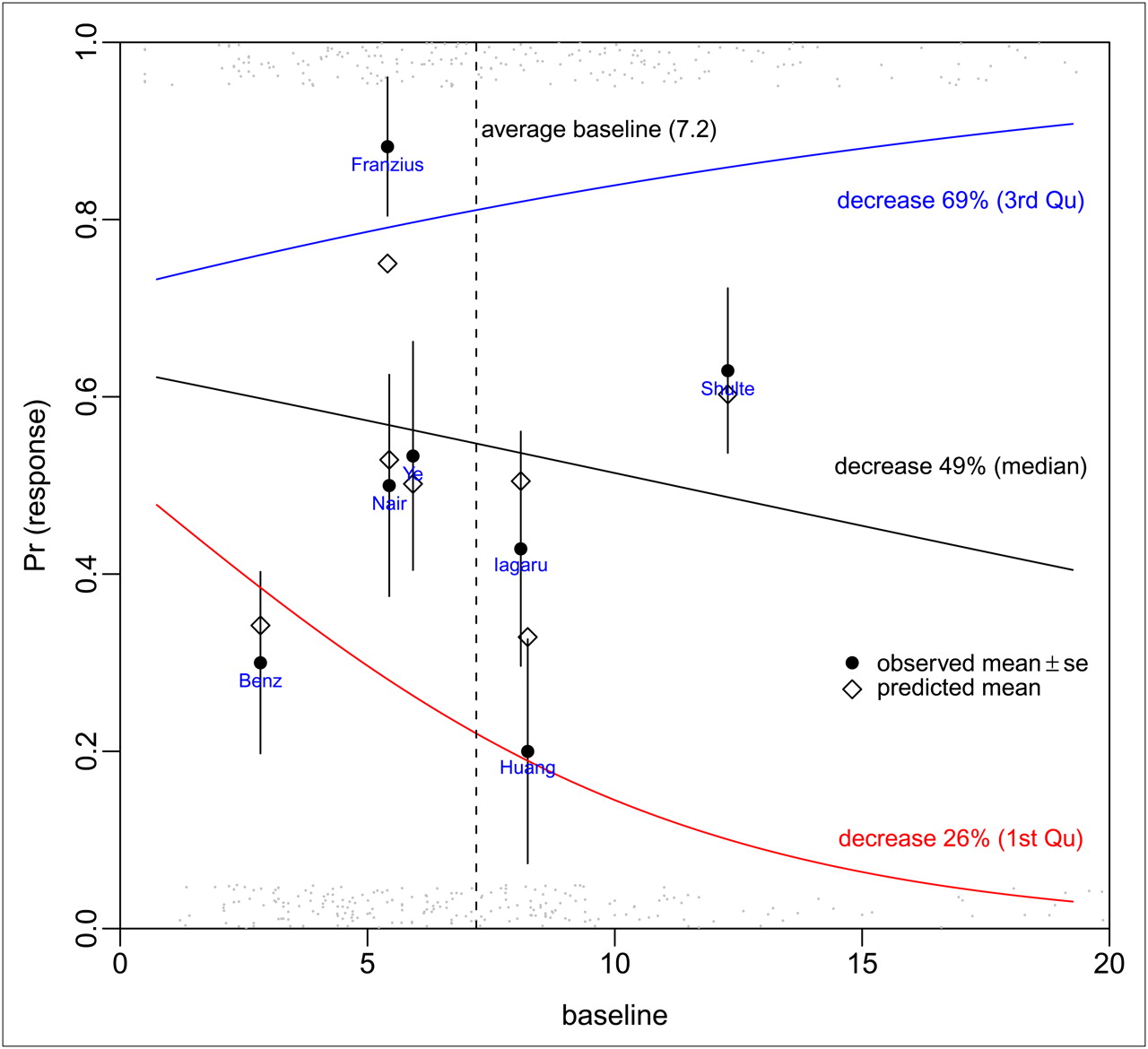
The relative change in 18F-FDG uptake was the strongest indicator (P < 0.0001) for predicting histopathologic tumor response. Baseline 18F-FDG uptake was not significantly associated as a main factor. However, there was a significant interaction (P < 0.0001) between the baseline 18F-FDG uptake and decrease in 18F-FDG uptake. This interaction is illustrated in Figure 4, where 3 quartiles of decrease (25th, 50th, and 75th) are plotted against the baseline 18F-FDG uptake (x-axis) and the probability of histopathologic response (y-axis). Among patients with a high fractional decrease of tracer uptake, those patients with high baseline 18F-FDG uptake values had a higher probability of histopathologic response than did those with low baseline 18F-FDG values. Conversely, among patients with low fractional 18F-FDG reductions, those patients with high baseline 18F-FDG uptake had a lower probability of histopathologic response than did those with low baseline uptake. In the group around the median fractional 18F-FDG decrease, the probability of response was almost constant along the range of baseline 18F-FDG values. Adding the baseline 18F-FDG uptake to the decrease in 18F-FDG uptake significantly improved the prediction (P < 0.0001).

Logistic regression estimating response rate (Pr [response]) as function of linear predictor of baseline 18F-FDG uptake at 3 different percentiles of relative decrease (25th, 50th, and 75th percentiles) in 18F-FDG uptake at end of treatment (indicated by colored lines). Black circles indicate actual average response rates, and open diamonds represent point estimates of response rate of studies in sarcoma. Gray dots at bottom (no response) and top (response) show actual individual patient data. Figure clearly shows interaction between level of decrease and baseline 18F-FDG uptake.
Compared with sarcomas (all receiving chemoradiotherapy), esophageal tumors had a lower histopathologic response rate (P = 0.001 for chemotherapy and P = 0.07 for chemoradiotherapy). This lower histopathologic response rate should be read with the greatly different histopathologic response criteria in mind (Table 2). The response rate of patients with other tumors receiving chemoradiotherapy did not differ from the response rate of sarcomas, but those receiving chemotherapy had the lowest response rate (P = 0.00063). Including the type of measurement did not improve the overall fit of the model significantly. Therefore, it was decided to leave the variable out.
The heterogeneity between studies with respect to the factors explaining the response was moderate (MOR, 1.89) and mostly explained by the tumor-treatment combination (interval odds ratio, esophageal chemotherapy, 0.03–0.36; other tumor chemotherapy, 0.04–0.49), also illustrated in Figure 1.
DISCUSSION
This meta-analysis provides evidence to suggest that baseline 18F-FDG uptake adds prognostically relevant information to the relative change of 18F-FDG uptake, in the context of neoadjuvant therapy of extracerebral solid tumors. The overall fit of the model (Fig. 3) suggests that the results are applicable to a broad spectrum of possible response rates and test conditions.
We hypothesized that baseline uptake might add information on responsiveness to relative change because baseline 18F-FDG uptake appears to be related to a more aggressive phenotype, probably mediated via hypoxia or proliferative activity. We also reasoned that the size of such potential effect modification of relative change was unpredictable because proliferation and hypoxia may affect therapy differently: high proliferative activity may be prognostically favorable in the case of chemotherapy, but the reverse may be true for radiotherapy (e.g., via repopulation effects, perhaps as a function of fractionation schemes). Alternatively, hypoxia is supposed to negatively affect the impact of either therapy. Therefore, we chose a phenomenologic rather than mechanistic approach.
Our meta-analytic method accounts for the variability of individual study characteristics. We applied a 2-level model, allowing the variances within and between studies to be different. Simultaneously, several sources of between-study heterogeneity could be considered. Although the heterogeneity between these studies with respect to the factors explaining the response proved to be moderate, each of the separate studies was small and contained a substantial heterogeneity in many other aspects. From a quantitative perspective, the findings need to be interpreted with caution: obviously, the model cannot account for technical measurement errors due to low contrast (tumors with low baseline uptake).
Without standardization of, for example, the PET methodology, comparison of results obtained from different centers is hampered by the diversity in methodology of acquisition, image reconstruction, and data-analysis procedures that are applied. To perform multicenter studies, standard protocols should and are being implemented (28). The implication of this finding is that standardization of PET methodology in oncologic trials should be intensified: to aggregate the evidence, it becomes even more important to standardize PET methodology, because the use of absolute values imposes stronger methodologic rigor than that of relative change alone. Obviously, an analysis of a study population with 1 type of tumor, treatment, and timing of scans relative to treatment improves homogeneity even further.
Additionally, this meta-analysis would have had more power if the community had adopted the habit of at least electronically publishing the individual patient results as a standard approach. It may be assumed that it is not feasible to report individual data in larger studies.
In this meta-analysis, we focused on chemotherapy as the mode of systemic therapy. Whether these findings can be extrapolated to newer forms of targeted therapy is unclear, because the interaction of 18F-FDG metabolism and therapy does not need to be consistent.
CONCLUSION
This meta-analysis supports the hypothesis of an interaction of baseline 18F-FDG uptake with its relative change during therapy in patients treated with neoadjuvant chemoradiotherapy. These data corroborate and extend the need for standardization, quality assurance, and control of PET studies quantifying 18F-FDG in oncologic treatment monitoring. Obviously, such standardization will also allow proper validation of the current findings.
Acknowledgments
We thank Tim van den Wijngaert, University of Antwerp, Antwerp, Belgium, for his contribution to this study.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication January 27, 2010.
- Accepted for publication July 14, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}