


Abstract
The aim of this study was to assess the pattern of annexin V uptake in hip and knee prostheses suspected of being infected. Methods: A total of 7 patients undergoing revision surgery for hip or knee prostheses were studied; 5 patients had total hip replacements, and 2 had total knee replacements. Infection was confirmed by pathology, culture results, laboratory evaluation, and clinical follow-up. All patients also underwent a bone scan before surgery. Results: Annexin V scan findings were positive in 5 patients and negative in 2. Annexin V uptake was either focal (n = 4) or linear (n = 1). There were 4 true-positive, 2 true-negative, 1 false-positive, and no false-negative annexin V studies. Annexin V uptake was either more extensive or less extensive than, and usually was incongruent with, 99mTc-methylene diphosphonate uptake. Conclusion: Our findings suggest that annexin V imaging shows greater uptake with infection than with aseptic loosening and has a high negative predictive value for prosthetic infection.
Aseptic loosening, an event that occurs months to years after surgery, is the most frequent cause of prosthetic joint failure (1). A less common but far more serious source of joint implant loosening is periprosthetic infection with Staphylococcus aureus, methicillin-resistant S. aureus, Staphylococcus epidermidis, Streptococcus oralis, Escherichia coli, Enterococcus faecalis, or Pseudomonas aeruginosa (2). Periprosthetic infections also tend to be low-grade and frequently cannot be detected by blood or tissue culture, leaving little clinical information to guide treating physicians. The differentiation of infection from aseptic loosening is important because loosening caused by a periprosthetic infection requires usually at least a 2-stage revision surgery involving the removal of the old implant, debridement, and placement of antibiotic-loaded cement beads in the surgical bed. This treatment is in contrast to the single-stage prosthetic joint–replacement treatment for aseptic loosening, a completely different process believed to be caused by repeated mechanical stress and local host response to the wear debris of high-density polyethylene, metals, and bone cement (1).
Because the clinical and laboratory signs of bacterial infection (culture-negative) are nonspecific, standard radiologic and nuclear medicine imaging remain essential first steps for the work-up of patients with painful prostheses (3). Radiographs reveal signs of loosening regardless of the presence or absence of bacterial infection. Although MRI or enhanced CT scans generally provide useful information for soft-tissue and bone infections, metallic artifacts from a given prosthetic device greatly interfere with the quality of the images obtained (4). Nuclear medicine techniques include 99mTc-methylene diphosphonate (99mTc-MDP) bone scanning, 67Ga imaging, and 111In- (or 99mTc-hexamethylpropyleneamine oxime-) white blood cell labeling. However, differentiation between infection and aseptic loosening may still not be definitive and may force a more invasive work-up that includes joint aspiration and washout or occasionally fresh-frozen biopsy sections obtained during joint surgery. A more reliable and noninvasive imaging tool is needed for better decision making and treatment planning for patients with painful joint prostheses.
Radiolabeled annexin V, a marker of apoptosis and cellular stress or activation, has detected acute, subacute, and chronic inflammation in several animal models and humans (5,6). The aim of this study was to assess the pattern of radiolabeled annexin V uptake in suspected infected hip and knee joint prostheses and determine whether annexin V can be used to differentiate infection from aseptic loosening.
MATERIALS AND METHODS
Study Population
The study was approved by the human subjects and ethics committee at our institution. Five women and 2 men (mean age, 78 y; age range, 69–85 y), undergoing revision surgery for hip or knee prosthesis, were prospectively entered into our study. Of these, 5 underwent a total hip replacement, and 2 underwent total knee replacement (Table 1). Pathology reports and culture results were available for 4 of the patients. Prostheses were considered infected if tissue cultures grew bacteria or if a grossly purulent periprosthetic fluid was seen at surgery. Prostheses were considered uninfected if purulent fluid was not seen at surgery and intraoperative biopsy samples were negative for bacteria. When tissue cultures were not available, decisions regarding infection were based on white blood cell counts, erythrocyte sedimentation rate, C-reactive protein levels, and clinical outcome assessed at 6 mo (or longer) after radionuclide scanning with annexin V.
Characteristics of Study Patients Undergoing Revision Surgery for Hip or Knee Prosthesis
All patients also underwent a standard bone scan with 99mTc-MDP consisting of whole-body and spot views of each affected joint; 3 of the patients also underwent an accompanying SPECT study.
Preparation of 99mTc-Hydrazinonicotinamide (HYNIC) Annexin V for Human Use
NAS 2020 kits were generously supplied by Theseus Imaging Corp. to the principal investigator. Recombinant human (rh) annexin V (molecular weight, 35,806) for the kit was produced by expression in E. coli as previously described (7). HYNIC-derivatized annexin V was prepared for later radiolabeling with a 99mTc-tricine precursor complex according to prior protocols (8).
The 2-vial kit included a 0.5-mL (0.25-mg) vial of frozen liquid HYNIC-rh-annexin V conjugate solution (vial 1) and a vial of lyophilized stannous tricine containing approximately 20 mg of tricine and 500–650 μg of stannous chloride (vial 2). Radiolabeling was conducted at room temperature. 99mTc-pertechnetate (1,110–1,850 MBq [30–50 mCi]; 0.4–0.6 mL) was added to the HYNIC-rh-annexin V conjugate (vial 1). The lyophilized stannous tricine (vial 2) was reconstituted with 3 mL of sterile saline; an aliquot of the stannous tricine solution (0.3 mL) was added to the HYNIC-rh-annexin V vial, which was mixed gently, allowed to incubate at room temperature, and diluted by the addition of 2 mL of sodium chloride for injection. The vial was then assessed for quality by visual inspection, by pH testing using pH strips, and by radiochemical purity testing using instant thin-layer chromatography silica gel and a solution of acid citrate and dextrose. The drug product was verified to be greater than 90% radiochemical purity, as determined by instant thin-layer chromatography (acid citrate and dextrose), in each dose administered. Each 99mTc-HYNIC-rh-annexin V dose (555–740 MBq [15–20 mCi]) was administered through an indwelling intravenous line, using the sterile syringe filter (0.22 μm) supplied as part of each 99mTc-HYNIC-rh-annexin V kit.
Annexin V Imaging
A dual-head γ-camera (Elscint-Helix) equipped with a pair of low-energy, high-resolution collimators was used for both 99mTc-annexin V and 99mTc-MDP radionuclide imaging. Images were acquired for 5 min in a 256 × 256 matrix simultaneously in anterior and posterior views of the pelvic and thigh area (i.e., for patients with hip prostheses) or in anterior and posterior views of the pelvic and knee area (patients with knee prostheses), 3 h after injection of the tracer. A SPECT study was also performed on each patient using 60 projections of 30 s each, in a 128 × 128 matrix at 6° angular steps. Transaxial, coronal, and sagittal slices (1 pixel thick) were reconstructed using a third-order Metz filter set to 8-mm full width at half maximum.
Image Interpretation
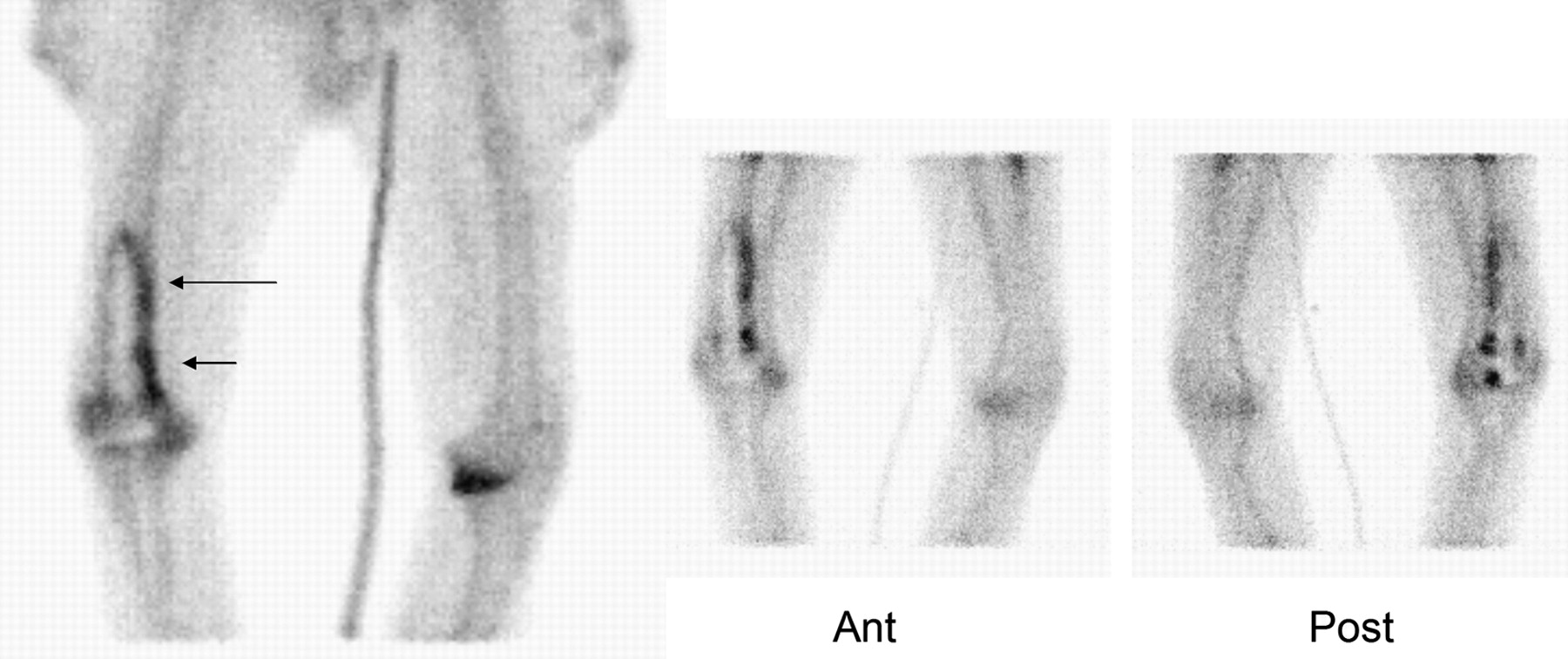
Each scan was assessed by an experienced nuclear medicine physician unaware of the clinical data. Evaluation criteria were as follows. Annexin V scans were considered positive when there was increased abnormal periprosthetic activity greater than that in the contralateral region or ipsilateral adjacent soft tissue. Scans were considered to be negative when the local activity was identical to that present in the contralateral bone segment or in the ipsilateral adjacent bone segment as shown in Figure 1.

A 79-y-old woman with unilateral right hip prosthesis for 15 y. Focus of increased MDP activity is seen at distal aspect of prosthesis, and second focus is seen proximally (planar image on left). Patient's annexin V study was read as negative (planar image on right).
RESULTS
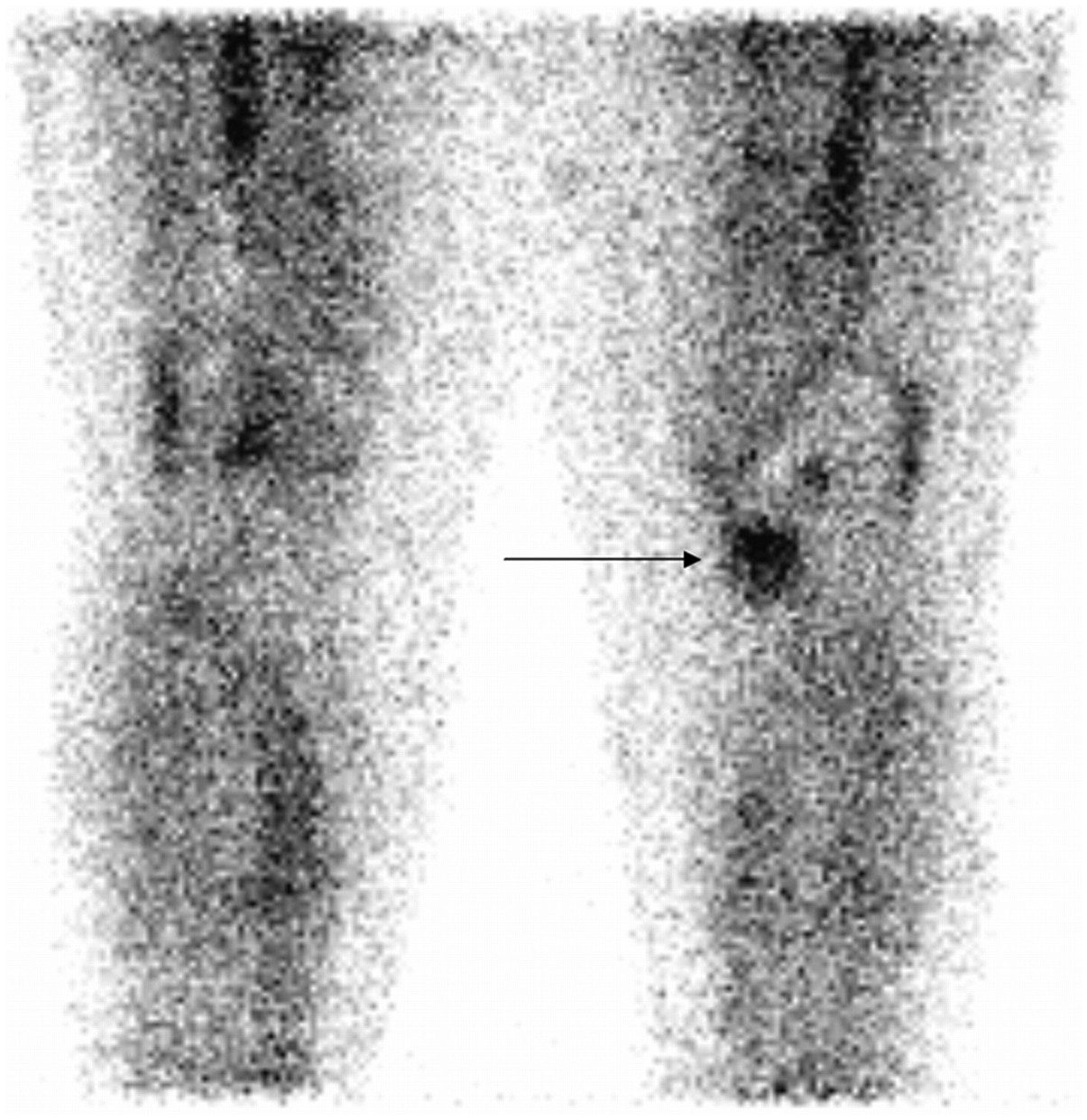
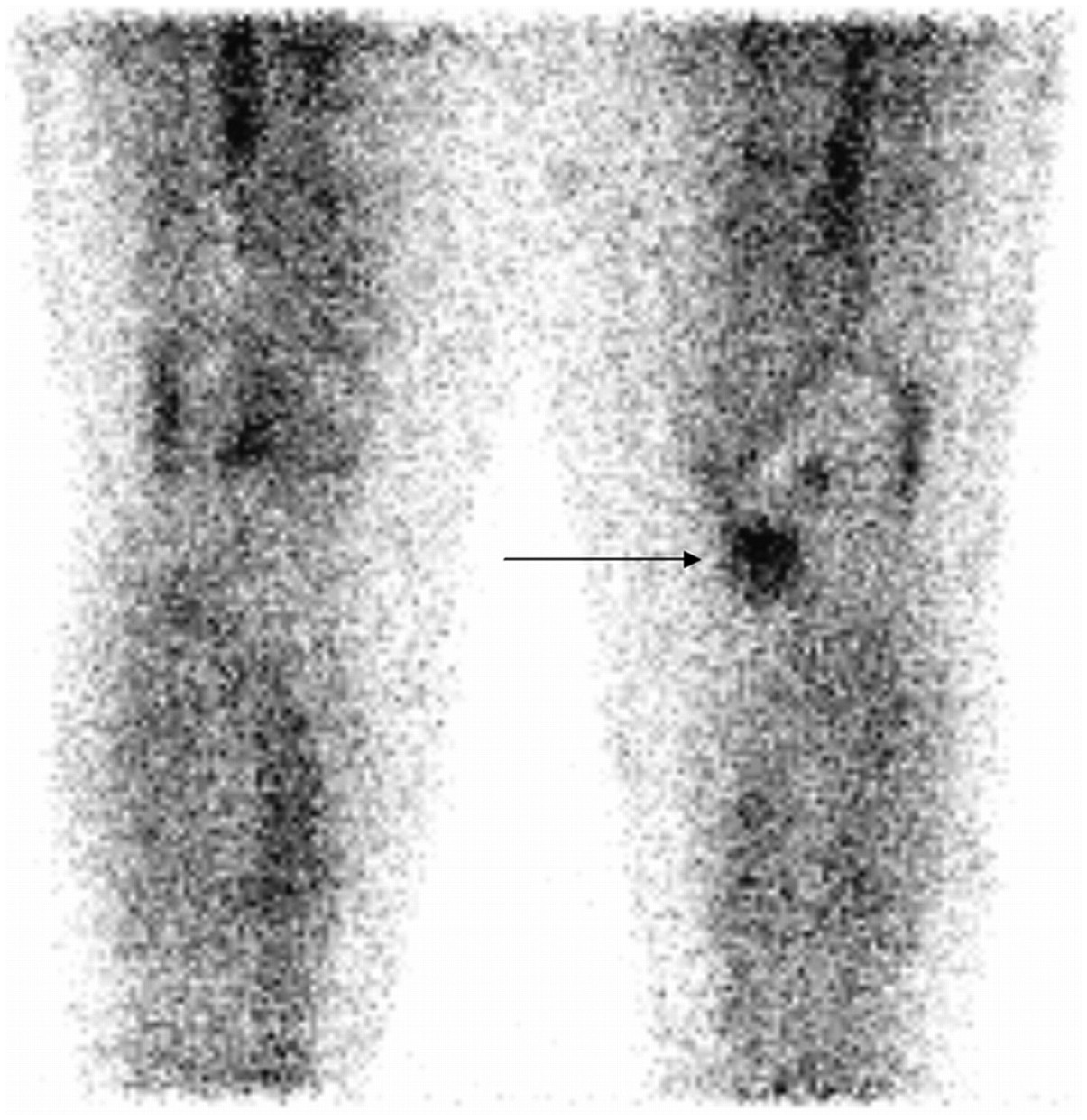
Four patients had a final clinical diagnosis of prosthetic infection, and 3 patients were determined to have no infection after at least 6 mo of follow-up (Table 1). Annexin V imaging results were positive in 5 patients and negative in 2. The pattern of annexin V uptake was focal in 4 of the 5 positive studies (Fig. 2) and linear in 1 (Fig. 3). Increased annexin activity was also seen in infected knee prostheses (Fig. 4). Overall, there were 4 true-positive, 2 true-negative, 1 false-positive (Fig. 5), and no false-negative annexin V imaging examinations, for a sensitivity of 100%, specificity of 67%, negative predictive value of 100%, and positive predictive value of 80%. Compared with the MDP distribution, annexin uptake was either more extensive or less extensive and usually incongruent in distribution with the bone tracer.

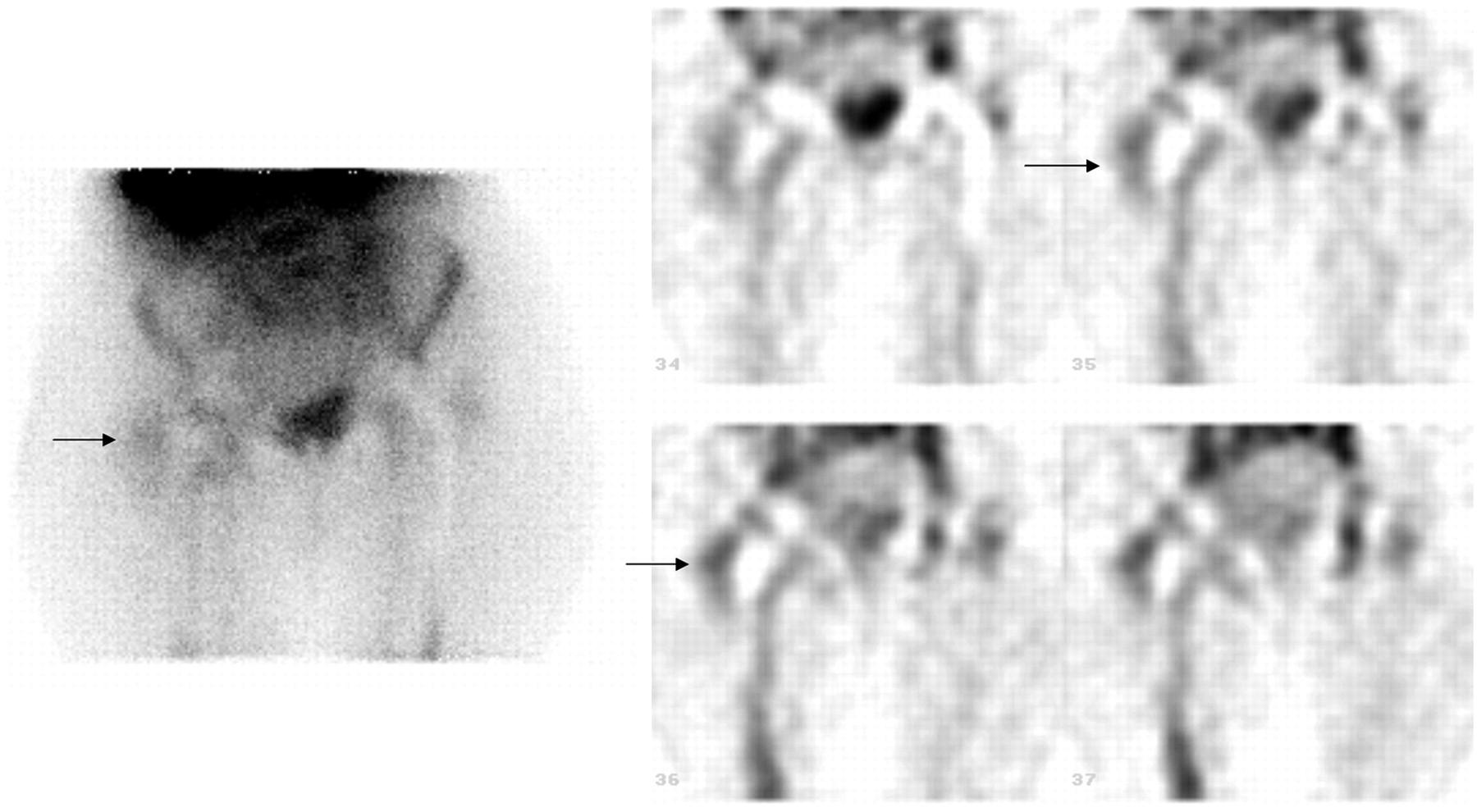
A 77-y-old woman with bilateral hip replacements. Left hip prosthesis shows normal 99mTc-annexin V activity, and right shows increased annexin V uptake on planar image (arrow). Tracer uptake is better visualized on representative coronal SPECT slices shown on right (arrows).

A 78-y-old woman with history of subcapital fracture of her left femur, leading to avascular necrosis and total hip replacement. Patient's bone scan shows diffusely increased MDP uptake around left hip prosthesis (planar image on left). Annexin study shows increased linear uptake on lateral aspect of prosthesis (planar image on right; arrows).
A 76-y-old man with painful unilateral right knee prosthesis and signs of loosening on plain radiograph. Linear increased activity around prosthesis on bone scan (planar image far left; arrows) is demonstrated, with similar activity noted on anterior (Ant) and posterior (Post) views of annexin study (planar images; center and right).
A 69-y-old woman with left knee prosthesis, showing focal increased annexin activity in left medial tibial plateau (arrow) but no evidence of infection.
DISCUSSION
99mTc-HYNIC-annexin V imaging can directly visualize and monitor the temporal activity of apoptosis in animals and humans (9). To our knowledge, this study describes the first reported in vivo examination of apoptosis in patients with hip and knee prostheses using 99mTc-annexin V radionuclide imaging. Although not highly specific for infection, a negative annexin V study in this small preliminary group of patients excluded the diagnosis of infection. Additionally, the remarkable uptake of annexin V that was noted in infected areas is at odds with the findings of other studies that reported a low level of apoptosis in infection, compared with aseptic loosening (10).
The presence of apoptosis has been investigated in the interface membranes collected during revision surgery of aseptically loosened total hip joint arthroplasty (11). Quantitative assays revealed a statistically significant presence of apoptosis in aseptic samples (compared with septic samples, in which apoptosis was almost absent) obtained from both cementless and cemented prostheses. Activated caspase-8 was almost undetectable in septic samples, and in the aseptic samples active caspase-8 was present weakly in the cementless samples and strongly in the cemented ones. In 1 study, apoptosis as seen by DNA fragmentation (late-stage apoptosis) was almost undetectable in samples from septic loosening and appeared significant in samples from aseptic loosening, in accordance with previous findings of a necrotic instead of apoptotic evolution of periprosthetic tissue in the presence of chronic infection.
Another possible explanation for these results is that annexin V localizes not only to sites of apoptosis but also to sites of cellular stress (9). With severe cellular stress, affected cells exhibit increased levels of phosphatidylserine exposure on the plasma membrane. Exposed phosphatidylserine is the target of annexin V binding to apoptotic cells in vitro and in vivo. Although levels of phosphatidylserine expression are lower with cellular stress than with apoptosis, phosphatidylserine expression is still detectable with annexin V imaging and is reversible with prompt therapeutic intervention. In addition, there are at least several alternative pathways by which bacterial infection can induce apoptosis that may not be easily detectable by standard assays. Furthermore, other modes of cell death with increased levels of phosphatidylserine exposure are possible in prosthetic joint infections, including pyroptosis—a pro-inflammatory form of leukocyte cell death induced by certain types of infection and uniquely dependent on caspase-1 (a caspase that is not normally considered part of the classic apoptotic caspase cascade) (12).
Improved longevity and the mounting proportion of the aging population will require a growing number of arthroplasties. Loosening or infection of the prosthesis after joint arthroplasty is relatively common and limits the lifetime of the replacement. The rate of infection after total hip or total knee replacement ranges from 1% to 4% and is higher after revision procedures (13). The differential diagnosis between loosening and infection is challenging and important because treatment strategies are different (1). Treatment of infection after total hip and total knee replacement requires adequate antibiotic therapy and further surgery, and treatment may also require prolonged hospitalization to eradicate the infection. Reimplantation of a prosthesis into an infected tissue bed, without appropriate debridement, is likely to result in persistent infection. Therefore, methods for accurate diagnosis are crucial to reduce the costs of joint replacement and the consequences of misdiagnosis.
Various approaches have been developed to visualize inflammation and infection by nuclear medicine techniques. 99mTc-MDP bone scintigraphy has been the most extensively examined radionuclide study for a painful joint replacement (14). Although increased periprosthetic uptake on a bone scan is suggestive of infection, other conditions including trauma, fractures, tumors, heterotopic ossification, and inflammatory disorders can result in an increased uptake in the periprosthetic tissue and may cause false-positive results. Moreover, bone scan findings can remain positive for as long as 1 y after an uncomplicated hip replacement and for more than 2 y after insertion of a prosthesis without cement (15).
67Ga scintigraphy has proven to be a useful addition to bone scintigraphy in patients with painful joint replacements (16). Although the sensitivity of gallium imaging alone is relatively low (17), the accuracy of combined 99mTc-MDP bone and gallium scintigraphy for detecting joint replacement infection is nearly 80% (18). Controversial results have been reported on the clinical value of 18F-FDG PET in detecting prosthetic joint infection, usually showing only moderate diagnostic performance (19).
The most accurate method for diagnosis of prosthesis infections has been imaging with 111In- or 99mTc-labeled leukocytes, when used in combination with bone or bone marrow scintigraphy (20). However, the time required to complete the procedures and the examination costs appear to represent an important limitation in the use of these modalities.
CONCLUSION
This preliminary study shows that annexin V imaging has a high negative predictive value for infection in hip and knee prostheses. We also found that annexin V uptake in the periprosthetic region is more common and intense in infected prostheses than in aseptic loosening. Prospective studies are needed in larger patient populations to assess features of annexin V imaging that could permit the distinction of aseptic inflammation from infection-related loosening of joint prostheses.
Acknowledgments
We thank Shula Calman and Vered Pilossoff for their expert technical support. This study was supported in part by Theseus Imaging Corporation, Cambridge, Massachusetts.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 4, 2008.
- Accepted for publication December 19, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.