


Abstract
In patients with diabetes mellitus, myocardial perfusion defects are often observed in the absence of obstructive epicardial coronary artery disease (CAD), thereby presenting a diagnostic problem. We hypothesized that these perfusion abnormalities may be explained by endothelial dysfunction or occult coronary atherosclerosis. Methods: Prospectively, 130 asymptomatic patients with diabetes mellitus underwent cardiovascular screening by coronary artery calcium (CAC) scoring, multislice CT coronary angiography, and myocardial perfusion imaging by SPECT. Multislice CT images were evaluated for the presence of obstructive epicardial CAD (≥50% luminal narrowing). To quantify abnormal myocardial perfusion on SPECT images, we determined the summed stress score for each patient. The presence of abnormal myocardial perfusion was defined as a summed stress score of 3 or more. In addition, flow-mediated dilatation of the brachial artery, a marker of endothelial function, was determined using ultrasonography. Results: In 35 patients (27%), obstructive epicardial CAD was observed on multislice CT, and these patients were excluded from further analysis. In the remaining 95 patients, abnormal myocardial perfusion was observed in 30 (32%) of patients. Flow-mediated dilatation was significantly lower in patients with abnormal myocardial perfusion (3.6% ± 2.4%) than in those with normal myocardial perfusion (6.4% ± 2.6%) (P < 0.001). Importantly, flow-mediated dilatation remained a significant predictor of the extent of abnormal myocardial perfusion after correction for cardiovascular risk factors and CAC score (P < 0.001). In contrast, no association was observed between nonobstructive plaque burden as reflected by CAC scores and extent of abnormal myocardial perfusion. Conclusion: In patients with diabetes mellitus, myocardial perfusion abnormalities in the absence of obstructive epicardial CAD are associated with endothelial dysfunction.
Coronary artery disease (CAD) constitutes a major cause of morbidity and mortality in patients with diabetes mellitus. In addition, because of diabetic neuropathy, myocardial ischemia and infarction may be prevalent in the absence of typical anginal symptoms. Noninvasive assessment of CAD in asymptomatic diabetic patients at higher risk has therefore been previously suggested by the guidelines of the American Diabetes Association and the American Heart Association (1). Those guidelines propose testing for the presence of myocardial ischemia by SPECT as a possible option for early detection and treatment of asymptomatic obstructive CAD. If myocardial perfusion abnormalities are identified, coronary angiography is considered to confirm the presence of clinically relevant obstructive CAD possibly requiring intervention. However, previous studies have shown a discrepancy between the presence of myocardial perfusion defects and obstructive CAD in diabetic patients. In approximately 20%−40% of diabetic patients, myocardial perfusion defects could not be clarified by obstruction of the epicardial coronary arteries (2,3). Also, in the general population, a discrepancy between the presence of myocardial perfusion defects and obstructive epicardial CAD has been observed (4–6). Both endothelial dysfunction and occult coronary atherosclerosis were shown to contribute to this condition (4–6). However, the potential mechanisms underlying myocardial perfusion abnormalities not attributable to obstruction of flow in the epicardial coronary arteries have not yet been studied in asymptomatic diabetic patients.
Ultrasonographic measurement of flow-mediated dilatation (FMD) of the brachial artery provides a noninvasive estimation of systemic endothelial function (7). The observed brachial artery dilatation has been shown to be closely related to coronary endothelial function and vasoreactivity (8,9). The reproducibility of assessments of brachial artery diameter has improved with the development of the wall-track system, rendering it suitable for cohort studies (10).
The current study was designed to prospectively evaluate the relationship between myocardial perfusion as assessed by SPECT and endothelial function as assessed by FMD in asymptomatic diabetic patients without epicardial obstructive CAD (as evaluated noninvasively by multislice CT coronary angiography). In addition, the association between nonobstructive plaque burden as reflected by coronary artery calcium (CAC) scores and myocardial perfusion was studied.
MATERIALS AND METHODS
Patients and Design
Prospectively, 130 asymptomatic diabetic patients were screened for cardiovascular disease. A structured interview, physical examination, and laboratory analysis were performed. Cardiovascular risk factors were assessed according to the following criteria. A family history of CAD was considered positive if CAD was present in any first-degree family member. Hypertension was defined as blood pressure greater than 140/90 mm Hg or treatment with antihypertensive medication. Hypercholesterolemia was defined as a total cholesterol level greater than 5.0 mmol/L or the use of lipid-lowering medication.
Noninvasive multislice CT, including CAC scoring and coronary angiography, and myocardial perfusion imaging by SPECT were performed as part of the clinical work-up of all patients. Concurrent measurement of brachial FMD was performed in a study setting approved by the institutional review committee of the Leiden University Medical Center.
Primarily, patients not eligible for multislice CT coronary angiography because of arrhythmia or contraindications to the use of iodinated contrast medium were excluded. Subsequently, those with obstructive epicardial CAD on multislice CT angiography were excluded from further analyses. The relationship between the presence of myocardial perfusion defects and FMD was thereby assessed in the remainder of patients free of obstructive epicardial CAD.
Multislice CT Data Acquisition
Imaging was performed with a 64-slice multislice CT scanner (Toshiba Medical Systems). In patients with a heart rate of at least 65 beats per minute, oral β-blocking medication (metoprolol, 50 mg or 100 mg), if tolerated, was provided 1 h preceding the scan. A nonenhanced prospective electrocardiographically gated scan, triggered at 75% of the R-R interval with 4 × 3.0-mm collimation was first obtained to measure the CAC score and to determine the start and end positions of the helical scan.
Subsequently, multislice CT angiography was performed using the following parameters: collimation, 64 × 0.5 mm; tube rotation time, 400, 450, or 500 ms, depending on the heart rate; tube current, 300 or 350 mA; and tube voltage, 120 kV. Nonionic contrast material was administered in the antecubital vein (90–100 mL, depending on the total scan time) at a flow rate of 5 mL/s, followed by 50 mL of saline solution flush. Timing of the scan was determined by automated bolus tracking in the aortic root. Data were acquired with simultaneous electrocardiography registration during a single breath-hold of approximately 10 s. Images were reconstructed in the cardiac phase that showed the fewest motion artifacts and were transferred to a remote workstation (Vitrea 2; Vital Images) for postprocessing.
Multislice CT Data Analysis
CAC Score
The CAC score was assessed using dedicated software (Vitrea 2). CAC was defined as a dense area in the coronary artery exceeding the threshold of 130 Hounsfield units. For each patient, the total Agatston score was determined.
Epicardial Obstructive CAD
Two experienced observers who were unaware of patient characteristics interpreted all multislice CT coronary angiograms. Discrepancies in interpretation were instantly resolved by consensus. Epicardial coronary arteries were examined by scrolling through axial images, followed by visual assessment of curved multiplanar reconstructions in at least 2 orthogonal planes. The presence of epicardial obstructive CAD (defined as luminal narrowing ≥ 50% in at least 1 vessel) was evaluated for each patient.
ECG-Gated SPECT Data Acquisition
During a 2-d stress and rest protocol, myocardial perfusion imaging was performed using ECG-gated SPECT with 99mTc-sestamibi. Patients were instructed to abstain from caffeine-containing products for 24 h preceding the stress test. Stress was induced using an intravenous infusion of adenosine at a rate of 140 μg/kg of body weight per minute for 6 min, accompanied by simultaneous handgrip exercise. After completion of the third minute, 99mTc-sestamibi (500 MBq) was injected intravenously. Blood pressure and a 12-lead electrocardiograph were recorded throughout the adenosine infusion. Imaging using a triple-head SPECT γ-camera (GCA 9300/HG; Toshiba Corp.) equipped with low-energy high-resolution collimators commenced 120 min after radiopharmaceutical injection. Images were acquired in accordance with American Society of Nuclear Cardiology guidelines, using a circular 360° orbit, 60 projections, and 40 s per projection. Attenuation correction was not applied. Images were processed in the usual manner, and short-axis, horizontal long-axis, and vertical long-axis views were reconstructed. Patient motion was evaluated through examination of the raw cine images.
SPECT Data Analysis
Short-axis slices were displayed in polar map format, adjusted for peak myocardial activity of 100%. Additional reconstruction yielded standard long- and short-axis projections perpendicular to the heart axis. All views were used for semiquantitative interpretation. As proposed by the American Society of Nuclear Cardiology guidelines, the myocardium was divided into 17 segments (11). Tracer uptake in each segment was evaluated by 2 observers in consensus, by use of a 5-point scoring system (0, normal reduction of tracer uptake; 1, mild reduction of tracer uptake; 2, moderate reduction of tracer uptake; 3, severe reduction of tracer uptake; and 4, apparent absence of tracer uptake). The total segmental score during stress and rest was used to determine the summed stress score (SSS) and summed rest score for each patient. Abnormal myocardial perfusion was defined as an SSS of at least 3. Patients with an SSS of 3–7 were classified as having moderately abnormal myocardial perfusion, and those with an SSS of at least 8 were classified as having severely abnormal myocardial perfusion. The location of myocardial perfusion abnormalities was classified as apical, anterior, inferior, or lateral (11). Finally, regional wall motion on gated SPECT images was analyzed to differentiate between true perfusion abnormalities and attenuation artifacts.
FMD
The brachial artery diameter was evaluated using a wall-track system (Scanner 200; Pie Medical), which consisted of an ultrasound imager with a 7.5-MHz linear array transducer connected to a data acquisition system and a personal computer. The principles of this system have been previously described in more detail (12). All measurements were performed by the same experienced sonographer, who was unaware of the clinical characteristics of the patients. On the basis of a previous study of 20 healthy middle-aged volunteers, the intraobserver coefficients of variation for FMD assessment by the same sonographer were previously determined to be 0.8% for the baseline diameter of the brachial artery, 2.0% for the maximal diameter, 24.2% for the change in diameter, and 24.4% for the calculated FMD. The mean FMD in this group of healthy volunteers was 8.4% ± 2.1%.
In the current study, patients were asked to abstain from medication use, caffeine-containing substances, and smoking for 24 h before the tests. All measurements were performed on fasting patients, in the morning, in a silent, temperature-controlled clinical research laboratory. Patients had a 15-min rest in a comfortable supine position and remained in that position throughout the examination. The patients' right arm was placed in extension in the elbow, with the hand in supination, thus eliminating longitudinal movements of the arm. The wrist and elbow were supported by cushions to minimize lateral movements. The heart rate was continuously monitored by a 3-lead electrocardiogram. The brachial artery was visualized distal to the elbow. First, 3 diastolic measurements were averaged to provide a baseline diameter. Then, ischemia was applied to the forearm distal to the location of the transducer by inflation of a blood pressure cuff for 5 min at a pressure of 200 mm Hg. After cuff deflation, ultrasonography continued for 5 min with measurements at 30-s intervals. The widest lumen diameter was used as maximal vasodilation. FMD was expressed as percentage change relative to the baseline diameter.
Statistical Analysis
Primarily, patients with obstructive epicardial CAD (≥50% luminal narrowing) on multislice CT angiography were identified and excluded from all further analysis.
Continuous variables were expressed as mean ± SD. Categoric variables were expressed as number, followed by percentage in parentheses.
To investigate the relationship between FMD and myocardial perfusion, we first stratified patients as having either normal myocardial perfusion (SSS < 3) or abnormal myocardial perfusion (SSS ≥ 3) on SPECT. Average FMD and SD were calculated for both groups, and the independent t test was applied to evaluate the difference in mean FMD.
To determine the relationship between cardiovascular risk factors and degree of myocardial perfusion abnormalities, a univariate linear regression analysis of baseline characteristics was performed to identify the potential predictors of the number of SSS. Thereafter, multivariate linear regression analysis with backward elimination was performed to identify the independent predictors of the number of SSS.
Finally, the relationship between FMD and prevalence of abnormal myocardial perfusion, as well as between the degree of nonobstructive atherosclerosis and abnormal myocardial perfusion, were evaluated. For this purpose, patients were first categorized according to FMD quartiles, and the prevalence of abnormal myocardial perfusion was determined for each FMD quartile. Subsequently, patients were stratified as having a CAC score of 0, 1–10, 11–100, or more than 100, and the prevalence of abnormal myocardial perfusion was assessed per CAC category. The influence of decreasing FMD (per quartile) and that of increasing CAC scores (per category) on the prevalence of abnormal myocardial perfusion was investigated.
RESULTS
Patient Characteristics
In the total population, multislice CT coronary angiography revealed obstructive epicardial CAD (≥50% luminal narrowing) in 35 patients (27%), and these patients were therefore excluded. The characteristics of the remaining 95 patients (73%) included in the analysis are provided in Table 1. Briefly, the mean age of this population was 48 ± 12 y, and 43 patients (46%) were male.
Characteristics of Study Population
Baseline Imaging Findings
Assessment of Myocardial Perfusion by SPECT
The mean SSS was 2.0 ± 3.0 (range, 0–13) in patients included in the analysis. In this asymptomatic diabetic population without obstructive epicardial CAD, myocardial perfusion abnormalities (SSS ≥ 3) were observed in 30 patients (32%). Within this group, moderately abnormal myocardial perfusion (SSS 3–7) was revealed in 25 patients (83%), whereas 5 patients (17%) were shown to have severely abnormal myocardial perfusion (SSS ≥ 8). Furthermore, observed myocardial perfusion abnormalities were reversible in 14 patients (47%), partially reversible in 6 (20%), and fixed in 10 (33%). Of note, fixed myocardial perfusion abnormalities comprised mainly a light or moderate decrease in tracer uptake (n = 8). Only 2 patients with a fixed abnormality were shown to have a severe decrease in tracer uptake. In total, 6 patients showed abnormal perfusion apically: 16 patients in the anterior wall of the myocardium, 15 in the inferior wall, and 8 in the lateral wall. Overall, 16 patients showed a myocardial perfusion abnormality in a single myocardial wall, 13 patients in 2 walls, and 1 patient in 3 walls.
Assessment of Endothelial Function by FMD
Mean FMD was 6.0% ± 3.0%, and FMD ranged from 0.0% to 13.3%. The median FMD was calculated to be 5.4% (lower quartile, 3.4%; upper quartile, 7.3%).
Assessment of CAC Score by Multislice CT
The average CAC score was 60 ± 170. Most patients (n = 53, 55%) had no coronary calcium. The CAC score was found to be in the range of 1–10 in 12 patients (13%), 11–100 in 15 patients (16%), and more than 100 in 15 patients (16%).
Relationship Between FMD and Abnormal Myocardial Perfusion
In diabetic patients with normal myocardial perfusion, the mean FMD was significantly higher (6.4% ± 2.6%) than in patients with abnormal myocardial perfusion (3.6% ± 2.4%) (P < 0.001) (Fig. 1).
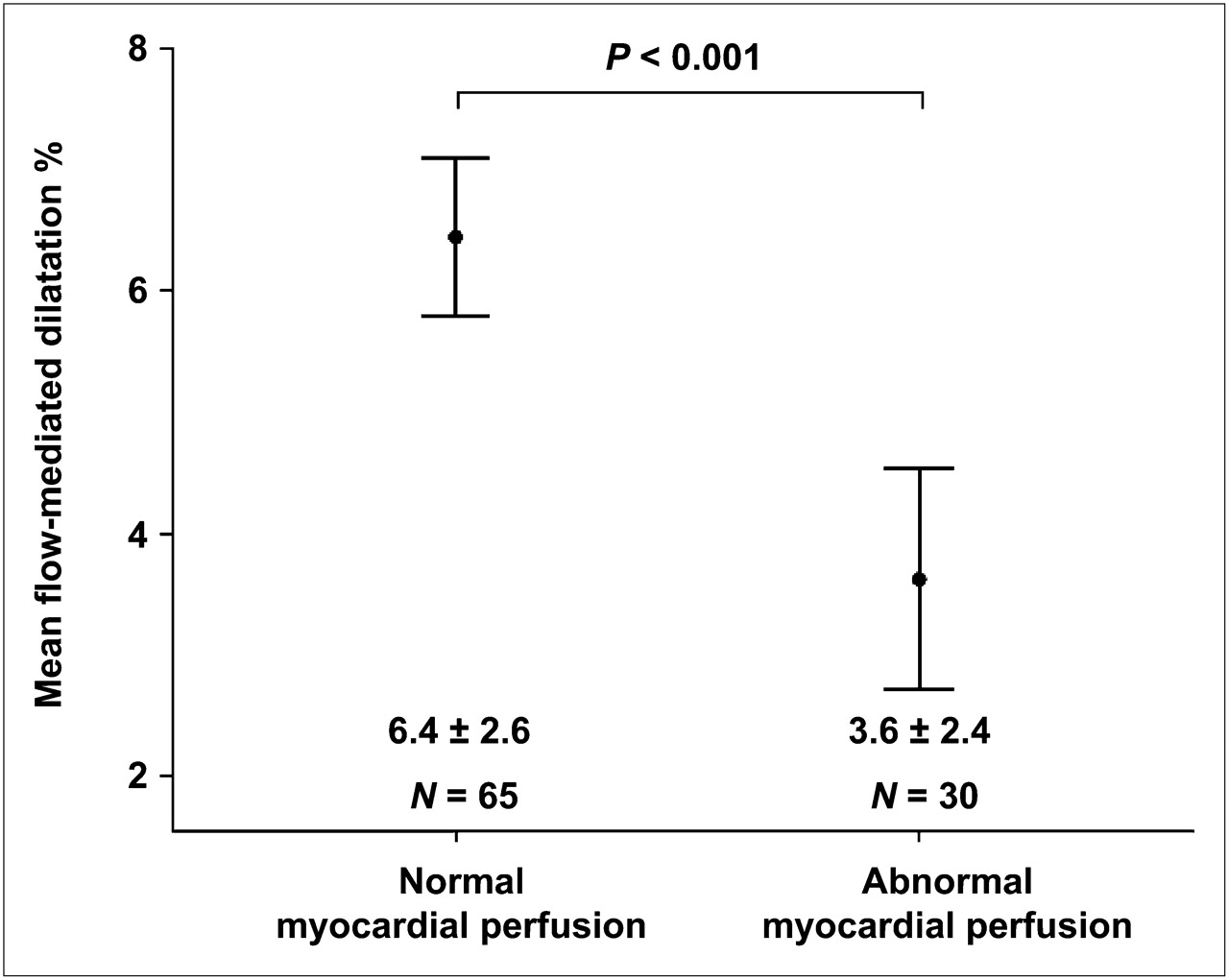
FMD in diabetic patients with normal and abnormal myocardial perfusion. Mean FMD was significantly lower in patients with abnormal myocardial perfusion.
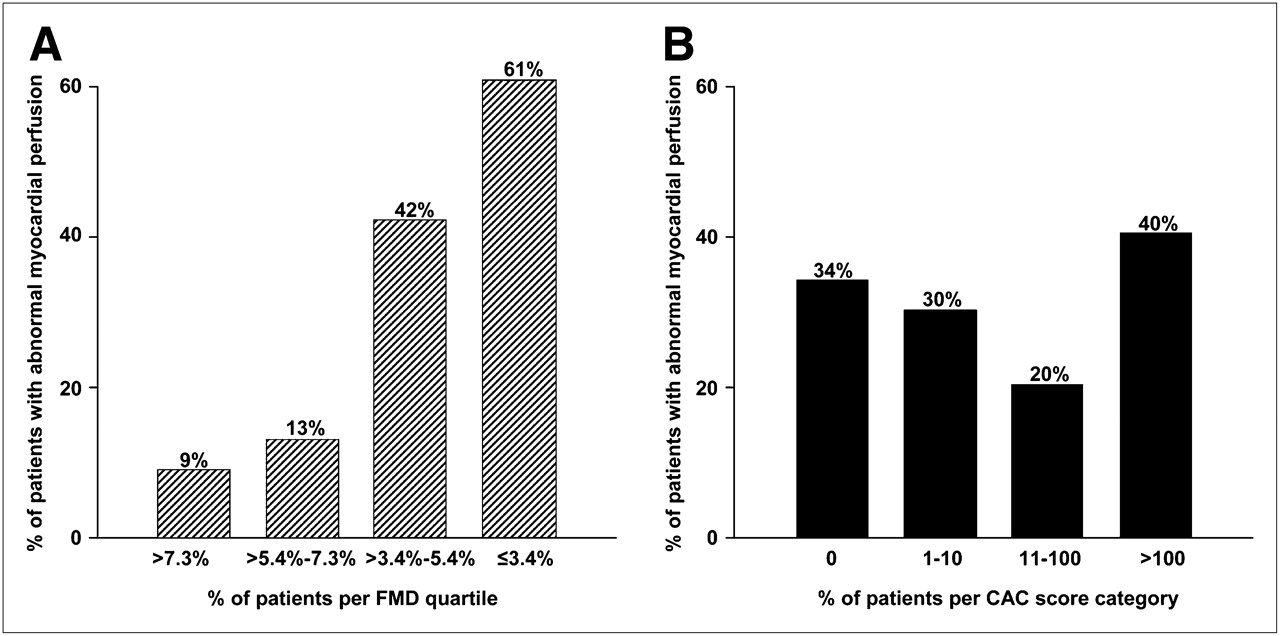
The prevalence of patients with abnormal myocardial perfusion per FMD quartile or CAC score category is provided in Figure 2A. Interestingly, the prevalence of myocardial perfusion abnormalities increased gradually from 9% to 61% with decreasing FMD quartiles.

Percentage of patients with abnormal myocardial perfusion per FMD quartile or CAC score category. Prevalence of abnormal myocardial perfusion increased with decreasing FMD (A), whereas no clear trend was observed among increasing CAC score categories (B).
In contrast, no trend was evident between the prevalence of abnormal myocardial perfusion and increasing CAC score categories (Fig. 2B). Although 34% of patients without coronary calcium showed abnormal myocardial perfusion, a similar prevalence (40%) was observed in patients with extensive coronary calcium (CAC > 100).
Predictors of the Extent of Abnormal Myocardial Perfusion
As illustrated in Table 2, FMD was the only significant predictor of the extent of abnormal myocardial perfusion in a univariate model (P < 0.001). Importantly, after correction for other cardiovascular risk factors in a multivariate model with backward elimination, FMD remained a significant predictor of the extent of abnormal myocardial perfusion (P < 0.001) (Table 2). Hemoglobin A1c and hypercholesterolemia were also shown to be independent predictors of the extent of abnormal myocardial perfusion.
Predictors of Extent of Abnormal Myocardial Perfusion (SSS) in Patients Without Obstructive Epicardial CAD
DISCUSSION
The current prospective study revealed that 32% of asymptomatic patients with diabetes mellitus had abnormal myocardial perfusion despite the absence of obstructive epicardial CAD. Assessment of brachial FMD showed less vasoreactivity in these patients than in those with normal myocardial perfusion. Importantly, after correction for risk factors and CAC scores, endothelial function remained a significant predictor of abnormal myocardial perfusion. Further analysis showed the prevalence of myocardial perfusion abnormalities to increase per decreasing FMD quartile, whereas no such trend was observed for occult atherosclerotic plaque burden as determined by CAC scoring.
Assessment of Myocardial Perfusion by SPECT
In the general population of patients with known or suspected CAD, myocardial perfusion imaging by SPECT has been shown to successfully identify obstructive CAD and predict future coronary events (13,14). The prognostic value of myocardial perfusion has also been confirmed in diabetic patients with suspected CAD, as well as in asymptomatic diabetic patients (15–17). Based on these observations in combination with the noninvasive nature of MPI by SPECT, the American Diabetes Association and the American Heart Association have proposed this technique as a potential screening tool for identification of asymptomatic diabetic patients with obstructive CAD (1). However, previous studies in diabetic patients imply that a significant proportion of observed perfusion abnormalities is not attributable to obstruction of blood flow in the epicardial coronary arteries (2,3). In the general population, a similar discrepancy has been observed regarding presentation with anginal symptoms and manifested ischemia in the absence of obstructive epicardial CAD (4–6). Mechanisms underlying myocardial perfusion abnormalities in that particular group of patients have been studied extensively and revealed the presence of diffuse coronary atherosclerosis and endothelial dysfunction as potential causal factors (4–6). However, little is known about the contribution of these parameters to the occurrence of myocardial perfusion defects in asymptomatic patients with diabetes mellitus. Therefore, in the current study we examined the influence of endothelial dysfunction and nonobstructive atherosclerotic plaque burden on myocardial perfusion in asymptomatic diabetic patients without epicardial obstructive CAD.
Assessment of Endothelial Function by FMD
Assessment of systemic endothelial function by FMD has been shown to relate closely to coronary vasoreactivity (8,9). To date, measurement of brachial FMD is accepted as the most validated and reproducible noninvasive technique for assessment of endothelial function (7). Interobserver reproducibility of the baseline and maximum postischemic brachial artery is satisfactory, with diameter variations of approximately 4%, and has improved with the introduction of semiautomated wall-track systems (10,18). In contrast, the intraobserver reproducibility is limited by within-subject variability and surrounding factors, as vasoreactivity fluctuates through the day and is further influenced by stress, temperature, diet, and glucose levels (10). Therefore, FMD appears to be less applicable to individual serial testing. However, a panel of experts has recognized the test as appropriate for cohort studies, provided that patient and surrounding factors are standardized (19). FMD ranges from approximately 20% in young adults to 0% in patients with established CAD (20). In diabetic patients, mean FMD values tend to be lower as well (range, 0%−12%) (20). In diabetes mellitus, endothelial dysfunction is suspected to be induced by hyperglycemia (sorbitol, hexosamine, protein kinase C, and advanced glycation end product pathways) and insulin resistance, which result in mitochondrial superoxide overproduction. As a consequence, nitric oxide availability is negatively affected, leading to endothelial dysfunction (21,22).
Relationship with Myocardial Perfusion
In the current study, FMD of the brachial artery was further decreased in diabetic patients with abnormal myocardial perfusion. Several studies have described an association between endothelial dysfunction and the occurrence of myocardial ischemia due to impaired endothelium-dependent coronary vasodilation during stress (23). It is therefore presumable that in the current study insufficient vasomotor response in the coronary microvasculature due to endothelial dysfunction may indeed have resulted in relative hypoperfusion during stress (reflected by reversible perfusion abnormalities on SPECT) in the absence of obstructive epicardial CAD (23). However, endothelial dysfunction has also been shown to affect resting myocardial perfusion (24). Accordingly, hypoperfusion of the microvasculature during rest may occur. Interestingly, in our study most fixed perfusion abnormalities comprised a mild decrease in tracer uptake, which has been linked to hypoperfused but viable myocardial tissue rather than scarring (25). Nevertheless, impaired coronary endothelial function has also been suggested as a cause of myocardial infarction in patients with minimally obstructive disease, possibly through prolonged vasoconstriction (26). Therefore, it is possible that the fixed abnormalities comprising severely decreased tracer uptake, which we observed in 2 patients, may indeed reflect loss of viable myocardium. Finally, the possibility remains that some of the fixed perfusion abnormalities were due to attenuation. However, in the current study, regional wall motion on gated SPECT images was analyzed for optimal differentiation between true perfusion abnormalities and attenuation artifacts.
Importantly, FMD was shown to be an independent predictor of the extent of abnormal perfusion, even after correction for occult coronary atherosclerosis by means of CAC scores. Accordingly, it appears that in the absence of epicardial obstructive CAD, endothelial dysfunction may have a greater impact on myocardial perfusion than the extent of diffuse atherosclerosis. Further investigations are needed to confirm these observations.
Potential Clinical Implications
The direct cardiovascular prognostic consequence of endothelial dysfunction in diabetic patients remains to be determined. In previous studies of nondiabetic patients, impaired endothelial function has been shown to predict cardiovascular events (27). In addition, Bugiardini et al. showed that reduced coronary vasoreactivity in angiographically normal coronaries was a predecessor of overt atherosclerosis on angiography after a long-term follow-up of 10 y (28). Therefore, dysfunction of the endothelium seems to occur in early stages of vascular disease and may be reversible. Accordingly, cholesterol-lowering therapy has been shown to improve endothelium-dependent vasomotion in patients with hypercholesterolemia, as well as myocardial perfusion in a nondiabetic cohort of patients with previous evidence of myocardial perfusion defects on SPECT (29,30). In line with these observations, inducible ischemia was shown to resolve in 79% of asymptomatic diabetic patients who had abnormal myocardial perfusion at baseline in the Detection of Ischemia in Asymptomatic Diabetics study (31). This recovery was associated with intensification of treatment with statins, aspirin, and angiotensin-converting enzyme inhibitors.
Thus, in the current study, abnormal myocardial perfusion not attributable to obstructive CAD was related to impaired endothelial function. Because this condition is most likely to be an early stage of vascular disease amenable to treatment, intensification of antiatherogenic therapy seems to be indicated in asymptomatic diabetic patients with perfusion abnormalities even in absence of obstructive epicardial CAD.
Furthermore, considering that in diabetes mellitus abnormal myocardial perfusion is often observed in the absence of epicardial obstructive CAD, the question emerges of whether this test should be accompanied by a noninvasive anatomic test such as multislice CT coronary angiography. Indeed, referral of all asymptomatic diabetic patients with abnormal myocardial perfusion for invasive coronary angiography should be avoided considering that many patients will not have obstructive epicardial stenosis amenable to revascularization. Accordingly, combined noninvasive imaging of myocardial perfusion imaging by SPECT and coronary anatomy by multislice CT may allow a more comprehensive and accurate assessment of CAD and facilitate further management. However, routine combination of these 2 noninvasive imaging modalities carries the disadvantage of increased costs and radiation exposure. Possibly, multislice CT coronary angiography could have the greatest incremental value in asymptomatic diabetic patients with abnormal myocardial perfusion, to differentiate between obstructive epicardial CAD and endothelial dysfunction as a causal factor.
Study Limitations
First, the size of the study population was limited. In addition, we acknowledge that brachial FMD is a measure of systemic endothelial function and not a direct measure of coronary endothelial function. However, previous studies have shown a good correlation between brachial FMD and direct invasive measures of coronary endothelial function (13,14). Furthermore, the radiation burden associated with combined multislice CT (64-slice multislice CT [∼9–15 mSv]) and SPECT myocardial perfusion imaging (99mTc-sestamibi [∼7 mSv per scan]) is a limitation (32,33). However, the radiation dose of multislice CT has been decreased significantly with the dedicated dose-reduction multislice CT acquisition techniques that have recently become available (34,35). Finally, no follow-up data were available, and whether our observations have prognostic implications should be evaluated in prospective follow-up studies.
CONCLUSION
In asymptomatic diabetic patients with no obstructive epicardial CAD, abnormal myocardial perfusion is common and is strongly associated with impaired endothelial function. In view of the likely reversible nature of endothelial dysfunction and the cardiovascular prognostic value of abnormal myocardial perfusion in asymptomatic diabetic patients, it is presumable that asymptomatic diabetic patients with abnormal myocardial perfusion will benefit from intensified pharmacologic treatment even in the absence of obstructive epicardial CAD.
Acknowledgments
The study was supported in part by grants from Medtronic, Biotronik, Boston Scientific, BMS Medical Imaging, St. Jude Medical, GE Healthcare, Edwards Lifesciences, Astra Zeneca, Pfizer, and MSD.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 15, 2009.
- Accepted for publication August 20, 2009.





{kind=link}
{kind=link}