


Abstract
The objective of this analysis was to assess the radiation exposure associated with 90Y-ibritumomab tiuxetan when used as consolidation therapy in adults with low or minimal tumor burden after first-line therapy of advanced follicular lymphoma (FL). Methods: The patients who were enrolled in the phase 3 first-line indolent trial were 18 y or older, with CD20+ grade 1 or 2 stage III or IV FL, and a partial response, complete response, or unconfirmed complete response to first-line chemotherapy. The patients were allocated randomly to receive a single infusion of unlabeled rituximab 250 mg/m2 on day −7 and consolidation on day 0 with a single dose of 90Y-ibritumomab tiuxetan, 14.8 MBq/kg, immediately after unlabeled rituximab, 250 mg/m2, or no further treatment. On day −7, a subset of patients received an injection of 185 MBq of 111In-ibritumomab tiuxetan immediately after unlabeled rituximab, 250 mg/m2, for central dosimetry analysis. Correlations were assessed between organ radiation absorbed dose and toxicity, body weight, body mass index, and progression-free survival. Results: Central dosimetry evaluations were available from 57 of 70 patients. Median radiation absorbed doses were 100 cGy (range, 28–327 cGy) for the red marrow and 72 cGy (range, 46–106 cGy) for the whole body. Radiation absorbed doses did not differ significantly between patients who had a partial response or complete response to initial therapy. Progression-free survival correlated significantly with the whole-body (r = 0.4401; P = 0.0006) and bone marrow (r = 0.2976; P = 0.0246) radiation dose. Body weight was significantly negatively correlated with whole-body radiation dose (r = −0.4971; P < 0.0001). Neither the whole-body radiation dose nor the bone marrow radiation dose correlated with hematologic toxicity. Conclusion: In patients with low or minimal residual tumor burden after first-line chemotherapy of advanced FL, whole-body and bone marrow exposure after 90Y-ibritumomab tiuxetan consolidation showed a significant positive correlation with progression-free survival, whereas dosimetric data could not predict hematologic toxicity.
Follicular lymphoma (FL) is the most common form of indolent non-Hodgkin lymphoma (NHL) in the United States and the European Union. The disease course of advanced-stage FL is characterized by recurrent relapses and remissions that decrease in duration over time (1). Although the relatively recent introduction of approaches combining monoclonal antibody therapy and chemotherapy has been estimated to have extended the previously reported 7- to 10-y median survival of patients with advanced FL (2,3), the need for treatment optimization remains, because such patients most likely will not be cured.
Because FL is radiosensitive, radioimmunotherapy is well suited to its treatment. Recently, an expert panel of oncologists, hematologists, and nuclear medicine physicians recommended the incorporation of radioimmunotherapy into national lymphoma treatment algorithms across Europe (4). Currently, the murine anti-CD20 monoclonal antibodies 90Y-ibritumomab tiuxetan (Zevalin; Bayer Schering Pharma AG) and 131I-tositumomab (Bexxar; GlaxoSmithKline) are registered in the United States for the treatment of relapsed or refractory low-grade or follicular NHL (5,6). In the European Union, 90Y-ibritumomab tiuxetan is also indicated as consolidation therapy after remission induction in previously untreated patients with FL (7), whereas 131I-tositumomab is not registered in Europe. As for chemotherapy, response rates after radioimmunotherapy tend to be higher and response durations tend to be longer when radioimmunotherapy is given during the early stage of the disease rather than after numerous earlier treatment courses (4,8). Excellent results have been obtained with 131I-tositumomab given as first-line therapy in FL (9).
Another approach consists of consolidation therapy in patients with an initial response to induction therapy. This paradigm may be particularly applicable for radioimmunotherapy in patients with advanced FL, as most patients who achieve a complete response (CR) or a partial response (PR) to initial therapy ultimately relapse and eventually die. Rapidly improving the quality of the initial response in patients with advanced FL may extend the response duration and improve survival. Retrospective analyses have indicated that the use of 90Y-ibritumomab tiuxetan does not compromise the efficacy or safety of subsequent therapy (4).
90Y-ibritumomab tiuxetan consolidation therapy was initially investigated in phase 2 trials that have shown promising results in terms of conversion from PR to CR and progression-free survival (PFS) (10,11). Recently, results of the phase 3, randomized first-line indolent trial showed that in patients with advanced FL who achieved at least a PR to different induction therapies, consolidation therapy with a single dose of 90Y-ibritumomab tiuxetan significantly prolonged PFS by 2 y, compared with no further treatment (12). Of 101 patients who achieved a PR with induction therapy, 78 converted to a CR after 90Y-ibritumomab tiuxetan consolidation therapy.
Dosimetry is incorporated into the design of radioimmunotherapy regimens to determine radiation exposure to various organs and to confirm tumor targeting. During the early development of 90Y-ibritumomab tiuxetan, dosimetry analyses in numerous clinical trials of adult patients with relapsed or refractory NHL showed that radiation absorbed dose estimates to bone marrow and other organs were within safety limits and did not correlate with toxicity (13–15). Therefore, dosimetry is not required with 90Y-ibritumomab tiuxetan when used in patients with relapsed or refractory NHL; instead, the activity to be administered is determined by patient weight and baseline platelet count (7). In contrast, radioiodine-labeled antibody conjugates tend to present with less predictable biokinetics. Consequently, dosimetry is mandatory before radioimmunotherapy with 131I-tositumomab to determine the appropriate activity to deliver a whole-body dose of 75 cGy (16).
When radioimmunotherapy is used for new applications, it is important to determine radiation absorbed dose estimates and their correlation with toxicity (17). The objectives of the current analysis were to assess the radiation exposure associated with 90Y-ibritumomab tiuxetan when given as consolidation therapy to adult patients with advanced FL who had achieved PR or CR after induction chemotherapy and to compare radiation dose with response, hematologic toxicity, and outcome.
MATERIALS AND METHODS
Patient Population
Patient eligibility criteria have been summarized in detail previously (12). Briefly, eligible patients were at least 18 y of age; had CD20+ grade 1 or 2 stage III or IV FL; and had achieved a PR, CR, or unconfirmed CR after first-line chemotherapy by International Workshop Criteria (18). A World Health Organization performance status of 0–2, normal peripheral blood cell counts, and less than 25% bone marrow involvement with lymphoma were also required. All patients provided informed consent before any study procedures were initiated.
Study Design
The first-line indolent trial was a phase 3 randomized international trial performed at 77 study centers in 12 European countries and Canada. A detailed description of the first-line indolent trial study design has been published (12). Briefly, patients were assigned randomly 1:1 to receive a single infusion of unlabeled rituximab, 250 mg/m2, on day −7 and consolidation therapy on day 0 with a single therapeutic dose of 90Y-ibritumomab tiuxetan, 14.8 MBq/kg (maximum activity, 1,184 MBq in patients weighing at least 80 kg), immediately after unlabeled rituximab, 250 mg/m2, or no further treatment (control). The study protocol was approved by the institutional review board at each site, and the study was registered at ClinicalTrials.gov under NCT00185393.
Dosimetry
The first 14 patients in the study underwent mandatory dosimetry as part of an interim safety evaluation, per the study protocol. After it was established that all 14 patients had exposure within safe limits (300 cGy for the red marrow and 2,000 cGy for normal organs), further dosimetry analyses were left to the discretion of the investigators or local needs. For patients who underwent dosimetry, the following treatment schedule was used: on day −7, immediately after receiving the infusion of unlabeled rituximab, 250 mg/m2, patients received an injection of 185 MBq of 111In-ibritumomab tiuxetan. Central dosimetry, based on locally measured blood samples and γ-scans, was performed by a single experienced nuclear medicine physician. Although local dosimetry was also performed, the results of the current analysis are based only on central dosimetry data, as the variation in investigator methods of drawing regions of interest was likely to confound an analysis of local dosimetry data.
At least 3 simultaneous anterior and posterior whole-body scans were performed with a γ-camera at the time points of 15–45 min; 3–6 h; and 1, 3–4, and 6 d after infusion. Blood samples were drawn at corresponding intervals. Radiation absorbed doses were calculated using the region-of-interest technique, the decay constant for 90Y, and the projected activity (14.8 MBq/kg or a maximum activity of 1,184 MBq in patients whose weight exceeded 80 kg) with the MIRDOSE 3 software program. Defined regions of interest included the kidney, liver, lung, spleen, and whole body. Observed residence times of 111In-ibritumomab tiuxetan in these regions of interest, obtained from conjugate anterior and posterior scans (geometric mean), were used in the calculations. Values for organ mass were based on those of the International Commission on Radiological Protection reference male and female. Whole-blood aliquots were counted, normalized, and corrected for decay using the decay constant of 90Y. Bone marrow dose was derived from whole-blood activity decay, corrected for hematocrit and International Commission on Radiological Protection reference male or female bone marrow mass. Hematocrit was considered constant during the measurement period. No correction for the contribution of extramedullary activity to the bone marrow dose was performed.
Response
PFS was determined from the date of randomization to the date of relapse, disease progression, or death (12). Tumor response was assessed by an independent central review board and was based on International Workshop Criteria (18).
Toxicity
Adverse events were recorded throughout the study and graded according to National Cancer Institute Common Toxicity Criteria, version 2 (19). For this particular analysis, only hematologic toxicity was considered.
Statistical Analyses
Descriptive statistics were calculated for estimated radiation absorbed doses. Pearson correlation coefficients were calculated to assess relationships between organ radiation absorbed dose and body weight, body mass index, and PFS. For further analysis, the population was divided into whole-body radiation dose quartiles as follows: quartile 1, 0.55 mGy/MBq < whole-body radiation dose ≤ 0.62 mGy/MBq; quartile 2, 0.62 mGy/MBq < whole-body radiation dose ≤ 0.73 mGy/MBq; quartile 3, 0.73 mGy/MBq < whole-body radiation dose ≤ 0.83 mGy/MBq; and quartile 4, 0.83 mGy/MBq < whole-body radiation dose ≤ 1.12 mGy/MBq.
RESULTS
Patients
Of the 208 patients assigned to receive consolidation therapy with 90Y-ibritumomab tiuxetan, 70 patients received 111In-ibritumomab tiuxetan on day −7. Central dosimetry evaluations were available for 57 patients (Table 1). Whole-body γ-camera scans of a patient at 4 time points after injection of 111In-ibritumomab tiuxetan are shown in Figure 1.
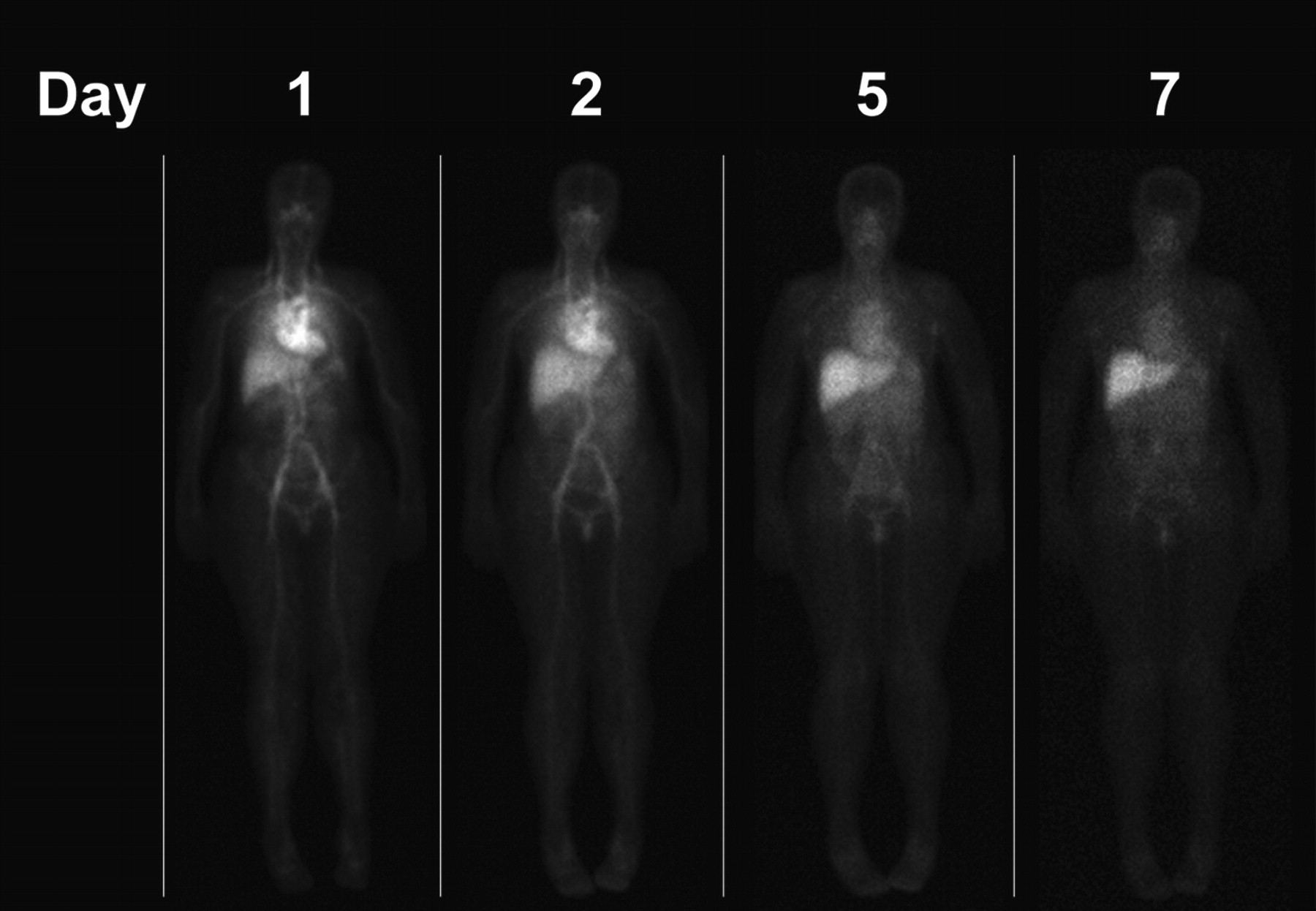
Sequential anterior whole-body γ-camera scans after injection of 111In-ibritumomab tiuxetan. Distribution is normal, and no evidence of residual tumor is seen.
Disposition and Demographics of Patients Who Received 111In-Ibritumomab Tiuxetan and Underwent Central Dosimetry Analysis
Exposure
Median radiation absorbed dose estimates are presented in Tables 2 and 3. The median radiation absorbed dose was 100 cGy (range, 28–327 cGy) for the red marrow and 72 cGy (range, 46–106 cGy) for the whole body. Bone marrow and whole-body radiation doses did not differ between patients who had a PR to initial therapy and those who had a CR to initial therapy (Fig. 2). None of the patients experienced higher than grade 3 anemia. Grades 3 and 4 neutropenia were observed in 44% and 26%, respectively, and grades 3 and 4 thrombopenia in 53% and 2%, respectively, as is in line with previously published results (12). Radiation exposure was within the protocol-defined upper limit to normal organs (2,000 cGy) in all patients and within the protocol-defined upper limit to red marrow (300 cGy) in all but 1 patient, who was treated without complications.

Bone marrow and whole-body radiation doses in patients with PR or CR to initial therapy.
Organ Radiation Absorbed Dose from 90Y, Based on Radiation Exposure by Organ
Organ Radiation Absorbed Dose Factor from 90Y
Response
Before radioimmunotherapy, 35 patients were in CR and 22 were in PR; 15 of these 22 patients (68%) converted to CR after radioimmunotherapy, and 7 remained in PR. The median exposures of whole body and bone marrow in these 3 groups of patients are shown in Table 4. The dose to both bone marrow and whole body was slightly lower in patients who remained in PR, but this difference was not statistically significant.
Bone Marrow and Whole-Body Doses According to Response to Radioimmunotherapy
Correlation Analyses
Patient body weight showed a significant negative correlation with whole-body radiation dose (r = −0.4971; P < 0.0001). Body mass index did not correlate significantly with organ or whole-body radiation doses. In addition, no significant correlation between body mass index and organ or whole-body radiation doses was obtained when the data were analyzed on the basis of response to initial therapy (CR or PR).
PFS correlated significantly with radiation dose to the whole body (r = 0.4401; P = 0.0006) (Fig. 3) and bone marrow (r = 0.2976; P = 0.0246). For the subset of patients (n = 35) who had a CR to initial therapy, PFS correlated significantly with the whole-body radiation dose but not with the bone marrow radiation dose. For the subset of patients who had a PR (n = 22) to initial therapy, PFS correlated significantly with the bone marrow radiation dose but not with the whole-body radiation dose. PFS negatively correlated with body weight (r = −0.3157; P = 0.0168). Neither the whole-body radiation dose nor the bone marrow radiation dose correlated with hematologic toxicity (Table 5). Additionally, we could not show any relationship between bone marrow toxicity and the presence of residual (<25%) bone marrow infiltration or type of induction chemotherapy.

Correlation of PFS with whole-body (WB) radiation dose. Quartile 1 (Q1) = 0.55 mGy/MBq < WB radiation dose ≤ 0.62 mGy/MBq; quartile 2 (Q2) = 0.62 mGy/MBq < WB radiation dose ≤ 0.73 mGy/MBq; quartile 3 (Q3) = 0.73 mGy/MBq < WB radiation dose ≤ 0.83 mGy/MBq; quartile 4 (Q4) = 0.83 mGy/MBq < WB radiation dose ≤ 1.12 mGy/MBq.
No Correlation Between Whole-Body or Bone Marrow Mean Radiation Absorbed Dose and Hematologic Toxicity
DISCUSSION
This dosimetric analysis showed that for patients who received a single dose of 90Y-ibritumomab tiuxetan as consolidation therapy after first remission, median organ radiation absorbed doses were within safe limits. This finding was important to establish, because although dosimetry is not required with 90Y-ibritumomab tiuxetan when used in patients with relapsed or refractory NHL, the population of patients eligible for consolidation therapy has a tumor burden much lower than that of patients with relapsed or refractory disease. It is interesting to note that even in patients with CR according to International Workshop Criteria, radioimmunotherapy with the high-energy electron emitter 90Y was efficient in prolonging PFS for about 2 y compared with controls, whereas mathematic models tend to predict diminished efficacy of long-range β-emitters in small tumors because of inefficient absorption of radiation energy (20).
One can discuss the adequacy of the dosimetry protocol used, based on International Commission on Radiological Protection reference male and female organ and bone marrow mass estimates, which did not correct for attenuation or scatter and estimated bone marrow dose from blood activity decay. Because this was a multicenter study, a robust protocol that could easily be performed in all participating centers was needed. Furthermore, it was important to be able to compare the results of this prospective study of patients with minimal residual disease with previously obtained data with the same compound using the same method to estimate the radiation exposure of the whole body, parenchymal organs, and bone marrow in patients with relapsed or refractory disease after previous chemotherapy. Median radiation absorbed dose to the bone marrow of the 10 patients with less than 25% bone marrow involvement was 92.5 cGy (range, 56–139 cGy), which is comparable to the whole cohort.
The radiation absorbed doses in the current trial were similar to those reported in relapsed or refractory patients treated with 90Y-ibritumomab tiuxetan (13,14). One notable exception was the kidney dose, which was nearly 15-fold higher in the current study than in a combined analysis of 179 patients from 4 previous studies of 90Y-ibritumomab tiuxetan in relapsed or refractory patients (13). In the present study, the median kidney dose was 3.078 mGy/MBq (range, 1.37–9.75 mGy/MBq), whereas it was 0.22 mGy/MBq (range, 0.00–0.95 mGy/MBq) in the analysis of 4 trials (13). However, the radiation absorbed dose to the kidney in the current trial was consistent with results obtained by Cremonesi et al., who compared 3 different methods of estimating organ dose in patients with relapsed or refractory NHL scheduled for high-dose 90Y-ibritumomab tiuxetan conditioning before autologous stem cell transplantation (21). With use of standard organ mass and images not corrected for background, scatter, or attenuation, the median kidney dose was 4.0 mGy/MBq (range, 2.3–8.1 mGy/MBq). These authors obtained somewhat lower kidney doses after background, scatter, and attenuation correction, as well as after adjusting the dose for measured individual organ mass (1.7 mGy/MBq [range, 0.6–3.8 mGy/MBq]), which were still far above those previously reported.
Another study reported a kidney dose of 2.5 mGy/MBq (range, 1.5–4.7 mGy/MBq). These authors calculated the kidney dose from the posterior view only using an effective linear attenuation coefficient determined from phantom studies to correct for kidney depth. They also used background subtraction and individual patient data for kidney mass but no scatter correction. As well, they calculated the left kidney dose, for which the influence of spillover is less important than on the right side, where the liver is overlying part of the kidney. The left kidney dose was 2.1 mGy/MBq (range, 0.92–4.4 mGy/MBq) (22).
Although the dose to the kidneys in the studies described above and in the current study was within safe limits and no renal toxicity was observed in our patients, the findings indicate that one must consider higher kidney exposure when designing high-dose or repeated-dose regimens. The differences in the radiation absorbed dose to the kidneys between the present study and earlier data might reflect differences in tumor burden between the 2 types of patient populations (i.e., patients receiving consolidation therapy after initially having at least a PR versus patients receiving therapy for relapsed or refractory disease). This hypothesis may be supported by a recent dosimetry study of patients with high-risk NHL but low tumor burden after 5 chemotherapy courses, who were scheduled for myeloablative radioimmunotherapy and tandem autologous stem cell support (23). These authors found a median kidney dose of 5.1 mGy/MBq (range, 2.8–10.5 mGy/MBq) based on attenuation and scatter-corrected data, with partial background subtraction and CT–based organ volume measurements. In addition to differences in tumor burden, methodologic and technical factors could contribute to the reported differences. Drawing of the kidney and background regions of interest might be part of the explanation. The relatively low kidney activity might be overestimated by spillover from liver and spleen activity. However, high-energy electrons emitted by 90Y within neighboring organs overlapping the kidneys are likely to contribute to the kidney dose. This phenomenon demands further analysis using more sophisticated dosimetry approaches, including 3-dimensional organ activity measurement (22,24–26).
The median bone marrow dose estimate (0.976 mGy/MBq) in this population was comparable with published results in patients with low or minimal residual tumors (1.0 mGy/MBq) (23), whereas it tended to slightly exceed those obtained in patients with a higher tumor burden (0.62 (13) and 0.8 (21) mGy/MBq). These data were extrapolated from the blood curve, rescaling or not for patients' sex, weight, and height; whereas by measuring antibody uptake by imaging the lumbar spine (L2–L4), Fisher et al. found a substantially higher median red marrow dose of 2.4 mGy/MBq (range, 1.7–4.5 mGy/MBq) in patients with relapsed or refractory NHL and less than 25% bone marrow involvement (27). Interestingly, Cremonesi et al. obtained a median absorbed dose to the bone marrow of 0.8 mGy/MBq using either a fixed ratio (adapted for males and females) of red marrow to measured blood mass or a model using the reference man and woman red marrow volumes, whereas doses to parenchymal organs were lower in a model using various correction parameters and organ mass assessment by CT (21). These results underline the uncertainties in estimating individual red marrow mass in patients after chemotherapy and consequently in calculating marrow exposure. The difficulties increase if the bone marrow contains cells, normal or abnormal, that are targeted by the radiopharmaceutical used for therapy (28).
The most striking result of this study is the correlation between whole-body and bone marrow dose and outcome expressed as PFS after a particularly long observation period (median, 3.5 y), suggesting that PFS with 90Y-ibritumomab tiuxetan may be influenced positively by higher whole-body and bone marrow radiation doses, at least in patients with small or minimal residual tumor burden. In contrast, a 90Y-DOTA humanized anti-CD22 IgG antibody (90Y-epratuzumab) studied in a very heterogeneous patient population showed no correlation of tumor radiation dose with tumor response, as measured by tumor size (29); however, a recent presentation showed that the response rate after fractionated radioimmunotherapy with 90Y-epratuzumab increased with injected activity, suggesting a dose–response relationship (30). A study that used patient-specific SPECT-based 3-dimensional dosimetry of 131I-anti-B1 found no correlation of dose with tumor response (24). In the present study, most residual tumors were too small or not even detectable on 111In-ibritumomab scans or CT images to allow specific tumor dosimetry and, consequently, evaluation of tumor response based on volume measurements. Prolongation of PFS with higher whole-body and bone marrow dose, however, is an even stronger indication in favor of a dose–response relationship expressed by PFS.
In contrast to previously published results that did not find a difference in response rate, time to progression, or toxicity after therapy between patients with relapsed NHL who weighed more than or less than 80 kg, in the present study, whole-body or bone marrow dose and PFS correlated negatively with body weight, suggesting that patients in PR or CR with weight exceeding 80 kg might not receive an adequate radiation dose by the arbitrarily determined maximal activity of 1,184 MBq. In fact, no negative correlation between body weight and outcome was observed in the control group.
However, similar to previous findings with 90Y-ibritumomab tiuxetan (13,14,31) and 90Y-epratuzumab (29), bone marrow radiation doses did not correlate with hematologic toxicity. In contrast, in dosimetry analyses with 131I-labeled antibody therapy, a dose–response relationship between bone marrow absorbed radiation dose and hematologic toxicity was found (32).
CONCLUSION
The efficacy results for the first-line indolent trial demonstrated that consolidation therapy with 90Y-ibritumomab tiuxetan is beneficial in patients with advanced-stage FL. A single therapeutic administration of 90Y-ibritumomab tiuxetan as consolidation after an initial response to induction therapy improved PFS significantly, compared with no further treatment, in a first-line indolent trial (12).
Dosimetry results in patients who received 90Y-ibritumomab tiuxetan as consolidation were consistent with previously published results (13,14), except in the kidneys, where much higher doses were found in the present study. Radiation exposure with 90Y-ibritumomab tiuxetan in patients who have a PR or CR after first-line therapy was within the limits of safety of normal organs and bone marrow.
The unique findings of this study showed that whole-body and bone marrow doses positively correlated with PFS and that patients with excess weight might be insufficiently treated by the predetermined maximum activity of 1,184 MBq of 90Y. There was a negative correlation between body weight and whole-body or bone marrow dose, as well as with PFS. Nevertheless, it is likely not possible to simply translate the results obtained in this population with low tumor burden to patients with recurrent or refractory FL or other types of NHL. However, the finding of a positive correlation between absorbed whole-body or bone marrow dose and PFS in this particular patient population encourages the development of more sophisticated dosimetric approaches and further studies that aim toward outcome rather than solely toward tumor response in larger patient populations with low and minimal tumor burden.
Acknowledgments
This research was supported by Bayer Schering Pharma AG, Berlin, Germany. We thank Stephanie Leinbach and Heather Nyce of SciStrategy Communications for their medical writing assistance on behalf of Bayer Schering Pharma AG. This paper was presented in part at the 49th annual meeting of the American Society of Hematology, December 8–11, 2007, Atlanta, Georgia, and at the annual congress of the European Association of Nuclear Medicine, October 11–15, 2008, Munich, Germany.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 23, 2009.
- Accepted for publication August 11, 2009.





{kind=link}
{kind=link}
{kind=link}