


Abstract
The impact of arrhythmias on the evaluation of perfusion data from myocardial gated SPECT has been assessed by comparing arrhythmic patients with nonarrhythmic patients or by simulating rhythm disturbances. Whether gating-related artifacts may have a clinically relevant influence on the evaluation of perfusion in atrial fibrillation (AF) patients is still uncertain. Recently, collection of nongated and gated datasets during the same SPECT acquisition has become possible. The aim of this study was to examine the difference in myocardial perfusion between simultaneously acquired gated and nongated SPECT data in AF patients. Methods: In 44 consecutive AF patients who underwent myocardial perfusion SPECT for standard clinical indications, both a gated and a nongated study were simultaneously acquired. Perfusion was estimated in a masked manner on a 20-segment model using an established scoring scheme. Results: Agreement was good between the gated and nongated perfusion scores on a segment basis; the agreement for resting scores was the highest, with those for stress and difference scores being lower (Spearman ρ = 0.82, 0.74, and 0.55, respectively). On a patient basis, a similar trend was seen in summed resting scores (ρ = 0.911), summed stress scores (ρ = 0.779), and summed difference scores (ρ = 0.596). When summed stress and summed difference data were grouped by severity class (normal, mild abnormality, moderate abnormality, and severe abnormality), agreement decreased from ρ = 0.818, κ = 0.639, for summed stress score to ρ = 0.549, κ = 0.367, for summed difference score. The severity class of inducible ischemia changed in 17 patients (39%) if a (summed) gated image was used instead of a standard nongated perfusion image. Conclusion: AF may have a clinically relevant impact on summed gated perfusion images, compared with images simultaneously obtained without gating in the same patients. Therefore, acquisition of a nongated SPECT study is mandatory for accurate assessment of myocardial perfusion in AF patients.
The current recommendation for patients with severe arrhythmias, and particularly atrial fibrillation (AF), is that myocardial perfusion SPECT should not be performed with electrocardiography (ECG) gating (1–3). The available studies, which were performed either by comparing the gated SPECT data of arrhythmic patients with the data of nonarrhythmic patients or by altering studies acquired in sinus rhythm to simulate various arrhythmias, suggest that not only functional parameters but also perfusion data may be altered, particularly in AF patients (4,5). Nevertheless, important reports include the gated SPECT perfusion data of AF patients and imply that in these subjects ECG gating can be used, taking into account the limited accuracy in left ventricular functional measurements (6,7). To be certain of the true influence of arrhythmias on perfusion images, one would need to simultaneously acquire both a gated and a nongated SPECT study. Recently, a γ-camera manufacturer has implemented on its system a patented technical modality (Concurrent Imaging, version 2.0; Philips) that allows multiple image sets to be created during the same acquisition. This capability makes possible the simultaneous acquisition of both a nongated and a gated SPECT study in the same patient. We took advantage of this opportunity to examine the differences between nongated and gated SPECT perfusion data in AF patients.
MATERIALS AND METHODS
Patient Population and Study Protocol
Our patient population consisted of 44 consecutive patients with chronic AF who were referred to our institution to undergo myocardial perfusion gated SPECT on the basis of the standard clinical indications. Gated SPECT images were acquired using a 2-d protocol. The same dose (740 MBq) of the myocardial perfusion tracer, 99mTc-sestamibi, was injected at rest and at peak exercise or during pharmacologic stress, and image collection began 60 min later for resting scans or 30 min later for stress scans.
Gated SPECT
Gated SPECT was performed using a dual-head γ-camera (Skylight; Philips) equipped with high-resolution collimators and using a 15% window centered on the 140-keV photopeak of 99mTc. SPECT images were acquired in step-and-shoot mode using a 180° elliptic orbit, a 64 × 64 matrix, and 32 projections at 60 s per projection. The Concurrent Imaging software was used to create 2 separate SPECT studies, one without ECG gating and the other with ECG gating. The software creates the 2 studies separately and not as a rearrangement of an original list-mode acquisition. The basic principle of the software is to create multiple image sets starting from a single acquisition. In the instance of a SPECT study, acquisition parameters that cannot be modified are the number of projections, the rotation arc, the relative angle, the orbit type, and the patient orientation. Other variables, such as (in this study) the presence or absence of gating, can be customized by the user, provided that the gantry motions and positions remain unchanged. We chose for gated SPECT an 8-frame acquisition without arrhythmia rejection, because this is the most widely used technical modality (3,8). SPECT images were reconstructed using filtered backprojection and realigned along the heart axis. In accord with our standard protocol—and because most γ-cameras do not allow for attenuation correction—no attenuation correction was performed (9).
Data Analysis
The gated SPECT studies were processed automatically using the quantitative gated SPECT algorithm (Cedars Sinai Medical Center) (10). The influence of arrhythmia on the gated data was visually analyzed, taking into account the number of frames with an evident drop in counts and the shape of the reconstructed left ventricular volume curve, according to the established criteria for quality control of gated studies (3,11). Gated SPECT findings were defined as normal when diastole was correctly positioned in the cardiac cycle, there were no frames with reduced counts, and the curve morphology did not appear to be affected by AF. Gated SPECT findings were defined as abnormal if there was 1 frame with reduced counts but the volume curve showed end-systole to be between frames 2 and 6, and if the end and the beginning of the curve were almost at the same level. Gated SPECT findings were defined as unreliable if 2 or more frames showed a drop in counts or if no reasonable volume curve was obtained. The gated data analysis was performed by an experienced observer who was unaware of the patient's data and was not involved in analysis of the perfusion images.
Perfusion defects were visually evaluated by an experienced observer who was unaware of the patient's data and who examined the reoriented left ventricular slices without knowing whether they were derived from the summed gated SPECT frames or directly from a nongated acquisition. The left ventricle was divided into 20 segments, and tracer uptake was classified using a 5-point scoring scheme (0 = normal uptake, 1 = mildly reduced uptake, 2 = moderately reduced uptake, 3 = severely reduced uptake, 4 = absence of uptake) (12). The summed resting score (SRS) and the summed stress score (SSS) were obtained by adding the scores of the 20 segments in the resting and stress images, respectively. The summed difference score (SDS) represents the difference between the stress and resting scores (12). An SSS of 4 or more was considered abnormal, and abnormality was classified as mild (4–7), moderate (8–13), or severe (>13) (13). An SDS of 2 or more was considered to indicate ischemia. Inducible ischemia was classified as mild (2–5), moderate (6–7), or severe (>7) (13).
Statistical Analysis
Variables are expressed as mean ± SD and were compared using the 2-tailed Student t test for paired data. Agreement between nongated and gated SPECT in classifying perfusion defects was analyzed by the Spearman ρ and the κ statistic (14). A P value of less than 0.05 was considered statistically significant.
RESULTS
General Findings
The patients (31 men and 13 women; mean age ± SD, 74 ± 9 y) had been referred for myocardial perfusion SPECT for the following indications: diagnosis of coronary artery disease (27 patients), reassessment of known coronary artery disease (4 patients), follow-up after revascularization (5 patients), or preoperative evaluation before major noncardiac surgery (8 patients). The stress test was exercise stress testing in 12 patients and pharmacologic stress with dipyridamole in 32 patients.
Analysis of Gated SPECT
The mean heart rate was 100 ± 24 bpm at the moment of the resting acquisition and 99 ± 28 bpm during the poststress acquisition (difference is not statistically significant). According to visual analysis of the gated data and the left ventricular volume curves, of a total of 88 (44 resting and 44 stress) gated SPECT studies, the results of only 6 (7%) could be considered apparently normal. The results of 19 (22%) were abnormal but still valuable, and the results of 63 (71%) were unreliable.
Myocardial Perfusion
Segment Analysis.
In the resting study, agreement between nongated and gated data was high for 880 segments, with 847 (96%) having the same score (Spearman ρ = 0.82 [P < 0.00001], κ = 0.733). Slightly worse results were obtained for the stress study, with 790 segments (90%) equally classified (Spearman ρ = 0.74 [P < 0.00001], κ = 0.630). Finally, when the segment difference score was examined, there were 787 consistent segments (89%), but Spearman ρ and κ decreased to 0.55 (P < 0.0001) and 0.472, respectively.
Patient Analysis.
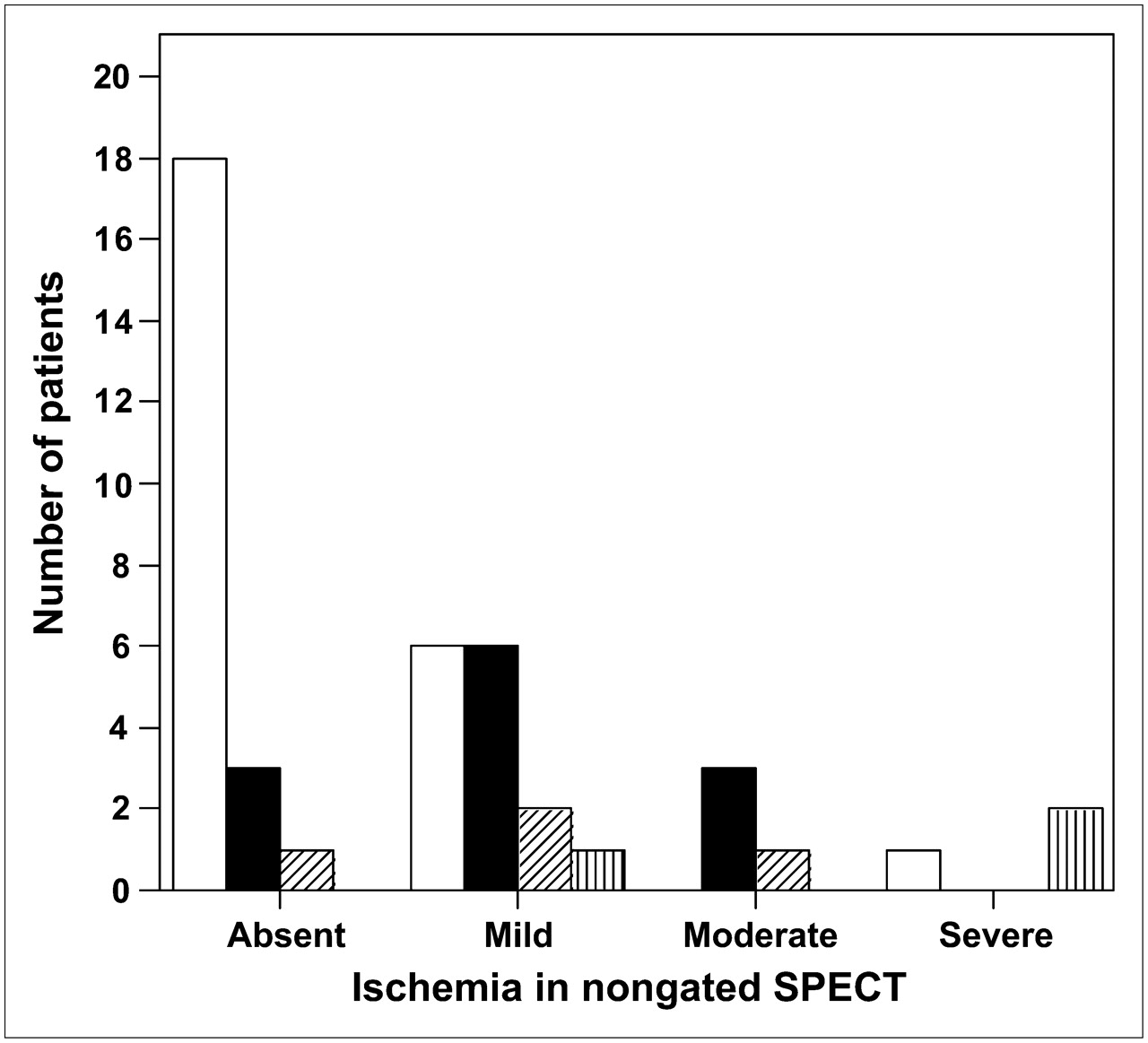
Comparison of the SRS values between gated and nongated SPECT showed good agreement, with a Spearman ρ of 0.911 (P < 0.00001). For SSS, the Spearman ρ was 0.779 (P < 0.00001). Finally, comparison of the SDS values obtained a Spearman ρ of 0.596 (P < 0.0001). Because the patient scores were not symmetric in the 2 evaluations of nongated versus gated studies, computation of the κ statistic was impossible. Therefore, the gated and nongated SSS and SDS values were compared in terms of score severity. As shown in Table 1, 34 patients (77%) were classified in the same SSS category according to both nongated and gated data (Spearman ρ = 0.818 [P < 0.00001], κ = 0.639). However, when the SDS values of the 2 studies were compared, only 27 patients (61%) had the same severity classification (Spearman ρ = 0.549 [P < 0.0001], κ = 0.367) (Table 2; Fig. 1).

Bar graph showing agreement between nongated and gated SPECT in classifying inducible ischemia in AF patients. x-axis shows classification according to nongated SPECT, and bar fill shows classification according to gated SPECT. White bars = absence of ischemia; black bars = mild ischemia; diagonally hatched bars = moderate ischemia; vertically hatched bars = severe ischemia.
Agreement Between Nongated and Gated SPECT for Severity Classification of Stress Perfusion Defects
Agreement Between Nongated and Gated SPECT for Severity Classification of Stress-Induced Ischemia
In 9 patients, coronary angiography data were available for comparison. In 7 of them, coronary angiography had been performed 3–7 mo before perfusion SPECT. Independently of gating, perfusion SPECT detected all defects that had been expected according to coronary angiography. However, the SDS derived from nongated images showed an abnormality in 10 of 10 diseased territories, whereas SDS derived from summed gated images showed an abnormality in an additional territory without stenosis. In another 2 patients, the referring cardiologist decided to have coronary angiography performed for diagnostic purposes after perfusion imaging, and the vessels were found to be normal. The SDS demonstrated ischemia in 3 territories (2 in the same subject) according to summed gated SPECT images but was fully normal according to nongated images.
DISCUSSION
So far, 2 studies by the same group have dealt with the specific issue of arrhythmic artifacts in gated SPECT (4,5). In a first study, Nichols et al. evaluated the prevalence of arrhythmias in patients who underwent myocardial perfusion imaging for standard clinical indications, validated an algorithm for arrhythmia detection, and examined the changes in count increase produced by different arrhythmias (4). AF patients showed the most important differences from subjects in sinus rhythm, both in terms of count loss in the various cinematic frames and in terms of abnormalities in systolic count increase. In another group of patients, the authors simulated various arrhythmias and examined differences between the sinus rhythm and the simulated data. They observed small changes in ejection fraction but significant differences in the extent and severity of abnormalities in perfusion polar maps; these differences were greatest in the case of simulated AF, but the clinical relevance of the arrhythmia-induced perfusion changes was not examined (4). In another study, the same authors simulated gating errors in a slightly larger patient population and analyzed functional parameters using 2 common algorithms for processing gated SPECT data (5). They found that ejection fraction data were relatively stable and that agreement was good for regional ejection fraction and wall motion analysis. A larger difference was observed for wall thickening and perfusion, although for the latter, agreement between visual readings of control versus simulated AF polar maps was excellent, with a κ value of 0.83 on a 3-coronary-artery-territory model on 100 scans (rest–stress in 50 patients). The authors concluded that a nongated SPECT acquisition should be preferred for perfusion analysis, but on the whole these reports suggest that most gated SPECT parameters are quite robust even in the case of major arrhythmias, including AF. What remains unclear is the clinical relevance of the possible gating-related perfusion abnormalities.
In the present study, we specifically addressed this issue by directly comparing perfusion data obtained with and without ECG gating during the same SPECT acquisition. This comparison was possible using dedicated software (Concurrent Imaging) that allows the creation of multiple datasets during a single acquisition. In this particular case, we acquired during the same SPECT orbit both a nongated and an 8-frame gated dataset. Our results confirmed the excellent agreement between nongated perfusion images and summed gated images on a segment basis in both the resting and the stress acquisitions. However, the agreement became clearly lower when the segment difference score was examined. The per-patient analysis confirmed a decrease in agreement from the SRS comparison, which showed the highest value, to the SSS and particularly the SDS comparisons. Even in such a relatively small patient population as ours, the severity classification of the stress perfusion defects and, most important, of the stress-induced ischemia was clearly different when nongated images were compared with summed gated images. Specifically, in 17 of 44 patients, the final SDS classification shifted by one (in 14 patients) or more (in 3 patients) severity categories for summed gated images, compared with nongated images. Although we do not have an external gold standard, there is no reason to consider the nongated SPECT perfusion pattern less reliable than the gated. Therefore, gating-induced abnormalities might significantly influence the image scoring and hence have important potential clinical implications. Certainly, it would be of interest to further improve the analysis by including a gold standard to establish which the true ischemic burden is. However, defining such a reference standard is quite difficult, and coronary angiography would be not completely satisfactory. Indeed, the finding of coronary obstruction would work well to define the accuracy of inducible perfusion defects versus normal perfusion but would be inadequate to establish the true extent of the expected perfusion defect (15). However, in the only 2 patients from our cohort who underwent coronary angiography after myocardial perfusion SPECT, the finding of normal coronary arteries corroborated the normal pattern found on nongated images and contradicted the perfusion defects observed using summed gated SPECT. This observation confirms that the main potential hazard of summed gated images is to show an apparent worsening in the perfusion pattern (5).
These results must be evaluated in the current setting of clinical diagnostic procedures. Gated SPECT is the state of the art in radionuclide perfusion imaging and offers major advantages in accuracy over nongated scans (16,17). The availability of gated images is helpful for identifying attenuation artifacts and represents an alternative to attenuation correction (18). A large body of evidence demonstrates that functional parameters derived from gated SPECT have incremental diagnostic and prognostic value over the standard perfusion assessment (19–23). On the one hand, the availability of gated SPECT has the potential to expand the traditional indications for myocardial perfusion imaging (24). On the other hand, accurate definition of myocardial perfusion remains the main asset of radionuclide methods and is the chief reason for their wide use. Therefore, although the accessibility of functional parameters through gated SPECT is highly desirable, we must still be attentive to the possibility that gating impairs assessment of the real perfusion pattern. Our results strongly support the current recommendation that gating be avoided in patients with severe arrhythmias, particularly AF patients (2,3). In these patients, a nongated study is necessary for reliable perfusion assessment. AF patients would thus be excluded from the potential advantages offered by examining functional parameters derived from gated SPECT. As far as the diagnostic accuracy of perfusion scans is concerned, the use of attenuation correction would be desirable to avoid the artifacts currently excluded using gated images. An additional gated SPECT acquisition should be considered but could prove impractical in a busy laboratory. Naturally, a technical modality such as the one we used, which allows the simultaneous acquisition of both gated and nongated SPECT, would represent an ideal solution.
CONCLUSION
In AF patients, the direct comparison of nongated and summed gated SPECT images demonstrates minor differences in perfusion scoring that, in a remarkable percentage of patients, lead to a clinically significant divergence in the severity classification of inducible ischemia. Therefore, a nongated SPECT acquisition is mandatory to reliably assess myocardial perfusion in AF patients.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 14, 2008.
- Accepted for publication April 14, 2008.





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.