


Abstract
Fever of unknown origin (FUO) is a challenging diagnostic problem. Timely identification and precise localization of the causing process are critical for appropriate patient management. The present prospective study evaluates the role of PET/CT using 18F-FDG in the investigation of FUO. Methods: A total of 48 consecutive patients (25 men, 23 women; age range, 24–82 y) with FUO underwent 18F-FDG PET/CT scans. FUO was defined as a fever of more than 38.3°C that lasted for more than 3 wk and failure to reach diagnosis after more than 1 wk of inpatient investigation. The performance of PET/CT for identifying the etiology of FUO was assessed. Final diagnosis was based on histopathology, microbiologic assays, or clinical and imaging follow-up. Results: PET/CT detected suggestive foci of increased 18F-FDG uptake in 27 patients. In 22 of these 27 positive studies (81%), PET/CT identified the underlying disease and diagnosed infection in 9 patients, an inflammatory process in 10 patients, and malignancy in 3 patients. 18F-FDG PET/CT was negative in 21 patients. All these patients were diagnosed as having systemic nonfocal infection or drug-induced fever or showed spontaneous resolution of the febrile state with no further evidence of a localized inflammatory, infectious, or malignant process for a clinical follow-up period of 12–36 mo. Conclusion: 18F-FDG PET/CT identified the underlying cause of the fever in 46% of the present study population and contributed to the diagnosis or exclusion of a focal pathologic etiology of the febrile state in 90% of patients. 18F-FDG PET/CT has a high negative predictive value (100%) for assessment of FUO. If confirmed by further studies, 18F-FDG PET/CT may be used in the future as an initial noninvasive diagnostic modality for assessment of this group of patients.
Defining the etiology of fever of unknown origin (FUO) is a clinical challenge, despite recent advances in diagnostic techniques (1–4). Infection accounts for about one third of cases of FUO, followed by noninfectious inflammatory processes and neoplasms. In an additional one third of this group of patients, a final diagnosis cannot be established (4–8). Early identification and precise localization of the cause for FUO are important for guiding further invasive diagnostic procedures and subsequently for prompt initiation of appropriate treatment, with a significant impact on patient care (5,7). Conventional anatomic imaging modalities such as ultrasound, CT, and MRI are used, as a rule, as the primary diagnostic modality for investigation of FUO but have a limited sensitivity and specificity, mainly during the early stages of disease (9).
Nuclear medicine techniques such as skeletal, 67Ga, or labeled leukocyte scintigraphy are indicators of the functional and metabolic status of pathologic processes and have been previously used in the differential diagnosis of FUO. However, each of these tests covers only part of the spectrum of possible diagnoses, and, in addition, some are time-consuming and labor-intensive techniques (10). PET using 18F-FDG is a well-accepted clinical tool for routine assessment of a wide range of malignancies. 18F-FDG is an indicator of increased intracellular glucose metabolism and therefore taken up not only by malignant cells but also by those involved in infectious and inflammatory processes (10,11). Initial studies have reported a high sensitivity of stand-alone 18F-FDG PET and PET/CT for diagnosis of infection and inflammation (10–13). PET/CT has the potential to further improve diagnosis and correct localization of disease processes, including infection and inflammation. The purpose of the present study was to prospectively assess the role of PET/CT using 18F-FDG in the investigation of FUO.
MATERIALS AND METHODS
Patient Population
A total of 53 consecutive patients admitted to the hospital for the investigation of FUO were referred by the Departments of Internal Medicine and Rheumatology, prospectively enrolled in this study, and underwent 18F-FDG PET/CT. FUO was defined as fever of over 38.3°C lasting for more than 3 wk and failure to reach diagnosis despite at least 1 wk of inpatient investigation. Clinical assessment included medical history, physical examination, and routine laboratory tests (erythrocyte sedimentation rate, C-reactive protein, hemoglobin, platelet and leukocyte count, blood chemistry, urinalysis, blood and urine cultures, chest radiography, and abdominal ultrasound or CT). Patients with active malignancy or a history of recent surgical procedures were not enrolled. All patients had the classic-type FUO. None of the patients was immunocompromised or had HIV infection. All patients were admitted for evaluation of FUO, and thus in none of the patients had the fever developed during hospitalization. The study included 27 men and 26 women, with a mean age of 57 y (range, 24–88 y). Five patients died shortly (average, 10 d; range, 3–18 d) after undergoing the PET/CT study, without receiving a final diagnosis, and were therefore excluded from further analysis. Forty-eight patients were eligible for inclusion and represent the final study population. The Institutional Review Board approved the study, and each patient signed a written informed consent form. Five of the 48 patients in this study population were diabetic. One of these patients had high glucose levels (272 mg/dL), and the other 4 patients with diabetes and the 43 patients without diabetes had glucose levels below 180 mg/dL (range, 50–179 mg/dL).
PET/CT Acquisition and Processing
Patients were instructed to fast, except for glucose-free oral hydration, for 4–6 h before the injection of 296–444 MBq (8–12 mCi) of 18F-FDG. The patients were instructed to keep their regular drug schedule. Blood glucose levels were measured before injection; none of the patients was withdrawn from the study because of high blood glucose levels, and no additional glucose-control drugs were used. Oral contrast was administered to the patients during the uptake time; no intravenous contrast material was administered for the CT scan. All patients underwent head to mid-thigh scans, and lower-limb scanning was added when clinically indicated. PET and CT images were acquired consecutively 90 min after the injection of 18F-FDG, using a PET/CT system (Discovery LS; GE Healthcare) combining a third-generation multislice spiral CT scanner with a dedicated full-ring PET scanner with bismuth germanate crystals. The PET and CT devices are mechanically aligned back to back and share a common table. Proper registration of the 2 images is ensured by shared positional information of the table and patient for both the CT and the PET image acquisitions. CT data were used for low-noise attenuation correction of PET emission data and for fusion with attenuation-corrected PET images. PET images were reconstructed iteratively using ordered-subset expectation maximization software. PET, CT, and fused PET/CT images were available for review and were displayed in axial, coronal, and sagittal planes. The PET data were displayed as noncorrected and attenuation-corrected images and also in a rotating maximum-intensity projection.
Interpretation and Analysis of PET/CT Images
All studies were reviewed prospectively by a combined team, including a nuclear medicine physician and radiologist, who had knowledge of the patient's clinical history and results of previous imaging studies. Foci of increased 18F-FDG uptake were recorded. Studies showing at least one area of increased 18F-FDG uptake with intensity higher than that of surrounding tissues, localized by hybrid images to an area that did not correspond to the physiologic biodistribution of the radiotracer, were defined as positive. Studies showing 18F-FDG activity only in areas of the physiologic tracer biodistribution or no sites of increased uptake were considered negative.
18F-FDG PET/CT studies were evaluated for their clinical contribution. A PET/CT study showing normal findings was considered as contributory in excluding focal disease and defined as true-negative (TN) when no localized disease process, including infection, inflammation, or malignancy, was further diagnosed; the patient was discharged from the hospital with no fever; and there was no evidence of disease for a clinical follow-up for at least 12 mo. A study with no suggestive foci was defined as false-negative when a focal disease process was found within a 4-wk interval from the PET/CT study. A PET/CT study demonstrating a focal, precisely localized disease process further confirmed as representing the cause of FUO was considered as contributory for diagnosis and defined as true-positive (TP). Abnormal findings in a patient with no final diagnosis of a focal disease process or with pathology identified in a location different from the site demonstrated on PET/CT was defined as noncontributory and false-positive (FP).
Of the 5 diabetic patients, 3 were TP and 2 were TN. One of TP patients had high glucose levels (272 mg/dL). The other 4 patients with diabetes with glucose levels below 180 mg/dL included 2 TP and 2 TN studies.
Final diagnosis was based on histopathology in 9 patients, on microbiologic or serologic assays in 10 patients, on clinical diagnostic criteria defined by the treating physician in 8 patients, and on a clinical and imaging follow-up period of at least 12 mo in 21 patients. Final diagnosis was determined by the treating physician and confirmed by one of the investigators. Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were calculated using standard definitions.
RESULTS
Forty-eight patients with FUO were evaluated (25 men, 23 women; age range, 24–82 y). The final diagnosis included a focal infectious process in 9 patients, systemic infection in 5, inflammatory noninfectious processes in 11, malignancy in 3, and drug-induced fever in 1. In 19 patients, the fever resolved spontaneously with no further evidence of any inflammatory, infectious, or malignant process for a clinical follow-up period of 12–36 mo. A total of 27 PET/CT studies (56%) demonstrated foci of increased 18F-FDG uptake, suggesting the presence of a disease process that could represent the cause for FUO. In 22 of these 27 positive studies (81%), PET/CT diagnosed the etiology of FUO and was thus defined as TP, including localized infection in 9 patients, inflammation in 10 patients, and malignancy in 3 patients (Table 1). PET/CT diagnosed and precisely localized an abscess in 7 of 9 patients diagnosed with infection. In 5 patients, the abscess was confirmed at surgery to be localized to the liver, a multicystic kidney, the abdominal wall, the pararectal region, or the ovary (Fig. 1). In 2 patients, a dental abscess and a soft-tissue abscess associated with osteomyelitis of the clavicle were confirmed by microbial assays and additional imaging workup. In 1 additional patient, a diagnosis of ascending cholangitis was confirmed at surgery; in 1 patient on hemodialysis who showed linear increased 18F-FDG uptake along an intravenous catheter, fever resolved after replacement of the infected device and a short course of antibiotic therapy.

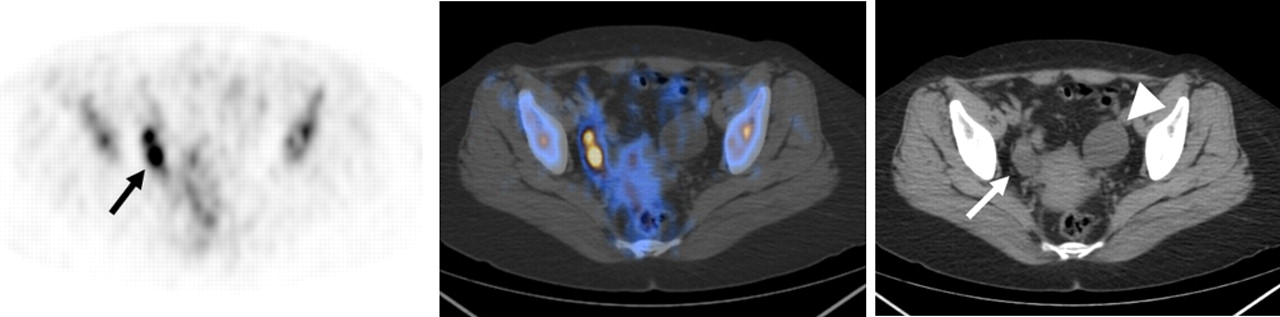
A 41-y-old woman presented with 3 wk of fever. CT demonstrated small amounts of pleural, pericardial, and peritoneal fluids and 2-cm hypodense lesion in left pelvis adjacent to uterus. Transaxial 18F-FDG PET (left) demonstrates focus of increased tracer uptake in right pelvis (arrow) localized by PET/CT image (center) to right ovary on CT (right, arrow), suggesting abscess. Previously reported hypodense lesion in left pelvis and demonstrated on CT component as well (right, arrowhead) is not metabolically active. Diagnosis of right ovarian abscess and left ovarian cyst was confirmed at surgery.
Clinical and Imaging Findings in 22 Patients with FUO and Positive Contributory PET/CT Studies
Ten patients had a final diagnosis of inflammatory noninfectious processes. In 3 of 10 patients, intense linear 18F-FDG uptake localized by PET/CT to the large abdominal (n = 1) or thoracic and abdominal vessels (n = 2) contributed to the diagnosis of arteritis, which was confirmed by biopsy in 2 patients and CT angiography in 1 patient (Fig. 2). Immediate institution of corticosteroid treatment led to complete resolution of the symptoms and imaging findings. In 3 additional patients, abnormal 18F-FDG uptake was localized by PET/CT to the pericardium, with the diagnosis of pericarditis further confirmed by electro- and echocardiography and clinical response to nonsteroidal antiinflammatory drugs. Two of the 10 patients showed mediastinal, hilar, and abdominal 18F-FDG–avid lymphadenopathy and diffuse spleen and bone marrow uptake; the final diagnosis, based on symptoms and laboratory tests, was sarcoidlike disease, which responded to corticosteroid therapy, with lymphoproliferative disorder excluded by bone marrow aspiration. One patient showing mediastinal, hilar, and abdominal 18F-FDG–avid lymphadenopathy had histologically proven sarcoidosis. One additional patient showed focal increased 18F-FDG uptake in axillary and mediastinal lymph nodes; common disease processes were excluded after thorough investigation, and the presence of lymphadenopathy was used as one of the diagnostic criteria (based on Cush et al. (14)) for Still disease.

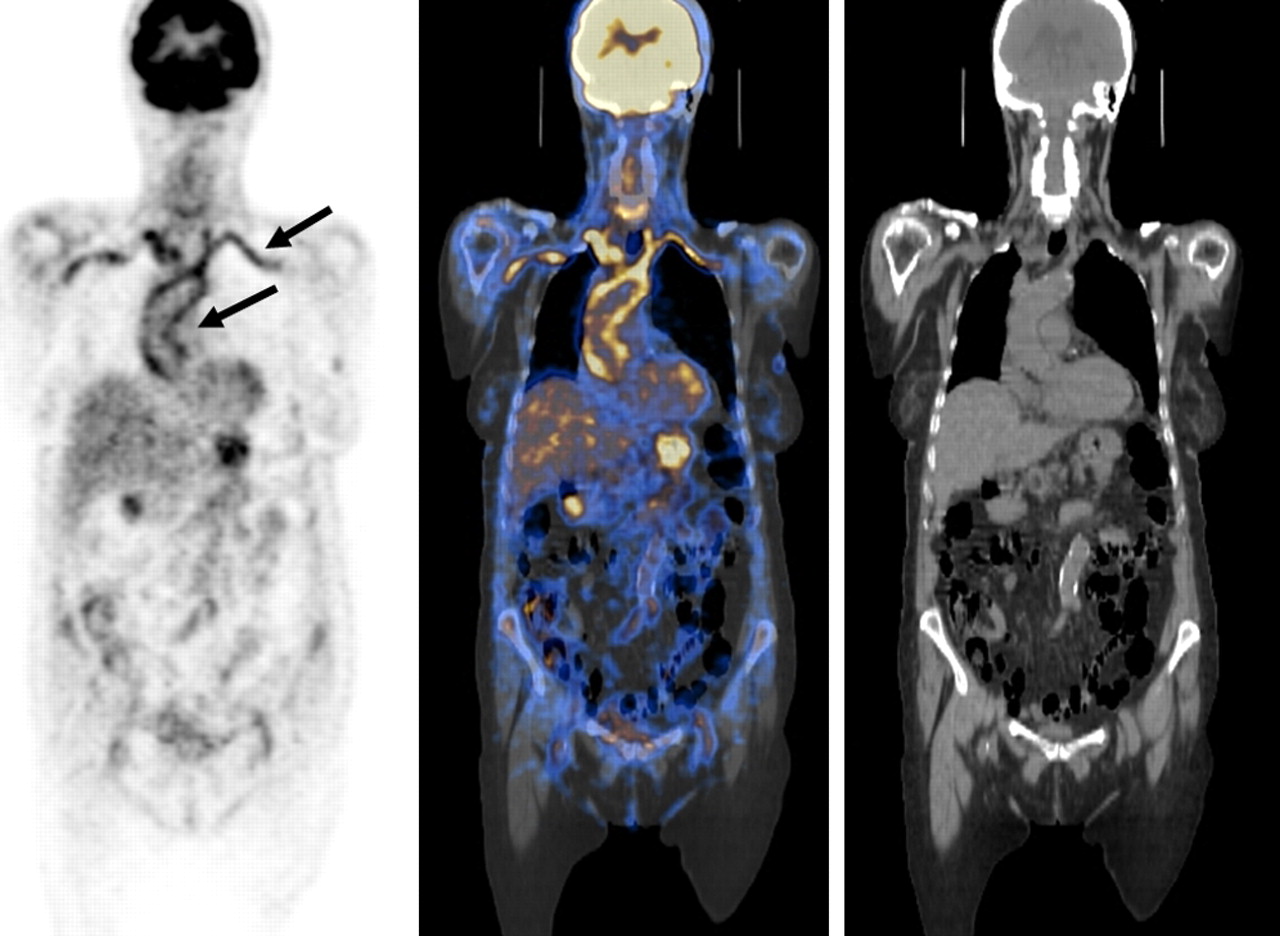
A 78-y-old woman presented with 6 wk of fever, night sweats, and weight loss. Coronal 18F-FDG PET (left), PET/CT (center), and CT (right) slices demonstrate intense linear 18F-FDG uptake along walls of thoracic aorta and brachiocephalic and subclavian arteries (arrows) consistent with arteritis. Giant-cell arteritis was diagnosed on temporal artery biopsy.
Non-Hodgkin lymphoma was diagnosed by biopsy in 2 patients after PET/CT detection of hypermetabolic 18F-FDG–avid lesions in the adrenal glands in 1 patient (Fig. 3) and in a cervical lymph node in the other. In 1 patient with diffuse 18F-FDG uptake in the skeleton, bone marrow biopsy revealed metastatic adenocarcinoma. PET/CT studies in all 22 patients (46%) were contributory to diagnosis and defined as TP (Table 1).
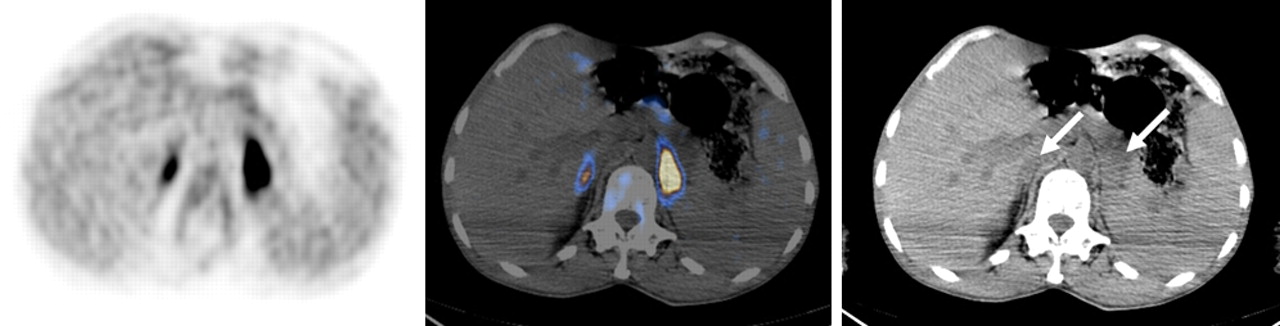
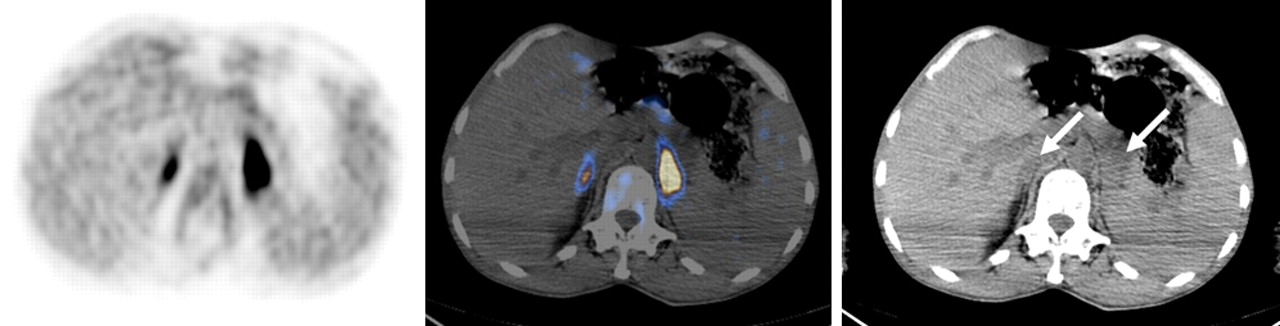
A 64-y-old man presented with 3 wk of fever, weight loss, confusion, and left adrenal enlargement of unclear etiology on CT. Transaxial 18F-FDG PET (left) demonstrates foci of increased tracer uptake in upper abdomen localized by PET/CT (center) to both adrenals, of higher intensity in enlarged left gland seen on CT (right, arrows). Biopsy revealed diffused large-cell non-Hodgkin lymphoma. Repeat PET/CT performed after 2 courses of chemotherapy became normal.
In 5 of the 27 patients, the positive PET/CT studies did not contribute to the final diagnosis and further patient management. Two patients showing inhomogeneous increased 18F-FDG uptake throughout the skeleton had no further evidence for skeletal or bone marrow disease at biopsy. In 1 of these patients, fever resolved spontaneously; the second patient was diagnosed with Still disease and successfully treated with corticosteroid therapy. Two additional patients showed focal 18F-FDG–avid lesions in axillary lymph nodes, and biopsy defined the presence of a nonspecific inflammatory process. Fever resolved spontaneously in both patients. In 1 patient, an 18F-FDG–avid paravertebral soft-tissue mass was diagnosed histologically as a reactive inflammatory process, with complete spontaneous resolution. These 5 positive PET/CT studies were thus considered as noncontributory to the final diagnosis and defined as FP (Table 2).
Final Diagnosis in 5 Patients with FUO and Noncontributory (FP) PET/CT Findings
PET/CT showed no abnormal 18F-FDG uptake in 21 patients. No focal disease process was diagnosed in any of these patients. Two patients had urinary tract infection, 1 had typhoid, 1 had Q fever, 1 had cytomegalovirus infection, and 1 had drug-induced fever. In the other 15 of 21 patients, FUO resolved spontaneously, with no further evidence of any inflammatory, infectious, or malignant process for a clinical follow-up period of 12–36 mo. These patients were defined as TN. None of the patients with negative PET/CT had a final diagnosis of focal infection, inflammation, or malignancy, and thus no false-negative studies were recorded.
The performance of PET/CT for the diagnosis of a focal disease process representing the etiology of FUO showed a sensitivity of 100%, specificity of 81%, PPV of 81%, NPV of 100%, and accuracy of 90%.
DISCUSSION
18F-FDG PET/CT was found to contribute clinically important information for the diagnosis or exclusion of a focal etiology in 90% of cases in this prospective series of 48 patients with FUO. In 81% of positive 18F-FDG PET/CT studies in the present series, hybrid imaging was contributory either by identifying the etiology of FUO or by guiding further management, including invasive therapeutic procedures. 18F-FDG PET/CT was FP in 10% of patients, including 2 with inhomogeneous increased skeletal uptake of 18F-FDG who had no further evidence of a focal pathologic process. Previous studies have hypothesized that increased bone marrow tracer uptake may be a consequence of interleukin-dependent upregulation of glucose transporters rather than the underlying etiology of FUO (15). Various benign and malignant diseases with bone marrow involvement can demonstrate diffuse increased skeletal uptake of 18F-FDG as well; therefore, PET/CT studies showing this pattern were defined as positive in the current study. Three additional FP cases were due to a nonspecific inflammatory process in normal-size axillary lymph nodes (2 patients) or paravertebral soft tissues (1 patient). Increased 18F-FDG activity in nonspecific inflammatory processes involving lymph nodes or soft tissues has been previously described (16,17). Tissue sampling should be performed as the next diagnostic step in patients showing solely nodal foci of increased 18F-FDG activity, in particular when the foci are of normal size and located in sites such as the axilla or inguinal region.
Overall, positive PET/CT studies contributed to final diagnosis in 46% of the present study population. Positive PET/CT studies in patients with FUO have to be correlated with the clinical, biochemical, and immunologic status of the patient, and when deemed clinically necessary they should be confirmed by other imaging or invasive diagnostic modalities.
In 21 negative PET/CT studies, no focal pathologic condition was further diagnosed. In 6 of these patients, a systemic disease with no focal manifestation was the cause for FUO; spontaneous resolution of the fever occurred in the other 15 patients, with no evidence for disease for a clinical and imaging follow-up period of 12–36 mo. These results, supported by a significantly longer follow-up period of 12 mo, as compared with a previously reported period of 3 mo (8), confirm the very high NPV of 18F-FDG imaging for assessment of FUO and indicate that 18F-FDG PET/CT can exclude a focal etiology of FUO with a high degree of certainty, avoid the need for further futile investigations, and thus affect patient care (5,8).
Final diagnosis of the cause of FUO in the current series included focal or systemic infection in 27% of patients, an inflammatory process in 25%, malignancy in 6%, and drug-induced fever in 1 patient. In 40% of patients, no cause was identified, and FUO resolved spontaneously. This array of etiologies and their proportional distribution in the present study are similar to previously reported data (8,18,19).
The use of 18F-FDG imaging as a tool for evaluation of patients with FUO is based on the metabolic properties of this tracer that have the potential to provide early diagnosis, even in the absence of overt morphologic changes, define or confirm the degree of activity in equivocal structural abnormalities, or identify inflammatory processes that are not well localized and are therefore difficult to detect, or are even missed, by conventional imaging modalities (18). Studies using 18F-FDG with stand-alone PET have found, both in inhomogeneous study populations (5,9) and in a prospectively selected group of patients with FUO, that this diagnostic test has an incremental value for further management in more than one third of patients (2,8). In contrast, albeit in a small group of 19 patients with FUO, stand-alone 18F-FDG PET had significantly lower performance indices than did 111In-labeled granulocyte scintigraphy, which was attributed by the authors mainly to the high FP rate among focal sites of abnormal 18F-FDG uptake (20). The present results provide additional evidence to support previous literature reports, including data from both stand-alone PET and PET/CT studies (9,18), suggesting that the additional information provided by the CT component of the hybrid imaging study may play an important role in the assessment of patients with FUO.
CONCLUSION
18F-FDG PET/CT was found to have a good PPV and high NPV in the assessment of patients with FUO. If proven by further studies, this noninvasive single imaging modality may in the future be used as one of the initial diagnostic investigations in patients with FUO.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 27, 2008.
- Accepted for publication September 2, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The diagnostic value of 18F-FDG PET/CT in identifying the causes of fever of unknown origin
- The value of 18F-FDG-PET/CT in identifying the cause of fever of unknown origin (FUO) and inflammation of unknown origin (IUO): data from a prospective study
- Does Antibiotic Treatment Affect the Diagnostic Accuracy of 18F-FDG PET/CT Studies in Patients with Suspected Infectious Processes?
- EANM/SNMMI Guideline for 18F-FDG Use in Inflammation and Infection
- Positron-Emission Computed Tomography in Cyst Infection Diagnosis in Patients with Autosomal Dominant Polycystic Kidney Disease
- Investigating and managing pyrexia of unknown origin in adults
- Do Hyperglycemia and Diabetes Affect the Incidence of False-Negative 18F-FDG PET/CT Studies in Patients Evaluated for Infection or Inflammation and Cancer? A Comparative Analysis