


Abstract
Although 18F-FDG PET has been used to monitor patients with lymphoma, its usefulness has not been determined in patients with extranodal natural killer/T-cell lymphoma (ENKTL). Therefore, we evaluated whether pretreatment 18F-FDG uptake was a predictor of survival in patients with ENKTL of the head and neck. Methods: Pretreatment staging work-ups, including whole-body 18F-FDG PET, were performed on 21 patients with previously untreated head and neck ENKTL. Fourteen patients received combined chemoradiotherapy (n = 14), and 7 received chemotherapy or radiotherapy alone. We assessed the relationship of maximum standardized uptake value (SUVmax) of the tumor to disease-specific survival (DSS) and to clinical parameters, including sex, age, Ann Arbor stage, performance status, International Prognostic Index score, presence of B symptoms, lactate dehydrogenase level, local tumor invasion (LTI), and lymph node involvement. Results: Mean tumor SUVmax was 5.5 and was significantly higher in patients with elevated lactate dehydrogenase level, LTI, or poor response to initial therapy (P < 0.05). All 5 nonresponders to therapy had an SUVmax greater than 5.5, whereas 11 of 16 responders (69%) had an SUVmax less than or equal to 5.5 (mean SUVmax, 8.4 vs. 4.5). Univariate analysis showed that an International Prognostic Index score greater than or equal to 2, LTI, and SUVmax category were significant predictors of 3-y DSS, although only the SUVmax category remained an independent determinant of DSS on multivariate analysis (P = 0.023). Conclusion: High tumor 18F-FDG uptake was closely associated with local tumor invasion, contributing to unfavorable treatment and survival outcomes in patients with ENKTL of the head and neck.
- extranodal natural killer/T-cell lymphoma
- head and neck
- 18F-FDG PET
- predictive factor
- standardized uptake value
Extranodal natural killer/T-cell lymphoma (ENKTL) is a distinct clinicopathologic entity within the World Health Organization (WHO) classification of lymphoid tumors (1). These tumors usually present within the nasal cavity and are strongly associated with Epstein-Barr virus (EBV) and angioinvasion (2–4). Although uncommon in Western countries, ENKTLs are fairly common in East Asia (3–7). For example, in Korea, ENKTLs account for 9% of all malignant lymphomas and 74% of lymphomas arising within the nasal cavity and paranasal sinuses (8). These tumors occur most frequently in middle-aged men, and a large proportion are localized stage I and II disease. Because ENKTLs are refractory to conventional chemotherapy but sensitive to radiotherapy, treatment at most institutions consists of either involved-field radiotherapy or chemotherapy followed by radiotherapy (3–7). Retrospective analyses have found that poor survival was associated with poor performance, an elevated level of lactate dehydrogenase (LDH), the presence of B symptoms, local tumor invasiveness, paranasal extension, regional lymph node involvement, and a high EBV DNA titer (6,7,9–11).
18F-FDG PET has been used increasingly to monitor treatment and follow-up in patients with lymphoma (12–16). Because the intensity of tumor 18F-FDG uptake can distinguish between indolent and aggressive forms of lymphomas (17,18), 18F-FDG PET can be used to identify the subset of patients who might respond to chemoradiation therapy. This may affect the prognostic stratification and clinical management of patients with lymphoma. To date, however, little is known about the relationship between tumor 18F-FDG uptake and survival outcomes in patients with ENKTL. We, therefore, evaluated pretreatment 18F-FDG uptake as a predictor of survival in patients with ENKTL of the head and neck.
MATERIALS AND METHODS
Patients
Patients presenting between 2002 and 2006 with previously untreated ENKTL of the head and neck at our institution were enrolled in this retrospective study. Patients were included if they had a pathologically confirmed diagnosis of ENKTL, according to the WHO classification; the NK/T-cell type as proven by immunohistochemical, flow cytometry, or EBV in situ hybridization analysis; and primary lesions within the nasal cavity, nasopharynx, or other head and neck regions and secondary spread to other organs. To be included, patients also had to have undergone whole-body 18F-FDG PET before initial treatment. Patients with other types of NK or T-cell lymphomas or primary lesions outside the head and neck or those who were not assessed by pretreatment 18F-FDG PET were excluded. All patients underwent pretreatment staging work-ups, including panendoscopy of the upper aerodigestive tract, chest radiography, CT/MRI of the head and neck, CT of the abdomen and pelvis, bone marrow examination, and whole-body 18F-FDG PET. Our Institutional Review Board waived informed consent and approved the design of this study.
Imaging
PET was performed using an ECAT HR+ scanner (Siemens/CTI), which provided an in-plane spatial resolution of 4.5 mm and an axial field of view of 15.5 cm. Patients fasted for at least 6 h before 18F-FDG PET, and their blood glucose concentrations were measured; patients with diabetes mellitus were required to have blood glucose concentrations of less than 11.0 mmol/L before the scan. All patients had rested for at least 1 h before the PET scan. Approximately 60 min after intravenous injection of 18F-FDG (∼555 MBq), whole-body imaging was performed with the patient supine. Data were reconstructed into coronal, sagittal, and transverse sections and a 3-dimensional rotating projection.
The degree of suspected malignant involvement was based on qualitative visual interpretation of the images and the determination of standardized uptake value (SUV), a semiquantitative measurement of relative 18F-FDG uptake within the regions of interest (ROIs). Maximum SUV (SUVmax) was calculated as follows: SUV = A/(ID/LBW), where A is the decay-corrected activity in tissue (in MBq/mL), ID is the injected dose of 18F-FDG (in MBq), and LBW is the patient's lean body weight. PET images were reviewed to calculate the SUV, and the slice containing the tumor was selected. For the calculation of SUV, ROIs of variable sizes were drawn on consecutive transaxial slices around the primary lesions of the head and neck with increased 18F-FDG uptake and corresponding to lesions detected on contemporaneous (≤2 wk) CT/MRI scans. SUV was calculated using the single maximum pixel count within the defined ROIs. Because the size of primary tumors was greater than or equal to 1.5 cm in the longest diameter, all primary lesions could be defined on both PET and CT/MRI scans.
Local Invasiveness and Histology of Tumor
Local tumor invasiveness (LTI) was defined as bony invasion or perforation or invasion of the skin (7). Briefly, the involved bony structure included the paranasal sinuses, orbit, skull base, palate, nasal bone, and septum. The extent of bony involvement, bone thinning, disorganized structure, or defects caused by a tumor was assessed on each CT scan. Infiltration of the skin surrounding the tumor was regarded as skin invasion.
All pathologic specimens were classified on the basis of strict morphologic criteria and immunophenotypic analyses, in accordance with the WHO criteria for pathologic diagnosis (1). Samples were immunophenotyped using monoclonal antibodies against CD3 (Dakopatts), CD 20 (Dakopatts), and CD 56 (Monosan). EBV RNA in situ hybridization was performed using a detection kit (Dakopatts).
Treatment
Fourteen patients received 3–6 cycles of chemotherapy plus involved-field radiotherapy, 4 received chemotherapy alone, and 3 received radiotherapy alone (Table 1). The selection of treatment modality was at the physician's discretion. Chemotherapy included the following regimens: cyclophosphamide, doxorubicin, vincristine, and prednisolone; cyclophosphamide, doxorubicin, vincristine, prednisolone, bleomycin, and procarbazine; ifosfamide, methotrexate, and etoposide; etoposide, methylprednisolone, cisplatin, and cytarabine; and dexamethasone, cytarabine, and cisplatin. The total radiation dose ranged from 28.0 to 59.5 Gy (mean dose, 45.6 Gy; ≥40 Gy in all patients, except for 1 who died early of progressive disease). Treatment response was assessed according to standard response criteria (19). Briefly, complete remission was defined as complete disappearance of all detectable clinical and radiologic evidence of disease; partial remission was defined as greater than or equal to a 50% decrease in the sum of the products of the greatest diameters (SPD); stable disease was defined as less than a partial remission but not progressive disease; and progressive disease was defined as greater than or equal to a 50% increase from the nadir in the SPD of previous lesions or the appearance of any new lesions during or at the end of therapy. The major endpoints of our study included disease-specific survival (DSS) and overall survival.
Demographic and Clinical Characteristics of Study Population (n = 21)
Statistical Analysis
A Fisher exact or a Mann–Whitney test was used to compare SUV category and other clinical variables (sex, age, B symptoms, Eastern Cooperative Oncology Group performance status, International Prognostic Index [IPI] score (20), LDH level, LTI, lymph node involvement, Ann Arbor stage, and response to initial therapy). Actuarial DSS and overall survival rates were calculated by the Kaplan–Meier method. Persistent or recurrent tumor was documented by CT/MRI or 18F-FDG PET. The log-rank test was used to assess the correlation of these endpoints with SUV and with the aforementioned clinical variables. Variables shown to be significant in univariate analysis were selected for multivariate analysis using the Cox proportional hazards model. A P value of less than 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics of Patients
The cohort consisted of 21 patients (14 men, 7 women), of mean age 46 y (range, 17–78 y) (Table 1). The primary tumor site was the nasal cavity in 16 patients, the oral cavity in 3, the nasopharynx in 1, and the oropharynx in 1. Two patients had tumors that originated in the nasal cavity and extended to the facial space, cranial base, or parotid lymphatics (Fig. 1). Seven patients (33%) showed involvement of cervical lymph nodes, 16 (76%) were in Ann Arbor stage I or II, and 3 (14%) had systemic dissemination. Eight patients each (38%) had B symptoms and IPI scores greater than or equal to 2. An elevated serum LDH level was observed in 13 patients (62%) and LTI in 7 (33%). Of the 21 eligible patients, 18 had the immunophenotype CD56+CD3+CD20−, 2 had CD56−CD3+CD20−, and 1 had CD56+CD3−CD20−. Nineteen patients (90%) were positive for EBV RNA. Sixteen patients (76%) responded to initial therapy (complete remission in 8 patients, partial remission in 8, stable disease in 3, and progressive disease in 2).

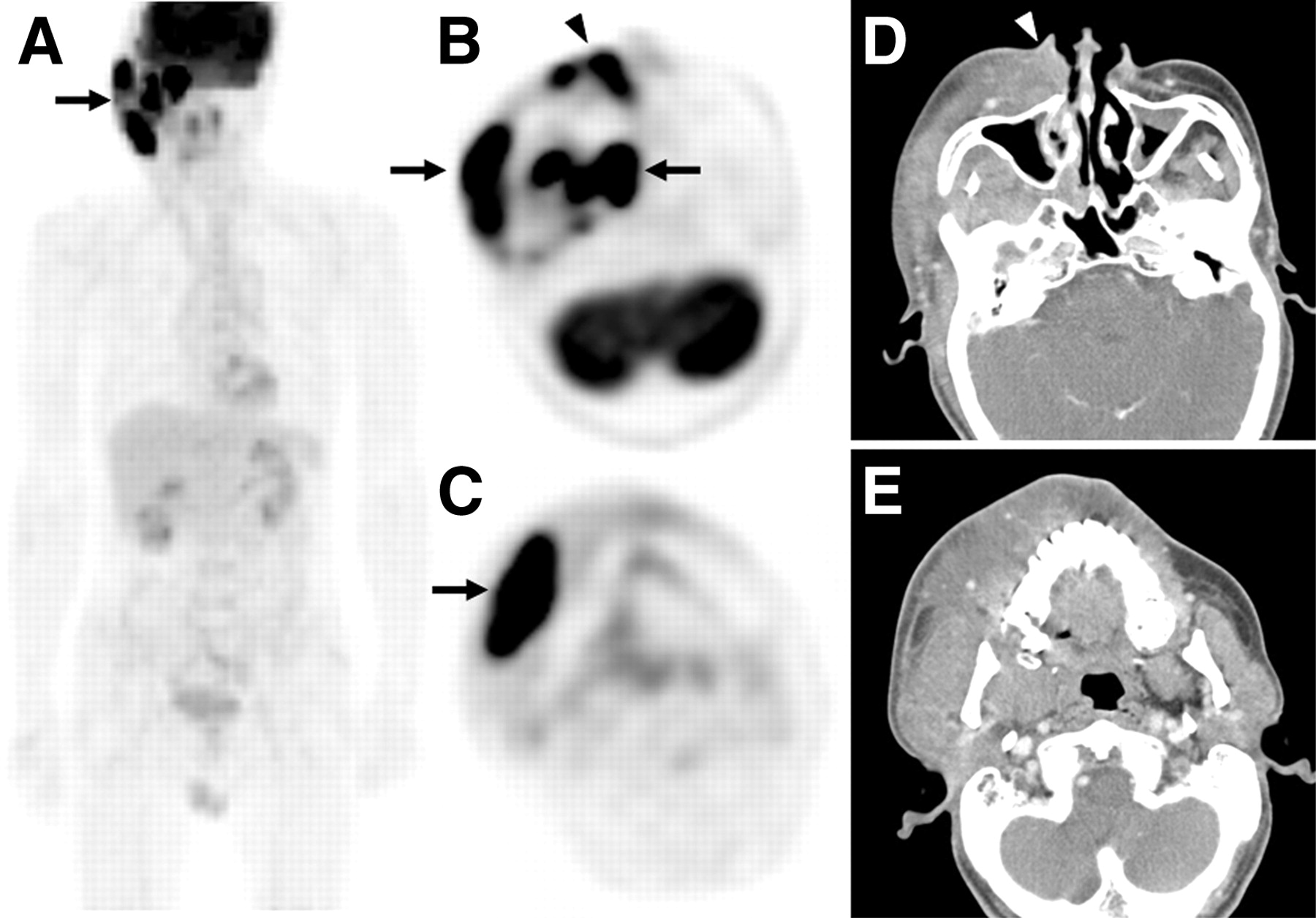
ENKTL with local tumor invasiveness. (A–C) Whole-body 18F-FDG PET showing focal 18F-FDG uptake (SUVmax, 13.0) in right posterior nasal cavity, masticator space, and cheek (arrows) and lateral side to the ala nasi (arrowhead) in 59-y-old male patient. (D and E) Axial CT scans showing ill-defined enhancement of diffuse swollen soft-tissue masses in same areas on right side and tumor involvement of overlying skin (arrowhead). Biopsies of masses in right nasal cavity and cheek revealed results typical of ENKTLs. Although patient had no metastatic disease, he died of disease 6 mo after initial treatment.
Tumor 18F-FDG Uptake
All primary lesions were positive at pretreatment 18F-FDG PET. The median SUVmax of the primary tumors was 5.3 (range, 2.1–13.0). The mean ± SD SUVmax of the primary tumors was 5.5 ± 2.8 (Table 1). In the absence of an established cutoff for SUV, the mean value was used to establish groups of patients with high (>5.5) and low (≤5.5) SUV, close to the mean and median SUVs. Using the cutoff value to compare SUV category and other clinical variables (Table 2), we found that LDH level, LTI, and response to initial therapy were significantly correlated with SUV category (P < 0.05). All 5 nonresponders to initial therapy had an SUV of greater than 5.5. In addition, pretreatment 18F-FDG PET detected lymph node involvement in 7 and spleen, liver, or other systemic involvement in 5 patients, which were confirmed by staging work-ups and aspiration or biopsy.
18F-FDG Uptake of Primary Tumors in Relation to Patient Clinical Parameters
Survival Analysis
At the last follow-up, 12 patients were alive; 9 had died of tumor-related disease. The mean follow-up for surviving patients was 34 ± 12 mo (range, 18–52 mo). Seven patients presented with persistent or recurrent locoregional diseases, and 3 presented with new systemic metastases. Eleven patients had no locoregional or distant failure. At 3 y, the DSS rate was 57.3%.
The mean ± SD SUVmax was significantly higher in the 9 patients who presented with local, regional, or distant failure than in the 11 remaining patients (7.0 ± 3.0 vs. 4.0 ± 1.7; P = 0.010). Univariate analysis survival showed that IPI score, LDH level, LTI, and SUV category of the primary tumor were significant predictors of DSS (P < 0.05; Table 3, Fig. 2). Multivariate analysis showed that only the SUV category of the primary tumor remained a statistically significant predictor of DSS (P = 0.023), whereas LTI was of borderline significance (P = 0.059) (Table 4, Fig. 3).
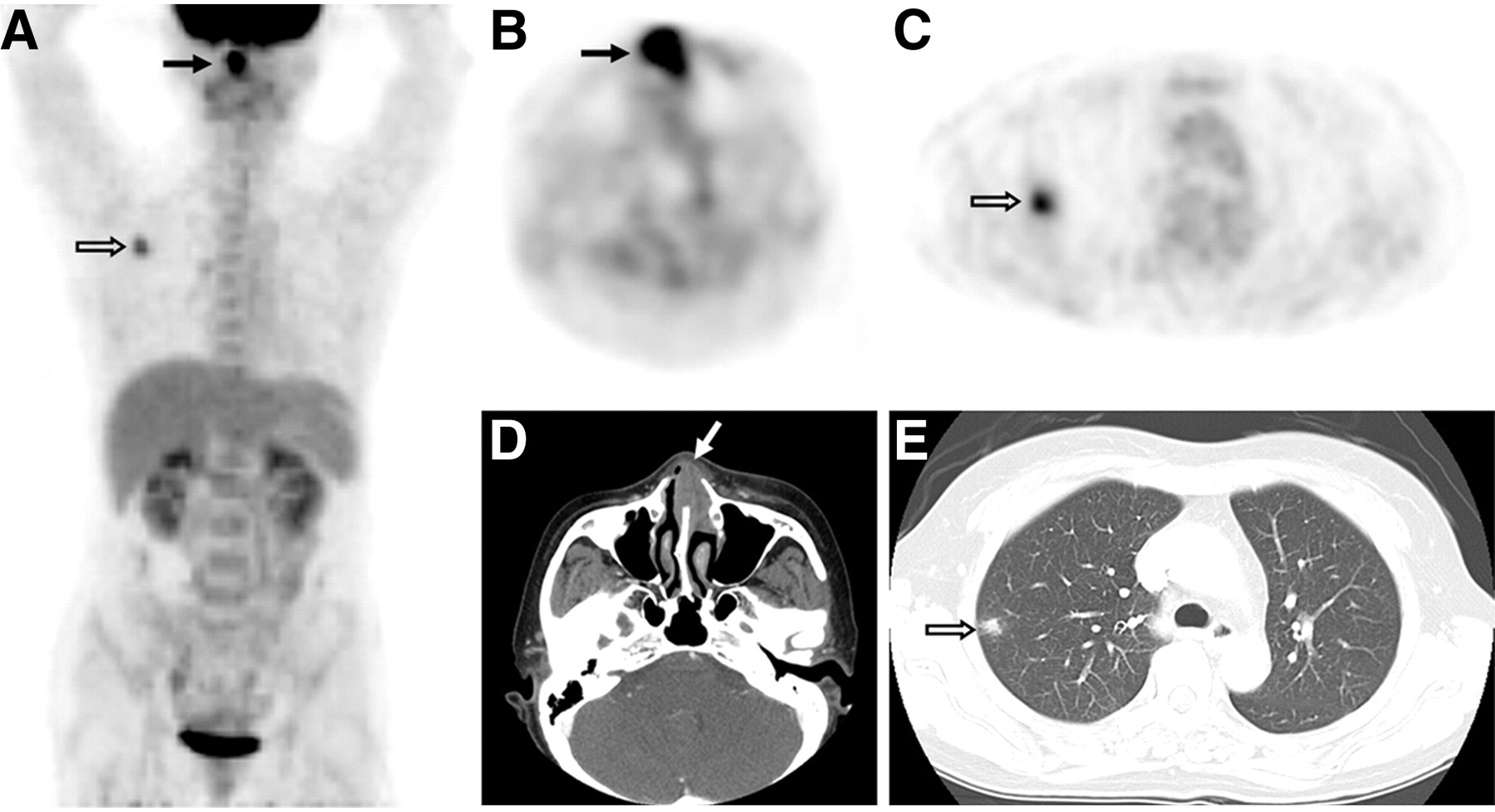
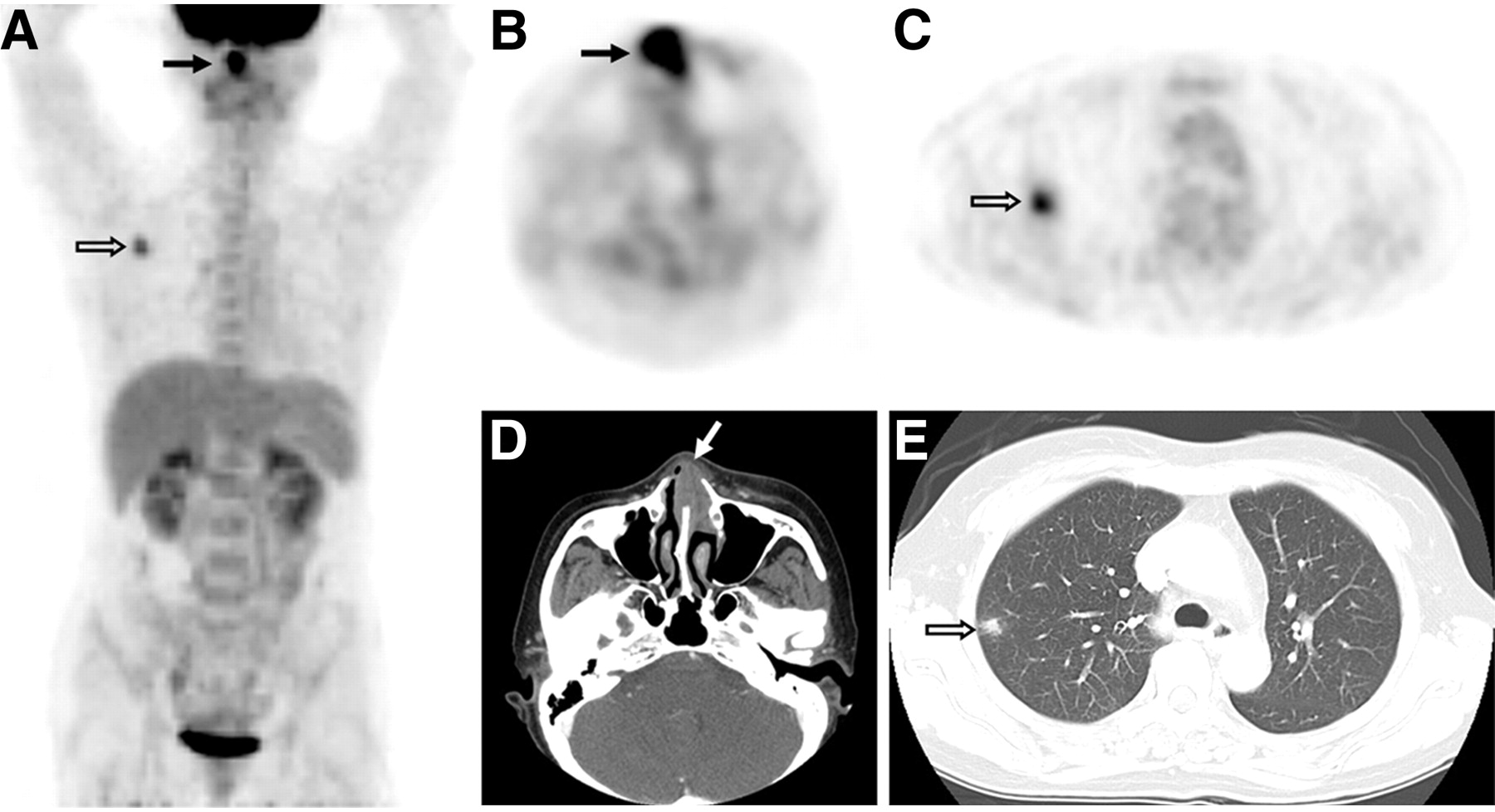
Images demonstrating tumor 18F-FDG PET uptake, local tumor invasiveness, and survival outcome. (A–C) Whole-body 18F-FDG PET showing focal 18F-FDG uptake in left anterior nasal cavity (solid arrows; maximum SUV, 6.6) and right upper lung (open arrows). (D) Axial CT scan showing mass (arrow) with destruction of nasal septum in left anterior nasal cavity. (E) Axial chest CT scan showing nodular mass with irregular margin in right upper lung. Biopsies revealed that nasal cavity lesion was ENKTL, but lung lesion did not contain tumor cells. Although patient was in Ann Arbor stage IE, he died of disease 10 mo after initial chemotherapy.

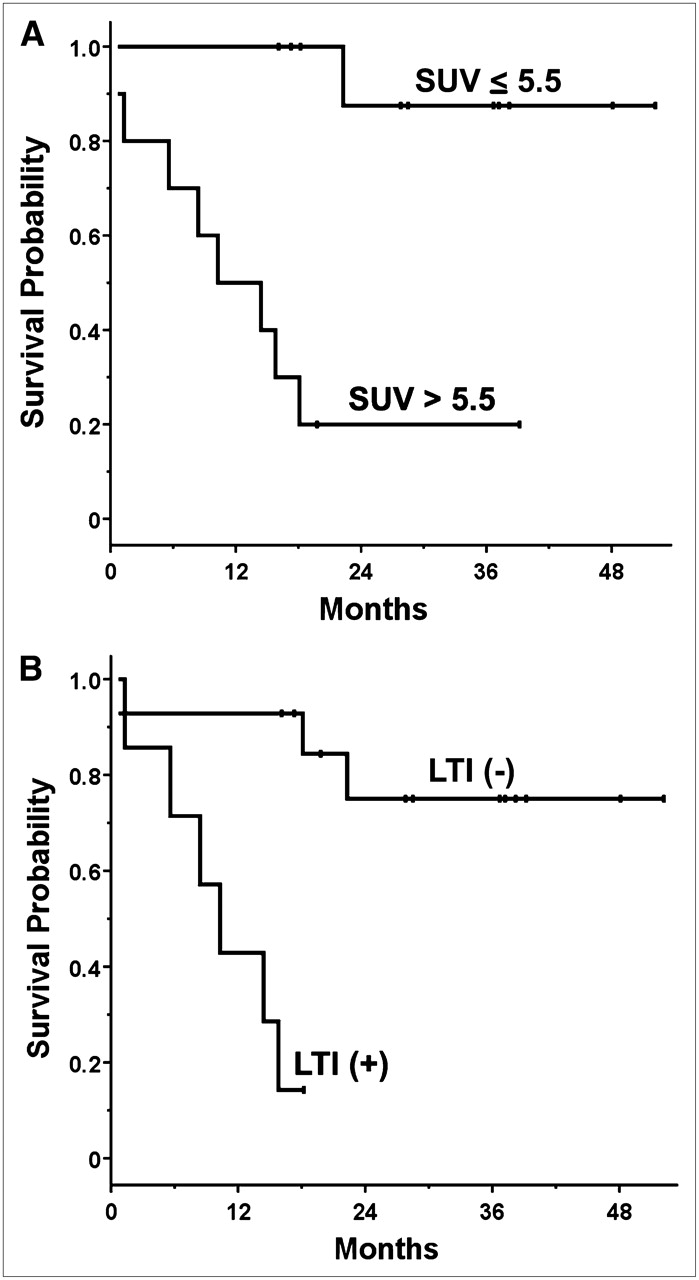
Prognostic factors for DSS. SUV category (A) was only independent determinant of patient DSS in multivariate analysis (P = 0.023); LTI (B) was of borderline significance (P = 0.059).
Univariate Analysis of Factors Predictive of DSS
Multivariate Analysis of Factors Predictive of DSS
DISCUSSION
Pretreatment 18F-FDG PET can predict treatment response and survival outcomes in patients with ENKTL of the head and neck. 18F-FDG uptake by primary tumors was higher in nonresponders to therapy and patients with poor survival outcomes. This finding is consistent with results in patients with non-Hodgkin's lymphoma, in whom the intensity of 18F-FDG uptake on PET images correlated with tumor aggressiveness (17,18). Conversely, the likelihood for aggressive diseases increased in parallel with increased SUV (17,18). Tumor 18F-FDG uptake may also have prognostic significance in other malignancies, in that patients with high 18F-FDG uptake had a less favorable outcome (21–25).
Prior reports have suggested that Ann Arbor staging, age, performance status, LDH level, IPI, paranasal extension, and LTI predicted the survival of patients with ENKTL arising in the upper aerodigestive tract (6,7,9,26). LTI, defined as bony invasion or perforation or invasion of the skin, was reported to be the most significant factor predicting a low probability of complete response and reduced survival in patients with ENKTL (7). In addition, paranasal local extension was significantly associated with poorer treatment outcome, suggesting a need to improve systemic treatment (11,27). Our multivariate analysis showed that the SUV category of the primary tumor was an independent predictor of DSS (P = 0.023), with LTI being of borderline significance (P = 0.059). LTI was also significantly associated with high tumor 18F-FDG uptake, implying that these 2 variables together contributed to treatment outcomes. The intensity of 18F-FDG uptake in lymphoma has been found to correlate with the histologic grade of malignancy (28,29). Although differences in SUV relative to histologic grade were significant, there were considerable overlaps between subgroups. This finding is in agreement with reports showing that enhanced glucose metabolism, as determined by SUV, was a strong indicator of tumor grade in other human malignancies, including gliomas and soft-tissue sarcomas (30,31). Because this study included patients with only a single type of lymphoma, ENKTL, the association between 18F-FDG uptake and histologic grade could not be assessed. The findings of our study indicate that tumor 18F-FDG uptake may reflect aggressive biologic behavior of ENKTL.
Indolent and aggressive lymphomas have shown considerable overlap in low SUV ranges (28,29). For example, the intensity of 18F-FDG uptake is generally lower in indolent than in aggressive non-Hodgkin's lymphomas (17). An SUV less than 10 captured 81% of indolent lymphomas, whereas an SUV greater than or equal to 13 was indicative of aggressive disease. The mean SUVmax of primary tumors in our patients (5.5) was generally lower than that in previous reports (17,28,29), possibly because of differences between institutions or lymphoma type. We used an SUV cutoff of 5.5 and found that all 5 nonresponders to initial therapy, compared with 5 of 16 responders (31%), had an SUV greater than 5.5 and that the mean SUVmax of these 2 groups was 8.4 and 4.5, respectively. Thus, an SUV greater than 5.5 was virtually indicative of aggressive disease, showing resistance to therapy.
Although involved-field radiotherapy or a combination of chemotherapy and radiotherapy is usually used to treat ENKTL, optimal therapy has not yet been determined. The management of this disease has been largely based on extrapolation from experiences with aggressive non-Hodgkin's lymphoma, with studies limited to small institutional series and heterogeneous treatments (4–7,10,11). Radiotherapy has been shown to improve patient survival, but the addition of anthracycline-based regimens had no effect (32,33). Moreover, in patients with extensive stage IE or IIE diseases, who have poor survival outcomes, the addition of chemotherapy to radiotherapy was not accompanied by improved survival (11,27). Therefore, although 18F-FDG PET can identify patients with ENKTL with aggressive disease or poor survival outcome, the therapeutic modality optimal for improving survival has not yet been determined.
To our knowledge, this study is the first to evaluate the utility of 18F-FDG PET in untreated patients with ENKTL. This study involved only patients with ENKTL of the head and neck, a rare clinical entity but not uncommon in East Asia. However, our study may have been limited by the relatively short follow-up after treatment, by its retrospective design, and by the small number of patients included. The limited number of patients may have contributed to our inability to determine the statistical significance of several reported prognostic factors, including IPI score, LDH level, the presence of B symptoms, and lymph node involvement. In addition, intermediate 18F-FDG PET after completion of treatment may be more accurate for prognostic prediction in patients with lymphoma (34) but has not been performed in this study. Early interim 18F-FDG PET may be a strong prognostic predictor, showing positive PET results after therapy indicating poor survival outcomes (34). Therefore, further prospective study, including therapy both before and after PET, may be required for clarifying the association between posttreatment PET results and treatment outcomes in ENKTL or other lymphoma subtypes.
CONCLUSION
We investigated the clinical usefulness of tumor 18F-FDG uptake on PET images in patients with ENKTL of the head and neck. We found that the SUV category of the primary tumor was an independent predictor of patient DSS. We also observed a strong association between LTI and SUV of the primary tumor. 18F-FDG PET may be clinically useful for predicting survival outcomes of patients with head and neck ENKTL. However, because our data applied to a particular selection of patients and the study collective was rather small, our results may not be generalized in patients with lymphoma.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 10, 2008.
- Accepted for publication August 11, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of Interim Positron Emission Tomography in Patients With Peripheral T-Cell Lymphoma
- Midtreatment 18F-FDG PET/CT Scan for Early Response Assessment of SMILE Therapy in Natural Killer/T-Cell Lymphoma: A Prospective Study from a Single Center
- The Role of 18F-FDG PET/CT for Initial Staging of Nasal Type Natural Killer/T-Cell Lymphoma: A Comparison with Conventional Staging Methods