


Abstract
Patients with esophageal squamous cell carcinoma (ESCC) are commonly at high risk of recurrence within 2 y after initial treatment. The aim of this study was to evaluate the role of 18F-FDG PET/CT in patients with possibly recurrent ESCC who underwent definitive treatment. Methods: Fifty-six patients with previously treated ESCC underwent PET/CT scans. The PET/CT findings were validated by histopathology or clinical follow-up of at least 6 mo. The sensitivity, specificity, and accuracy of PET/CT for detecting recurrence were calculated. Comparison of the standardized uptake value (SUV) was performed between patients grouped according to their status at the last follow-up (relapsed or relapse-free, alive or dead). The overall survival rates were estimated by the Kaplan–Meier method. The Cox proportional hazards model was used to evaluate independent prognostic variables for both univariate and multivariate survival analysis. Results: Forty-five (80.4%) patients had recurrence in 72 (66.1%) malignant sites. On PET/CT, there were 9 false-positive and 5 false-negative results. The overall sensitivity, specificity, and accuracy of PET/CT for detecting recurrence at all sites were 93.1% (67/72), 75.7% (28/37), and 87.2% (95/109), respectively. PET/CT was highly sensitive, specific, and accurate at regional and distant sites. At local sites, sensitivity was high, but specificity was lower (50%) because of a high incidence of false-positive findings. Patients who were confirmed with recurrence or who had died at the last follow-up had higher SUVs (P = 0.027 and <0.001, respectively). In multivariate survival analysis, therapeutic modality (hazard ratio = 0.437; P = 0.044), SUV (hazard ratio = 1.071; P = 0.029), and disease status on PET/CT (hazard ratio = 2.430; P = 0.045) were independent significant prognostic predictors for overall survival. The Kaplan–Meier survival curves indicated poor prognostic outcome in subgroup patients with higher SUVs or systemic disease on PET/CT. Conclusion: 18F-FDG PET/CT is highly effective for detecting recurrent ESCC. The relatively low specificity at local sites is associated primarily with a high rate of false-positive interpretations at anastomoses. PET/CT can also provide noninvasive and independent prognostic information using SUV and recurrent disease pattern on PET/CT images for previously treated ESCC.
Long-term survival remains poor for patients with esophageal cancer, with a 5-y survival rate of 15%–40%, even after apparently radical treatment (1–4). This finding occurs partly because most of these patients have advanced disease at the time of diagnosis, and the surgeries for them were often incomplete or even impossible. The survival rate could be even worse by exclusive palliative treatment in inoperable patients. The recurrence arising from the operative fields, radiotherapeutic targets, as well as regional lymph nodes was proven as the main cause for such a poor prognosis. About two thirds of the recurrence occurred within 1 y, and nearly all occurred within 2 y after the initial therapy (5). Early detection of these recurrences is often necessary because further treatment can contribute to prolonged tumor-free survival or occasional cure in this patient population (6).
Conventional imaging modalities such as CT, endoscopic ultrasonography (EUS), and MRI are the methods currently available for detecting recurrence on the basis of the alteration of tissue morphologic features. However, the diagnostic value of these techniques is practically limited because the initial treatment will inevitably cause significant distortions of the target tissues such as edema, fibrosis, or cicatrization, which would hamper an instant clinical diagnosis and the early subsequent treatment (7–11). Use of 18F-FDG PET as a functional imaging technique has been suggested to overcome these obstacles, as the additional metabolic information offered by PET usually precedes a structural change (8), and PET has recently shown promising results in detecting a large variety of recurrent malignancies besides esophageal cancer (9–11).
Combined functional–anatomic imaging with fused PET/CT is regarded as a further development of the PET technique (12). PET/CT can help in differentiating pathologic activity from physiologic radiotracer uptake and in localizing the lesion with more legible anatomic details (13). The aim of this study was to evaluate the diagnostic and prognostic value of PET/CT for patients with suspected recurrence after definitive treatment of esophageal squamous cell carcinoma (ESCC).
MATERIALS AND METHODS
Patients
From June 2003 to June 2005, 228 patients with newly diagnosed esophageal cancer had undergone definitive therapy in our Shandong Cancer Hospital and Institute. After providing written consent, 112 of these patients underwent whole-body PET/CT for the detection of possible recurrence. Only patients meeting the following 3 criteria were included in the study: (i) detailed medical records for the initial treatment, including curative operation or definitive radiation; (ii) indication of possible recurrence, such as questionable symptoms or signs, equivocal diagnosis by CT, EUS, MRI, or barium swallow; and (iii) no sign of infection at the time of posttreatment PET/CT scans.
Twenty-four patients were excluded from analysis because of inadequate medical records. Also excluded were 22 patients who underwent PET/CT as posttreatment surveillance, 8 patients who had infectious diseases at the time of PET/CT, and 2 patients with pathologically proven esophageal adenocarcinoma. The remaining 56 patients (47 men, 9 women; age range, 38–77 y) formed the cohort analyzed in this study. The clinicopathologic characteristics for those selected samples are outlined in Table 1. The interval between the conclusion of the initial therapy and PET/CT was 9.3 mo (95% confidence interval [CI], 7.4–11.2 mo). The dominant treatment modalities preceding PET/CT were primarily surgery (surgery alone, 4 patients; surgery plus radiation, 11 patients; surgery plus chemoradiation, 8 patients; surgery plus chemotherapy, 3 patients) or radiotherapy (radiotherapy alone, 3 patients; radiotherapy plus chemotherapy, 27 patients). Prescribed tumor dosages of 55∼65 Gy during 6∼7 wk were given to patients treated with postoperative radiation and 60∼75 Gy during 6∼8 wk to nonoperative patients. Maintenance chemotherapy using platinum with 5-fluorouracil was given when necessary.
Characteristics of Patients and Results of Univariate and Multivariate Survival Analysis for Predicting Overall Survival
18F-FDG PET/CT
All patients fasted and rested for at least 6 h before undergoing PET/CT (Discovery LS PET/CT system; GE Healthcare). Serum glucose levels were measured to ensure that the results were <6.6 mmol/L. Patients received no urinary bladder catheterization, no oral muscle relaxants, and no CT contrast agents. Sixty minutes after intravenous injection of 370 MBq (10 mCi) of 18F-FDG, PET emission images were acquired from the level of the middle skull to that of the proximal thigh for 5 min per field of view, each covering 14.5 cm, at an axial sampling thickness of 4.25 mm per slice. The spiral CT component was performed with an x-ray tube voltage peak of 120 kV, 90 mA, a 6:1 pitch, a slice thickness of 4.25 mm, and a rotation speed of 0.8 s per rotation. A full-ring dedicated PET scan of the same axial range followed. Both the PET and the CT scans were obtained during normal tidal breathing. The total acquisition time varied between 25 and 35 min per patient. PET images were reconstructed with CT-derived attenuation correction using the ordered-subset expectation maximization (OSEM) algorithm.
The attenuation-corrected PET images, CT images, and fused PET/CT images displayed as coronal, sagittal, and transaxial slices were viewed on a Xeleris workstation (GE Healthcare). Three experienced nuclear medicine physicians, who were aware of the patient's clinical history and recent radiographic data, reviewed together and interpreted the PET/CT images by consensus. For visual interpretation of the images, a focal 18F-FDG accumulation of intensity higher than that in surrounding tissues and not clearly associated with normal structures was considered to be indicative of malignancy. For further semiquantitative analysis, regions of interest (ROIs) were delineated on transaxial images around the areas with increased 18F-FDG uptake, and the standardized uptake value (SUV) was calculated on the Xeleris workstation. The maximum SUV within a ROI was used to minimize partial-volume effects.
The final PET/CT reports (positive, equivocal, or negative) were based primarily on the visual analysis, using SUV ≥ 2.5 only as the reference criterion. The reports were validated by comparison with histopathologic findings or clinical follow-up of at least 6 mo. Recurrence or metastasis was considered when there was an abnormal finding suggesting recurrence or metastasis on serial imaging studies or pathologically confirmed malignancy. For patient-based analysis of the diagnostic value of PET/CT, any single true-positive site was deemed sufficient to consider PET/CT true-positive. All 3 sites (local, regional, and distant) were required to be true-negative to consider PET/CT true-negative.
Data Analysis
With equivocal sites considered positive, the sensitivity, specificity, and accuracy of PET/CT for detecting recurrence were analyzed by the Pearson χ2 test (or the Fisher exact test). An independent sample t test was used for comparing SUVs between patient subgroups. Only the highest SUV among all sites was analyzed for each patient, and the SUV of the site to be evaluated at the presentation for PET/CT (e.g., the primary tumor after treatment) was recorded if the corresponding PET/CT images had no positive findings.
All patients were monitored to a closeout date of July 1, 2006. The overall survival (OS) was measured from the date of the conclusion of the initial therapy to that of death from any cause. The Kaplan–Meier survival curve was used to estimate OS. Survival differences between subgroups were tested using the log-rank test. The Cox proportional hazards regression model was used to evaluate prognostic factors (using SUV and age as continuous variables) in univariate analyses. Only significant variables after univariate analysis (P < 0.1) were included in multivariate survival analysis. All statistical analyses were performed using the SPSS version 12.0 software package for Windows (Microsoft). P < 0.05 was considered significant.
RESULTS
Validation of Recurrence
The gold standard (histology or follow-up) established tumor recurrence at 72 sites in 45 (80.4%) patients. Of these, the presence of 33 recurrent sites were established by histopathology, which consisted of local recurrence in 21, mediastinal nodal metastasis in 3, supraclavicular lymph nodes metastasis in 5, liver metastasis in 2, incision metastasis in 1, and rib metastasis in 1. The remaining 39 sites were confirmed by follow-up, which consisted of local recurrence in 11, mediastinal lymph nodes metastasis in 16, distant lymphatic metastasis in 4, liver metastasis in 3, lung metastasis in 2, bone metastasis in 2, and adrenal gland metastasis in 1.
Diagnostic Value of PET/CT
PET/CT reported 76 positive sites of recurrent diseases. Of these, 37 sites were locally positive, 19 were regionally positive, and 20 were distantly positive. The sensitivity, specificity, and accuracy of PET/CT were 96.9%, 50%, and 84.1% for local recurrence, 89.5%, 81.8%, and 86.7% for regional recurrence, and 90.5%, 92.9%, and 91.4% for distant metastasis, respectively. The sensitivity and accuracy at all sites tended to be high, whereas the specificity at local sites was significantly lower than that at distant sites (50% vs. 92.9%; P = 0.026). The overall specificity in both site-based (75.7%) and patient-based (54.5%) analysis was decreased accordingly (Table 2).
Diagnostic Value of PET/CT for Detecting Recurrent ESCC
Among the 9 false-positive (FP) interpretations rendered on PET/CT, 5 lesions exhibited distinctly increased 18F-FDG uptake at the esophagogastric anastomosis but revealed no biopsy-proven recurrence by repeated endoscopy (Fig. 1). The remaining 4 FP interpretations—including 1 focus near the back wall of gastric pull-up, 2 at hilar nodes, and 1 in the left lower lung—had also been excluded from recurrence after close follow-up.

A 49-y-old male patient with ESCC complained of discomfort of retrosternal burning after esophagectomy. PET/CT scan 4 mo after surgery demonstrated on fusion (A) and serial PET (B) images a positive focus suggestive of recurrence at esophagogastric anastomosis (SUV = 9.8); the lesion was shown to be FP by repeated endoscopy with biopsy.
PET/CT also had 5 false-negative (FN) interpretations. The first one occurred in a patient who had no positive PET/CT findings after radical radiotherapy. Five months later, he had dysphagia, and endoscopy validated malignancy at the location of primary tumor. The second patient had a subcarina lymph node measuring 1.2 cm in short-axis diameter on PET/CT (maximum SUV, 2.3) at 2 mo after the completion of radiation therapy. Three months after the PET/CT scan, the shortest diameter of this node in the transverse axis increased to approximately 3 cm on follow-up CT. The third patient had a persistent dry cough starting at 2 mo after surgery, but both subsequent CT and PET/CT showed no trace of a cancer-related focus. However, a paratracheal lymph node measuring 2.3 cm in diameter was detected on CT at 6-mo follow-up after surgery. The fourth FN interpretation involved a supraclavicular lymph node in a patient with upper-segment esophageal cancer that was treated with radiation at both the primary tumor and the regional nodes (Fig. 2). The last FN interpretation was a 0.5-cm lung nodule at the right lower lobe. It was first detected by contrast-enhanced CT after radiation and was not visible on the concurrent PET/CT image. Serial CT images during follow-up confirmed this lesion to be a distant metastasis.
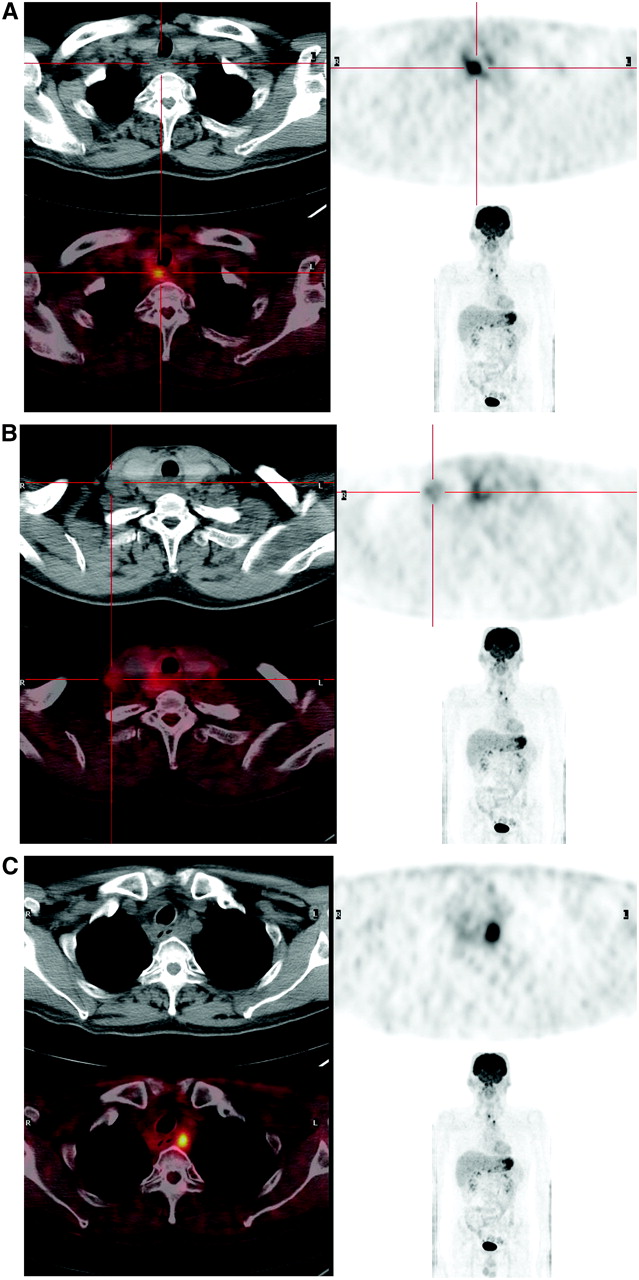
Whole-body PET/CT in 65-y-old man who received irradiation of primary tumor in upper segment of esophagus and regional lymph nodes in supraclavicular and upper mediastinal area. PET/CT displayed multifocal recurrence. (A) Increased 18F-FDG accumulation remained at primary tumor site (SUV = 6.1), indicating tumor residual disease. (B) Mild focal uptake exhibited in a supraclavicular lymph node with a minor SUV of 2.1. This lesion was subsequently confirmed as malignant by biopsy. (C) Area of abnormally increased uptake was also visible at a left paratracheal lymph node (SUV = 7.8), which proved to be metastatic on follow-up.
Comparison of SUVs
The overall mean SUV for all 56 patients was 9.26 (95% CI, 7.92–10.61). Forty-five patients confirmed with recurrence had a significantly higher SUV than that of the remaining 11 relapse-free patients (mean SUV: 9.98 [95% CI, 8.48–11.50] vs. 6.29 [95% CI, 3.60–8.97]; P = 0.027). Thirty-two patients who died (including 2 patients who were lost to follow-up) had a significantly higher SUV than that of the remaining 24 patients who were still alive at last follow-up (mean SUV: 11.24 [95% CI, 9.54–12.94] vs. 6.62 [95% CI, 4.84–8.40]; P < 0.001).
Prognostic Value of PET/CT
Up to the closeout date of July 1, 2006, the median follow-up period was 24.5 mo (range, 4–34.5 mo) with 2 (3.6%) patients lost to follow-up. Univariate survival analysis indicated that the therapeutic modality, tumor location, SUV, and disease status on PET/CT were significant prognostic predictors for OS. After multivariate analysis, only the therapeutic modality, SUV, and disease status on PET/CT were independent prognostic predictors for OS (Table 1).
We selected the overall mean SUV of 9.26 as a cutoff value to form 2 groups—one above and the other below the cutoff value. The mean OS was estimated as 15.2 mo (95% CI: 11.6–18.7 mo) for the higher SUV group (n = 26) and was 24.3 mo (95% CI: 19.9–28.7 mo) for the lower SUV group (n = 30). The Kaplan–Meier analysis indicated that OS was significantly higher for the lower SUV group than that for the higher SUV group (P = 0.0102; Fig. 3).
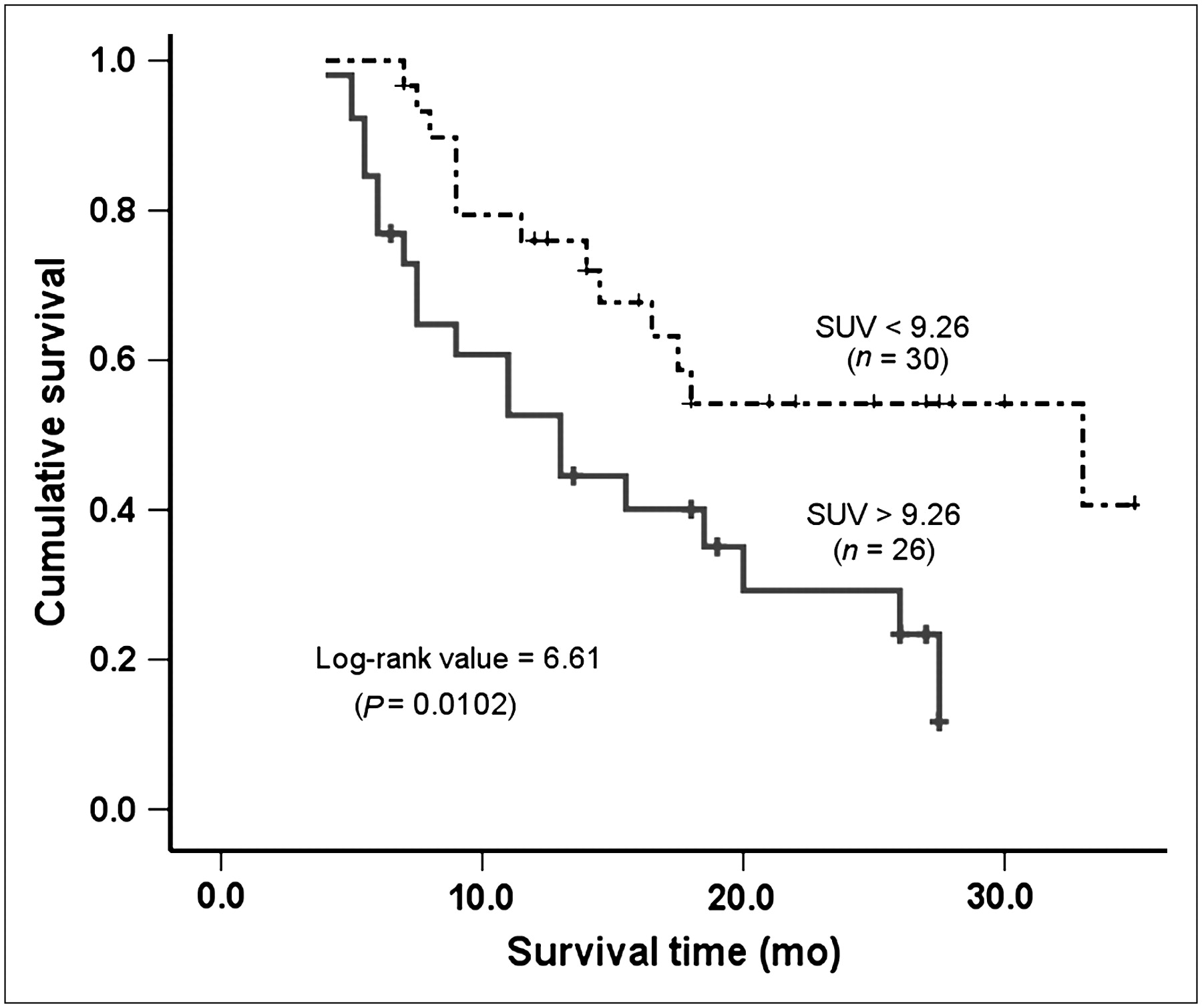
Kaplan–Meier curves of OS for 2 subgroups divided according to SUV (cutoff, 9.26). Patients with censored OS times are shown by tick marks.
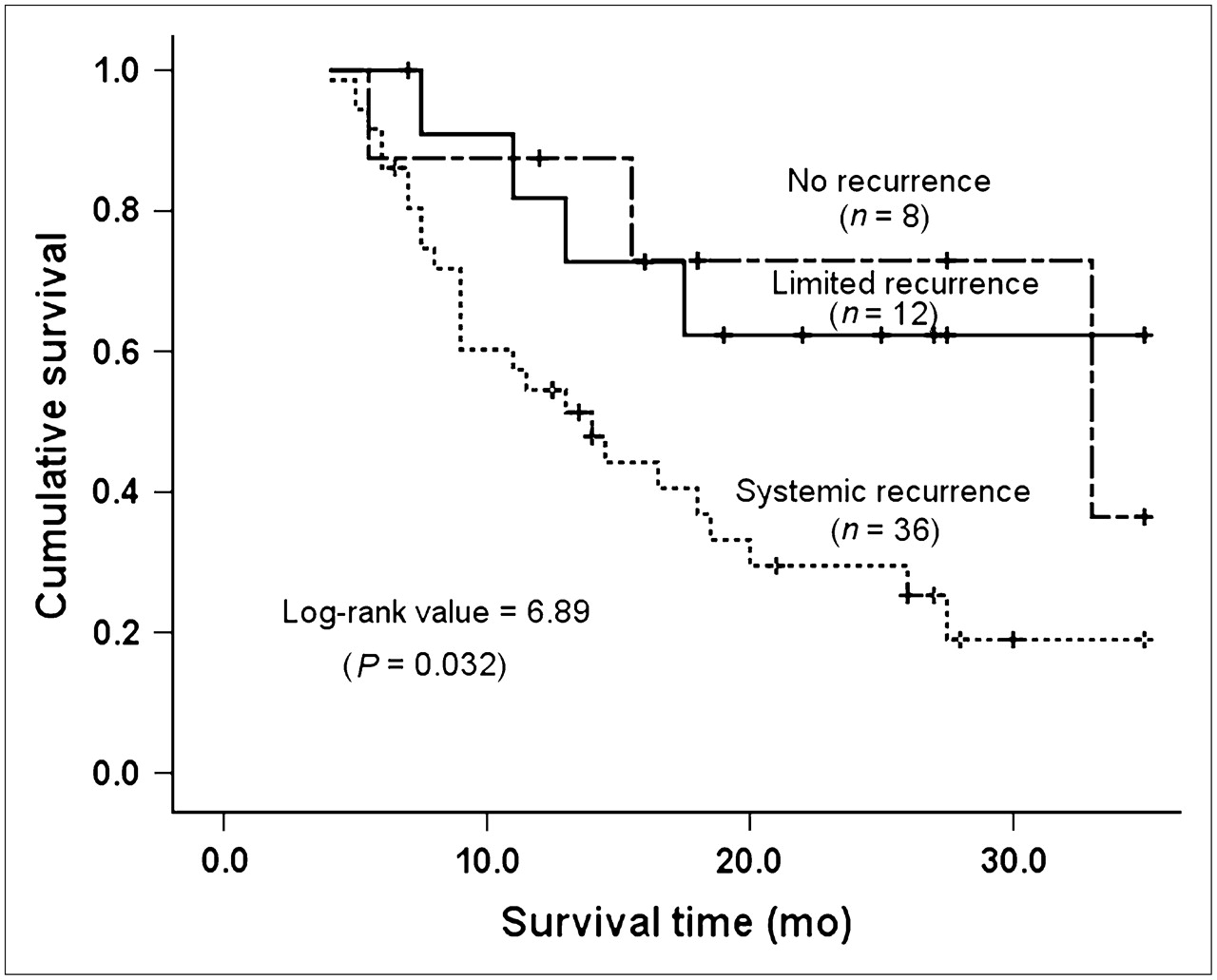
On the basis of the disease distribution on PET/CT, patients were classified as having no recurrence (8 patients), having limited recurrence (limited locoregional or solitary metastasis, 12 patients), and having systemic recurrence (extensive locoregional or multifocal metastasis, 36 patients). PET/CT accurately classified 5 of 11 patients as having no recurrence, 7 of 11 patients as having limited recurrence, and 32 of 34 patients as having systemic recurrence (Table 3). In survival analysis with the Kaplan–Meier method (Fig. 4), there was a significant difference in OS among the 3 groups (P = 0.032, log-rank test). However, the survival curves of the patients with limited recurrence and negative scans cross. Comparing patients having (36 cases) and not having (20 cases) systemic disease indicated that the estimated mean OS for the former (17.1 mo; 95% CI: 13.3–20.8 mo) was significantly lower than that for the latter (26.9 mo; 95% CI: 22.0–31.9 mo). OS was significantly lower for the group of patients having systemic disease (P = 0.009, log-rank test).
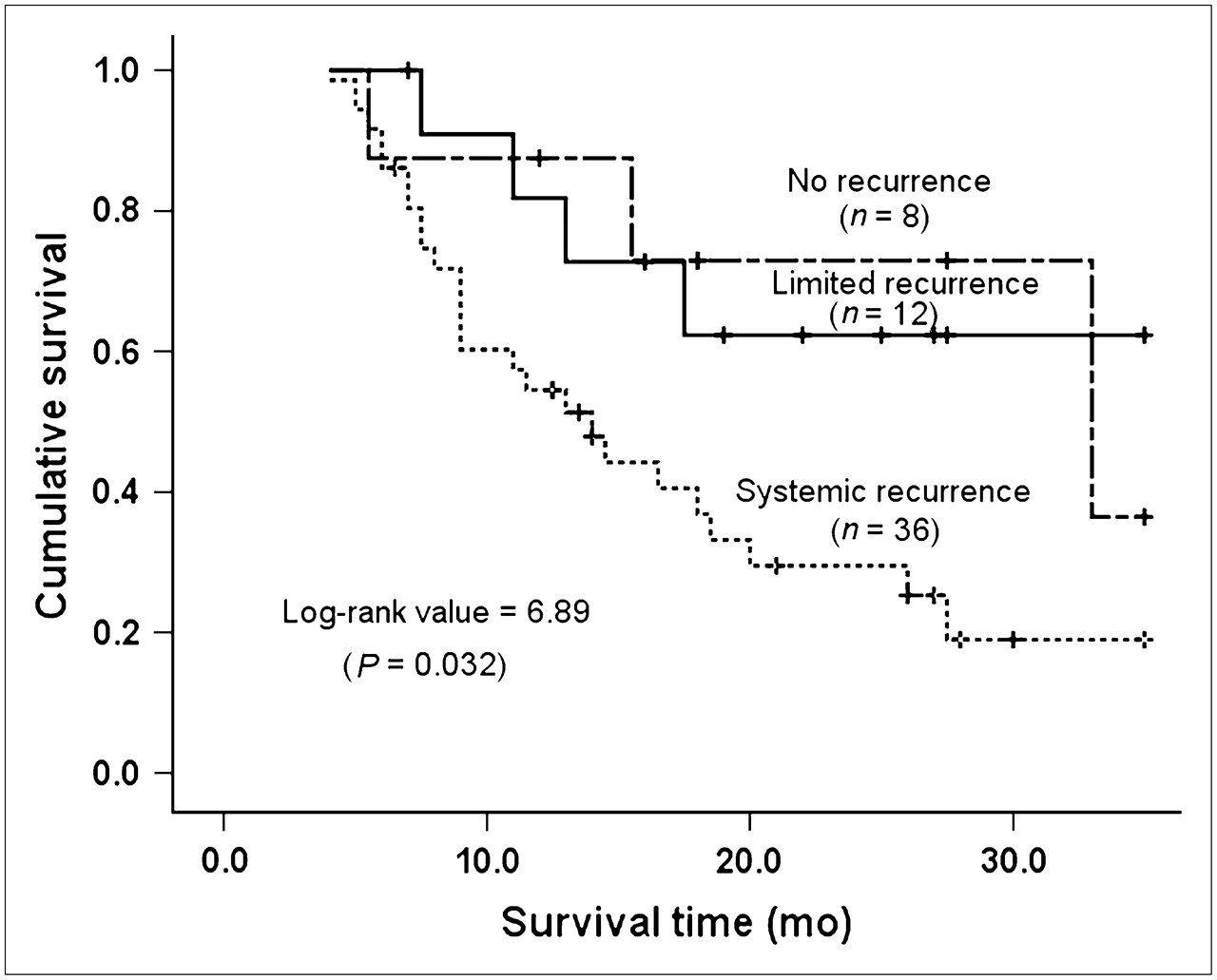
Kaplan–Meier curves of OS for 3 subgroups stratified by disease pattern according to PET/CT. Patients with censored OS times are shown by tick marks.
Categorization of Disease According to PET/CT and Pathologic/Clinical Validation
DISCUSSION
It was reported that PET/CT using the radiolabeled glucose analog 18F-FDG was valuable in detecting recurrence of esophageal cancer, particularly when anatomic imaging modalities have presented equivocal interpretations (9–11,14). Whole-body PET not only gains an advantage over CT in detecting distant metastatic lesions (11) but also improves currently applied staging of esophageal cancer (15). Moreover, it allows a highly sensitive diagnosis and accurate whole-body staging in postoperative patients with esophageal cancer (9,10). However, clinicians often face the problem of recurrence in patients treated by multiple modalities. The indications that might prompt a PET scan usually include new or suggestive symptoms, equivocal or suspicious findings on clinical examination, and equivocal or abnormal radiologic results. Taking the expensive cost into consideration, use of PET only as a tool for postoperative monitoring in the absence of any apparent indications is often unusual. Therefore, we conducted a study enrolling problematic patients with esophageal cancer after complex treatment, and available clinical and recent radiographic data could correlate with the PET/CT findings during interpretation. As most of the requested PET/CT scans met the clinical need, the current study could be merged easily into the routine clinical practice and patients were willing to participate in the study.
Our study demonstrated that PET/CT was highly sensitive and accurate for detecting recurrent ESCC, particularly at regional and distant sites (sensitivity, 89.5% vs. 90.5%; specificity, 81.8% vs. 92.9%; accuracy, 86.7% vs. 91.4%). It seems that the identification of any one positive site of focal 18F-FDG uptake in the regional or distant area was deemed sufficient to determine a subsequent therapeutic regimen for the involved sites. In contrast, the specificity at local sites (50%) and in patient-based analysis tended to be lower because of a high incidence of FP findings. However, PET/CT had a high sensitivity in detecting recurrence (93.1% in overall site-based analysis and 95.6% in patient-based analysis), and positive PET/CT may encourage a clinician to scout the suggestive area or even pursue more aggressive biopsies in an attempt to establish a definitive diagnosis, as PET/CT provides precise anatomic localization through its resolution details (13,16).
Physiologic 18F-FDG uptake in the alimentary tract, including esophagus, gastric tube, and anastomosis, was often presented in a mild degree. However, the enhanced 18F-FDG uptake due to postoperative tissue repair or inflammatory changes would make it difficult to differentiate nontumor-specific disorders from malignancy. In our study, 5 FP sites at esophagogastric anastomosis and one FP site at gastric pull-up might be associated with gastroesophageal reflux or the healing phase after surgery. The other 2 FP results of hilar nodes might arise from chronic inflammation, as commonly seen in patients with chronic respiratory tract disease or in heavy smokers. The last FP interpretation of pulmonary focus turned out to be radiation-induced pneumonitis after follow-up. This finding suggests that thorough inquiry of the medical record, careful physical examination, repeated review of previous imaging results, and close communication between clinicians and radiographic physicians may potentially limit the FP findings of PET/CT.
Small lesions beyond the resolution of the PET/CT system may be missed because of the partial-volume effect (17,18). This was illustrated by one of the FN cases with an enlarging paratracheal lymph node. Similarly, pulmonary nodules of <1 cm in diameter might blur on PET images (19). In the case of PET/CT, a 0.5-cm pulmonary nodule was also misdiagnosed in our study. Another possible reason for this FN result might be associated with the error in imaging coregistration between PET and CT. Pan et al. (20) reported that a moving organ with respiration (lung) or peristalsis (bowel) often causes this mistake. Repeated review of the images on the CT component, or gated PET/CT, or additional contrast-enhanced CT may partially solve this problem. The remaining 3 FN results were all correlated with the changes after radiation; PET/CT showed a temporary decrease in metabolic activity of the irradiated lesion with a decreased SUV, whereas the residual tumor still posed a threat of recurrence (21). In this instance, the optimal timing of the PET/CT scan after the conclusion of therapy should be further investigated to minimize these FN interpretations.
Our study demonstrated that the mean SUV tended to be high for patients with confirmed recurrence or patients who had died during follow-up, and a higher SUV generally indicated an adverse prognostic outcome. However, the SUV itself may be affected by many different factors, including body fat, body surface area, blood sugar level, blood supply of the target organ, and the method to draw the outline of the ROI (22,23). Therefore, the criterion for measuring the SUV must be standardized and unified, and the optimal timing of the PET/CT scan after the conclusion of therapy should be considered to avoid recent infection or invasive procedures such as esophageal dilation. Furthermore, a thorough awareness of the patient's medical record and prior radiologic data might add favorable information to the SUV criterion for improving diagnostic accuracy.
Several reports (24,25) have described the role of the PET scan on prognosis, but none has touched on recurrent esophageal cancer. In our study, both SUV and disease status on PET/CT were independent significant predictors for OS in multivariate analysis. Furthermore, Kaplan–Meier analysis indicated that a subset of patients with higher SUVs (Fig. 3) or systemic recurrent disease on PET/CT (Fig. 4) was subject to remarkably increased risks of death. This suggests that PET/CT findings can stratify survival, specifically between those with systemic spread compared with either limited recurrence or a negative scan. Although the survival curves of the patients with limited recurrence and negative scans cross (Fig. 4), PET/CT still offered substantially significant incremental information beyond clinical examination, which may have clinical implications with regard to patient surveillance and subsequent treatment.
There are several limitations in our study. First, interpreting PET/CT images without double blindness to the clinical information might result in a higher sensitivity of PET/CT and preclude a fair comparison between PET/CT and other imaging modalities. Second, too many patients lack pathologic validation in potentially recurrent sites, and, third, most subjects were at an advanced stage (stage III–IV). Therefore, patients with a high incidence of recurrence readily present with positive PET/CT findings or even multifocal 18F-FDG accumulation. Other limitations of this study include the possible variability of interpretation between different nuclear medicine physicians and the potential underreporting of the lesions on PET/CT with multiple foci of 18F-FDG uptake.
CONCLUSION
In this study, PET/CT has displayed a remarkable sensitivity and a high specificity and accuracy at regional and distant sites for recurrent ESCC. 18F-FDG PET/CT can be recommended as a preferred tool for patients who have elusive clinical manifestations or equivocal results from conventional imaging modalities. The SUV and the disease pattern (with or without systemic recurrence) on PET/CT can offer incremental information in the prognostic evaluation. Although the specificity at the local area tends to be lower due to a high rate of FP findings, PET/CT remains valuable because positive PET/CT can encourage clinicians to make efforts to establish a definitive diagnosis through biopsies or close follow-up, and the patients confirmed with recurrence would benefit from subsequent salvage therapy.
Acknowledgments
The authors thank Prof. Fang-Fang Yin (Department of Radiation Oncology, Duke University Medical Center, Durham, NC) for his active cooperation.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 15, 2006.
- Accepted for publication May 1, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}