


Abstract
Pulmonary uptake of 18F-FDG assessed with PET has been used to quantify the metabolic activity of inflammatory cells in the lung. This assessment involves modeling of tracer kinetics and knowledge of a time–activity curve in pulmonary artery plasma as an input function, usually acquired by manual blood sampling. This paper presents and validates a method to accurately derive an input function from a blood-pool region of interest (ROI) defined in dynamic PET images. Methods: The method is based on a 2-parameter model describing the activity of blood and that from spillover into the time–activity curve for the ROI. The model parameters are determined using an iterative algorithm, with 2 blood samples used to calibrate the raw PET-derived activity data. We validated both the 2-parameter model and the method to derive a quantitative input function from ROIs defined for the cavities of the right and left heart and for the descending aorta by comparing them against the time–activity curve obtained by manual blood sampling from the pulmonary artery in lungs with acute inflammation. Results: The model accurately described the time–activity curve from sampled blood. The 2-sample calibration method provided an efficient algorithm to derive input functions that were virtually identical to those sampled manually, including the fast kinetics of the early phase. The 18F-FDG uptake rates in acutely injured lungs obtained using this method correlated well with those obtained exclusively using manual blood sampling (R2 > 0.993). Within some bounds, the model was found quite insensitive to the timing of calibration blood samples or the exact definition of the blood-pool ROIs. Conclusion: Using 2 mixed venous blood samples, the method accurately assesses the entire time course of the pulmonary 18F-FDG input function and does not require the precise geometry of a specific blood-pool ROI or a population-based input function. This method may substantially facilitate studies involving modeling of pulmonary 18F-FDG in patients with viral or bacterial infections, pulmonary fibrosis, and chronic obstructive pulmonary disease.
PET imaging of 18F-FDG is increasingly used to assess the metabolic activity of pulmonary inflammatory cells (1–7). The uptake rate of 18F-FDG by tissue can be computed using either compartmental models (8) or a graphical technique (9). A prerequisite for either analysis is knowledge of the input function to the system in the form of a plasma time–activity curve. Acquisition of such an input function typically involves sequential blood sampling, a process that is invasive, is prone to measurement artifacts, exposes the clinical staff to radiation and blood, and adds costly laboratory procedures. To avoid or minimize manual blood sampling, substantial effort has been devoted to developing alternative techniques, which have successfully been applied to estimate 18F-FDG uptake in tumors and brain. Some of these techniques involve population-based assumptions about the input function (10–13), whereas others directly estimate the input function from blood-pool regions of interest (ROIs) in the PET images (14–18).
However, population-based assumptions about the input function are not available for 18F-FDG uptake by the inflamed nonneoplastic lung and may vary for different types of pulmonary inflammation. Also, estimates of the input function from blood-pool ROIs are affected by partial-volume effects and by activity spillover from the heart or inflamed pulmonary tissues. Moreover, in contrast to brain, heart, or solid tumor tissues, where the blood-to-tissue fraction is low, blood volume in the lung may account for as much as half the parenchymal volume. As a result, the blood compartment is a dominant source of lung 18F-FDG activity, particularly early after tracer injection. Because early-phase kinetics affect estimates of distribution volumes and rapid rate constants, accurate assessment of the early-phase input function might be crucial for characterizing the inflamed lung. Although techniques to reduce blood sampling are available, they seem to have limited accuracy in describing the early-phase input function (13,14,17–19) or are unable to assess the early phase of the input function at all (10–12). Techniques involving image-derived assessment of the early input function either neglected partial-volume effects (18) and activity spillover artifacts (15) or mathematically corrected for these artifacts by measuring the anatomic dimensions of the blood-pool ROI used (16). Alternatively, spillover from myocardium into the left ventricle was calculated on the basis of the difference in activity between the arterial and ROI-derived curves at the last sampled point, and a standard myocardial wall thickness was assumed to correct for partial-volume effect (17).
In this paper, we present and validate a method of obtaining an image-derived input function for compartmental modeling of 18F-FDG kinetics in the lung. The method is based on a 2-parameter model of the blood-pool ROI that accounts for partial-volume and spillover artifacts, is not restricted to a blood-pool ROI with precisely known geometry, and does not assume a population-based input function.
MATERIALS AND METHODS
Model-Based Computation of a PET Image–Derived Input Function
We model the PET signal from a blood-pool ROI (CROI(t)) by 2 compartments. One accounts for 18F-FDG activity from blood plasma (Cp(t)), and the other for spillover activity from tracer that accumulates in tissue surrounding the ROI. We define a recovery coefficient (RC) quantifying a geometric partial-volume effect and a spillover coefficient (SC) to quantify activity spillover from phosphorylated 18F-FDG in the surrounding tissue. SC is a function of the 18F-FDG uptake rate in surrounding tissue, the geometry of the ROI, and the spatial resolution of the imaging instrument. CROI(t) is expressed as Eq. 1where the integral describes the time course of 18F-FDG phosphorylation in surrounding tissue as a function of 18F-FDG availability in blood. This simplification is expected to yield a time course that is sufficiently accurate for the purpose of spillover correction. Dividing both sides of Equation 1 by Cp(t) yields an instantaneous calibration factor between CROI(t) and Cp(t):
Eq. 1where the integral describes the time course of 18F-FDG phosphorylation in surrounding tissue as a function of 18F-FDG availability in blood. This simplification is expected to yield a time course that is sufficiently accurate for the purpose of spillover correction. Dividing both sides of Equation 1 by Cp(t) yields an instantaneous calibration factor between CROI(t) and Cp(t): Eq. 2
Eq. 2
The structure of this linear equation is identical to the equation used in the Patlak method (20). However, in addition to a different interpretation of the slope in our model (SC), the ordinate intercept (termed initial volume of distribution in the Patlak method) represents here the RC, which depends on ROI geometry and spatial resolution characteristics of the PET camera. By assuming that RC and SC are constant during the imaging period and measuring plasma activity with 2 blood samples, Cp(t1) and Cp(t2), taken at time points t1 and t2, we can write Equation 2 as an equation system: Eq. 3
Eq. 3
To solve Equation 3 for RC and SC, we need the integral of the unknown time course of Cp(t), which is obtained using the iterative algorithm summarized in the flow chart in Figure 1. The algorithm begins by assuming that CROI(t) is an initial estimate of Cp(t) ( ), which is used to calculate the integral in Equation 3 as
), which is used to calculate the integral in Equation 3 as Eq. 4where Δtk was the duration of the kth image frame and n refers to the nth time point of the integral. Then, solving Equation 3 provides current (ith) estimates of RC and SC (RC[i] and SC[i]), which are used to obtain the next estimate of Cp(t),
Eq. 4where Δtk was the duration of the kth image frame and n refers to the nth time point of the integral. Then, solving Equation 3 provides current (ith) estimates of RC and SC (RC[i] and SC[i]), which are used to obtain the next estimate of Cp(t),  , as
, as Eq. 5
Eq. 5
This procedure is repeated until estimates of plasma activity at t1 and t2 converge to measured values (i.e.,  and
and  with an error (e) defined as
with an error (e) defined as Eq. 6of less than 105.
Eq. 6of less than 105.

Iterative algorithm for calculating model-adjusted input function ( ). Method is based on 2-compartment model. PET signal from blood-pool ROI is separated in blood and activity spillover component by estimating RC and SC. Index [i] refers to number of iterations. CROI(t) = raw PET signal from blood-pool ROI;
). Method is based on 2-compartment model. PET signal from blood-pool ROI is separated in blood and activity spillover component by estimating RC and SC. Index [i] refers to number of iterations. CROI(t) = raw PET signal from blood-pool ROI;  estimate of plasma activity; Cp(t1) and Cp(t2) = calibration measurements of plasma activity, obtained at times t1 and t2.
estimate of plasma activity; Cp(t1) and Cp(t2) = calibration measurements of plasma activity, obtained at times t1 and t2.
Experimental Data
We analyzed data from previous studies of pulmonary inflammation in sheep. These studies, in which pulmonary 18F-FDG kinetics were measured with dynamic PET and pulmonary artery blood sampling, included 5 sheep exposed to unilateral smoke inhalation (3) and 10 sheep exposed to unilateral injurious ventilation (2). Specific details about animal preparation can be found in the original publications. In brief, a Swan–Ganz catheter (7.5 French) was advanced to the pulmonary artery. The proximal (central venous) port was used for administration of the radioisotope and the distal port for sampling of pulmonary artery blood. Each sheep was positioned prone in the PET camera (Scanditronix PC4096; GE Healthcare), with the most caudal slice adjacent to the diaphragmatic dome to maximize the imaged lung volume (21). The camera collected 15 transverse cross-sectional slices of 6.5-mm thickness over a 9.7-cm-long axial field.
PET data recorded during intravenous bolus injection of 13NN saline solution (344 ± 96 MBq dissolved in 30 mL) were used to define the ROI for the right heart (RH) cavities. These PET data were acquired to assess regional pulmonary perfusion in the previous studies (2,3), in which simultaneously with the start of the 13NN-saline injection, image acquisition was started with an initial framing rate of 2.5 s per frame.
After the 13NN was cleared from the lungs, a bolus of 18F-FDG (∼370 MBq) was injected at a constant rate over 1 min into the superior vena cava, followed by a flush of saline at the same rate. Acquisition of a series of PET images was started simultaneously with 18F-FDG injection (t = 0). The protocol consisted of acquiring consecutive images for a total of 75 min (6 × 30 s, 7 × 1 min, 15 × 2 min, 1 × 5 min, and 3 × 10 min). An additional study was conducted with a modified protocol involving a prolonged tracer injection time (90 s) and an increased initial framing rate (8 frames over the first 2 min after tracer injection).
PET images were reconstructed in an interpolated matrix of 128 × 128 × 15 voxels, each with a size of 2 × 2 × 6.5 mm. The time course of 18F-FDG activity in blood plasma was measured from sequential 1-mL samples of pulmonary artery blood in a well counter cross-calibrated with the PET camera. The intervals between blood samples were 11 × 15 s, 4 × 30 s, 5 × 1 min, 11 × 5 min, and 1 × 10 min. Thus, for the first 4.5 min, the time points of blood sampling were synchronized with the mid-frame time points of PET. For t > 4.5 min, the plasma measurements were linearly interpolated and values coinciding with the mid-frame time points of the PET frames were derived from the interpolated data.
Three ROIs were defined in the images delineating the descending aorta, RH cavities, and left heart (LH) cavities. The RH-cavity ROI was identified by thresholding the regional activity of 13NN during the first 5 s after 13NN-saline injection. During this time 13NN is confined mostly to the RH cavities and pulmonary arteries, and only a minor amount has diffused into the alveolar gas volume (Fig. 2A). The LH-cavity and aorta ROIs were generated using the 18F-FDG image data. To delineate the aorta, we applied a threshold of about 50% to regional 18F-FDG activity from 1.5 to 2.5 min after the start of injection (Fig. 2B). Regional activity in the interval from 55 to 65 min after 18F-FDG bolus injection was used to identify the wall of the left ventricle (Fig. 2C). The ROI over the LH cavities was manually drawn along the inner border of the left ventricular wall by the use of custom-made image-processing software. In cases in which myocardial uptake was low, the LH-cavity masks were generated from the early injection images.
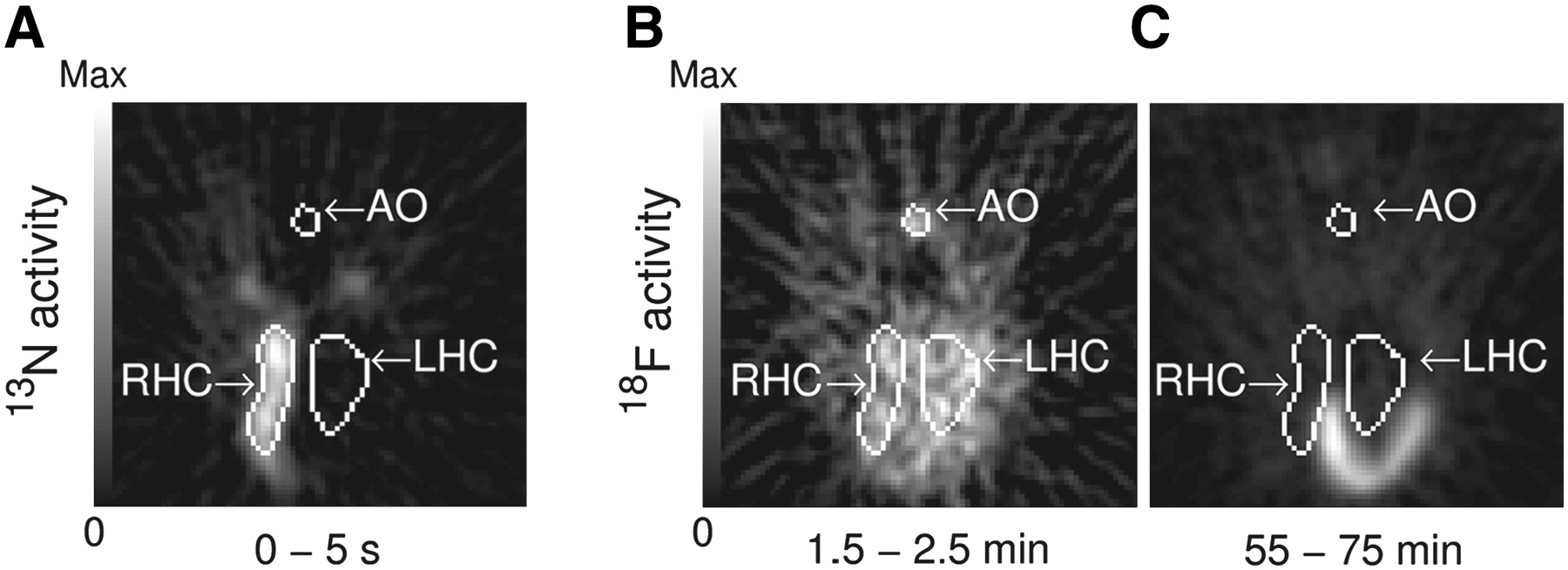
Delineation (white outlines) of blood-pool ROIs in descending aorta (AO) and in RH cavities (RHC) and LH cavities (LHC) on representative image slice: regional activity after intravenous single-bolus injection of 13N-nitrogen dissolved in saline (A) and 18F-FDG activity, on identical scale, shortly after tracer injection and at end of imaging (B and C, respectively). The 3 ROIs are shown together only for illustration purposes.
Comparison Between Model-Adjusted Input Function and Manual Blood Samples
The relative mean squared error (mse) between manually sampled plasma activity (Cp(t)) and the time course of the model-adjusted input function (C̃p(t)), excluding the first 2 blood samples, was calculated from all points at which PET image frames coincided with blood samples: Eq. 7with n = 32. The first 2 measurements were excluded because, at this early phase, some of the manually sampled data were skipped or corrupted by timing errors.
Eq. 7with n = 32. The first 2 measurements were excluded because, at this early phase, some of the manually sampled data were skipped or corrupted by timing errors.
To evaluate the influence of the first calibration sample time on mse, its timing (t1) was systematically varied within the interval from 1.75 to 25 min, using time points corresponding to mid-frame time points. The timing of the second calibration sample was fixed at t2 = 50 min. An identical procedure was followed for each of the 3 ROIs, and the corresponding mse data were compared with the nonparametric Wilcoxon signed rank test. The level of significance was P < 0.05. To test the robustness of our method to blood-pool ROI definition, the ROIs were systematically dilated, and the model-adjusted input function was computed for each increment in ROI volume. Bland–Altman plots (22) were used to illustrate the agreement between Ki values computed with manual blood sampling and either raw or model-adjusted input functions.
Patlak Graphical Analysis
The pulmonary uptake rate of 18F-FDG (Ki) for injured and control lungs was calculated by Patlak graphical analysis (20), starting 15 min after tracer injection, using the manually sampled input function, raw PET signals from the blood-pool ROIs, and input functions generated with the 2-compartment model.
RESULTS
The linear model formulated by Equation 2 provided an excellent approximation of the PET signals from the blood-pool ROIs (Fig. 3A). Using the iterative algorithm (Fig. 1), we found that estimates of RC and SC converged within ≤6 iterations to their final values (Fig. 4). For the ROI volumes used, RC was on average highest for the LH cavities and lowest for the aorta (Table 1). SC was about the same for all 3 ROIs. With increasing ROI volume, average SC increased for all 3 ROIs and was highest for the LH cavities and lowest for the RH cavities for ROI volumes > 70 mL (Fig. 3B). Figure 3C depicts average SC values normalized by (1 − RC) as a function of blood ROI volume. Values of SC/(1 − RC) were consistently highest for the LH cavities and smallest for the aorta for ROI volumes ≤ 75 mL. For 1.75 min ≤ t1 ≤ 25 min, the mse between model-adjusted input function and manually sampled input function was on average lowest for the LH cavities and highest for the RH cavities (Fig. 5). Also within this period, mean mse for the LH cavities was fairly insensitive to t1, with a minimum at t1 = 4.5 min.
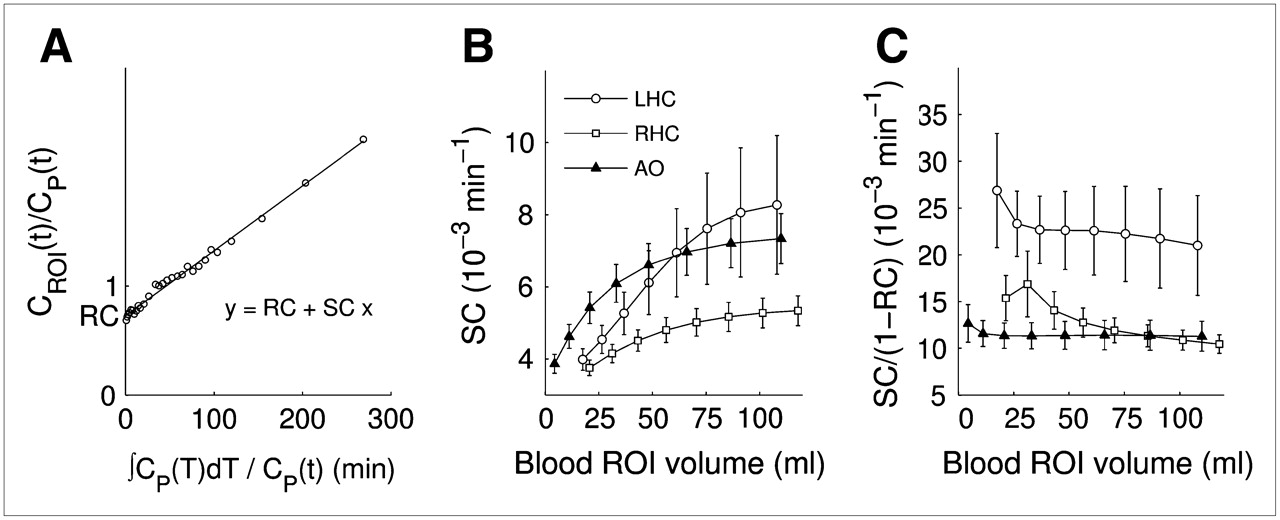
Evaluation of model fit and effect of ROI volume on estimated parameter SC: representative model fit according to Equation 2 for dynamic PET data measured in blood-pool ROI over LH cavities (A), average SC obtained for blood-pool ROIs of varying size, illustrating how algorithm adjusts SC to different conditions (B); normalized SC/(1 − RC), illustrating differences in 18F-FDG uptake rates (C). Error bars are ±1 × SE. ROIs with lowest volume were used for analyses.
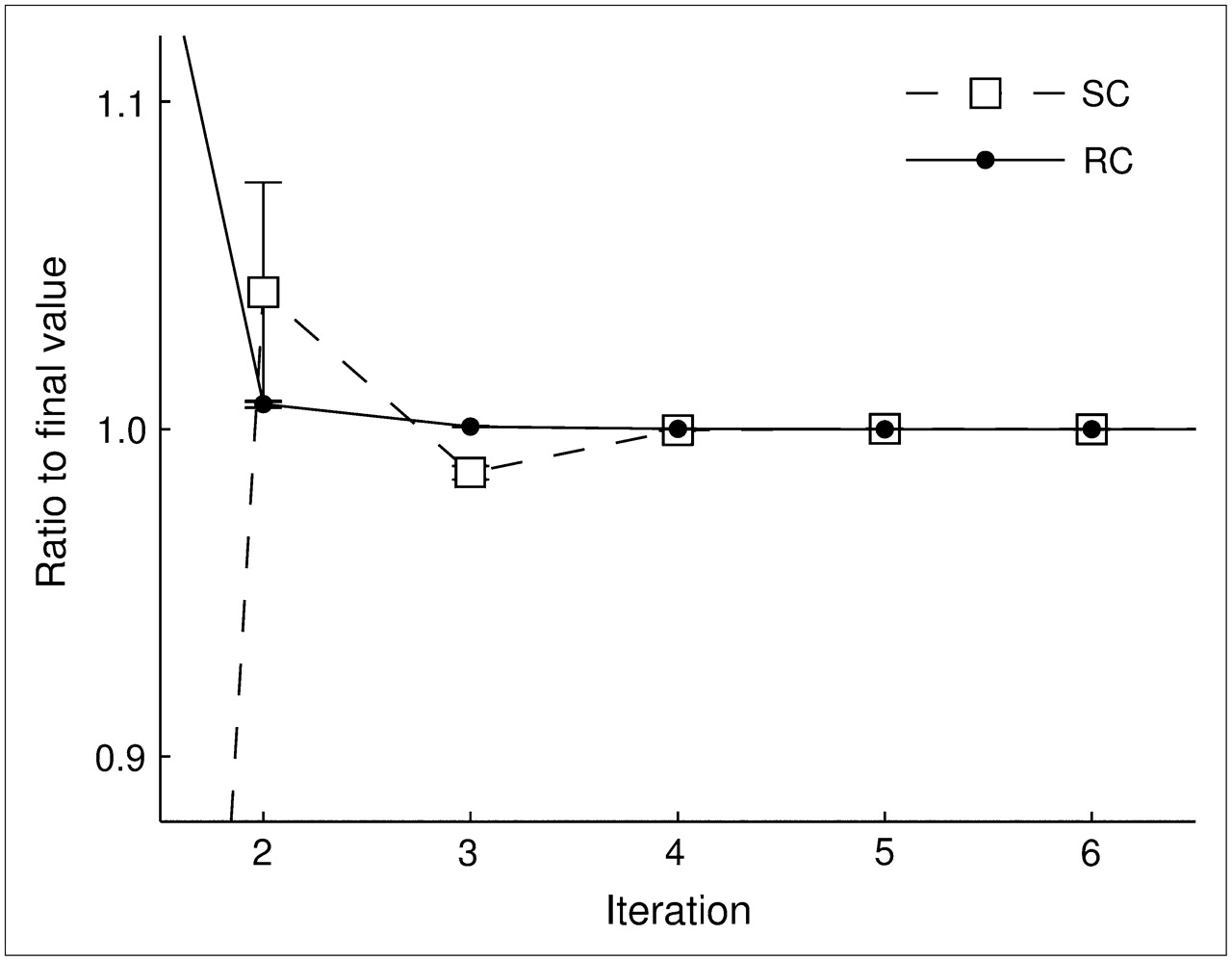
Convergence of iterative algorithm (Fig. 1) for model parameters RC and SC. Plot was generated for blood-pool ROIs in LH. Error bars are ±1 × SE.
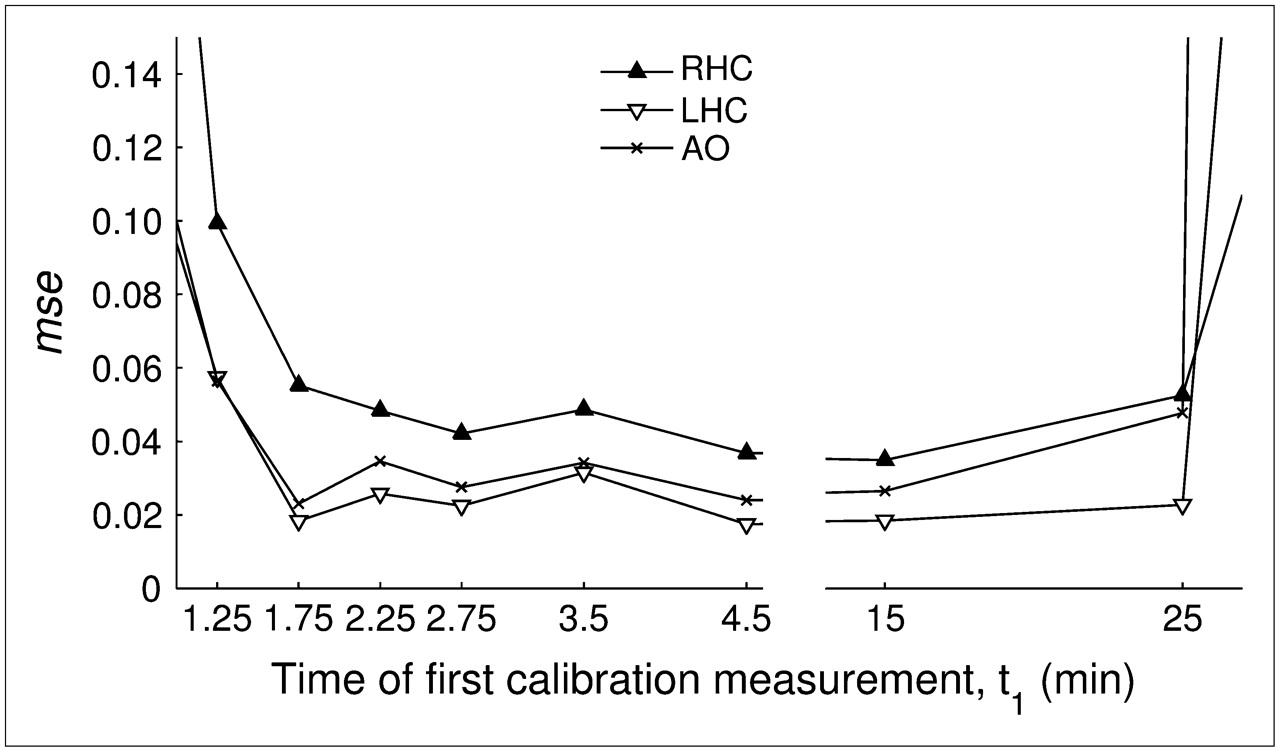
mse between model-adjusted input function and manually sampled input function as function of time point of first calibration measurement, t1. Plot shows results for blood-pool ROIs in RH and LH cavities (RHC and LHC, respectively) and descending aorta (AO). Values are out of scale for t1 = 0.25 min, t1 = 0.75 min, and t1 > 25 min (not shown).
Volume of Blood-Pool ROIs and Estimates of Model Parameters RC and SC
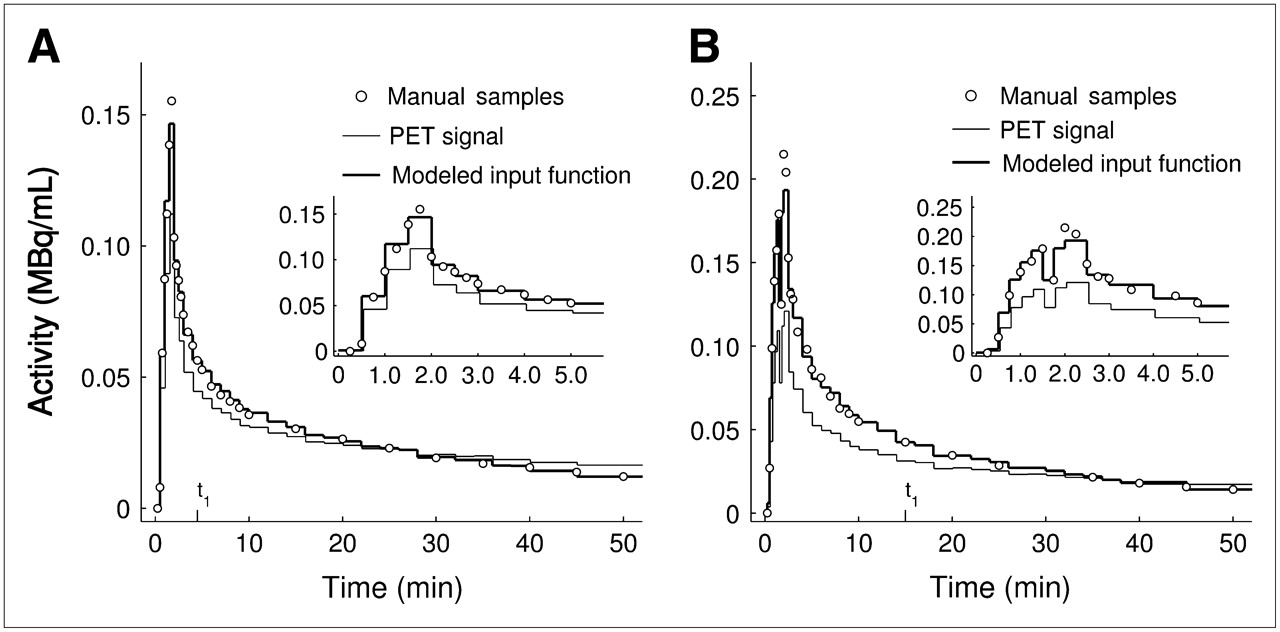
The raw PET signal from the blood-pool ROIs systematically underestimated the manually sampled input function during the early phase and overestimated it during the late phase (Fig. 6A). In contrast, the model-adjusted input functions provided excellent agreement with the manually sampled data for most time points, although during the peak phase (t < 2 min) manual blood samples differed slightly from the model-adjusted input function (insets of Fig. 6). Similar results were obtained for experimental data with prolonged tracer injections and higher framing rates during the early phase (Fig. 6B).
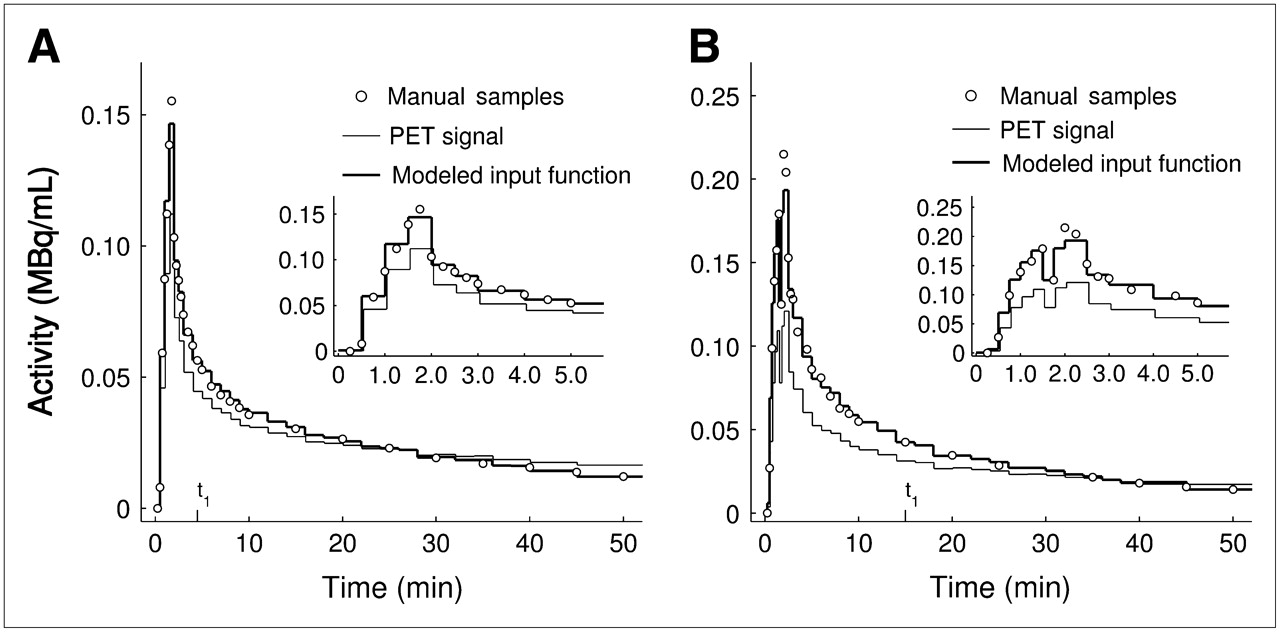
Comparison of activity in manual blood samples of pulmonary artery plasma, raw PET signal from blood-pool ROI in LH cavities, and model-adjusted input function: example of calibration measurements at t1 = 4.5 min and t2 = 50 min (A); example of longer tracer injection time (90 s instead of 1 min) and shorter initial PET frames (15 s instead of 30 s), with t1 = 15 min and t2 = 50 min (B). Discontinuity during peak was due to delay between end of tracer injection and flush of saline used to remove remaining tracer from infusion system.
When raw PET signals from the blood-pool ROIs were used as input functions, Patlak Ki values were systematically underestimated, compared with those calculated with the manually sampled input functions (Fig. 7A; Table 2). This bias was particularly pronounced in lungs with high values of Ki (Fig. 7B). In contrast, with model-adjusted input functions, Ki values were highly correlated with those obtained with manual blood sampling (Table 2; Fig. 7C), without any bias between the 2 methods (Fig. 7D).
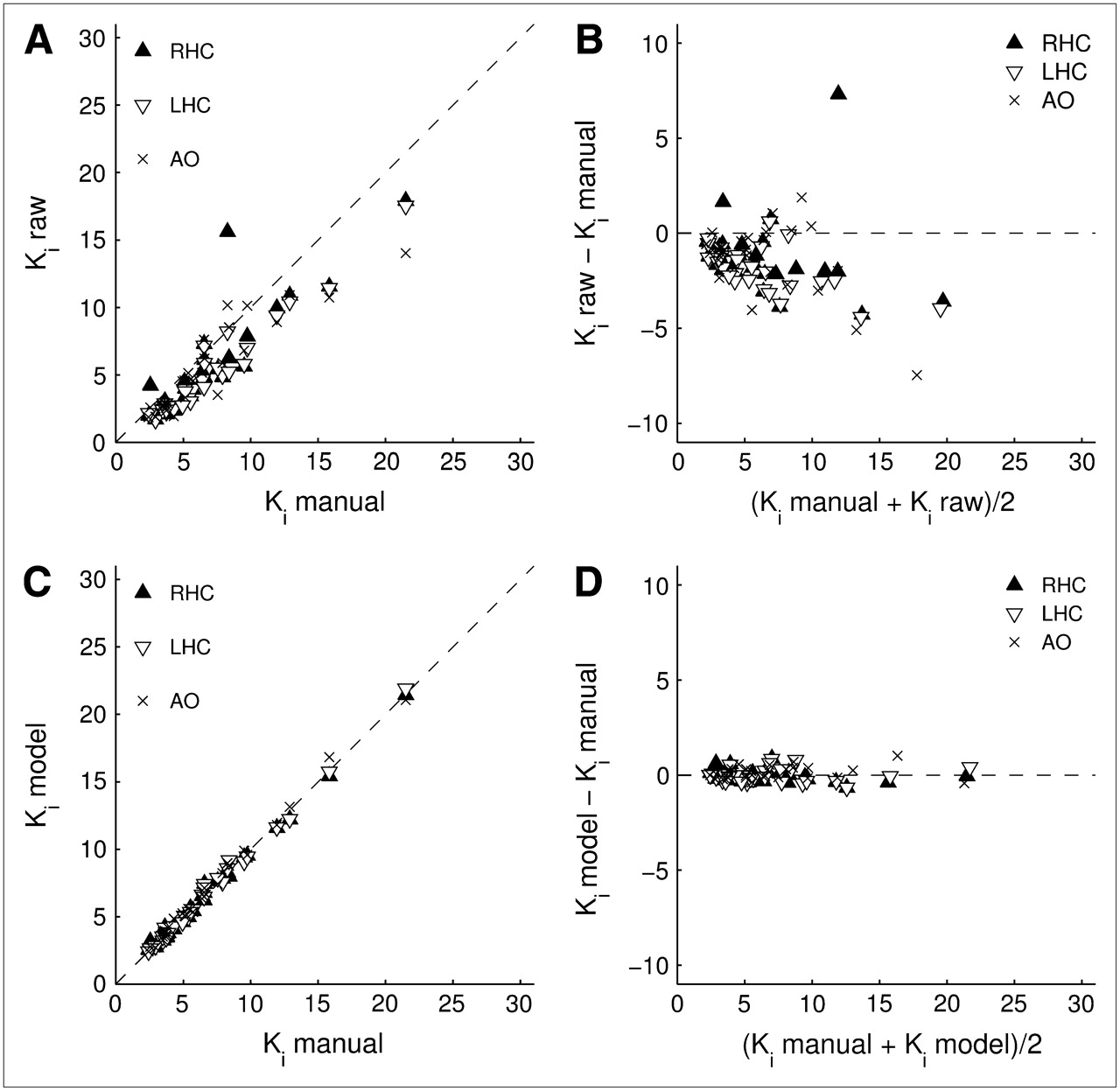
Evaluation of 18F-FDG uptake rates (Ki) for raw image–derived input functions and for model-adjusted input functions in comparison to Ki values obtained with manual blood sampling. Ki values include exposed and nonexposed lungs and were obtained with input functions from blood-pool ROIs in RH cavities (RHC), LH cavities (LHC), and aorta (AO). Shown are Ki obtained with raw image–derived input functions (A) and corresponding Bland–Altman plot (B), and Ki values calculated with model-adjusted input functions (C) and corresponding Bland–Altman plot (D). All values are in 10−3 mL blood/mL lung/min. Parameters of linear regression analysis are summarized in Table 2.
Regression Analysis of 18F-FDG Uptake Rates (Ki) for Model-Adjusted Input Functions and for Raw Image–Derived Input Functions in Comparison to Manual Blood Sampling (Figs. 7A and 7C)
DISCUSSION
We have presented here a model-adjusted input function that, requiring only 2 calibration blood samples, agrees very well with the manually sampled pulmonary artery input function and leads to unbiased estimates of 18F-FDG uptake in the normal and inflamed lung. The method is rather insensitive to the collection time of the first calibration sample, which can be chosen to be between 3.5 and 25 min after the start of tracer injection when a second calibration sample is taken at 50 min from injection. More important, the approach performs well with blood-pool ROIs affected by activity spillover or partial volume, without requiring a priori knowledge of a population-based input function or of the exact ROI anatomy.
Our basic model assumption was that the instantaneous calibration factor (CROI(t)/Cp(t)) could be described by the simple linear function in Equation 2 to adjust the PET ROI data for spillover and partial-volume artifacts. This assumption is clearly supported by the linearity of the plot between the CROI/Cp and the normalized integral of Cp obtained from the experimental PET and blood sampling data (Fig. 3A). In that plot, the y-axis intercept corresponds to an RC and the slope of the function to an SC. SC is a function of the 18F-FDG uptake rate in surrounding tissue, and like RC, is also a function of ROI geometry and the spatial resolution of the imaging instrument, which our algorithm automatically adjusts for each individual ROI. The geometric effects on SC are demonstrated by its dependence on blood ROI volume (Fig. 3B), where SC became larger for the LH cavities than for the aorta at increasing ROI volume as more activity from the myocardium was included in the LH-cavity mask. Furthermore, if the factor (1 − RC) is taken as a rough estimate of the geometric and spatial resolution effects on SC, normalizing SC by this factor would approximate the 18F-FDG uptake rate in surrounding tissues. SC/(1 − RC) was relatively independent of ROI volume and substantially larger (and more variable) for the LH cavities, compared with that of the aorta (Fig. 3C). This finding is consistent with the expectation of higher 18F-FDG uptake in the myocardium than surrounding the aorta. Therefore, if ROI design is aimed at minimizing the amount of tissue in the blood-pool ROIs, Equation 2 seems to be a robust and practical approach to adjusting the time–activity curve from the blood-pool ROIs for partial-volume and spillover effects.
A second model assumption was that the concentrations of 18F-FDG in whole blood and plasma were in equilibrium. This assumption seems justifiable given that 18F-FDG equilibrates almost instantaneously between plasma and erythrocytes (23), as supported by the fact that the model-adjusted input function agreed well with manually sampled blood plasma activity during the first few minutes after injection.
Our approach involves 2 user inputs in the computation of the input function. One is the delineation of the blood-pool ROIs, and another the selection of time points for withdrawing calibration blood samples. The method presented here was found rather insensitive to both of these steps. ROI delineation can be a subjective process, requiring individual adjustment of threshold values and manual editing to account for imaging artifacts. However, because the model parameters were automatically adjusted for an ROI, it was sufficient to define a rough outline of the ROI without precise knowledge of myocardium or vessel anatomy. Indeed, when we generated model-adjusted input functions for ROIs of different sizes to calculate Ki values in smoke-exposed and control lungs, these values changed by less than 0.5% despite a 5-fold difference in defined ROI volumes. Our results also suggest that for Patlak analysis, any of the 3 blood-pool ROIs studied could be used with our model-adjusted input function. However, for estimating individual rate constants of a more complex compartmental model, such as that of Sokoloff et al. (24), defining ROIs over the LH cavities or aorta could be preferable given the lower mse values they yield, compared with the ROI over the RH cavities. This is advantageous because defining the LH cavities and aorta does not require a 13NN-saline injection.
The second user input in calculating the model-adjusted input function is the timing of the calibration measurements. There are 2 competing effects for this timing. To maximize the robustness of linear regression in Equation 3, one should choose t1 and t2 to be as far apart as possible. On the other hand, the closer t1 is to the time of tracer bolus injection, the greater is the chance of measurement artifacts during the manual blood sampling because of the rapid tracer kinetics taking place. Because the mse between manually sampled and model-adjusted input functions was relatively constant for a wide range of initial calibration sample timings (t1), it is feasible to choose the first calibration sample over a wide range of times without substantially affecting the robustness of the model-adjusted input function. This feasibility was also demonstrated for a study with a modified tracer injection rate, where the variation in peak tracer activity was particularly high because of a delay between the end of tracer injection and the start of a flush removing remaining tracer from the injection system.
Although the use of the model-adjusted input function reduces the total number of blood samples, sampling of mixed venous blood is still involved. It is reasonable to expect that for large values of t1, plasma activity in the peripheral veins could sufficiently approximate plasma activity in mixed venous blood. Future studies are needed to validate the use of peripheral venous blood in combination with our model.
For compartmental modeling of 18F-FDG kinetics in pulmonary inflammatory states, an accurate estimate of the early-phase input function is desirable. Previously published techniques (11,13,15,18,19,25) may be limited for this purpose. For instance, in the presence of significant myocardial 18F-FDG uptake, the uncorrected image signal from an ROI in the LH was found to substantially differ from the manually sampled input function during the early phase, and the tumor metabolic rate of glucose was underestimated by as much as 12% with this raw image–derived input function (18). In accordance with our analysis, those errors could explain the substantial bias in Ki when an unadjusted PET signal from a blood-pool ROI is used as the input function.
Takikawa et al. (13) calculated a population-based input function by averaging manually sampled input functions that were obtained in a particular population. The disadvantage of this approach is that the individual input function of a subject may be very different from the population-based input function, and it is unclear if population-based input functions can be used to accurately estimate parameters reflecting early-phase tracer kinetics.
Another method used to estimate the plasma time–activity curve described clearance of 18F-FDG from the blood by a sum of 3 decaying exponential functions that have to be known a priori for a specific population (11). However, this method fails to account for early-phase tracer kinetics. Yet another method has derived the arterial input function from an ROI over the descending aorta, by assuming a signal free from activity spillover (15). This freedom from spillover cannot be guaranteed in the case of increased uptake in lung regions, as encountered during acute lung inflammation (2–4,6). In fact, we found that the SC for the aorta was on average as large as that of the other 2 ROIs. Other elegant methods to estimate an image-derived input function require a priori assumptions (17) or measurements (16) of myocardial anatomy and are restricted to ROIs within the left ventricle. Our method circumvents these requirements, although it involves the withdrawal of 2 calibration blood samples. For applications in brain, Naganawa et al. (25) developed a method that extracts the input function by independent-component analysis based on the fact that cerebral blood volume is very small (2%–4%) and that there is only a small fraction of voxels (1%–2%) with a substantial blood content. These conditions are clearly not met in the lung, where blood volume can be as much as 20% of a voxel (7).
CONCLUSION
Our model-adjusted method to estimate a PET-derived input function allows accurate reconstruction of the time–activity curve in pulmonary artery blood for modeling pulmonary uptake of centrally injected 18F-FDG. This method requires only 2 blood samples, the first of which can be taken as late as 25 min, with the second sample taken 50 min after tracer injection. Delineation of the blood-pool ROI is less critical than in other techniques, because the model implicitly adjusts the data for partial-volume and activity spillover effects. This approach is expected to substantially facilitate studies involving compartmental modeling of 18F-FDG kinetics of the inflamed lung, possibly also including patients with viral or bacterial infections, pulmonary fibrosis, and chronic obstructive pulmonary disease.
Acknowledgments
This work was funded by NIH grants RO1-HL-086827, HL-056879, HL-068011, and HL-076464. One of the authors was supported in part by the German Academic Exchange Service (DAAD) and by Roland Ernst Stiftung.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 26, 2007.
- Accepted for publication July 30, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- High-Temporal-Resolution Kinetic Modeling of Lung Tumors with Dual-Blood Input Function Using Total-Body Dynamic PET
- Total-Body Multiparametric PET Quantification of 18F-FDG Delivery and Metabolism in the Study of Coronavirus Disease 2019 Recovery
- High-Temporal-Resolution Lung Kinetic Modeling Using Total-Body Dynamic PET with Time-Delay and Dispersion Corrections
- Measurement of PET Quantitative Bias In Vivo
- Quantification of Lung PET Images: Challenges and Opportunities
- Reply: 18F-FDG Uptake to Assess Eosinophilic Inflammation in Asthma: Would SUV at Late Imaging Be Relevant?
- 18F-FDG Uptake Rate Is a Biomarker of Eosinophilic Inflammation and Airway Response in Asthma