


Abstract
Conventional work-up (CWU) with chest radiography, abdominal ultrasonography, and skeletal scintigraphy has limited value in M staging of nonkeratinizing nasopharyngeal carcinoma (NPC). Our aim was to evaluate whether 18F-FDG PET could replace CWU by comparing their diagnostic efficacies. Methods: Patients with histologically proven nonkeratinizing NPC and no prior treatment were prospectively enrolled. All study participants underwent CWU and 18F-FDG PET for primary M staging. Distant metastasis was considered to be present if there was any reliable evidence identified within 1 y after diagnosis. The comparative diagnostic efficacies of 18F-FDG PET, CWU, and the combination of 18F-FDG PET and CWU (PET+CWU) were evaluated using the areas under the receiver-operating-characteristic (ROC) curves. Results: Sixty-one (20.3%) of 300 eligible patients were found to have distant metastases. On a patient-based analysis, 18F-FDG PET was found to be more effective than CWU (P < 0.001), whereas it was equally effective with PET+CWU (P = 0.130). On region-based analyses, 18F-FDG PET was more effective than skeletal scintigraphy and chest radiography for detecting bone metastases (P < 0.001) and chest metastases (P < 0.001), respectively. 18F-FDG PET and abdominal ultrasound were equally effective for detecting hepatic metastases (P = 0.127). On region-based analyses, the combination of 18F-FDG PET and CWU did not yield any noticeable increase in diagnostic efficacy. Conclusion: 18F-FDG PET can replace CWU in primary M staging of nonkeratinizing NPC.
Nonkeratinizing nasopharyngeal carcinoma (NPC), with a World Health Organization (WHO) histologic classification of type II (differentiated nonkeratinizing carcinoma) or type III (undifferentiated carcinoma), is an epithelial malignancy distinct from squamous cell carcinomas of the head and neck (1). It is etiologically associated with the Epstein–Barr virus and endemic in southern China, Southeast Asia, the Middle East, North and East Africa, Greenland, and Alaska (2). Early locoregional spread is a well-known characteristic of nonkeratinizing NPC, and a higher incidence of distant metastasis has been found in this tumor compared with other head and neck cancers (3). Conventional work-up (CWU) with chest radiography, abdominal ultrasonography, and skeletal scintigraphy is routinely performed for detecting distant metastases (4). On the other hand, CT of the thorax is not generally recommended because of its very low yield (5). Although widely available and affordable, these techniques have important limitations (6). Chest radiography is insensitive in detecting mediastinal and hilar lymphadenopathies because of structure overlapping and inadequate soft-tissue contrast. Ultrasonography can visualize superficial hepatic structures well; however, this technique is relatively operator-dependent and has inherent problems in differentiating between benign and metastatic tumors (7). Finally, skeletal scintigraphy appears to be insensitive for detecting early bone or bone marrow metastasis (8). With the development of newer imaging modalities and instrumentation, distant metastases could be detected earlier. This would have a considerable impact on patient staging and stratification, thereby permitting the development of more reliable treatment protocols. As nonkeratinizing NPC is a chemosensitive and radiosensitive tumor and a minority of patients with overt distant metastases can obtain long-term survival (9), it may be possible that identification of early distant metastasis can improve survival in this patient group by early utilization of proper treatment.
18F-FDG PET is capable of imaging tumors with high glucose metabolism. This method is useful for staging in many types of cancer by detecting unsuspected distant metastases. 18F-FDG PET has been proven to be more sensitive than skeletal scintigraphy for detecting bone metastases in primary staging of NPC patients (10). However, it remains to be elucidated whether 18F-FDG PET plays a complementary role or can replace CWU for primary NPC staging. To address this issue, we compared the diagnostic efficacies of 18F-FDG PET, CWU, and their combination in the present study. We also evaluated the frequency and distribution patterns of distant metastases in these patients.
MATERIALS AND METHODS
Patients
Patients with histologically proven nonkeratinizing NPC and no prior treatment were prospectively enrolled. The study was approved by our Institutional Review Board, and all participants provided written informed consent. Patients with a history of previous or synchronous second malignancy, tumor histology other than WHO type II or type III, or insufficient follow-up data were excluded.
CWU for detecting distant metastases consisted of chest radiography, abdominal ultrasonography, and whole-body skeletal scintigraphy. MRI of the head and neck was performed for locoregional staging. These studies, along with 18F-FDG PET, were performed within 2 wk after the patient enrollment.
The T and N staging for each patient, according to the American Joint Committee on Cancer (AJCC) TNM staging system published in 2002, was determined by combining clinical information, imaging findings, and biopsy or aspiration results. Patients with suggestive distant metastases on CWU or 18F-FDG PET received additional studies, including CT, MRI, or biopsy or aspiration at the sites in question. If the presence of distant metastases could not be confirmed by additional studies, the patients were considered to have locoregional disease only. After primary staging, patients without proven distant metastases were treated with concurrent chemoradiotherapy or radiotherapy. Radiotherapy was used primarily for patients with AJCC stage I disease or severe comorbid conditions. Systemic chemotherapy was initiated if the presence of distant metastasis had been confirmed. In the presence of a good response to chemotherapy, further treatment with curative intent would be considered. The first imaging follow-up, including head and neck MRI and 18F-FDG PET, was scheduled at 3 mo after completion of radiotherapy or 1 mo after completion of chemotherapy. Patients without evidence of residual disease were monitored at 3-mo intervals for the first 2 y and every 6 mo thereafter. Patients with suspected residual disease, recurrence, or metastasis would receive further imaging studies and histologic examination. If recurrent malignancy was proven, further chemotherapy, radiotherapy, surgery, or combined-modality treatment was suggested according to each individual clinical condition.
Conventional Work-up for Distant Metastasis
Chest radiography was performed according to the institutional standard protocol and interpreted by the attending radiologist. Abdominal ultrasonography was performed and interpreted by the attending physician, with the liver as the primary target. Skeletal scintigraphy was performed using a dual-head γ-camera (Dual Genesys; ADAC Laboratories) equipped with general-purpose collimators. Anterior and posterior whole-body images were acquired 3−4 h after intravenous administration of 925 MBq 99mTc-labeled methylene diphosphonate.
18F-FDG PET
All patients fasted for at least 6 h before the examination and received intravenous injections of 370 MBq ± 10% 18F-FDG after initial preparation. An ECAT EXACT HR+ PET scanner (Siemens Medical Solutions USA, Inc.) was used for image acquisition. Early-phase PET acquisition from the vertex to the upper thighs was started 40 min after injection. Delayed-phase PET was acquired at about 3 h after injection. Transmission scans using the 68Ge rod source were obtained for attenuation correction. The accelerated maximum-likelihood algorithm with ordered-subset expectation maximization was applied for image reconstruction. The maximal standardized uptake values (SUVmax) of the lesions obtained in both early and delayed images were available to interpreters.
Image Interpretation
A 3-point scoring system for distant metastasis was used: 0 = negative (normal or benign), 1 = equivocal, and 2 = positive. For chest radiography and abdominal ultrasonography, the scoring was assigned by the attending radiologist or physician who was unaware of the 18F-FDG PET results. For skeletal scintigraphy and 18F-FDG PET, 3 nuclear medicine staff physicians independently interpreted the scans while unaware of the patients' clinical findings. The final scoring was the value given by 2 or more interpreters. For combined interpretation of 18F-FDG PET and CWU, the maximal score was used.
Determination of Presence of Distant Metastasis
Distant metastasis was considered to be present if one or more of the following conditions were met within 1 y from primary diagnosis: (a) histologic proof of distant metastasis, (b) unequivocal evidence of distant metastases in the imaging studies, with a concordant clinical course, (c) equivocal evidence of distant metastases in the imaging studies, with subsequent histologic proof or clinical progression. Sites of distant metastases were grouped into 4 regions: skeleton, thorax, liver, and others. The thorax includes mediastinum, pulmonary hilum, lung, and pleura.
Impact of 18F-FDG PET on Patient Management
The impact of 18F-FDG PET on patient management was defined as the proportion of patients who were truly upstaged or downstaged by 18F-FDG PET. Because further confirmatory studies were necessary before a correct choice of the therapeutic protocols, the management of patients with false upstaging or downstaging by 18F-FDG PET was considered to be unaffected.
Statistical Analysis
The multiple logistic regression model was applied to compare the characteristics between patients with single-region and multiple-region metastases. The diagnostic efficacies of 18F-FDG PET, CWU and the combination of 18F-FDG PET and CWU (PET+CWU) were evaluated and compared using the receiver-operating-characteristic (ROC) curves, both for patient-based and region-based analyses. Areas under the empiric ROC curves (AUCs) were estimated nonparametrically and compared using the method of Hanley and McNeil (11). P values < 0.05 were considered statistically significant. The sensitivity, specificity, and accuracy were calculated by considering equivocal findings as negative. All calculations were performed with the SPSS (version 13.0; SPSS Inc.) and MedCalc (version 7.6.0; MedCalc Software) statistical software packages.
RESULTS
Patient Demographics
One patient with concurrent hepatoma, 4 patients with tumor histology other than WHO type II or type III, and 10 patients who were lost at follow-up were excluded. Three hundred patients who were diagnosed between April 2002 and August 2005 were deemed to be eligible for the present study. Baseline characteristics of the study participants are presented in Table 1. The mean age at diagnosis was 50.0 y, and the male-to-female ratio was 2.33:1. The percentages of patients assigned to N0, N1, N2, and N3 stages were 10.7%, 22.7%, 40.3%, and 26.3%, respectively.
Baseline Characteristics of 300 Patients at Primary Diagnosis
Frequency and Distribution Patterns of Distant Metastases
Frequency and distribution patterns of distant metastases are presented in Tables 2 and 3. Sixty-one patients (20.3%) were found to have distant metastases, including 48 (16.0%) with skeletal metastases, 27 (9.0%) with chest metastases, 23 (7.7%) with hepatic metastases, and 15 (5.0%) with metastases involving other sites. Twenty-nine patients had metastases at 2 or more regions. In patients with single-region metastases, regions where metastases were detected were skeleton (22 cases), chest (9 cases), and liver (1 case). The differences in baseline characteristics between patients with single-region and multiple-region metastases are presented in Table 4. Patients with multiple-region metastases had more advanced N stage than those with single-region metastases with a borderline statistical significance (P = 0.095).
Number of Patients by Metastatic Regions and by Scoring of 18F-FDG PET and CWU
Frequency of DM by Number of Metastatic Regions
Comparison Between Patients with Single-Region and Multiple-Region DM
Impact of 18F-FDG PET on Patient Management
18F-FDG PET had an impact on the management of 39 (13%) patients. Specifically, 31 patients were truly upstaged and 8 were truly downstaged. Seven patients were falsely upstaged and 1 patient was falsely downstaged by 18F-FDG PET. Because additional studies did not confirm the findings of 18F-FDG PET in these patients, their management was considered to be unaffected.
Diagnostic Efficacies of 18F-FDG PET, CWU, and Their Combination
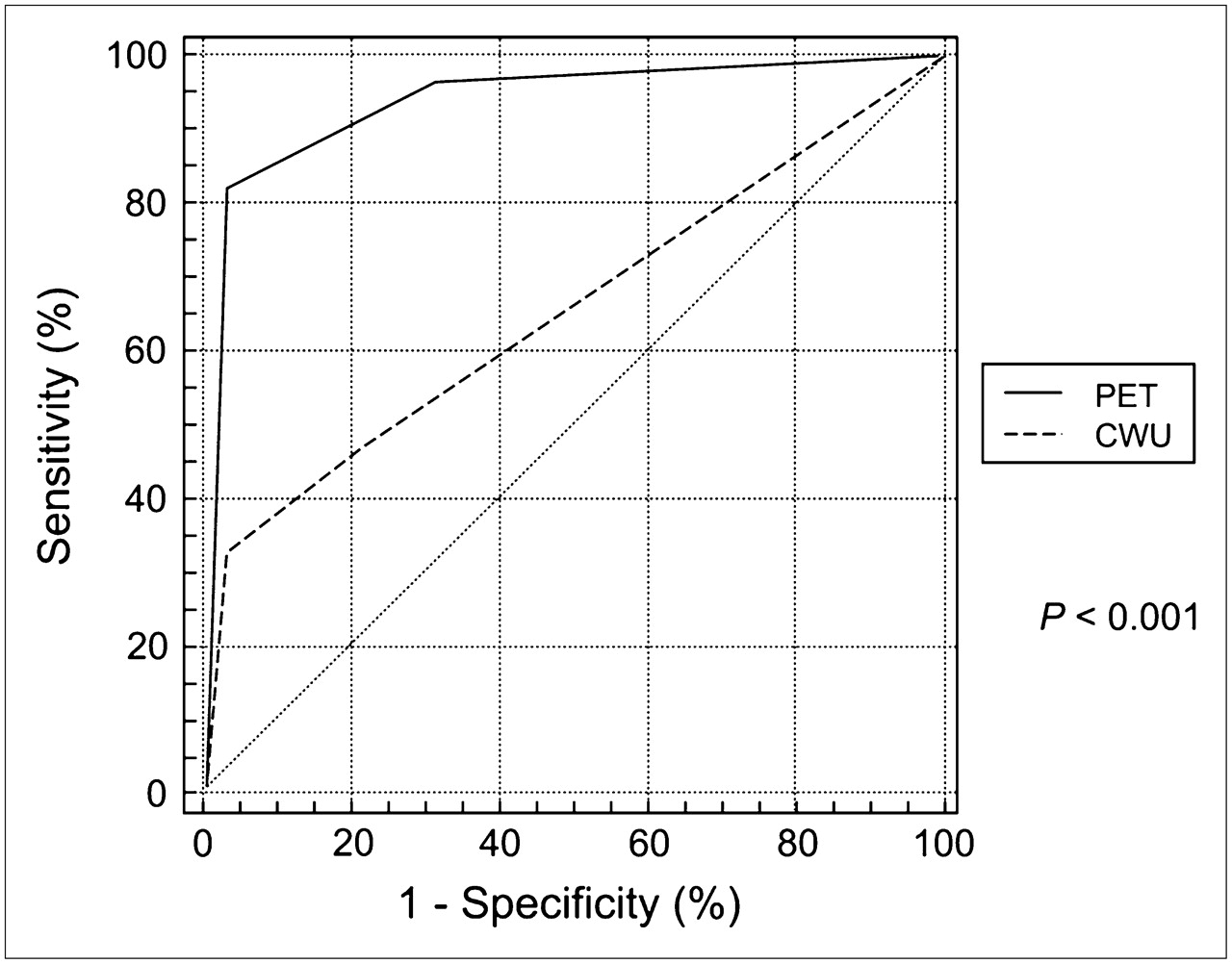
The numbers of patients with different scoring of 18F-FDG PET and CWU are presented in Table 2. Diagnostic efficacies of 18F-FDG PET, CWU, and PET+CWU are shown in Table 5. AUC values in both patient-based and region-based analyses are provided, along with sensitivity, specificity, and accuracy. On a patient-based analysis, 18F-FDG PET was found to be more effective than CWU (P < 0.001; Fig. 1), whereas it was equally effective with PET+CWU (P = 0.130; Fig. 2). Among patients with distant metastases (n = 61), 50 patients (82.0%) were detected by 18F-FDG PET and 20 patients (32.8%) were detected by CWU. PET+CWU yielded a slightly higher sensitivity (83.6%), at the cost of specificity and accuracy. In region-based analyses, 18F-FDG PET was significantly better than skeletal scintigraphy and chest radiography for detection of bone metastases (P < 0.001) and chest metastases (P < 0.001), respectively. Two patients with negative CWU and positive 18F-FDG PET findings are presented (Figs. 3 and 4). 18F-FDG PET and abdominal ultrasound were equally effective for detecting hepatic metastases (P = 0.127). PET+CWU did not yield higher AUC values in both patient-based and region-based analyses.

Patient-based comparison of ROC curves for 18F-FDG PET and CWU in primary M staging of NPC patients.

Patient-based comparison of ROC curves for 18F-FDG PET and PET+CWU in primary M staging of NPC patients.

A 69-y-old woman who was a patient with NPC of stage T2 N3. (A) Skeletal scintigraphy revealed no evidence of bone metastasis. (B) Maximum-intensity-projection image of 18F-FDG PET revealed multiple metastases in skeletal system. Patient died of disease 11 mo later.

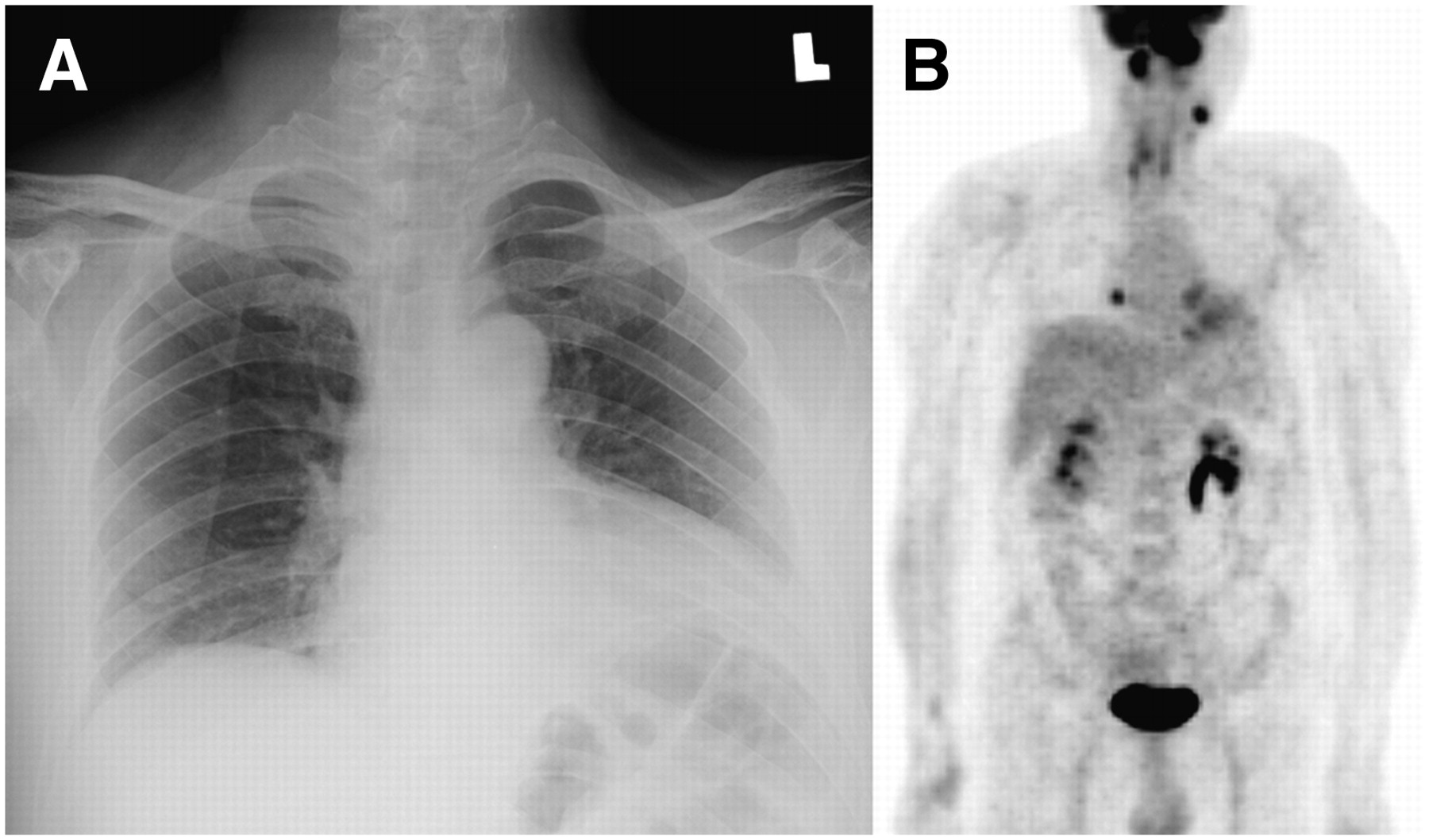
A 49-y-old man who was a patient with NPC of stage T4 N2. (A) Chest radiography revealed no evidence of chest metastasis. (B) Maximum-intensity-projection image of 18F-FDG PET revealed focal metastasis in right lower chest. CT-guided biopsy of 0.8-cm nodule in right lower lung confirmed it to be a metastatic tumor.
Diagnostic Efficacies, Sensitivities, Specificities, and Accuracies of 18F-FDG PET, CWU, and Their Combination
DISCUSSION
The presence of distant metastases is the most important predictor of patient survival in most cancers. As the majority of nonkeratinizing NPC patients (89.3% in the current study) are N-positive at presentation and the presence of distant metastases is strongly associated with the N stage (10), a substantial proportion of patients are expected to have distant metastases. At primary staging, overt distant metastases have been detected in up to 11% of patients by means of conventional studies, whereas subclinical metastases that remained initially undetected may become apparent shortly thereafter (12,13). In a study by Micheau et al., about 40% of nonkeratinizing NPC patients with advanced N-stage disease (N2 or N3) had tumor invasion in the bone marrow as demonstrated by transiliac biopsy (14). As 18F-FDG PET was more sensitive than skeletal scintigraphy for detecting bone metastases, we asked whether 18F-FDG PET could replace CWU for primary M staging in nonkeratinizing NPC patients. To the best of our knowledge, our study represents the first large-scale evaluation of the diagnostic efficacies of 18F-FDG PET, CWU, and their combination in this patient group.
Major sites of metastatic disease were, in descending order of frequency, the skeleton, the thorax, and the liver. These findings are in keeping with those of Sham et al. (15) and Teo et al. (16), who previously analyzed large cohorts of NPC patients in Hong Kong. In our study, clinical or subclinical distant metastases at presentation were found in about 20% of the study participants. Half of them had 2 or more regions of involvement by metastases. This phenomenon is probably due to the delay in medical consultation and diagnosis that typically occurs in NPC patients. Patients with early-stage NPC usually present with nonspecific symptoms and often remain undiagnosed until the occurrence of metastatic neck lymphadenopathies. Additionally, the incidence of distant metastases increased strikingly from 14% in N2 patients to 48% in N3 patients. This implies that significantly improved survival may be achieved if NPC patients could be diagnosed before the N3 stage.
On a patient-based analysis, the diagnostic efficacy of 18F-FDG PET was proven to be significantly better than that of CWU for primary M staging. On region-based analyses, 18F-FDG PET was superior to CWU for both the skeleton and the chest. In contrast, the superiority of 18F-FDG PET over abdominal ultrasonography for detecting hepatic metastases was not statistically significant. This phenomenon may be due to the small number of patients with hepatic metastases (n = 23). However, this issue is likely to be of scarce clinical relevance because of the rare incidence of distant metastasis confined only to the liver in patients with nonkeratinizing NPC (only 1 case in the current study). In our experience, the sensitivity of 18F-FDG PET for detecting hepatic metastasis was associated primarily with the lesion size. Small-sized lesions may be easily missed because of both the partial-volume effect and the blurring effect introduced by respiration.
The diagnostic efficacies of combined 18F-FDG PET and CWU were not superior compared with those of 18F-FDG PET alone, both in patient-based and region-based analyses. Although the sensitivity of combined 18F-FDG PET and CWU may be slightly higher, the diagnostic efficacy, specificity, and accuracy were reduced. Several different methods for combining the results of 18F-FDG PET and CWU have been exploited, but the method used in our current study had the best performance.
Ideally, chest radiography and abdominal ultrasonography should be interpreted by independent readers in the same way as 18F-FDG PET and skeletal scintigraphy. However, we were unable to do so because of limited financial resources. In addition, we are confident that both chest radiography and abdominal ultrasonography are well-established procedures. Thus, it is posited that interpretation by the attending radiologist or physician could reflect the “real-world” diagnostic efficacy in routine clinical practice. 18F-FDG PET required multireader interpretation inasmuch as it is a newer imaging modality with probably more significant interobserver variability due to lack of experience. Skeletal scintigraphy was interpreted in the same manner as 18F-FDG PET because the same interpreters evaluated both studies.
The diagnostic efficacies of different imaging studies were evaluated by using ROC curve analysis. This methodology is different from other methods requiring a binary-mode interpretation. Equivocal lesions were defined as abnormalities that could not be classified confidently as benign or malignant. Classification of such lesions as either benign or malignant may result in a single pair of sensitivity and specificity but is generally considered not sufficient for describing the diagnostic performance of a test (17). It should be also noted that ROC curves were constructed without application of any smoothing technique in our study.
NPC patients with subclinical metastases might be currently considered as having M0 disease. These subjects may be treated by radiotherapy, either with or without chemotherapy. Recent meta-analyses suggested that the addition of concomitant chemotherapy to radiotherapy can result in an absolute survival benefit for patients with locoregionally advanced NPC (18). We proposed the possibility that some of these patients had undetected subclinical metastases, and addition of concurrent chemotherapy might be beneficial in these patients. Thus, early identification of distant metastases may improve patient stratification as well as the pursuit of optimal clinical management. Patients with early distant metastases may benefit from more aggressive treatment. Notably, some of these patients can be identified by 18F-FDG PET. Radiotherapy combined with a higher dose of concurrent chemotherapy, neoadjuvant chemotherapy, targeted therapy, or other novel treatment modalities may be of value (18,19). A clinical trial to investigate whether more aggressive treatment may improve survival in this patient group is suggested. On the other hand, radiotherapy with a lower dose of concurrent chemotherapy could be considered for patients at low risk of distant metastasis to decrease the toxicity profile. The optimal therapeutic protocols must be investigated in future studies, and 18F-FDG PET may serve as a more reliable means for disease staging and treatment monitoring.
This study evaluated the diagnostic efficacy of 18F-FDG PET. However, it is posited that dual-modality PET/CT will fully replace single-modality PET in cancer imaging. In this regard, PET/CT can provide additional anatomic information and has been found to be superior to PET alone (20). It is reasonable to hypothesize that our findings may be inferred in the application of 18F-FDG PET/CT in primary M staging of nonkeratinizing NPC.
CONCLUSION
Our current study confirmed the superiority of 18F-FDG PET over CWU in primary M staging of nonkeratinizing NPC patients. On the other hand, diagnostic efficacy did not improve with the combined use of these techniques. Thus, we conclude that 18F-FDG PET can replace conventional work-up in primary M staging of nonkeratinizing NPC.
Acknowledgments
We thank all members of the cross-disciplinary NPC team at our institution for their devotion and help. This work was supported by grants from the Chang Gung Memorial Hospital (CMRPG32034-32043) and Chang Gung University.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 7, 2007.
- Accepted for publication July 3, 2007.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prospective Study of Tailoring Whole-Body Dual-Modality [18F]Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography With Plasma Epstein-Barr Virus DNA for Detecting Distant Metastasis in Endemic Nasopharyngeal Carcinoma at Initial Staging
- Preliminary Study of 11C-Choline PET/CT for T Staging of Locally Advanced Nasopharyngeal Carcinoma: Comparison with 18F-FDG PET/CT
- Prolonged Remission in a Patient With Nasopharyngeal Carcinoma With a Solitary Bone Metastasis
- Randomized Phase II Trial of Concurrent Cisplatin-Radiotherapy With or Without Neoadjuvant Docetaxel and Cisplatin in Advanced Nasopharyngeal Carcinoma