


Abstract
Small pulmonary nodules with little or no perceptible 18F-FDG uptake are relatively common findings on combined PET/CT images of patients with nonthoracic malignancies. Interpreting such nodules is often a diagnostic challenge, and this study aimed to evaluate the clinical significance of the nodules. Methods: Patients with pulmonary nodules ≤1 cm in diameter showing no 18F-FDG uptake or uptake less than the mediastinal background were included. Nodules with clearly benign or metastatic findings on CT were excluded. One hundred twenty-one patients had either tissue confirmation or clinical follow-up with additional chest images. The subjects were studied by 3 variables: (i) solitary versus multiple nodules, (ii) presence of accompanying benign lung lesion versus absence, and (iii) imperceptible 18F-FDG uptake versus faint 18F-FDG uptake. The malignancy rates were calculated for each variable. Results: Of the 121 patients, 24 had malignancy, with a strong possibility of pulmonary metastasis (19.8%). Six of the 44 patients with solitary nodules (13.6%) and 18 of the 77 patients with multiple nodules (23.4%) had malignancies, though there was no statistically significant difference in the incidences of malignancy between the solitary and multiple groups. On the other hand, there was a statistically significant difference (P = 0.040) between the accompanying lung lesion present (8.3%) and absent (24.7%) groups. No statistically significant difference was noted between the 18F-FDG uptake imperceptible group and faint 18F-FDG uptake group (20.7% vs. 17.2%). Conclusion: For patients with incidental lung nodules of indeterminate nature with no 18F-FDG uptake or uptake less than that of the mediastinum on PET/CT images, >19% of the cases turned out to be malignant. The nodule was more likely to be malignant when no other benign pulmonary lesions could be identified elsewhere in the lung field. Thus, regardless of the number of nodules and 18F-FDG uptake, tissue confirmation or close imaging follow-up is necessary when small nodules with imperceptible or faint 18F-FDG activity are present on the PET/CT images, especially in the absence of accompanying benign lung lesions.
PET with 18F-FDG is widely used for the staging and restaging of various malignancies, such as lung cancer, esophageal cancer, colorectal cancer, lymphoma, melanoma, breast cancer, and head and neck cancers (1,2). As a typical scan inspects the body from head to pelvic floor, PET is especially useful for finding distant metastases in many cases of malignant tumors (3–8). In the last few years, combined PET/CT scanners have become very popular, and >400 scanners were installed worldwide (9). The addition of CT allows more accurate anatomic localization and provides the data necessary for attenuation correction of PET images (1,9). In addition to the regions of primary interest, various lesions are incidentally detected on the noncontrast CT portion of the PET/CT scans (10). One example is nodules 1 cm in diameter or smaller discovered on the CT images in the lung window setting with either faint 18F-FDG uptake or no perceptible 18F-FDG uptake on the corresponding PET images.
A lower accuracy of 18F-FDG PET for the smaller lung lesions is widely reported. Gould et al. stated that the true-negative rate of PET scans for small pulmonary lesions cannot be determined, as few data exist for nodules <1 cm in diameter (11), and Imdahl et al. did not believe that PET can serve as a gold standard for early detection of small lung tumors (12).
Characterization of small lung nodule on CT images is very difficult because detailed morphologic features often cannot be perceived. In a study by Li et al. on lung cancers missed on low-dose helical CT screening, the mean size of missed lung cancers due to detection error was 9.8 mm, and the mean size for those due to interpretation errors was 15.9 mm (13). To make the diagnosis even more difficult, numerous benign conditions can appear as nodules, such as granuloma, hamartoma, round pneumonia, round atelectasis, hematoma, and arteriovenous malformation (14–16). Furthermore, in areas with high prevalence of granulomatous diseases, higher false-positive rates could result in lower specificity of the imaging modality (17,18).
Among the malignancies of various nonthoracic organs, no routine lung CT image follow-up is done unless there is a high tendency for the primary tumor to develop lung metastases. Available plain chest radiographs most likely do not contribute to the characterization of such small nodules. Consequently, we were often faced with the problem of deciding what significance to accord the small pulmonary nodule with no or little 18F-FDG uptake discovered on PET/CT images obtained for the staging or restaging of other proven primary malignancy.
To our knowledge, no previous study has reported the overall malignancy rate of small pulmonary nodules discovered on the CT portion of the PET/CT scans of patients with extrathoracic malignancy. Thus, the first aim of this study was to determine the overall rate of metastases among small pulmonary nodules with little or no 18F-FDG uptake seen on the PET/CT scans obtained for the staging or restaging in patients with underlying nonthoracic malignancies. Second, we wanted to see if there were differences in the rates of metastases depending on 3 specific variables: the number of nodules, the presence of accompanying lung lesions, and the degree of 18F-FDG uptake by the nodule.
MATERIALS AND METHODS
Patient Population and Study Design
The population of this retrospective study consisted of patients with proven underlying nonthoracic malignancy who had whole-body PET/CT with 18F-FDG for initial staging or restaging from December 2003 to December 2005 (Table 1). The inclusion criteria were (a) one or more well-defined nodular density measuring ≤1 cm in diameter on the noncontrast CT images of the PET/CT, (b) a peak standardized uptake value (pSUV) lower than that of the mediastinum on the PET images, and (c) a newly developed nodule or no previous chest CT or PET/CT images available for comparison. A pulmonary nodule that demonstrated no change for a year or longer after the previous chest image was regarded as more likely to be benign and was excluded from the study. Cases that were strongly indicative of metastatic or benign findings were also excluded from the study. Findings such as dense calcification in the nodule, continuation with fibrosis band, and being part of a “tree-in-bud” appearance were believed to point toward a benign nature.
Specific Primary Tumor Sites of Patients Included in Study
The subjects were grouped according to 3 variables: the number of nodules, the presence or absence of accompanying benign lung lesion, and the degree of 18F-FDG uptake. (i) If only 1 nodule that satisfied the inclusion criteria was present, it was classified into the “solitary” group, and if ≥2 such nodules were seen, it was classified into the “multiple” group. (ii) The CT images were further examined for benign accompanying lung lesions independent of the nodule in question, such as inflammation or fibrocalcific scar in other parts of the lung field. The presence of any other benign lesion in the lungs was classified as the benign lesion “present” group and, if no other abnormal finding could be seen, the nodule in question was classified as an accompanying benign lung lesion “absent” group. (iii) From the PET images, the degree of 18F-FDG uptake in the corresponding area was checked. A nodule with 18F-FDG uptake that is perceptible but with the pSUV lower than that of the mediastinum was classified into the 18F-FDG uptake faintly “perceptible” group; if the pSUV was not higher than that of the surrounding normal lung parenchyma uptake and, thus, no 18F-FDG uptake could be observed, the nodule was classified into the “imperceptible” group.
The ethical committee of our institution does not require patient consent for retrospective review of imaging studies.
Imaging
All patients fasted for at least 6 h before the PET/CT study. An average amount of 550 MBq of 18F-FDG was injected intravenously, and scanning began 60 min later. None of the patients had blood glucose levels exceeding 130 mg/dL before the injection. No intravenous contrast agent was used. A combined PET/CT in-line system (Biograph LSO; Siemens Medical Solutions) was used to acquire all data. A full-ring PET scanner integrated with a dual-section helical CT scanner (Somatom Emotion; Siemens) acquired the coregistration of PET and CT images in one session. There were 6–8 bed positions, and the acquisition time was 2 min per bed position. All patients were in supine position with their arms raised. CT began at the orbitomeatal line and progressed to the upper thigh (30 mA·s; 130 kV; 5-mm slice thickness). PET followed immediately over the same body region. The CT data were used for attenuation correction, and images were reconstructed using a standard ordered-subset expectation maximization algorithm. The axial spatial resolution was 6.5 mm at the center of the field of view.
Interpretation
All PET/CT images were reviewed at a workstation with fusion software (Syngo; Siemens) that provided multiplanar reformatted images and displayed PET images either before or after attenuation correction, CT images, and PET/CT fusion images. The CT images were set in the lung window setting and closely searched for any nodular density by 2 physicians who were board certified in both nuclear medicine and radiology.
The nodule's diagnosis was verified by 2 methods. First, biopsy or surgery yielded tissue histology for 17 patients. Second, a series of consequent imaging studies were obtained during a clinical follow-up period of 1 y or longer: Enhanced lung CT studies were performed on 70 patients, successive PET/CT scans were performed on 7 patients, and only successive chest radiographs were performed on 27 patients. No further treatment for the underlying malignancy was performed when there was no clinical evidence of tumor recurrence, and the referring physician opted for close follow-up with imaging studies for the indeterminate lung nodules. Malignancy was concluded when the nodule showed a significant increase in size, the number of pulmonary nodules, or the pSUV at any time point during the follow-up imaging studies. Though pulmonary metastasis is most likely in the setting of underlying cancer, primary lung cancer cannot be excluded without tissue confirmation. Therefore, the term “malignancy” is used rather than metastasis in this article. Nodules that remained unchanged after at least 1 y of follow-up from the PET/CT scan were presumed to be granulomas. Nodules that were visualized and then spontaneously resolved without further therapy on the later chest images were also considered benign lesions.
Statistical Analysis
Statistical analysis was performed using the statistical package for social sciences (SPSS) software, version 13.0. The Mann–Whitney test was used to compare the differences between the conclusively benign and malignant groups. The paired results of the 3 variables—that is, solitary versus multiple, accompanying lung lesion absent versus present, and 18F-FDG uptake imperceptible versus perceptible—were also compared. Multiple regression analysis was performed to find characteristics with significant correlation (P < 0.05 was considered significant).
RESULTS
One hundred twenty-one patients (55 men, 66 women; mean age, 56.6 ± 10.9 y; age range, 31–79 y) were included in the study. Twenty-four (19.8%) of the patients were identified as having lung malignancies: 4 cases were histologically confirmed as pulmonary metastases after tissue biopsy and 20 cases were confirmed by the results of a series of enhanced lung CT or PET/CT studies.
The number of nodules identified as either benign or malignant are shown according to the 3 variables (Table 2). First, malignancies were more common in the multiple nodules groups (18/77, 23.4%) than in the solitary nodule group (6/44, 13.6%), but there was no statistically significant difference between the 2 groups (P = 0.198).
Number of Cases Proven to Be Either Benign or Malignant for 3 Variables
Second, more nodules were confirmed to be malignant in the absent group with no accompanying benign lung lesions (21/85, 24.7%) than in the present group with accompanying lung lesions (3/36, 8.3%). In the case of absent versus present groups, the difference was statistically significant (P = 0.040) (Figs. 1 and 2).

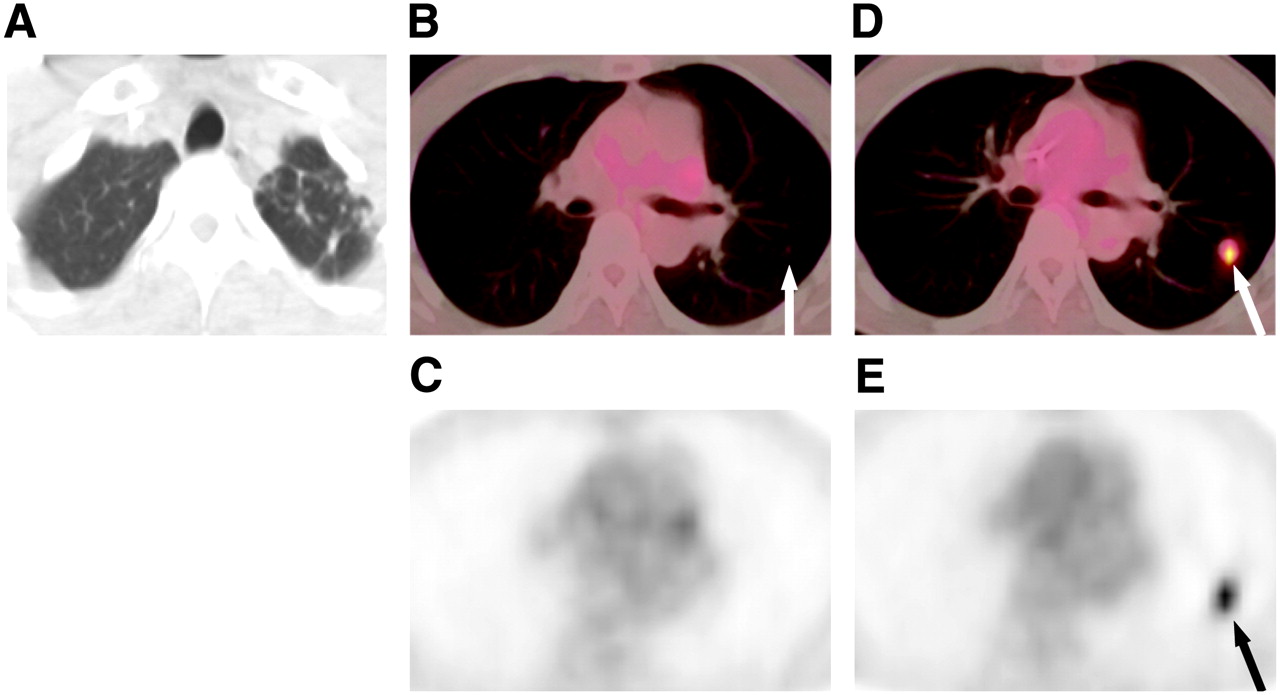
Fibrotic scar (arrow) is present in right middle lobe on lung setting window CT image (A) of 42-y-old female breast cancer patient with past history of modified radical mastectomy, chemotherapy, and radiation therapy. PET/CT fusion images show small nodule in right upper lobe (B, arrow) and another in right middle lobe (C, arrow) without any 18F-FDG uptake on PET images (D and E). Follow-up lung CT images demonstrated no difference in size and shape of these nodules for >27 mo (image not shown), and nodules were presumed to be benign.

Fibrotic scars are present in left apex on lung setting CT image (A) of 44-y-old male colon cancer patient with past history of right hemicolectomy and chemotherapy. PET/CT fusion image (B) shows small nodule in left upper lobe (arrow) without any 18F-FDG uptake on PET image (C). On follow-up PET/CT (D) and PET (E) images performed 5 mo later, left upper lobe nodule demonstrates increased size and 18F-FDG uptake, indicating malignancy (arrow).
Finally, of the nodules with no perceptible 18F-FDG uptake, 20.7% (19/92) were recognized as lung malignancies, and 17.2% (5/29) of the nodules with faintly perceptible 18F-FDG uptake were malignancies. Again, there was no statistically significant difference between the results of the 18F-FDG uptake imperceptible group and the perceptible group (P = 0.644) (Figs. 3 and 4).
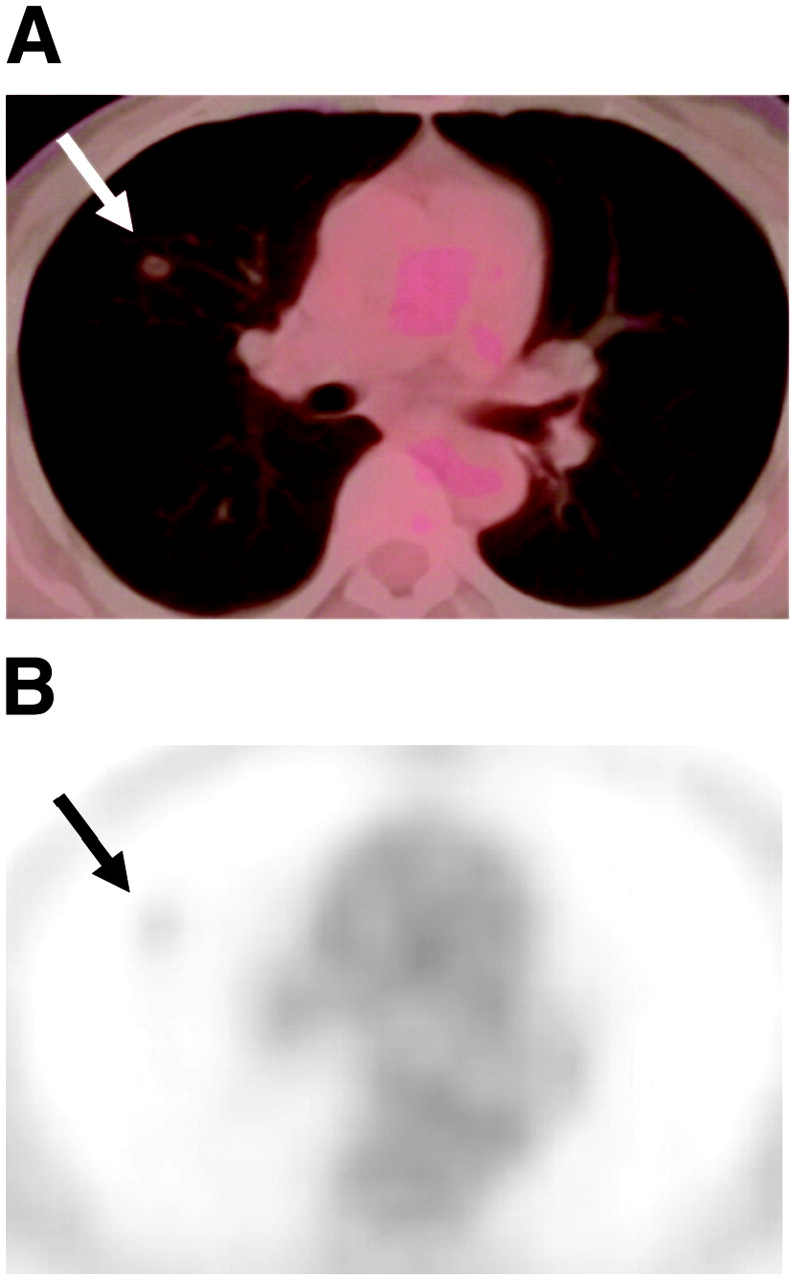
PET/CT fusion (A) and PET (B) images of 52-y-old female breast cancer patient who underwent modified radical mastectomy show solitary nodule with faintly perceptible 18F-FDG uptake in right upper lobe (arrow). Wedge resection confirmed metastatic adenocarcinoma.
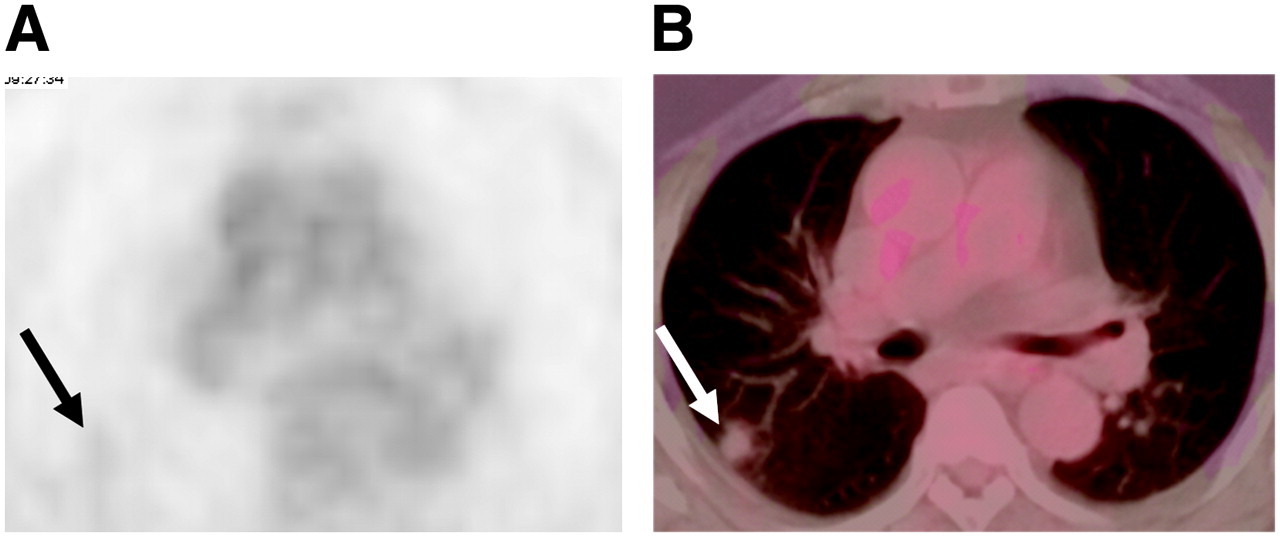
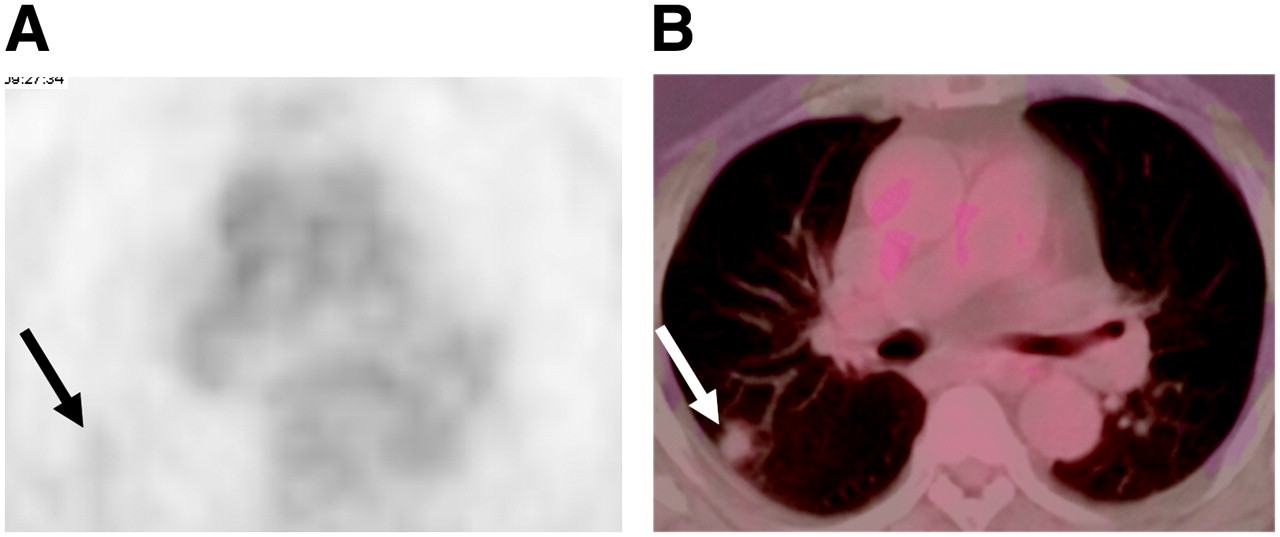
PET (A) and PET/CT fusion (B) images of 73-y-old male patient who received chemotherapy and radiation therapy for sigmoid colon cancer demonstrate solitary nodule measuring 1 cm in diameter with faint 18F-FDG uptake in right upper lobe (arrow). Eosinophilic lung disease was diagnosed after correlation with laboratory results and clinical course.
Logistic regression analysis was performed with the 3 variables, and the computed odds ratios are shown in Table 3. With an adjusted odds ratio of 4.9, only the absence of a benign lung lesion elsewhere in the lungs was a statistically significant risk factor for the small nodule being a malignant lesion. Though the multiplicity of nodules gave an odds ratio of 2.8, and thus suggested increased likelihood for being malignant compared with solitary nodules, the odds ratio is statistically insignificant.
Unadjusted and Adjusted Odds Ratios for Nodule to Be Malignant
The primary tumors of the patients diagnosed with malignant lung nodules were diverse and included cancers of the uterine cervix (4/8 were malignant), prostate (1/2), liver (4/13), breast (8/28), colon (3/18), ovary (1/8), head and neck (2/13), and bone and connective tissue (1/4). The histologic types of the primary tumors with the highest number of pulmonary nodules proven to be malignant were adenocarcinoma (6/36 were malignant), invasive ductal carcinoma (8/24), and hepatocellular carcinoma (4/13).
On multiple regression analysis, none of the variables—not the number of nodules (P = 0.140), the presence of other benign lung lesions (P = 0.085), or the degree of 18F-FDG uptake (P = 0.811)—was statistically significant in distinguishing benign and malignant nodules.
DISCUSSION
In addition to the clear roles the unenhanced CT portion of PET/CT plays in reducing imaging time, attenuation correction, and better localization of lesion, the CT images discover clinically significant findings missed by the PET portion when reviewed by an expert radiologist (5,19). A small, non-18F-FDG–avid pulmonary nodule is one example (10). We wanted to discover the overall rate of metastases for such subcentimeter lung nodules. In our study, nearly one fifth of such nodules turned out to be malignant.
Furthermore, we were troubled by 3 additional questions. One, are lesions with faint 18F-FDG uptake more likely to be malignant than the 18F-FDG uptake imperceptible lesions? The results of this study show that no difference exists between the malignancy rates of faintly 18F-FDG perceptible nodules and 18F-FDG imperceptible nodules. PET, as with any imaging modality, can fail to detect certain lesions for a certain number of reasons. Partial-volume-averaging effect is a reduction in detected activity that occurs when the object size is smaller than the axial or transaxial spacing (20). The signal of small lesions can be “diluted” during reconstruction and malignant lesions can result in false-negative findings on PET images (21). Owing to the restricted resolution of PET scanners, Kernstine et al. believed that a negative PET finding in lesions 5–10 mm in size provided no information at all (22). Effects of respiratory motion are also well known to cause artifacts on PET images (23,24). The small number of tumor cells can be the limiting factor for detection by PET, as a low tumor cell-to-background ratio can evade detection (25,26). Fischer et al. estimated 106 malignant cells, possibly 1 mm in diameter, as the PET detection limit in the clinical setting (27). Finally, the 18F-FDG avidity of the tumor in question—that is, the degree of elevated glucose metabolism—can determine the sensitivity of 18F-FDG PET. Malignancies such as prostate cancer, renal cell carcinoma, low malignant potential and early-stage ovary carcinoma, bronchioalveolar cell carcinoma, and carcinoid tumors are several examples of tumors that have demonstrated low 18F-FDG uptake (28–30). Therefore, the pSUV of the subcentimeter nodules is not accurate, and distinguishing the incorrect values as either faintly perceptible or imperceptible may be pointless.
Two, will the presence of other benign lung lesions predispose the nodule as benign also? Here, a significant difference in the rates of malignancy was noted between the present and absent groups. The accompanying benign lung lesion present group had a lower rate of malignancies (8.3%) than that of the absent group (24.7%), and the malignant nodules showed an increased odds ratio of 4.9 to be unaccompanied by other benign pulmonary conditions. However, even with benign lung lesions present elsewhere in the lung field, malignancy was confirmed in 3 cases. Also, on multivariate analysis this feature of accompanying benign lung lesion did not have statistical significance.
Three, as with standard lung CT, are multiple nodules seen on the CT portion of PET/CT more likely to be metastases than solitary nodules? Patz et al. claimed that as high as 97% of multiple lesions seen on lung CT images are metastatic diseases when primary malignancy is known to be present (31). When ≥2 nodules were noted in our study, more were found to be metastatic (23.4%) than when only 1 nodule was present (13.6%). Nevertheless, these 2 rates have no statistically significant difference, and 59 of 77 cases in the multiple group were ultimately diagnosed as benign lung nodules.
Subcentimeter pulmonary nodules seen on lung CT present very difficult interpretation problems. For small pulmonary nodules, CT morphology is quite nonspecific, no typical feature of malignancy is defined, and considerable error is associated in the density measurement (32). Munden et al. reviewed the CT evaluation results of 3 different study groups for small pulmonary lesions and found that among the 246 lesions of 1 cm or smaller, 125 lesions were indeterminate on CT, and all 80 malignant lesions were from this indeterminate group (33). In a survey about the interpretation and management of very small (3–5 mm) pulmonary nodules that 151 members of the Society of Thoracic Radiology completed, most recommended short-term follow-up, though biopsy was more frequently chosen, with increased likelihood of malignancy in areas not endemic for granulomatous disease. Mundan and Hess also suggested that when very small nodules are detected on CT, the benign or malignant nature of many remains uncertain, and the method of further evaluation for the lesion in question is often based on the radiologist's suggestion (34).
In patients with previously confirmed malignancy, small pulmonary nodules become an even bigger concern. Benjamin et al. suggested that small nodules in patients with primary neoplasms were more likely to have a higher malignancy rate (35). In a study by Ginsberg et al. in which small nodules (<1 cm) detected on CT were removed by video-assisted thoracoscopic surgery, the malignancy rate was 42% in patients with prior malignancy (36). On the other hand, in a study on pulmonary nodules in children with malignant extrathoracic solid tumors by Grampp et al., 70% of solitary nodules (<5 mm) were benign, and the authors cautioned that smaller solitary nodules should not be automatically regarded as metastatic nodules (37). Other studies have reported greatly varying rates of malignancy, from 13% of Chalmers and Best (38) to 87% of Peuchot and Libshitz (39) for small pulmonary nodules in patients with extrathoracic malignancy.
However, directly comparing the studies done with standard diagnostic lung CT may be difficult because many of the CT scans obtained as part of PET/CT fusion scans are obtained at relatively lower power settings. We had 3 cases in which small pulmonary nodules were of indeterminate nature on the PET/CT images, but the diagnostic lung CT scans performed within a week of the PET/CT scans readily demonstrated more detailed features indicating that the nodules were benign.
The relatively low malignancy rate of our results compared with the studies discussed here may be due to a few factors: the difference in the quality of CT scanners, Korea being an endemic area for tuberculosis, and the fact that this study included only indeterminate nodules and excluded nodules strongly suggestive of being benign or malignant.
Tumors of the kidney, colorectum, liver, head and neck, breast, thyroid, testis, melanoma, endometrium, uterine cervix, ovary, prostate, choriocarcinoma, leiomyosarcoma, and sarcomas of other soft tissue and bone show a relatively high incidence of spread to the lungs (40). In our study, no lung metastasis was observed in the renal cell carcinoma, choriocarcinoma, thyroid cancer, melanoma, endometrial carcinoma, or bone sarcoma cases, most likely due to the limited number of cases. In addition, the melanoma and bone sarcoma patients were diagnosed at early stages (TNM stage I) and received prompt treatment for the underlying primary tumors. Thus, the all-benign results for the cases with underlying malignancies that are known to spread frequently to the lungs seen in our study are not reliable reflections of the true malignancy potential of the primary tumors.
This study has several limitations. The case selection was a relatively subjective process, albeit by experienced radiologists, where the definition of “most likely benign” is not clear-cut. Not all cases were pathologically confirmed. Although the cases concluded to be malignancies had more distinctive features on the following series of lung imaging studies—such as definitely increased tumor size and numbers—lesions thought to be benign may have been affected by several factors. For example, no change in size or shape may have been the belated results of previous chemotherapy on an actually malignant nodule, rather than a faithful sign of being benign. In addition, there were, in fact, 21 more cases demonstrating pulmonary nodules that matched the above criteria but were excluded because a subsequent imaging study was missing and, thus, the nature of the nodule in question remained undetermined. Furthermore, if higher resolution (4 mm) PET were applied, 18F-FDG uptake could have been more accurate, the grouping of faint or imperceptible 18F-FDG uptake may have been different, and higher-dose lung CT could have characterized the small nodules in more detail.
Further investigation with a larger number of cases collected from multiple centers may provide answers about the likelihood of malignancies and the optimal method of follow-up for such nodules. Computing the number of small pulmonary nodules that are consequently identified as malignant, and recognizing the conditions rendering malignancy more likely would provide clues to the interpretation of small lung lesions with 18F-FDG uptake less than that of the mediastinum. Knowing the incidence and likelihood of malignancies of subcentimeter pulmonary nodules with faint or no 18F-FDG uptake seen on the PET/CT images can guide the physician in determining further evaluation and management methods of patients with extrathoracic malignancy.
CONCLUSION
Small pulmonary nodules with faint or no 18F-FDG uptake discovered on PET/CT scans may harbor malignancy just beyond the detection powers of either PET or CT. The presence of a concomitant benign lung lesion showed a significantly lower likelihood of malignancies. No other factor inclined toward the nodule being benign or malignant. Therefore, regardless of the number of nodules or perceptibility of 18F-FDG uptake, pulmonary malignancies should be considered, especially if no other benign lung lesion can be seen in both lungs. Short-term follow-up examination with standard enhanced lung CT or tissue confirmation should be recommended to the physician who consulted for PET/CT in the staging or restaging of a known primary malignancy.
Footnotes
-
COPYRIGHT © 2007 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 7, 2006.
- Accepted for publication September 28, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}