


Abstract
The aim of this study was to explore the differential diagnostic value of PET using the amino acid O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) in patients with newly diagnosed solitary intracerebral lesions showing ring enhancement on contrast-enhanced MRI. Methods: 18F-FET PET analyses were performed on 14 consecutive patients with intracerebral ring-enhancing lesions. Eleven of the patients were additionally studied with 18F-FDG PET. In all patients, the main differential diagnosis after MRI was a malignant lesion, in particular glioblastoma multiforme, versus a benign lesion, in particular brain abscess. A malignant tumor was suspected for lesions showing increased 18F-FET uptake on PET images with a mean lesion-to-brain ratio of at least 1.6 (18F-FET PET positive). A nonneoplastic lesion was suspected in cases of minimal or absent 18F-FET uptake, with a mean lesion-to-brain ratio of less than 1.6 (18F-FET PET negative). Histologic diagnosis was obtained by serial biopsies in 13 of the 14 patients. One patient refused the biopsy, but follow-up indicated an abscess because his lesion regressed under antibiotic therapy. Results: Histology and clinical follow-up showed high-grade malignant gliomas in 5 patients and nonneoplastic lesions in 9 patients. The findings of 18F-FET PET were positive in all 5 glioma patients and in 3 of 9 patients with nonneoplastic lesions, including 2 patients with brain abscesses and 1 patient with a demyelinating lesion. The findings of 18F-FDG PET were positive (mean lesion-to-gray matter ratio ≥ 0.7) in 4 of 4 glioma patients and 3 of 7 patients with nonneoplastic lesions. Conclusion: Although 18F-FET PET has been shown to be valuable for the diagnostic evaluation of brain tumors, our data indicate that, like 18F-FDG PET, 18F-FET PET has limited specificity in distinguishing between neoplastic and nonneoplastic ring-enhancing intracerebral lesions. Thus, histologic investigation of biopsy specimens remains mandatory to make this important differential diagnosis.
The differential diagnosis of solitary intracerebral ring-enhancing lesions on contrast-enhanced MRI includes different types of malignant tumors, as well as various benign, nonneoplastic lesions. Among the tumors, high-grade glioma, in particular glioblastoma multiforme, and metastasis, most commonly metastatic carcinomas of the lung or breast, are the main differential diagnoses. Nonneoplastic masses that may appear as ring-enhancing lesions include intracerebral abscesses (including toxoplasmosis and fungal abscesses), demyelinating and reactive/resorptive lesions (acute inflammatory demyelination, resolving hematoma or infarction, radiation necrosis) and parasitic lesions (cysticercosis cyst, pork tapeworm). Because of the known uncertainties about the accuracy of MRI for noninvasive assessment of brain lesions (1,2), several attempts have been made to improve brain tumor diagnostics by metabolic imaging using PET and SPECT. Radiolabeled amino acids proved to be useful tracers for brain tumor diagnostics (3,4). Encouraging data showing improved tumor delineation with PET have been reported, especially with PET using [methyl-11C]-l-methionine (11C-MET) (5–13). Because of the short physical half-life of the 11C label (20 min), however, 11C-MET remains restricted to a few PET centers with a cyclotron on site and cannot become established in routine clinical practice.
The recently developed 18F-labeled amino acid O-(2-18F-fluoroethyl)-l-tyrosine (18F-FET) can be synthesized with high radiochemical yields, thus allowing large-scale production for clinical purposes (14,15). Initial clinical studies using 18F-FET PET in human brain tumors have shown results similar to those for 11C-MET PET (16,17). 18F-FET PET has been reported to allow tumor recurrence to be distinguished from radiation-induced changes in cases of suspected recurrent high- and low-grade gliomas (18). In addition, we have shown that delineation of the cellular tumor mass of human gliomas is better by 18F-FET PET than by MRI alone (19,20). In a prospective study of 50 patients with newly diagnosed lesions, we found that 18F-FET PET had a high specificity for the detection of both high- and low-grade gliomas and could serve as a useful tool for the diagnostic assessment of suspected glioma lesions, in particular concerning biopsy site planning (21).
For 11C-MET PET, several cases of significant tracer accumulation in histologically confirmed brain abscesses have been reported (22–25). Recent data from animal experiments indicate that 18F-FET, in contrast to 11C-MET and 18F-FDG, exhibits low uptake in nonneoplastic inflammatory cells and in inflammatory lymph nodes, thus promising a higher specificity for the detection of tumors (26,27).
The aim of the present prospective study was to explore the potential of 18F-FET PET for distinguishing between neoplastic and nonneoplastic solitary ring-enhancing lesions in humans.
MATERIALS AND METHODS
Patient Population
From June 2001 to June 2005, we screened 373 patients with newly diagnosed intracerebral mass lesions for the following inclusion criteria: an isolated solitary intracranial lesion with ring-shaped enhancement and central hypointensity on gadolinium-enhanced MRI but without solid or nodular enhancing areas; no systemic signs of infection, such as fever, nuchal rigidity, leukocytosis, or elevated C-reactive protein; and stable clinical and neurologic status without signs of increased intracranial pressure, thus allowing for elective management. The exclusion criteria included pretreated or multiple lesions; ring-enhancing lesions with areas of nodular enhancement; progressive clinical or neurologic deterioration with signs of increased intracranial pressure, thus necessitating emergency management; and clinical signs of infection, such as fever, nuchal rigidity, leukocytosis, or elevated C-reactive protein, indicating an active brain abscess requiring urgent puncture.
Within the 5-y study period, a total of 18 patients presented with a newly diagnosed solitary ring-enhancing lesion. Four of these patients had to be excluded: Two patients had large lesions with a midline shift and rapid clinical deterioration requiring emergency decompression. Glioblastoma multiforme was diagnosed in both patients. Two patients had signs of acute meningeal infection, such as fever, nuchal rigidity, or an elevated level of C-reactive protein, and in one of these patients the symptoms occurred in combination with a severely reduced neurologic status requiring emergency puncture. Purulent brain abscesses were found in both patients.
Finally, a total of 14 patients with solitary ring-enhancing lesions were able to undergo elective management including preoperative metabolic imaging with 18F-FET PET. Eleven patients (patients 1, 3–6, and 8–13) were additionally investigated by preoperative PET with 18F-FDG. Histologic diagnoses were obtained through neuronavigated biopsies in 13 patients. One patient (patient 2) refused the biopsy, and empiric antibiotic therapy was administered for 4 mo without a histologic diagnosis. The further course of this patient confirmed the working diagnosis of an intracerebral abscess; that is, MRI follow-up demonstrated continuous regression of his brain lesion, and MRI 1 y after diagnosis showed complete resolution of the lesion.
Initial symptoms were seizures in 8 patients and focal neurologic deficits in 6 patients. Eight patients presented with space-occupying lesions causing a mass effect (ventricular compression, midline shift), whereas the remaining 6 patients showed lesions without a significant mass effect. All patients had supratentorial lesions, 13 of which were lobar and 1 deep seated. Nine lesions were right hemispheric and 5 were left hemispheric. Detailed data on the individual patients is provided in Table 1. The study was approved by the local institutional review board at the Medical Faculty of Heinrich-Heine-University Düsseldorf and by federal authorities. All subjects gave written informed consent to participate in the study.
Clinical Data
MRI
MRI examinations were performed on a 1.5-T system (Sonata; Siemens). The conventional imaging protocol consisted of a T1-weighted 3-dimensional magnetization-prepared rapid-acquisition gradient-echo sequence (field of view, 25 cm; matrix, 205 × 256; repetition time, 2,200 ms; echo time, 3.9 ms; inversion time, 1,200 ms; flip angle, 15; number of slices, 128; slice thickness, 1.5 mm; slice gap, 0 mm; number of signals averaged, 1; time of acquisition, 6:38 min) before and 2 min after injection of 20 mL of gadolinium-diethylenetriaminepentaacetic acid (Magnevist; Schering) and a transversal fluid-attenuation inversion-recovery sequence (field of view, 25 cm; matrix, 205 × 256; repetition time, 9,000 ms; echo time, 119 ms; inversion time, 2,500 ms; flip angle, 90; number of slices, 25; slice thickness, 5 mm; slice gap, 0 mm; number of signals averaged, 2; time of acquisition, 4:32 min).
18F-FET PET
The amino acid 18F-FET was produced via phase transfer–mediated nucleophilic 18F-fluorination of N-trityl-O-(2-tosyloxyethyl)-l-tyrosine tert-butyl ester and subsequent deprotection (14). The uncorrected radiochemical yield was about 35% at a specific radioactivity of greater than 200 GBq/μmol and a radiochemical purity of greater than 98%. PET studies were acquired 15–40 min after intravenous injection of 200 MBq of 18F-FET, which was administered as an isotonic neutral solution. The measurements were performed on an ECAT EXACT HR+ scanner (Siemens Medical Systems) in 3-dimensional mode (32 rings, 15.5-cm axial field of view). For attenuation correction, transmission scans with 3 68Ge/68Ga rotating line sources were measured. After correction for random and scattered coincidences and dead time, image data were obtained by filtered backprojection in Fourier space using the ECAT 7.2 software (direct inverse Fourier transformation; Shepp filter, 2.48 mm in full width at half maximum; pixel size, 2 × 2 × 2.4 mm). The reconstructed images were decay corrected; the reconstructed image resolution was about 5.5 mm.
Preoperative MRI and 18F-FET PET were coregistered using dedicated software (MPI tool, version 3.28; ATV). Because most of the benign lesions exhibited indifferent 18F-FET uptake, an objective positioning of regions of interest (ROIs) on the PET scans based on threshold values was impossible. Therefore, irregular ROIs were placed manually on the contrast-enhancing ring on MR images and transferred to the coregistered 18F-FET and 18F-FDG PET scans. Information on the size of the ROIs is given in Table 1. A larger reference ROI was placed on contralateral normal-appearing brain, including white and gray matter. Mean and maximal standardized uptake values of 18F-FET were calculated by dividing the radioactivity (kBq/mL) of the ROIs by the radioactivity injected per gram of body weight for the corresponding PET scans. Mean and maximal lesion-to-brain ratios were calculated by dividing the mean and maximal ROI value of the lesion by the mean ROI value of the normal brain in the 18F-FET PET scan (18F-FET ratio). In a previous biopsy-controlled study, we found for tissue samples corresponding to normal and peritumoral tissue a mean lesion-to-brain ratio of 1.2 ± 0.4 (n = 26) for 18F-FET uptake (20). Therefore, a mean lesion-to-brain ratio of 1.6 was taken as the threshold for distinguishing between malignant and benign lesions. A lesion with a tracer uptake ratio of less than 1.6 was judged as 18F-FET negative, and a lesion with a ratio of at least 1.6 was judged as 18F-FET positive.
18F-FDG PET
18F-FDG was synthesized as previously described (28). The average specific radioactivity was greater than 200 GBq/μmol. The PET studies with 18F-FDG were done on a different day within 1 wk before or after the 18F-FET study. PET scans were acquired 30–60 min after intravenous injection of 200 MBq of 18F-FDG, which was administered as an isotonic neutral solution. The methods of reconstruction and attenuation correction were the same as described for 18F-FET. The 18F-FDG scans were coregistered to the preoperative MR images and to the 18F-FET PET scans as already described. The ROIs for the ring-enhancing lesions as used in the 18F-FET scans were transferred to the corresponding 18F-FDG scans. Because 18F-FDG uptake in gray matter is different from 18F-FDG uptake in white matter, the reference ROI for normal brain was different from that in the 18F-FET scans. A circular ROI was placed on contralateral gray matter, and mean and maximal lesion-to-brain ratios were calculated by dividing the mean and maximal ROI values of the lesion by the mean value of the cortical ROI in the 18F-FDG PET scan (18F-FDG ratio). A mean lesion-to-brain ratio of 0.7 was taken as the threshold for distinguishing between malignant and benign lesions (29). A lesion with a tracer uptake ratio of less than 0.7 was judged as 18F-FDG negative, and a lesion with a ratio of at least 0.7 was judged as 18F-FDG positive.
Neuronavigated Biopsy Procedure
MRI data were incorporated into the neuronavigation system. For coregistration, anatomic landmarks and external cutaneous fiducial markers were used in each examination. Tissue samples were collected in all cases from both the outer area of ring enhancement and the inner area of hypointensity. The biopsies were sampled with the aid of a standard stereotactic biopsy cannula, which was referenced to the neuronavigation system and connected to an adjustable Leyla arm. Through a small skin incision and a standard 8-mm burr hole, the cannula was placed under neuronavigated control into the area of interest. A 2-mm stereotactic forceps was used to obtain at least 5 and at most 12 biopsy specimens.
Histopathology
Routine histologic sections of each biopsy specimen were assessed by an experienced neuropathologist after they had been fixed in formalin and embedded in paraffin. Neoplastic lesions were classified according to the World Health Organization (WHO) classification of tumors of the nervous system (30). If necessary, immunohistochemical analyses were performed on formalin-fixed paraffin sections according to standard protocols, including staining for glial fibrillary acidic protein, neurofilament protein, myelin basic protein, macrophage/microglia marker CD68, lymphocytic markers (CD3, CD20, CD45), and the proliferation marker Ki-67 (MIB1). A conclusive histologic diagnosis was made for all 13 biopsied patients.
RESULTS
Histologic investigation revealed malignant gliomas in 5 of 14 patients, with 4 lesions corresponding histologically to glioblastomas of WHO grade IV and 1 lesion to anaplastic astrocytoma of WHO grade III. All 4 glioblastomas and the 1 anaplastic astrocytoma were 18F-FET positive. 18F-FDG PET was performed on 4 glioma patients (3 glioblastomas and 1 anaplastic astrocytoma) and had positive findings in all cases. Data on standardized uptake values and mean and maximal lesion-to-brain ratios are given in Table 2.
PET Results
In 9 patients, benign nonneoplastic lesions were diagnosed, including 5 cases of brain abscess, 1 case of acute demyelinating disease, 1 subdural empyema, and 2 intracerebral hematomas in resorption. 18F-FET PET had negative findings in 6 of 9 patients with benign lesions but (false) positive findings in 2 patients with brain abscess (Fig. 1) and in the patient with acute demyelination (Fig. 2). 18F-FDG PET was performed on 7 patients and had negative findings in 4 patients but (false) positive findings in 2 patients with brain abscess and in 1 patient with subdural empyema.

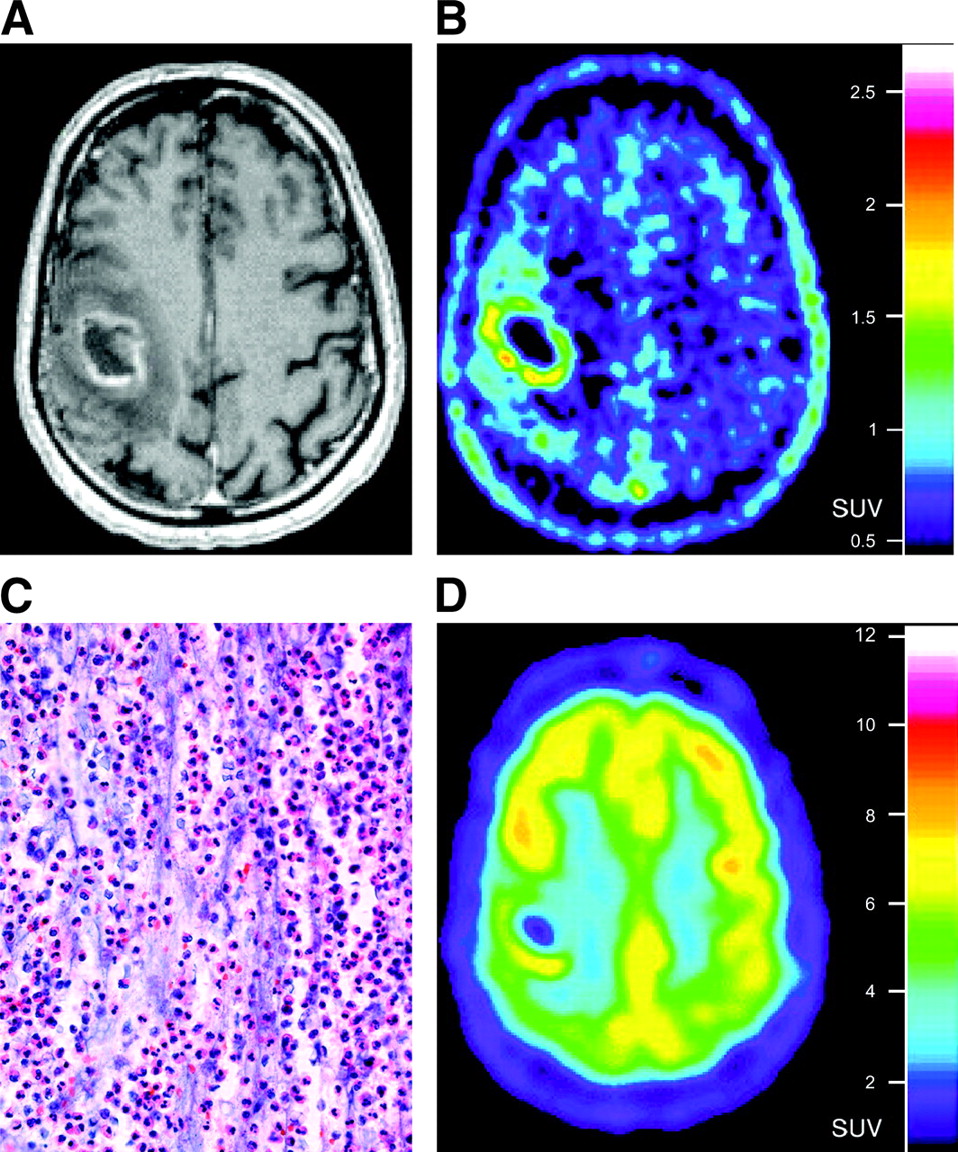
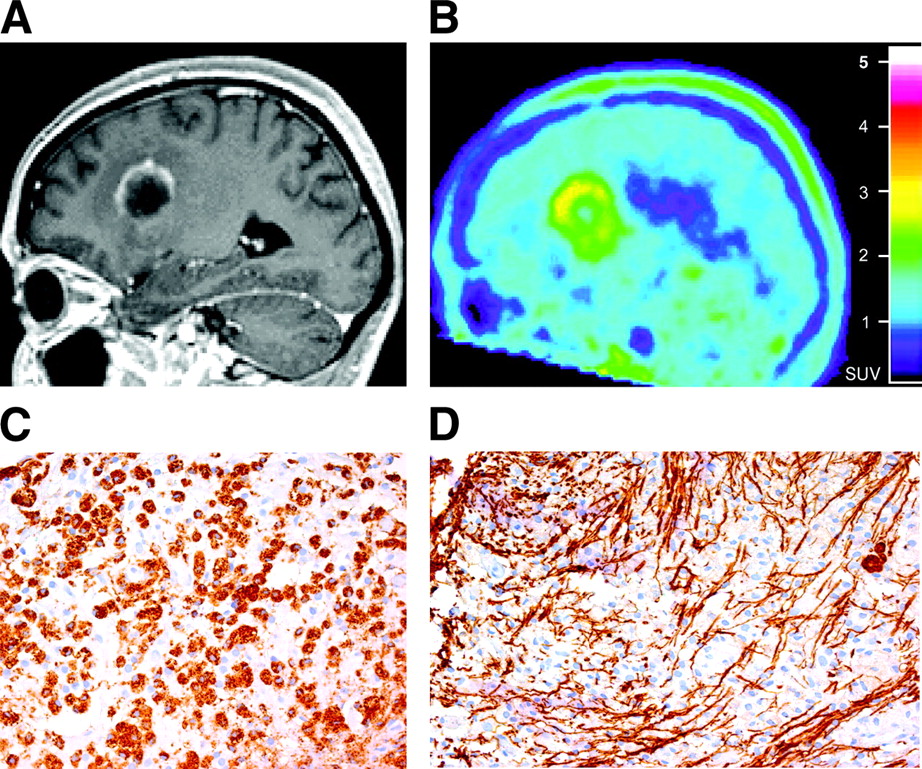
Intracerebral abscess in patient 4. (A) Gadolinium-enhanced MR image shows single right parietal ring-enhancing lesion. (B and D) 18F-FET PET image (B) and 18F-FDG PET image (D) demonstrate significant tracer uptake highly suggestive of malignant neoplastic lesion. (C) Photomicrograph of hematoxylin- and eosin-stained biopsy specimen reveals brain abscess with purulent content and partially necrotic granulocytes in fibrinoid exudations.
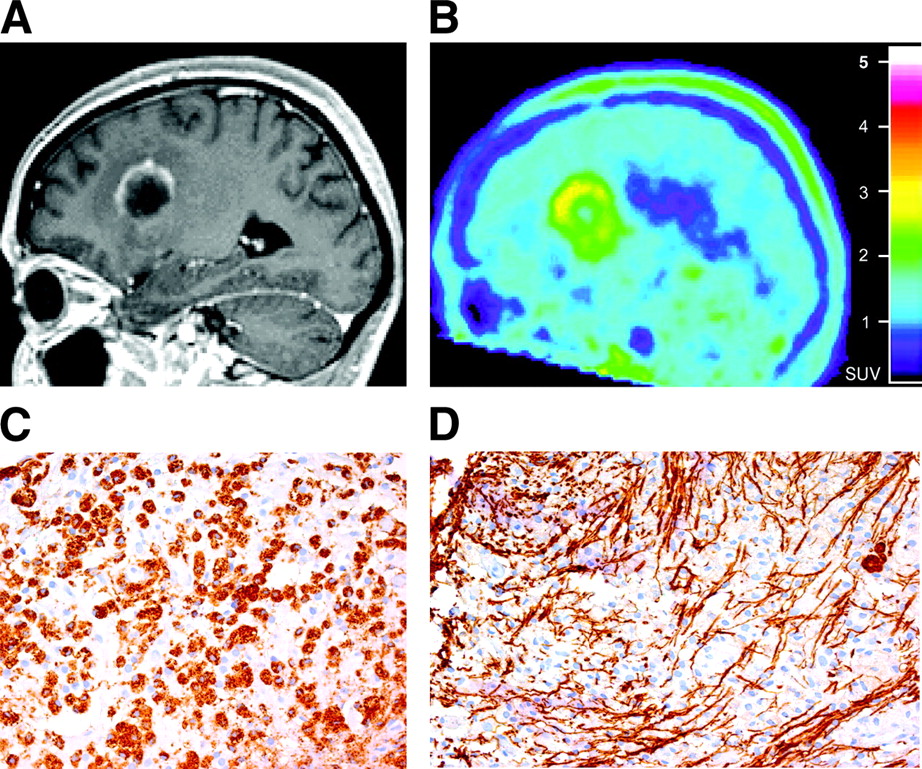
Demyelinating lesion in patient 7. (A) Gadolinium-enhanced MR image shows single left frontal ring-enhancing lesion. (B) 18F-FET PET image reveals significant uptake indicative of neoplastic lesion. (C) Photomicrograph of biopsy specimen reveals acute demyelinating lesion with massive invasion of macrophages as indicated by immunostaining for CD68. (D) Immunohistochemistry for neurofilaments shows persisting axonal processes but also axonal damage within lesion.
Accumulation of 18F-FET and 18F-FDG in the investigated ring-enhancing lesions was always within the boundaries of the gadolinium enhancement on MR images (irrespective of histology). In some cases, the distribution of the tracer uptake was identical to the area of gadolinium enhancement, and in some cases, the area of tracer uptake was smaller than the area of gadolinium enhancement. No 18F-FET or 18F-FDG uptake occurred outside the area of gadolinium enhancement, that is, within the central hypointensity or the perifocal edema. Tracer uptake did not correlate with patient age, sex, lesion location, seizure activity, lesion size and mass effect, extent of perifocal edema, or detection of a causative organism in an abscess.
DISCUSSION
Because of the known uncertainties in the differential diagnosis of an intracerebral ring-enhancing lesion on CT and MRI (31), preoperative metabolic imaging with PET is under investigation as a novel tool for the noninvasive identification of benign or malignant ring-enhancing lesions. Numerous case reports and studies on small patient groups have demonstrated that the gold standards of PET—imaging with the glucose analog 18F-FDG and the amino-acid 11C-MET—cannot reliably predict whether a lesion is malignant. Several studies have shown accumulation of these tracers in brain abscesses (23,24,32,33). A more recent study on 4 patients with brain abscesses reported that pre- and postoperative PET scans demonstrated significant tracer accumulation of both 11C-MET and 18F-FDG in all lesions both before treatment and during antibiotic treatment after puncture of the abscesses (25). The area of increased 11C-MET and 18F-FDG uptake corresponded closely to the enhancing area on CT and MR images. The authors speculated that the mechanism of 11C-MET uptake in the inflammatory area might be related to the higher metabolic rate and the active transport of amino acids, as well as to disruption of the blood–brain barrier. The mechanism of 18F-FDG uptake was thought to be related to a higher metabolic rate and the increased density of inflammatory cells. It was concluded that PET images reflect the degree of inflammatory response in brain abscesses—thus suggesting that PET is useful in detecting inflammatory lesions and in assessing the clinical effects of antibiotic treatment (25).
In most cases of brain abscesses, the area of increased 11C-MET and 18F-FDG uptake corresponds closely to the area of gadolinium enhancement on CT and MR images. However, on record are individual patients showing 18F-FDG uptake within a brain abscess and not in the contrast-enhancing walls (34) or high uptake of both 11C-MET and 18F-FDG around a brain abscess (22). Taken together, these findings allow one to conclude that there is a frequent lesional accumulation of 11C-MET and 18F-FDG in patients with a brain abscess and that the uptake usually correlates with the disruption of the blood–brain barrier visible as gadolinium enhancement on MR images.
The amino acid 18F-FET shows a high diagnostic accuracy in brain tumors (21,22), and experimental studies have indicated that 18F-FET is more specific than 18F-FDG and 11C-MET in distinguishing inflammatory lesions from malignant lesions (26,27). Recently, a PET study of peripheral tumors demonstrated that 18F-FET, unlike other tyrosine derivatives such as l-11C-tyrosine, 2-18F-fluoro-l-tyrosine, or l-3-18F-fluoro-α-methyltyrosine, showed no uptake in lymphomas or in most adenocarcinomas (35). On the contrary, all squamous cell carcinomas turned out to be 18F-FET positive in this study. Another report, on patients with squamous cell carcinomas of the neck, revealed low 18F-FET uptake in inflammatory tissue surrounding the tumors, which themselves exhibited high 18F-FDG uptake (36). The investigators speculated that a selective transport of 18F-FET via subtype 2 of the amino acid transport system L might account for the rather selective accumulation of 18F-FET in certain tumor types and the low uptake in inflammatory tissue (35).
The result of the present pilot study on ring-enhancing brain lesions indicates that the situation in the brain may be different from that in peripheral tissue. We observed a significant uptake of 18F-FET in 2 of 5 brain abscesses. It remains to be elucidated which specific cellular components other than macrophages in brain lesions lead to the increased 18F-FET uptake. In any case, high 18F-FET uptake in a ring-enhancing lesion should be interpreted with caution and a biopsy remains necessary.
A diagnostic challenge in the field of ring-enhancing lesions is the distinction of acute inflammatory demyelination. Demyelinating disease may manifest in the form of a solitary lesion but often presents as multiple intracerebral ring- or ringlike-enhancing lesions. The main differential diagnoses include metastatic carcinoma, high-grade glioma, and brain abscess. In a retrospective analysis of 6 patients with histologically proven acute demyelination treated between 1990 and 2001, PET was performed in 2 cases to assess the metabolic activity of the lesions (37). The histopathologic diagnosis was established by stereotactic biopsy in 5 patients and by microsurgical resection of the lesion in 1 patient. In 1 patient, both 11C-MET PET and 18F-FDG PET were performed, and there was no uptake of either tracer. In another patient, only 11C-MET PET was performed, and the lesion showed only an unspecific, low uptake of the tracer (lesion-to-brain ratio, 1.25). In contrast to these observations, we detected marked 18F-FET uptake (mean lesion-to-brain ratio, 2.0) in patient 7, who had an acute demyelinating lesion. This result indicated tumor, and additional investigation of this patient with single-voxel MRI spectroscopy supported the hypothesis of a neoplastic lesion: The spectra patterns were typical, showing a high concentration of choline (indicating cellular proliferation) and the absence of N-acetyl-aspartate (denoting loss of neurons), with an N-acetyl-aspartate–to–choline ratio of 0.5. However, histologic examination revealed an acute inflammatory demyelinating lesion with massive invasion of macrophages. With steroid medication, the lesion nearly disappeared within 3 mo, but all tests for multiple sclerosis were negative at that time. Six months later, typical periventricular lesions developed and the diagnosis of multiple sclerosis was established.
A limitation of our study might be that static 18F-FET scans were acquired only from 15 to 40 min after injection. 18F-FET uptake usually reaches a maximum approximately 15 min after injection, and tumor-to-brain ratios have shown only a minor decrease up to 60 min after injection (17). During the first 15 min after injection, the tracer concentration in the blood pool is high and may mimic pathologic 18F-FET uptake in benign lesions—for example, in aneurysms (38). Therefore, imaging during the first 15 min after injection was avoided in our study.
A recent study found that a dynamic acquisition of 18F-FET uptake might be helpful in differentiating between high-grade and low-grade gliomas (38). Although low-grade gliomas exhibited increasing tumor-to-brain ratios at 0–10 min after injection, compared with at 30–40 min after injection, decreasing tumor-to-brain ratios were observed for high-grade gliomas. However, because gliomas may exhibit both increasing and decreasing tumor-to-brain ratios, it is unlikely that a dynamic evaluation will be helpful in differentiating gliomas, abscesses, and demyelinating processes.
Taken together, our data indicate that metabolic imaging using 18F-FET PET does not appear to be sufficiently specific to allow for a reliable noninvasive distinction between neoplastic and nonneoplastic intracerebral ring-enhancing lesions. Therefore, a histologic diagnosis should be attempted in all such patients. Although a morbidity ranging from 1% to 2% and lethal outcome in rare cases has to be tolerated (39), stereotactic or neuronavigated biopsy remains the method of choice to obtain the firm diagnosis that is necessary to guide adequate treatment.
CONCLUSION
Although 18F-FET PET has been demonstrated to be a useful method to detect the extent of gliomas and to differentiate tumor recurrences from unspecific posttherapeutic changes in brain tissue, our data indicate that in newly diagnosed solitary intracerebral ring-enhancing lesions, 18F-FET PET is not able to distinguish reliably between benign nonneoplastic lesions and malignant gliomas. High uptake may occur in cases of brain abscess and in acute inflammatory demyelination. In accordance with previous findings, 18F-FDG PET did not improve the predictive value of preoperative imaging. Therefore, a biopsy with sampling of tissue specimens for neuropathologic evaluation remains the gold standard to establish a definite diagnosis in patients with newly diagnosed intracerebral ring-enhancing lesions.
Acknowledgments
The authors thank Suzanne Schaden, Elisabeth Theelen, Barbara Elghahwagi, and Gabriele Oefler for assistance with the patient studies and Silke Grafmüller, Bettina Palm, and Erika Wabbals for radiosynthesis of 18F-FET. This work was supported by the Brain Imaging Center West and a grant from the Deutsche Krebshilfe (70-3088-Sa I). The facility for MRI at the Institute of Medicine–Research Center Juelich was supported by the Bundesministerium für Bildung und Forschung grant BMBF 01GO0104.
References
- Received for publication December 16, 2005.
- Accepted for publication January 24, 2006.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amino Acid PET in Neurooncology
- Amino Acid PET in Neurooncology
- Epileptic Activity Increases Cerebral Amino Acid Transport Assessed by 18F-Fluoroethyl-L-Tyrosine Amino Acid PET: A Potential Brain Tumor Mimic
- TSPO Imaging in Glioblastoma Multiforme: A Direct Comparison Between 123I-CLINDE SPECT, 18F-FET PET, and Gadolinium-Enhanced MR Imaging
- The Usefulness of Dynamic O-(2-18F-Fluoroethyl)-L-Tyrosine PET in the Clinical Evaluation of Brain Tumors in Children and Adolescents
- Replay: Being Sensitive: to Specify When Amino Acid Tracers Accumulate in a Brain Lesion
- Diagnostic Performance of 18F-FET PET in Newly Diagnosed Cerebral Lesions Suggestive of Glioma
- Performance of 18F-Fluoro-Ethyl-Tyrosine (18F-FET) PET for the Differential Diagnosis of Primary Brain Tumor: A Systematic Review and Metaanalysis
- O-(2-18F-Fluoroethyl)-L-Tyrosine PET Predicts Failure of Antiangiogenic Treatment in Patients with Recurrent High-Grade Glioma
- Comparison of O-(2-18F-Fluoroethyl)-L-Tyrosine and L-3H-Methionine Uptake in Cerebral Hematomas
- Tumor Cell Metabolism Imaging
- Prognostic Value of 18F-Fluoroethyl-L-Tyrosine PET and MRI in Small Nonspecific Incidental Brain Lesions
- Metabolic Imaging of Cerebral Gliomas: Spatial Correlation of Changes in O-(2-18F-Fluoroethyl)-L-Tyrosine PET and Proton Magnetic Resonance Spectroscopic Imaging
- Differential Uptake of O-(2-18F-Fluoroethyl)-L-Tyrosine, L-3H-Methionine, and 3H-Deoxyglucose in Brain Abscesses
- PET/CT of Skull Base Meningiomas Using 2-18F-Fluoro-L-Tyrosine: Initial Report