


In the last hundred years, lung cancer has risen from a reportable disease to the most common cause of death from cancer in both men and women in developed countries (1). When descriptions of lung cancer were published in 1912, there were only 374 reported cases (2). In the 1950s, little more than the chest radiograph and sputum cytologic analysis were available for lung cancer screening. Since then, the mortality from lung cancer has decreased, but the 5-y cure rates have barely improved (1). The annual number of deaths from lung cancer is greater than the numbers of deaths from breast, colon, and prostate cancers combined. More than 150,000 patients died of lung cancer in 2004. The 5-y survival rates currently are 16% in the United States and 5% in the United Kingdom. The association of lung cancer with tobacco smoking was initially reported in the 1950s (3) and subsequently led to the determination by the U.S. Surgeon General that smoking is harmful to one's health (4). Further investigation has led to the discovery that this association is related to the type and amount of tobacco product used, the age at initiation, and the duration of use.
Lung cancer often presents as a solitary pulmonary nodule on chest radiographs. Chest radiographs usually are performed for patients as a preoperative or physical examination screening test, often in the absence of symptoms. Few signs and symptoms are present at an early stage, leading to more advanced disease when patients present to their physicians. One third of lung nodules in patients more than 35 y old are found to be malignant. Over 50% of the radiographically indeterminate nodules resected at thoracoscopy are benign (5). It is clear that there is a need for the accurate diagnosis of these lesions. The use of PET has much promise as an aid to the noninvasive evaluation of lung cancer. 18F-FDG PET currently is indicated for the characterization of lung lesions, staging of non–small cell lung carcinoma (NSCLC), detection of distant metastases, and diagnosis of recurrent disease. Furthermore, many institutions have found significant value in 18F-FDG PET for treatment monitoring (6–8).
CONVENTIONAL IMAGING OF LUNG NODULES
The definition of a solitary pulmonary nodule is an opacity in the lung parenchyma that measures up to 3 cm and that has no associated mediastinal adenopathy or atelectasis. Lesions measuring greater than 3 cm are classified as masses (9). Lung nodules can be benign or malignant and can have a multitude of causes, ranging from inflammatory and infectious etiologies to malignancies. The morphologic characteristics revealed by chest radiographs and CT provide much information to aid in the diagnosis of a nodule. 18F-FDG PET provides complementary information on the metabolic activity of a nodule that cannot be obtained by radiographic methods and that otherwise can be inferred only over time.
The evaluation of a solitary pulmonary nodule often begins when it is discovered incidentally on a chest radiograph, prompting further workup. Additional evaluation may reveal characteristics that indicate benignity or that warrant follow-up or biopsy. A nodule newly discovered on a chest radiograph should be analyzed for benign characteristics. A uniformly and densely calcified rounded nodule on a chest radiograph is classified easily as benign. Few nodules can be determined to be benign on the basis of chest radiographic findings, and most cases are referred for CT evaluation. Radiographs obtained before CT are invaluable for determining the time course of the development of a nodule. Subtle changes are not well evaluated on chest radiographs, but finding little change in appearance over 2 y or, preferably, longer would be more convincing of benignity.
Before the advent of PET, an indeterminate nodule on a chest radiograph was best evaluated initially with CT (10,11). CT remains an integral part of the evaluation of solitary pulmonary nodules; however, more options are now available to clinicians for evaluating such nodules. CT is used to evaluate the shapes, borders, and densities of nodules. CT densitometry has been used to detect calcifications within nodules. Although internal calcifications in general are frequently associated with benignity, calcified lung nodules also may result from metastasis from primary bone tumors, soft-tissue sarcomas, and mucin-producing adenocarcinomas. In addition, internal hemorrhage, such as that which occurs within choriocarcinoma and melanoma metastases, can simulate the increased density of calcifications. Diffuse calcifications measuring greater than 300 Hounsfield units (HU) throughout a nodule are indicative of a benign nodule. A well-circumscribed nodule with central or lamellar calcifications also is indicative of benignity (9). The diagnosis of a benign nodule is presumed only when a majority of the lesion demonstrates attenuation consistent with calcium. The calcifications must be located in the center of the lesion to be considered benign. Other patterns include popcorn or chondroid calcifications, which, in conjunction with fat, are characteristic of hamartomas. Figures 1 and 2 demonstrate shapes, borders, and patterns of calcification in pulmonary nodules. In addition, the pattern of contrast enhancement can indicate benignity. A nodule that enhances at less than 15 HU in its central portion is considered benign. A nodule with enhancement at greater than 25 HU is considered malignant (12,13). The use of contrast enhancement to characterize pulmonary nodules as benign or malignant has not gained widespread acceptance.
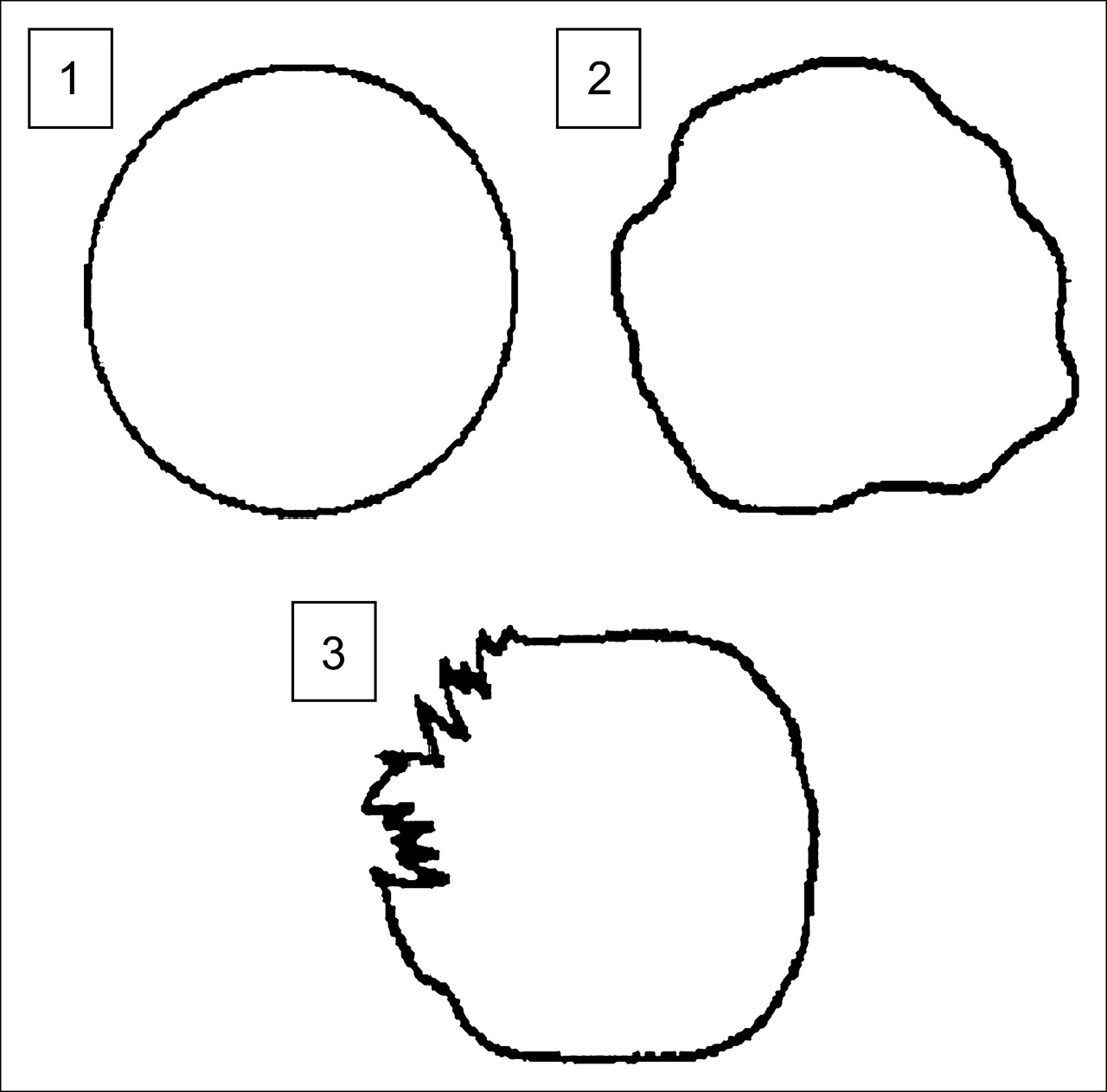
Schematic diagram of pulmonary nodules. Nodule 1 has smooth, well-defined border. Nodule 2 has lobulated border. Nodule 3 has spiculated border. (Reprinted with permission of (9).)

Patterns of calcification in pulmonary nodules. Nodules 1 and 2 have central calcifications, a benign pattern. Nodules 3 and 4 have eccentric calcifications, which cannot be classified as benign. (Reprinted with permission of (9).)
Ground-glass opacities also can have a nodular appearance. Ground-glass nodules are less dense than solid nodules and the surrounding pulmonary vasculature and do not obscure the lung parenchyma (Fig. 3). These nodules also are referred to as subsolid nodules and can be purely ground-glass in appearance or can have mixed solid and ground-glass components. Ground-glass opacities continue to be a dilemma, as the morphologic characteristics of a benign or malignant ground-glass nodule are less well described. According to the Early Lung Cancer Action Program (ELCAP) study, 20% of pulmonary nodules on baseline screening are ground-glass or subsolid (14). That study demonstrated that the overall frequency of malignancy is much higher in ground-glass and mixed nodules than in solid nodules. The cell types of malignancies within these nodules also are different from those within solid nodules. The cell types typically included pure bronchioalveolar cells or adenocarcinomas with bronchioalveolar features. Solid nodules are typically invasive subtypes of adenocarcinoma. There are few data on the evaluation of ground-glass nodules by 18F-FDG PET. One source reported a sensitivity of 10% and a specificity of 20% for ground-glass nodules on 18F-FDG PET (15). Further investigation is necessary; however, the pathology findings of the ELCAP study suggest that there will be little utility in the diagnosis or follow-up of ground-glass nodules by 18F-FDG PET because of the small size of the nodules and the potential for false-negative findings in focal bronchioalveolar cell carcinoma.
Ground-glass opacity in peripheral right lung. Mild 18F-FDG activity is associated with this lesion.
Certain morphologic characteristics of pulmonary nodules are considered indicative of malignancy; these include a spiculated outer margin (Fig. 1), a hazy and indistinct margin, endobronchial extension, extension to pulmonary veins, and focal retraction of the adjacent pleura. Heterogeneous internal composition and associated necrosis are indicative of malignancy. Malignant lesions also can simulate benign conditions by creating air bronchograms that are commonly associated with pneumonia. Entities such as bronchioalveolar cell carcinoma and lymphoma can masquerade as benign lung lesions.
Malignant nodules are not always easily distinguished from benign nodules. Furthermore, 25%−39% of malignant nodules are inaccurately classified as benign after radiologic assessment of morphologic characteristics, including size, margins, contour, and internal characteristics (16). Morphologic stability over 2 y is considered a reliable sign of benignity. The doubling time of the volume of a nodule is a commonly used marker of the growth of the nodule. For malignant nodules, the doubling time is usually 30–400 d. Benign nodules demonstrate doubling times outside this range, both higher and lower. Because a doubling in volume amounts to a 26% increase in nodule diameter (17), a significant change in nodule size may be difficult to appreciate, especially for a small nodule. Furthermore, the predictive value of stability in size may be only 65% (18).
Clinical information often is useful in the assessment of pulmonary nodules. Important features of the patient's history can be combined with imaging findings to calculate a likelihood ratio for malignant disease (Table 1). This type of Bayesian analysis can be used to stratify the patient's risk of malignancy and to guide management. In this scheme, patients are monitored if the probability of cancer is less than 5%, the lesion is biopsied if the probability is between 5% and 60%, and nodules are resected if the probability is greater than 60% (19,20). About half of the patients undergoing surgical biopsy of an indeterminate pulmonary nodule have benign disease (5,21).
Likelihood Ratios for Lung Cancer, as Determined by Morphologic and Demographic Information
18F-FDG PET FOR EVALUATION OF SOLITARY PULMONARY NODULES
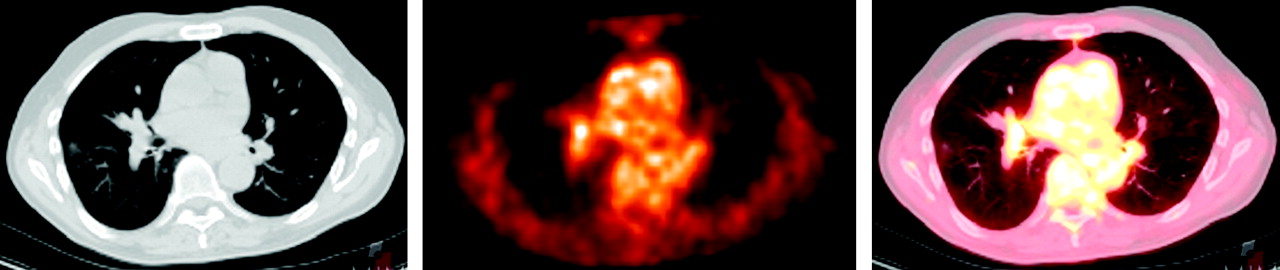
The development of 18F-FDG PET has taken the evaluation of solitary pulmonary nodules beyond morphologic and predictive analyses to functional and metabolic analyses of disease. PET alone has been described as a better predictor of malignancy than clinical and morphologic criteria combined (22,23). A prospective study of 87 patients examined whether preferential 18F-FDG uptake in malignant nodules could differentiate these from benign pulmonary nodules (24). The investigators found that when a mean standardized uptake value (SUV) of greater than or equal to 2.5 was used for detecting malignancy, the sensitivity, specificity, and accuracy were 97%, 82%, and 92%, respectively (Fig. 4). In addition, they also determined that there was a significant correlation between the doubling time of tumor volume and the SUV. Subsequent studies demonstrated a sensitivity of 90%−100% and specificity of 69%−95% for PET (15,25,26). Although the SUV is a useful tool, it has been shown to be equivalent to the visual estimate of metabolic activity by experienced physicians (27,28).

Solitary pulmonary nodule with spiculated borders in left upper lobe. No mediastinal adenopathy was present on additional images. Hypermetabolism is present within this nodule. Maximum SUV measures 6.7 g/mL. Findings are consistent with malignancy.
Studies that favor 18F-FDG PET for the diagnostic workup of solitary pulmonary nodules to reduce inappropriate invasive diagnostic investigation and subsequent complications are emerging. A study performed in Italy compared the traditional workup of a solitary pulmonary nodule with CT, fine-needle aspiration, and thoracoscopic biopsy with a diagnostic workup including 18F-FDG PET (29). That study demonstrated a cost reduction of approximately €50 (∼$60) per patient when PET was added to the traditional workup. A recent study in France compared the cost-effectiveness ratios of 3 management scenarios for solitary pulmonary nodules: wait and watch with periodic CT, PET, and CT plus PET (30). For their typical patient, a 65-y-old male smoker with a 2-cm solitary pulmonary nodule and an associated high risk of malignancy of 43%, the wait-and-watch scenario was the least effective strategy. CT plus PET was the most effective strategy and had a lower incremental cost-effectiveness ratio. Their conclusion was that CT plus PET was the most cost-effective strategy for patients with a risk of malignancy of 5.7%−87%. The wait-and-watch scenario was most cost-effective for patients with a risk of 0.3%−5%.
The minimum size of a pulmonary nodule has been an issue with regard to accurate diagnostic evaluation, follow-up, and even biopsy. The NY-ELCAP study monitored 378 patients with pulmonary nodules determined by CT to be less than 5 mm in diameter. None of these nodules was diagnosed as pathologically malignant, leading the researchers to suggest limiting further workup to nodules that were 5 mm or larger (31). A group in Spain investigated the utility of PET in evaluating nodules of 5–10 mm in diameter and greater than 10 mm in diameter; the sensitivity for detecting malignancy in all nodules was fairly low, at 69%, whereas the sensitivity for detecting malignancy in nodules of greater than 10 mm was 95% (32). The authors noted that the apparent uptake in nodules decreased when the diameter was less than twice the spatial resolution of the system (approximately 7−8 mm); thus, different criteria are needed to determine malignancy in nodules of less than 15 mm. Short-term follow-up of 5- to 10-mm nodules with CT alone to evaluate for growth resulted in a low rate of invasive procedures for benign nodules. In a phantom study with 18F-FDG-filled spheres measuring between 6 and 22 mm, the detection of nodules of less than 7 mm was unreliable (33). Further investigation is necessary to determine the best method for evaluating subcentimeter nodules.
Dual-time-point imaging has emerged as a potential discriminator of benign and malignant diseases, with images being obtained at 1 and 2 h after the administration of 18F-FDG. In a study involving in vitro samples and animal and human subjects, 18F-FDG uptake was measured over time; Zhuang et al. found that malignant lesions showed a significant increase in SUV over time and that benign lesions showed a decrease over time (34). Additional investigation has reached similar conclusions (35). One study compared single-time-point imaging and dual-time-point imaging with a cutoff SUV of 2.5 and a 10% increase in SUV for malignancy; the authors determined that the sensitivity and specificity of the tests were 80% and 94% (single) and 100% and 89% (dual), respectively (36). Pathophysiologically, the differences in levels of glucose-6-phosphatase and hexokinase within benign and malignant cells have been postulated as the reason for this effect (37). Although these studies appear promising, the use of dual-time-point imaging remains controversial. Further data are needed before widespread use can be recommended.
18F-FDG PET is known to show little uptake in malignancies with low metabolic activity. Focal bronchioalveolar cell carcinoma has been shown to have less proliferative potential and a longer mean doubling time than NSCLC (38,39). Further investigation has shown that different subtypes of bronchioalveolar cell carcinoma exhibit different rates of metabolic activity. Focal or pure bronchioalveolar cell carcinoma appears as a peripheral nodule or localized ground-glass attenuation and may show false-negative results on 18F-FDG PET (40). In contrast, the multifocal form appears as multiple nodules or ground-glass consolidation (40) and is detected at a relatively high sensitivity on 18F-FDG PET (41). Carcinoid is another malignancy that grows slowly and has low mitotic activity (42). The sensitivity of 18F-FDG PET for the detection of focal bronchioalveolar cell carcinoma and carcinoid tumor is lower than that for other cell types of lung cancer and has been reported to be as low as 50%.
Several groups have investigated the prognostic value of 18F-FDG PET (43–45). In a study of 155 patients with NSCLC, median survival was compared with the standardized uptake ratio (analogous to the SUV) of the primary tumor (43). Median survival decreased with increasing mean SUV. SUVs of less than 10 and greater than 10 indicated median survival times of 24.6 and 11.4 mo, respectively (Fig. 5). Furthermore, a mean SUV of greater than 10 with a tumor larger than 3 cm indicated a median survival of 5.7 mo. A retrospective study of 100 patients demonstrated that the 2-y survival rates were 68% for patients with a maximum SUV of more than 9 and 96% for those with a maximum SUV of less than 9 (45).
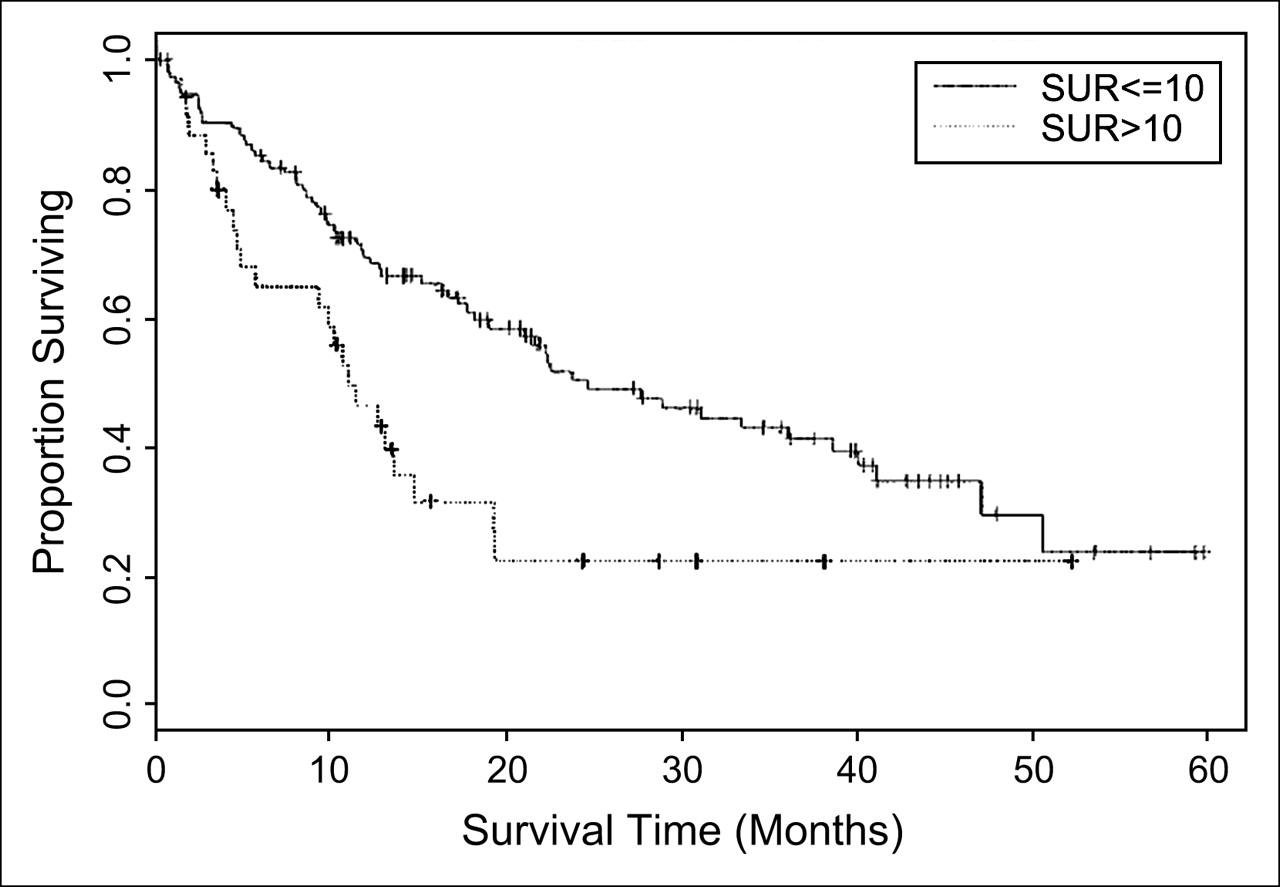
Survival among NSCLC patients stratified by standardized uptake ratio (SUR). (Reprinted with permission of (43).)
MULTIPLE PULMONARY NODULES
The evaluation of multiple pulmonary nodules can be limited by potential false-positive findings on 18F-FDG PET. Increased 18F-FDG activity has been demonstrated in instances of active granulomatous disease, such as tuberculosis, fungal disease, and sarcoidosis, as well as other inflammatory processes, such as rheumatoid nodules (46,47). CT in combination with 18F-FDG PET aids in the evaluation of multiple pulmonary nodules. In addition to the shapes, borders, and densities of the nodules, the distribution of the nodules can provide important clues to their etiology. There are 3 different distribution patterns: perilymphatic, random, and centrilobular. Perilymphatic nodules are located along the pleural surfaces, interlobular septa, and peribronchovascular interstitium, particularly in the perihilar regions and centrilobular regions. Random nodules have a more even and symmetric, yet random, distribution within the lung fields bilaterally. Centrilobular nodules spare the pleural surfaces and are associated with small pulmonary artery branches. There are 2 subcategories of centrilobular pulmonary nodules, those associated with and those not associated with tree-in-bud opacities. A tree-in-bud opacity is a branching opacity that represents filling of the alveolar spaces. This process typically occurs from an inflammatory or infectious process rather than a malignant process. The remaining nodular distributions are more often associated with malignancy and include lymphangitic spread of cancer with a perilymphatic pattern, hematogenous metastasis with a random distribution, and bronchioalveolar cell cancer with centrilobular opacities.
STAGING OF LUNG CANCER
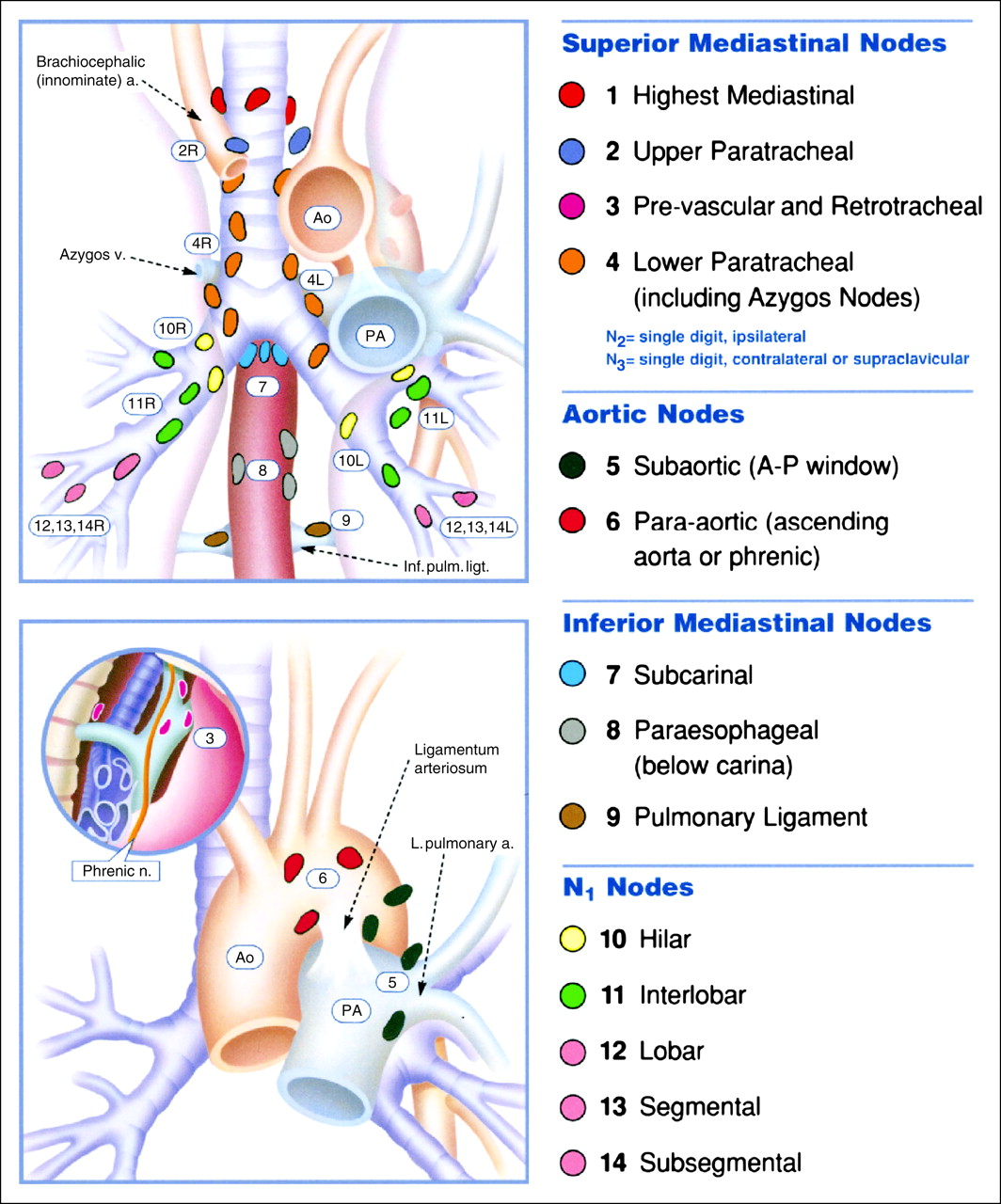
Before 1996, there were 2 mediastinal lymph node classification schemes. The 2 schemes were unified in 1996 by the American Joint Commission on Cancer and the Prognostic TNM Committee of the Union Internationale Contre le Cancer. As shown in Figure 6, thoracic lymph nodes can be organized into 4 groups: superior mediastinal, inferior mediastinal, aortic, and N1 nodes. These nodal groups can be divided further into anatomic lymph node regions or levels (Table 2) (48).
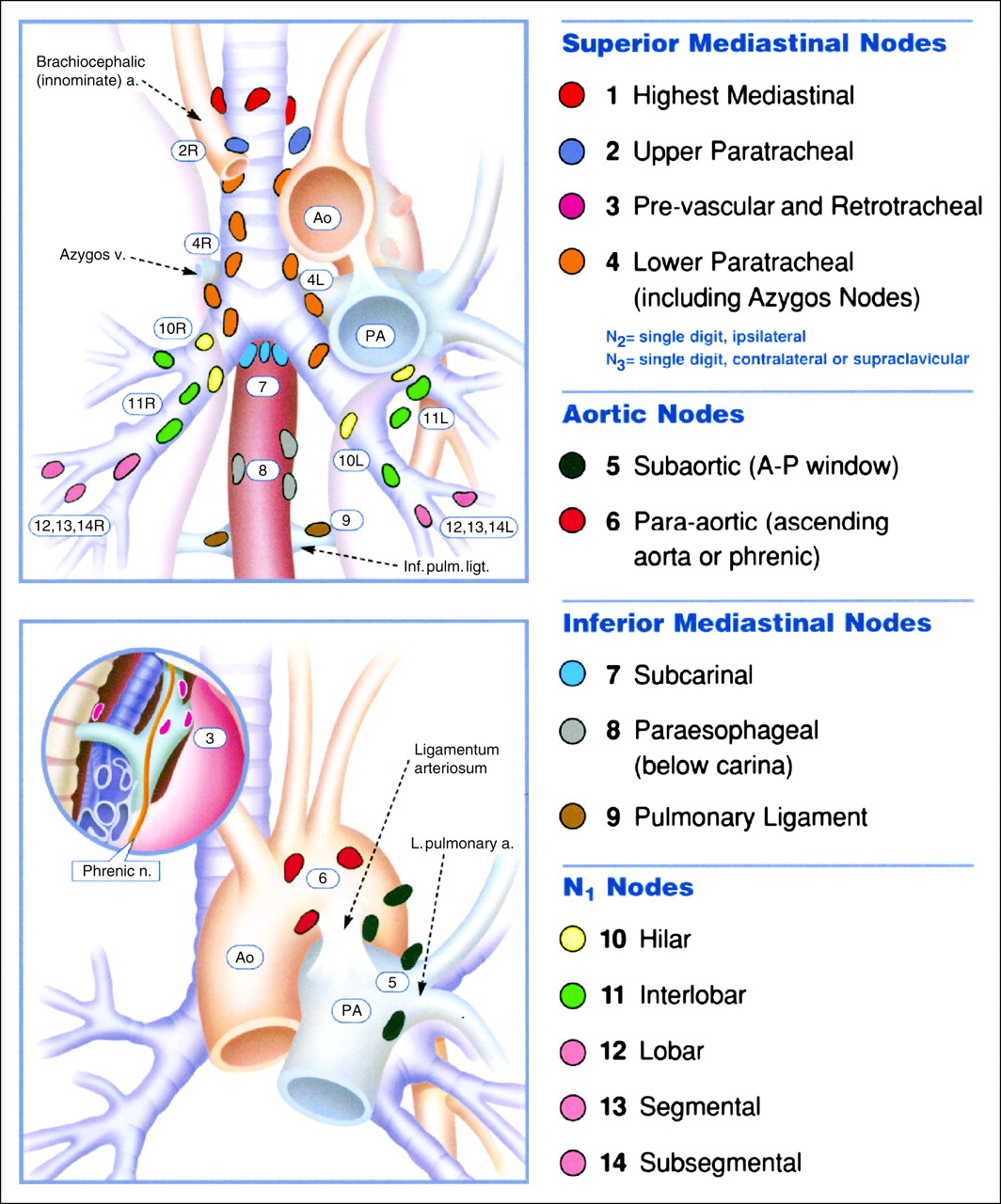
Thoracic lymph node stations. Subcategories include superior mediastinal nodes, aortic nodes, inferior mediastinal nodes, and N1 nodes (64). a. = artery; v. = vein; Inf. pulm. ligt. = inferior pulmonary ligament; Ao = aorta; PA = pulmonary artery; A-P = aortopulmonary; L. pulmonary a. = left pulmonary artery; Phrenic n. = phrenic nerve. (Reprinted with permission of (64).)
Lymph Node Map Definitions
One of the uses of this lymph node classification is to identify the proper method for lymph node sampling. Different invasive procedures typically are used for lymph node sampling; these include mediastinoscopy, video-assisted thoracic surgery (VATS), endoscopic sonography, and thoracotomy (Table 3) (49). Mediastinoscopy is best used for the evaluation of level 2, 4, and 7 lymph node stations. VATS can be used for multiple stations, depending on the approach, and is commonly used for level 5, 6, and 10 stations. Endoscopic sonography with transbronchial needle aspiration can be used for level 4–9 stations. All nodal groups can be reached by thoracotomy and potentially by CT-guided percutaneous needle biopsy.
Procedures Used to Sample Lymph Nodes, by Lymph Node Level
The location of the primary tumor determines the lymphatic pathway for spread to regional lymph nodes (50). A tumor in the right lung sends metastasis to hilar (10R) lymph nodes, which proceed to right paratracheal (4R and 2R) lymph nodes. Such a tumor rarely metastasizes to the contralateral side. A left upper-lobe cancer sends metastases to the aortopulmonary window (5) and left paratracheal nodes (4L). Left upper- and lower-lobelesions also may spread initially to left hilar (10L) lymph nodes. Involvement of prevascular (6) lymph nodes is almost invariably associated with paratracheal involvement. Tumors in the right middle lobe and bilateral lower lobes can metastasize early to subcarinal (7) nodes. Lower-lobe cancers also can send metastases to paraesophageal (8), pulmonary ligament (9), and subdiaphragmatic (14) lymph nodes.
CONVENTIONAL STAGING
The staging of malignancies with the TNM system was created to provide consistency in communication of the extent of disease, to provide a basis for the selection of therapy, and to help determine prognosis (51). The important decision in using this system is whether the disease is resectable. The T status classifies the features of the primary tumor. The N status classifies the presence or absence of regional lymph node involvement. The M status classifies the presence or absence of extrathoracic metastasis (Table 4).
TNM Classification of Lung Cancer
The T status evaluates the extent of the primary tumor by size and invasiveness. The current system describes the size of the tumor and its relationship with the pleura, bronchovascular structures, and mediastinum. A T1 lesion is defined as a tumor that is 3 cm or smaller (in the greatest dimension), with lung or visceral pleura separating the lesion from the mediastinum, but that does not extend proximally to the lobar bronchus. A T2 lesion is larger than 3 cm, invades the visceral pleura, and extends proximally to the lobar bronchus but does not extend to within 2 cm of the carina. Extension of the primary tumor into the mediastinum precludes curative surgical resection (52). The preservation of mediastinal fat planes or intervening lung between the tumor and the mediastinum is a clear indication that there is no direct extension into the mediastinum. Extension into the chest wall, diaphragm, mediastinal pleura or pericardium, or main bronchus is defined as a T3 lesion. The presence of T3 lesions does not necessarily preclude curative resection. Invasion of the mediastinum, vertebrae, and vital structures, such as the great vessels, trachea, esophagus, or heart, is classified as a T4 lesion and does preclude curative resection.
Lymph node status (N status) is integral to determining the resectability of a tumor; it describes the presence or absence and extent of regional lymph node metastasis. Metastasis to lymph nodes in the ipsilateral peribronchial or hilar regions is classified as N1 disease, a classification that alters the stage and prognosis of disease. The presence of N1 lymph nodes, however, does not preclude curative resection and does not accurately predict mediastinal lymph node involvement. Metastatic involvement of ipsilateral mediastinal lymph nodes is defined as N2 disease and represents at least stage IIIA disease. The presence of contralateral mediastinal, hilar, scalene, or supraclavicular lymph node involvement is defined as N3 disease and increases the patient's clinical stage to stage IIIB or higher. At stage III, evaluation of the mediastinum for either direct extension to vital structures or contralateral mediastinal lymph node disease determines resectability.
The CT evaluation of mediastinal lymph nodes has extremely variable sensitivity and specificity, with false-negative results of 7%−39% and false-positive results of 20%−45% (9). Size criteria alone are not very reliable in the staging of mediastinal lymph nodes (53,54). Lymph nodes of greater than 1 cm in the short axis are considered abnormal by CT criteria (55). Fifteen percent of patients with clinical stage I disease may have micrometastases in normal-size lymph nodes (56). Other morphologic features of lymph nodes are unlikely to be helpful in differentiating benign disease from malignant disease (57). Fat within a lymph node hilum is believed to be a sign of benignity. Adenopathy detected by CT is useful in directing invasive sampling techniques. Mediastinoscopy traditionally has been used for tissue diagnosis of mediastinal lymph node metastasis; however, additional techniques, such as transbronchial, percutaneous, or videoscopic biopsy, may be used when appropriate.
Evaluation of distant metastasis (M status) also is a critical step in determining the resectability of a tumor. M status defines the presence or absence of tumor spread to distant lymph node or organ sites. The brain, central nervous system, bone, liver, and adrenal glands are common sites for distant metastases, and such extension is considered to represent M1 disease (58). Metastases to the contralateral lung also are considered distant metastases. The radiologic workup for metastatic disease often begins with clinical history, physical examination, and laboratory studies. The frequency of occult metastasis at the time of presentation may be as high as 30% in patients with adenocarcinoma or large cell carcinoma of the lung (59). Squamous cell carcinoma of the lung appears to have a lower frequency of occult metastasis (<15%) at presentation. Routine radiologic evaluation for occult metastases without clinical or laboratory findings is not clearly indicated (60). The adrenal glands and liver are the most common sites for occult extrathoracic metastases. The adrenal glands occasionally may be the only sites for metastasis; however, incidental benign adenomas occur with a similar frequency in patients with bronchogenic carcinomas. Three to 5% of the overall population has incidental nonfunctioning cortical adenomas, whereas approximately 10% of patients with bronchogenic cancer have an adrenal mass on CT (61,62). In the absence of other known extrathoracic metastases, adrenal masses usually are benign. The liver usually is never the only site for metastasis, unless the primary malignancy is an adenocarcinoma. CT and MRI traditionally have been used for the evaluation of distant metastasis. Unenhanced CT followed by MRI is reported as the most cost-effective morphologic evaluation of suggestive adrenal lesions (63). Adrenal lesions that measure less than 10 HU on unenhanced CT are considered benign. Adrenal lesions that do not have CT signs of benignity are followed up with MRI with opposed-phase imaging. 18F-FDG PET is sensitive for the detection of adrenal metastases, but some benign adrenal adenomas may be abnormal on PET.
The International System for Staging Lung Cancer was developed in response to the need for a classification scheme to unify the variations in staging definitions and provide consistent meaning and interpretation for different stages. The value of this system in predicting prognosis relies on the identification of consistent and reproducible patient groups with similar outcomes. The International System for Staging Lung Cancer applies to all 4 major cell types of lung cancer: squamous cell, adenocarcinoma (including bronchioalveolar cell), large cell, and small cell. Multiple factors are directly related to the extent of disease at diagnosis; these include the proportion of patients achieving a complete response, the duration of the response, and recurrence after a complete response.
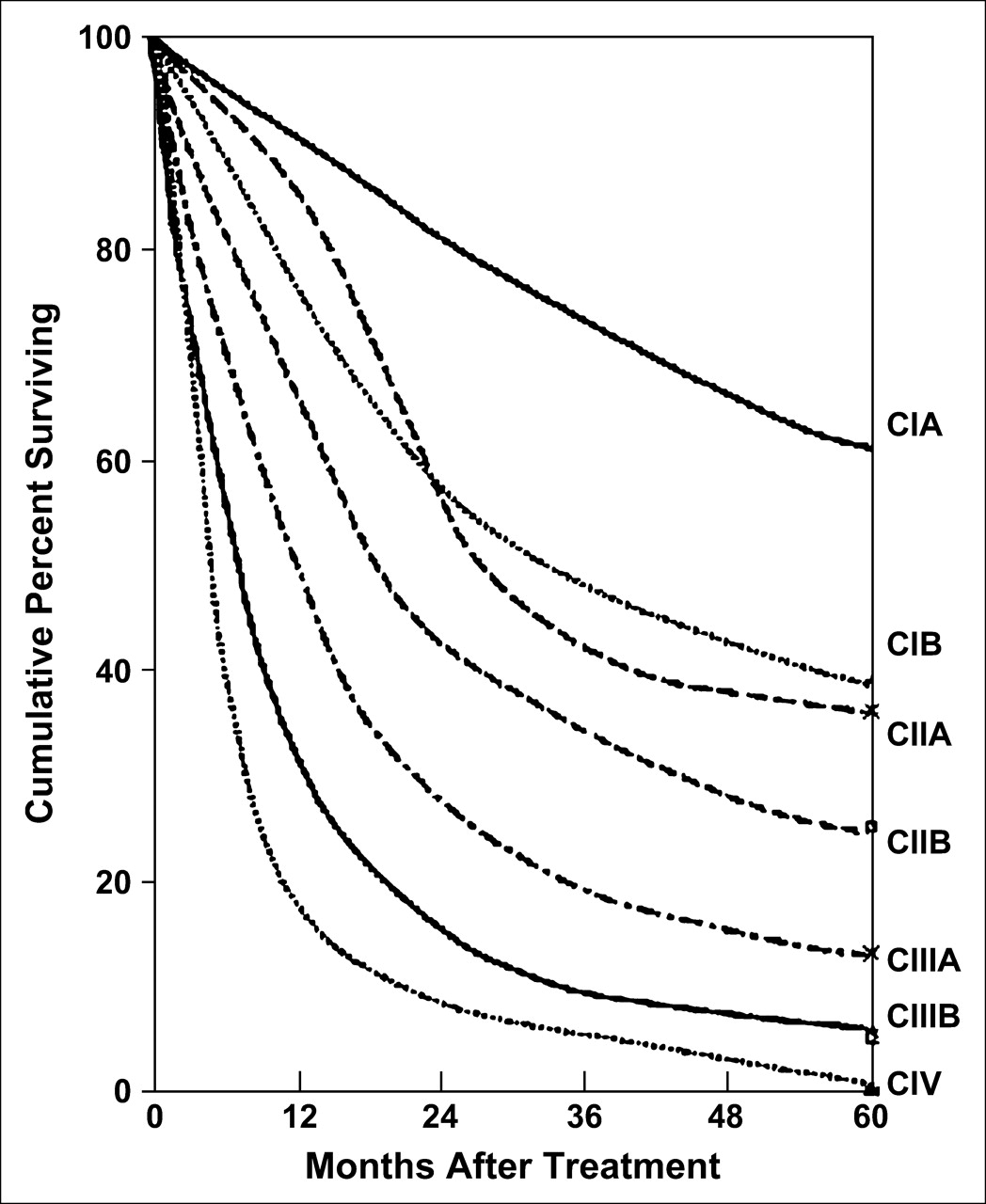
The TNM system is used to define 7 stages of disease (Table 5) (51). Stage IA includes small tumors of less than or equal to 3 cm, without invasion proximal to a lobar bronchus, and without metastasis. Stage IB includes larger tumors, tumors with invasion of the visceral pleura or main bronchus (>2 cm distal to the carina), or both, and tumors without metastasis. There is a significant difference in survival between IA disease and IB disease, with 5-y survival rates of 61% and 38%, respectively (64). Stage IIA includes T1 tumors with metastases to ipsilateral peribronchial lymph nodes, hilar lymph nodes, or both. These metastases are difficult to document radiographically. Stage IIB includes T2 lesions with metastases to ipsilateral peribronchial lymph nodes, hilar lymph nodes, or both and T3 tumors without metastasis. The 5-y survival rates for stage IIA and stage IIB are 37% and 24%, respectively (64). Stage IIIA includes T3 tumors with metastases to intrapulmonary lymph nodes, hilar lymph nodes, or both (N1). T1 through T3 tumors with ipsilateral mediastinal lymph node metastases (N2) also are included in IIIA disease. This stage includes limited invasion of the mediastinum or chest wall (T3). Such lesions have an improved outcome and are potentially resectable if vital structures in the mediastinum are not involved. Stage IIIB involves extensive extrapulmonary involvement, with invasion of the mediastinal structures, esophagus, trachea, carina, heart, major vessels, or vertebral bodies. An associated pleural effusion also is considered to represent stage IIIB disease. No distant metastatic disease is present. This stage of disease is virtually always nonresectable (9). The 5-y survival rates for stage IIIA and stage IIIB are 9%−13% and 5%, respectively (Fig. 7) (64). Stage IV includes any T status and N status with distant metastases. Non–lymph-node metastases in ipsilateral lobes not involved by the primary tumor also are considered stage IV disease. Stage IV disease is considered a contraindication to surgical resection (9). As expected, survival with stage IV disease is poor, with less than 1% survival at 5 y (64).
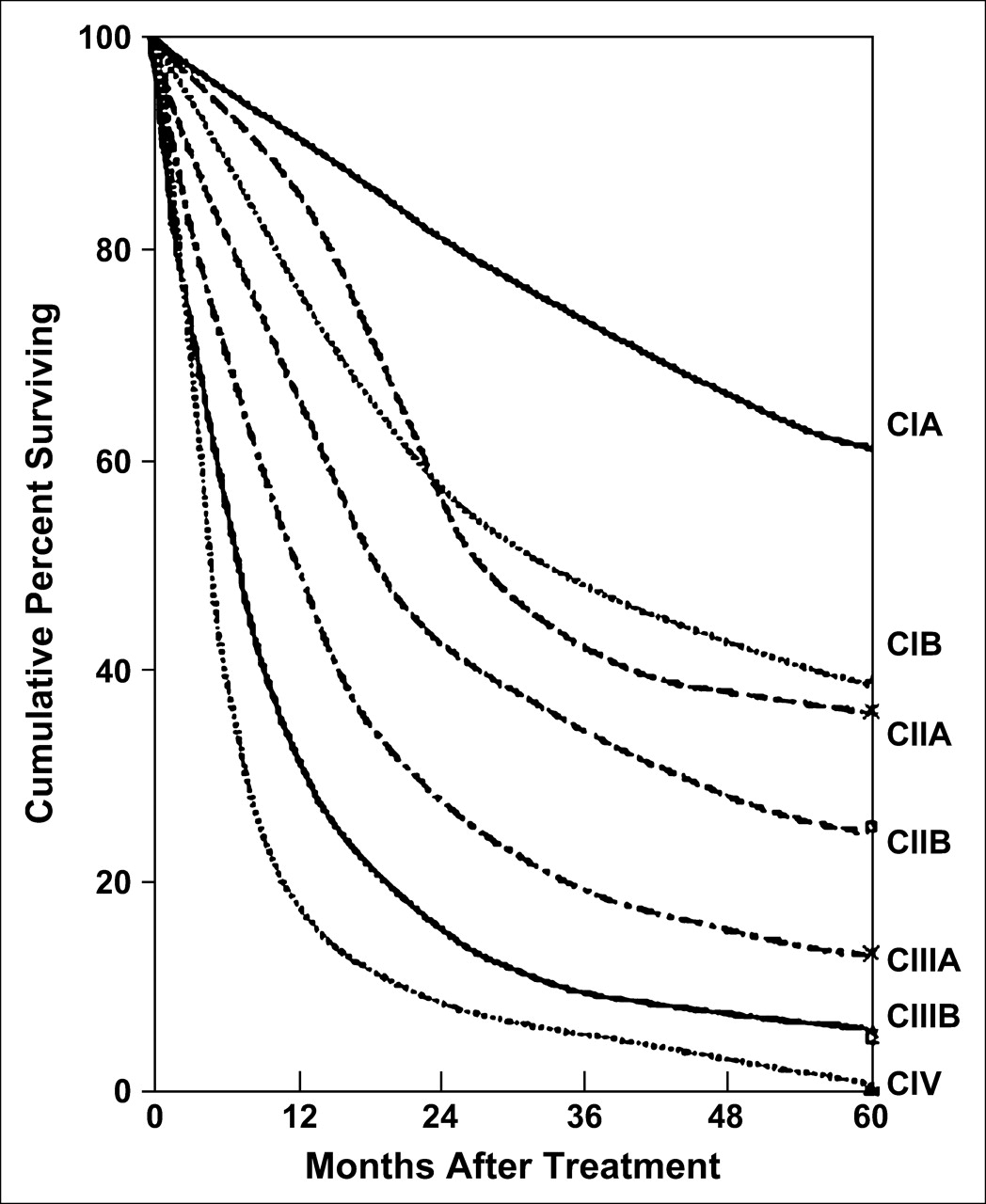
Patient survival in relation to stage of disease. c = clinical stage. (Reprinted with permission of (51).)
International Staging System for NSCLC, Including Stage Groups and TNM Subsets
COMBINING CONVENTIONAL STAGING WITH METABOLIC IMAGING
As a measure of metabolic activity, 18F-FDG PET adds a functional evaluation to the staging of lung cancer. The PET in Lung Cancer Staging trial attempted to determine the value of 18F-FDG PET in lung cancer staging (65). The goal was to determine whether unnecessary surgery could be reduced. The researchers enrolled 188 patients in a randomized controlled trial comparing a conventional radiologic staging workup (CWU) to CWU and PET. The conclusions of the study were that the addition of PET to CWU prevented unnecessary surgery in 1 of 5 patients with suspected NSCLC. In addition, the staging of disease was increased for 27% of patients. The researchers believed that the negative predictive value of PET for mediastinal lymph node involvement was sufficiently high to avoid mediastinoscopy for noncentral tumors. Another prospective study of 102 patients went further to conclude that invasive procedures probably are not necessary in a patient with negative findings on PET for the mediastinum (66). In that study, the sensitivity and specificity of PET in detecting mediastinal lymph node metastasis were 91% and 86%, respectively.
The high negative predictive value of PET led some institutions to accept negative PET results without pathologic confirmation and to proceed to curative surgical resection. This management scheme has led to much controversy with regard to the role of PET in mediastinal staging. Although the PET in Lung Cancer Staging study demonstrated a clear benefit of PET in predicting disease, the results may not be generalizable to other populations (67). The accuracy of clinical evaluation for distant metastasis in NSCLC has been investigated for each stage of the disease. These studies reported a 5% false-negative rate for the clinical evaluation of stage I and II diseases (68–70). The false-negative rate for stage III disease was reported to be 15%−20%. Without clinical evidence of distant metastatic disease, mediastinal involvement becomes a crucial issue in determining the stage of the disease. CT evaluation of the mediastinum has a false-negative rate of 15% overall; the false-negative rate increases to 20%−25% for central lung tumors (71,72). A meta-analysis of the diagnostic performance of PET versus CT for mediastinal staging was performed by Dwamena at al. (73). For 14 PET and 29 CT case series, they determined that PET was statistically superior to CT for mediastinal staging. With respect to CT, PET has been shown to have a higher negative predictive value, and combined PET/CT has an even higher negative predictive value (49,74–76).
The use of PET to exclude mediastinal metastasis remains controversial. From the data available, classification of disease as stage I on the basis of a clinical examination and negative results from CT and PET examinations appears sufficient to exclude mediastinal disease. Classification of stage II and III diseases is more controversial; the negative predictive value of PET decreases in relation to the size of the metastasis, the presence of centrally located primary disease or N1 nodes, and the avidity of the primary tumor for 18F-FDG (77,78). Micrometastatic disease cannot be imaged effectively on PET because of the spatial resolution of the imaging system (79,80). Takamochi et al. found that the diameters of false-negative lesions ranged from 1 to 7.5 mm (80). In addition, the presence of hypermetabolic central tumors or hilar lymph nodes can decrease the detectability of mediastinal lymph nodes and thus the negative predictive value of mediastinal PET (78). Finally, the metabolic activity of low-grade malignancies cannot be expected to be any greater than that of the primary tumor (77). Mediastinal activity is a source of potential error attributable to random inhomogeneity and misregistration from respiratory, cardiac, and body motions. For stage II and III diseases, the incidence of false-negative results is still greater with PET than with mediastinoscopy. In a comparative study, the false-negative rates of mediastinoscopy and PET were 3% and 11.7%, respectively (81). Mediastinoscopy likely will remain part of the standard protocol for mediastinal staging for stage II and III diseases. The clinical importance of differentiating stage IIIA and IIIB diseases, with regard to denying curative resection, is a significant factor in the continued use of mediastinoscopy. Several studies have demonstrated the potential of PET to alter patient management (82–84). Hicks et al. found that PET caused a major management change in 40 of 63 patients (63%) who had previously undergone potential curative surgery for NSCLC (82). Seltzer et al. demonstrated that PET changed the staging of lung cancer in 44% of cases (83). The use of PET in stage IV disease is less of an issue for mediastinal staging, as the patient's N status is no longer relevant. The use of PET in stage IV disease will be discussed further with regard to identifying and monitoring distant metastasis.
Because 18F-FDG describes metabolic activity, it cannot distinguish malignancy from inflammation or infection. 18F-FDG uptake is demonstrated in sites of active acute inflammation because of increased glucose uptake by activated macrophages and inflammatory cells (85). Multiple studies have demonstrated a positive predictive value for PET of 74%−93% for evaluation of the mediastinum (66,86). A study comparing PET and mediastinoscopy evaluations of 202 patients showed a positive predictive value for PET of 44.6% (81). The high rate of false-positive results demonstrates the necessity for mediastinoscopy in the staging of PET-positive mediastinal lymph nodes (80,87). The added benefits of PET in this setting include the ability to direct mediastinal lymph node biopsy and to aid in selecting additional invasive methods for lymph nodes inaccessible to mediastinoscopy (Table 3).
STAGING OF SMALL CELL LUNG CANCER (SCLC)
SCLC represents approximately 18%−25% of all cases of lung cancer (88,89). SCLC is a neuroendocrine tumor that has an aggressive growth pattern, that commonly displays early widespread metastases, and that has a rapid tumor doubling time (90). Consequently, patients often present with bulky hilar and mediastinal lymph node metastases (91). The tumors usually are located centrally (89,92), often with encasement of mediastinal structures and tracheobronchial compression (91,93). The primary tumor may be small or undetectable by radiographic methods, whereas early extrathoracic metastases are common and can present before clinical symptoms (94,95). Unlike the situation for NSCLC, there is a 2-stage classification scheme proposed by the Veterans Administration Lung Cancer Study Group. Patients with SCLC are classified as having either limited or extensive disease (96). Limited disease refers to tumor that is confined to the thorax. Extensive disease includes distant metastases, including those to the contralateral lung. Whether 18F-FDG PET has a role in the staging of SCLC is controversial. Detterbeck et al. stated that the clinical presentation and radiographic appearance are sufficiently characteristic of the disease to eliminate the need for further confirmation (97). A few studies have been performed to compare the staging of SCLC by conventional radiography with that by 18F-FDG PET. PET changed patient management in 8.3%−29% of these cases (98–101). Patients with limited disease were given chemoradiation, whereas patients with extensive disease were given chemotherapy alone. The available studies show a possible role for 18F-FDG PET in the staging of SCLC; however, further study is necessary to evaluate the clinical necessity.
COST-EFFECTIVENESS OF STAGING BY PET
The cost-effectiveness of PET for the staging of NSCLC has been extensively studied in multiple health care systems. Cost-effectiveness is analyzed with respect to the cost of patient care and life expectancy. The incremental cost-effectiveness ratio quantifies the difference in cost for different therapeutic strategies versus the difference in life expectancy (102). A study comparing 5 different clinical strategies was performed with Medicare reimbursements in the United States as the basis for the cost analysis. Conventional CT staging followed by biopsy and surgical versus nonsurgical therapy was compared with 4 strategies integrating PET. Three strategies used confirmatory biopsy before diverting patients from curative resection. The final strategy eliminated confirmatory biopsy and proceeded to surgical or nonsurgical therapy. That study demonstrated that the most cost-effective strategy involved the use of PET for CT evaluations with negative results followed by confirmatory biopsy. The strategy involving the elimination of confirmatory biopsy after CT and PET evaluations with positive results had the lowest cost but also the lowest life expectancy (103). A direct comparison of the cost-effectiveness of PET for demonstrating additional or unanticipated results using PET with confirmatory mediastinoscopy and PET with selective mediastinoscopy demonstrated a savings in both instances. Selective mediastinoscopy showed approximately double the cost savings per patient ($2,267 vs. $1,154) but missed 1.7% of patients who might be cured (104). A comparison of cost-effectiveness in other health care systems is more difficult because of the use of different therapeutic strategies. A study of the French health care system involved a significant difference in staging strategies (105). The therapeutic strategies in that study did not mandate confirmatory biopsy before surgical or nonsurgical therapy. That study determined that the most cost-effective strategy involved the use of PET after a CT examination with negative or positive results. The PET results then were used to make decisions regarding biopsy, surgery, or chemotherapy. Similar findings were demonstrated in studies of the Italian (29), Canadian (106), and German (107) health care systems. Irrespective of the use of mediastinoscopy, PET for the evaluation of mediastinal disease in NSCLC has been shown to be cost-effective in several health care models.
DETECTION OF DISTANT METASTASIS
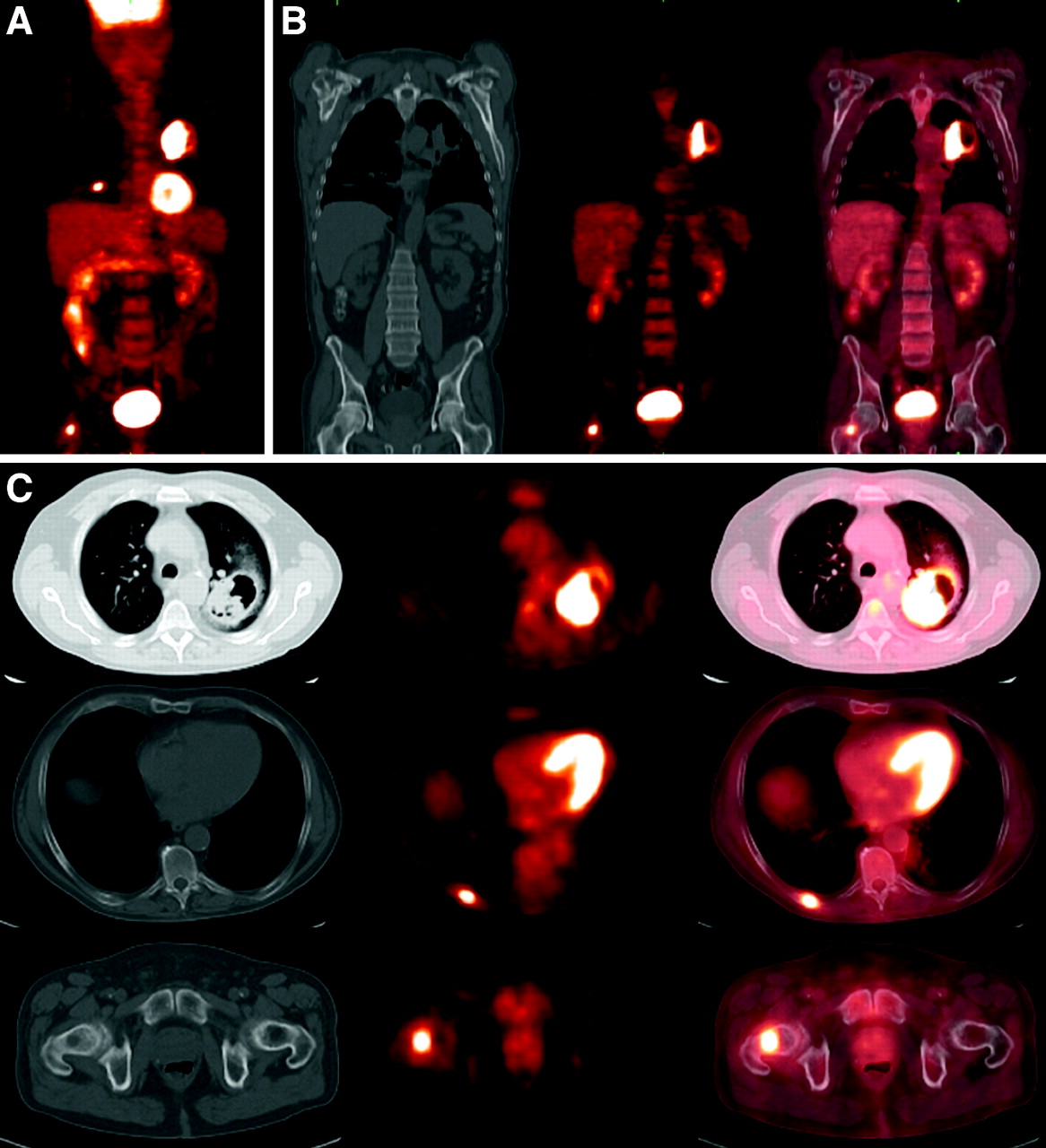
The presence of distant metastasis is classified as stage IV disease, which precludes a patient from the possibility of curative surgical resection. The patient therefore is prescribed palliative therapy. An inherent advantage of PET is the use of whole-body scanning, which facilitates the survey of a much larger area than is possible with commonly used radiographic methods (Fig. 8). Distant metastases commonly involve the adrenal glands, bones, liver, and brain (108). Multiple studies have demonstrated the ability of 18F-FDG PET to detect distant metastasis of lung cancer with greater specificity than can conventional imaging, including CT (109). The mean frequency of extrathoracic metastases in these studies was 13%. In 18% of the cases, the PET results altered management. As expected, the frequency of distant metastases was shown to increase with higher stages: 7.5% in stage I, 18% in stage II, and 24% in stage III (110).
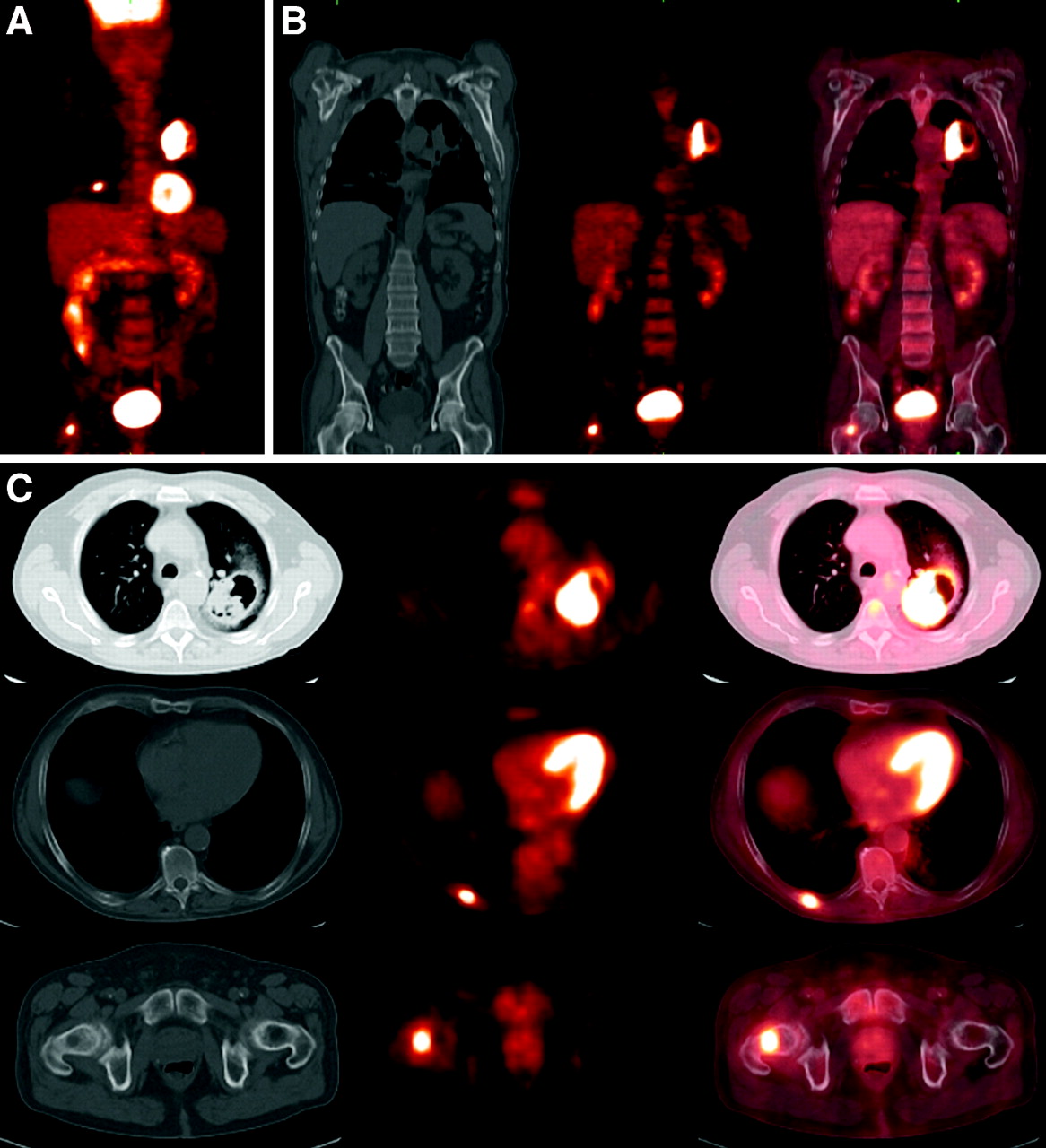
Lung cancer with osseous metastases. Hypermetabolic cavitary lung mass is seen in left upper lobe (A–C). Maximum-intensity-projection image (A) demonstrates additional lesions in contralateral thorax and hip. Additional focus of hypermetabolism is seen in right femoral neck (A–C) and corresponds to subtle lytic lesion on CT. Axial images (C) show hypermetabolism in right posterior 8th rib without osseous changes on CT.
As discussed earlier, the adrenal glands and liver are the most common sites of extrathoracic metastases in lung cancer. At the time of presentation, up to 10% of patients will have an adrenal mass. Approximately two thirds of these masses will be benign (111,112). In a study of 27 patients with 33 adrenal masses, the ability of PET to differentiate benign from malignant adrenal masses was investigated (113). The sensitivity of PET for detecting adrenal metastasis was 100%, and the specificity was 80%. A subsequent study of adrenal lesions demonstrated a sensitivity of 100%, a specificity of 94%, and an accuracy of 96% for detecting metastasis (114). The evaluation of liver metastasis by PET is less well studied. Liver metastases are rarely the only demonstrable site of metastatic disease (9).
In a study of 110 patients with NSCLC, 18F-FDG PET was compared with methylene diphosphonate bone scanning for the evaluation of bone metastases (115). 18F-FDG PET had a higher specificity for detecting bone metastases (98% vs. 61%). Some additional studies demonstrated a higher specificity (116,117), and some demonstrated a higher accuracy (115,118,119). Marom et al. (120) found that, compared with bone scintigraphy, 18F-FDG PET had a higher sensitivity but an equivalent specificity for 90 patients who underwent both studies. Fogelman et al. (121) reviewed the literature on this topic and concluded that, with regard to lung cancer, 18F-FDG PET had a sensitivity similar to that of bone scintigraphy but a specificity higher than that of bone scintigraphy. The practical advantage of 18F-FDG PET over bone scintigraphy remains controversial. Mechanistically, there are different patterns of uptake related to the morphology of the lesion: lytic, sclerotic, or mixed (121). As demonstrated in a study of breast cancer patients with bone metastases, 18F-FDG PET appears to have the advantage of detecting osteolytic lesions, whereas bone scintigraphy has the advantage of detecting osteoblastic lesions (122).
The detection of brain metastasis by PET also has been evaluated. In a study of 1,026 patients with multiple different malignancies, unsuspected cerebral or skull metastases were detected in only 0.4% of the patients (123). PET is less effective than CT or MRI for the detection of cerebral metastasis.
RESTAGING
The benefit of determining a metabolic response to therapy over a morphologic response has led to the investigation of PET for the restaging of NSCLC. The criteria for conventional restaging were determined by the World Health Organization and later modified by the National Cancer Institute and the European Association for Research and Treatment of Cancer. Tumor response is defined as a therapy-induced reduction of the largest dimension of the tumor by 30% (124). Complete and partial responses are determined by the amount of tumor size reduction. Measuring and evaluating the morphologic response to therapy is less than ideal. A morphologic response to therapy usually occurs over several weeks to months. During the interim, patients with nonresponding tumors are treated without benefit. In addition, morphologic evaluation can be inaccurate because of peritumoral scar tissue formation and edema, which can mask tumor regression (125).
PET has been investigated in 3 different scenarios: restaging after neoadjuvant therapy, early assessment of response to therapy, and restaging after completion of therapy. In the first scenario, PET could be used after induction chemotherapy or chemoradiation to evaluate for tumor resectability. Few studies have been performed to investigate the reliability of PET in assessing mediastinal “downstaging.” From the studies that are available, it appears that there is much variability in the results (97). Studies evaluating for a complete pathologic response appear to have high false-positive and false-negative rates (126–129). The second scenario was investigated in a study of 57 patients who were evaluated by PET 1 wk before and 3 wk after the first cycle of chemotherapy (130). It was found that a reduction in metabolic activity correlated closely with the final outcome of the therapy. An early metabolic response predicted better survival, and a poor response predicted disease progression within the first 3 cycles of chemotherapy. The impact of this evaluation on the morbidity and cost of nonresponding tumors suggests much merit in this strategy. The third scenario is the most commonly performed scenario for restaging. Multiple studies have demonstrated a high specificity for the characterization of viable tumor and scar tissue after therapy (109). Furthermore, Patz et al. have shown that 18F-FDG PET has prognostic value and correlates strongly with rates of survival of patients with treated lung cancer; patients with positive 18F-FDG PET results have a significantly worse prognosis than patients with negative results (131). Hicks et al. demonstrated a significant impact of PET on further management, with major changes being made in 63% of studied cases (82).
RADIATION THERAPY PLANNING
Radiation therapy currently involves CT-based planning to provide radiation selectively to a tumor. In lung cancer, the chest is a critical area for treatment planning because of the vital structures in close proximity to treatment ports. Limiting radiation strictly to tumor tissue may be nearly impossible, and nontarget tissues are inevitably affected. PET has been investigated for refining treatment volumes for the purpose of limiting them to allow an increase in dose to target tissues and a reduction in toxicity to nontarget tissues. In a retrospective study of 34 patients, Nestle et al. determined that the use of PET would have led to a substantial reduction in the size of radiation portals (132). Multiple studies have demonstrated significant changes in target volumes after planning with PET (133–137).
PLEURAL DISEASE
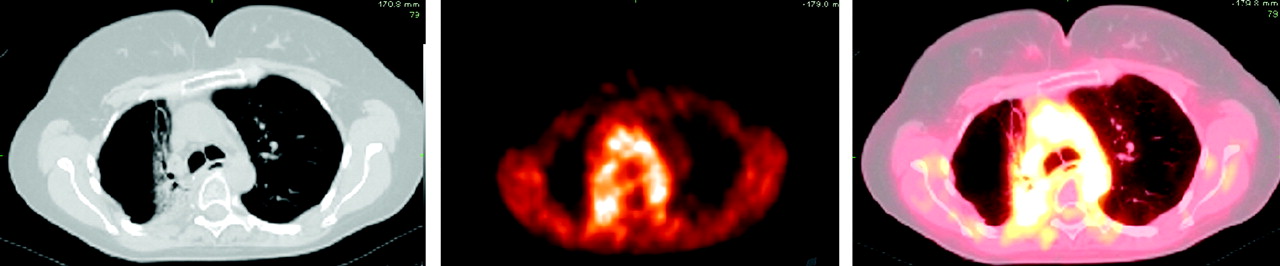
18F-FDG PET has been used to evaluate pleural fluid and pleural masses for evidence of malignancy. Erasmus et al. evaluated 25 patients with suspected malignant pleural effusions (138). They reported the sensitivity, specificity, and positive predictive value to be 95%, 67%, and 95%, respectively. With a high positive predictive value, 18F-FDG PET is likely to improve staging in patients with NSCLC. A later study of 92 patients compared the utility of 18F-FDG PET with that of CT in the differentiation of benign from malignant pleural effusions (139). A total of 71% of pleural effusions seen on CT were indeterminate for malignancy. With 18F-FDG PET, the sensitivity, specificity, and positive predictive value were 100%, 71%, and 63%, respectively. The difference in positive predictive values may be attributable to the larger number of benign pleural effusions included in the more recent study. Despite some differences in results, 18F-FDG PET was found to be useful for the evaluation of suspected malignant pleural effusions (Fig. 9). 18F-FDG PET likely will provide information complementary to that obtained with other methods, because the results of fluid cytologic analysis have been reported to be positive for only 66% of malignant pleural effusions from NSCLC (140).

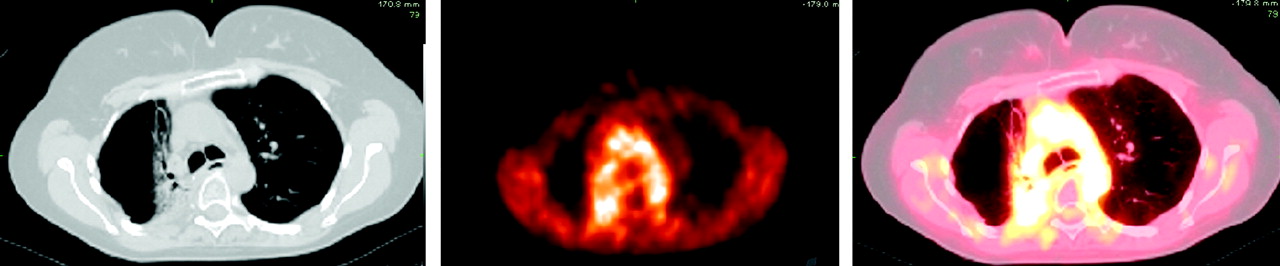
Malignant pleural effusion in right hemithorax. Hypermetabolism is associated with this effusion, consistent with malignant pleural effusion.
CT is commonly used to diagnose, stage, and monitor treatment response for malignant pleural mesothelioma (MPM). The CT findings associated with mesothelioma include a unilateral pleural effusion, nodular pleural thickening, interlobar fissure thickening, and tumor invasion of the chest wall, mediastinum, and diaphragm (141). In a study of 20 patients, CT was shown to have limitations in the evaluation of chest wall, transdiaphragmatic, and peritoneal involvement, as well as mediastinal involvement (142). Several studies have demonstrated a sufficient elevation in 18F-FDG accumulation within malignant pleural mesotheliomas to distinguish benign from malignant pleural disease (143–146). In a study of 15 patients with MPM, the impact of PET on staging was evaluated (147). For 13% of patients, the staging of disease was increased, whereas for 27% of patients, the staging of disease was decreased, leading to the conclusion that 18F-FDG PET played a worthwhile role in staging. Erasmus et al. evaluated the role of PET/CT in patients who had MPM and who were being evaluated for surgery (extrapleural pneumonectomy) (148). That study of 29 patients determined that PET/CT can improve the accuracy of M staging, resulting in a more appropriate selection of surgical candidates. Erasmus et al. found limitations of PET in T staging and N staging. Further investigation is necessary to determine the specific uses of PET in the staging of MPM. In addition to staging, 18F-FDG PET may be useful in the prognosis of patients with MPM. Flores evaluated the risk of mortality from MPM in 65 patients and determined that patients with tumors with an SUV of greater than 4 had a 3.3-fold greater risk of death than did patients with tumors with a lower SUV (149).
EVALUATING PET SCANS
In the examination of thoracic PET studies, it is helpful to review regions of physiologic 18F-FDG uptake, normal variants, and nonmalignant causes of 18F-FDG uptake. Areas directly relevant to thoracic PET include the neck, thorax, and upper abdomen. Table 6 describes potential false-positive findings on 18F-FDG PET. Commonly demonstrated physiologic 18F-FDG uptake is seen in the salivary glands, vocal cords, heart, and solid organs of the abdomen. 18F-FDG uptake has been demonstrated within the walls of the aorta and great vessels. This finding correlates with the patient's age and hypercholesterolemia and may represent areas of atherosclerosis (150–152). The esophagus may show physiologic 18F-FDG uptake or uptake within areas of esophagitis, Barrett's esophagus, and gastroesophageal reflux (153). The thymus typically shows physiologic 18F-FDG uptake in children less than 13 y old. Uptake within the thymus also can be seen after chemotherapy (154). Thymic hyperplasia is thought to be due to chemotherapeutic drugs causing increased uptake in patients up to 30 y old (155). Physiologic muscular uptake can occur from muscular contraction during tracer uptake. Commonly observed muscular uptake occurs in the trapezius, scalenius, genioglossus, sternocleidomastoid, paraspinal, and diaphragm muscles. Hickeson et al. showed that patients with chronic obstructive pulmonary disease may be predisposed to having thoracic and abdominal muscular uptake (156). Diffuse muscular uptake can be caused iatrogenically. The administration of insulin before the injection of 18F-FDG causes diffusely increased skeletal muscle uptake (157). Brown fat is a well-described site of physiologic 18F-FDG uptake commonly located in the cervical, axillary, paravertebral, mediastinal, and abdominal regions. The distribution usually is bilateral and symmetric but may be asymmetric and focal (158). Joints and bone may show 18F-FDG uptake from inflammatory or arthritic processes (159). Abnormal bone uptake also can be shown from benign and malignant bone tumors, osteomyelitis, acute fractures, Paget's disease, bone infarcts, pseudofractures, and poststernotomy wounds (160). Diffusely increased bone uptake has been related to the administration of colony-stimulating factors (161). Multiple iatrogenic causes of 18F-FDG uptake have been reported; these include axillary nodal uptake from the infiltration of an 18F-FDG dose and pericatheter uptake from tracheostomies, central venous catheters, chest tubes, gastrostomy tubes, and other drainage tubes. Various interventions can produce uptake in healing wounds; these include sternotomy, needle biopsies, mediastinoscopy, thoracotomy, and talc pleurodesis (Fig. 10). Radiation has been shown to produce pneumonitis (Fig. 11) as well as esophagitis. Asymmetric vocal cord uptake may be caused by paralysis of one of the vocal cords by compression of the recurrent laryngeal nerve. One of the treatments for vocal cord paralysis, which involves Teflon (DuPont) injection, also may cause focal 18F-FDG uptake (162).

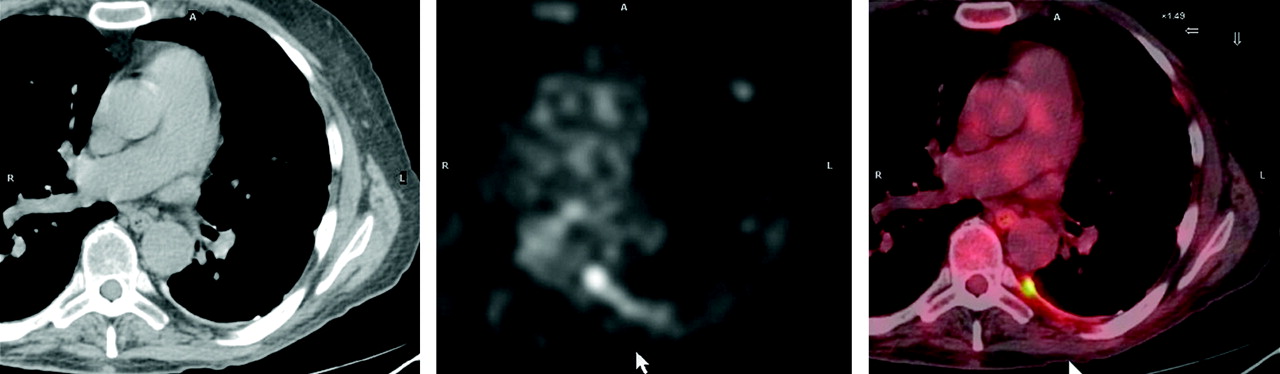
Pleurodesis. CT demonstrates left posterior pleural thickening. Hypermetabolism is associated with this area of pleural thickening. Additional sites of pleural hypermetabolism were seen throughout left pleural space on whole-body images. Patient had had pleurodesis in past, consistent with current findings.
Radiation pneumonitis. Heterogeneous opacities demonstrated in a “geometric configuration” (straight edges) within medial right lung correspond to radiation therapy portal. Associated hypermetabolism is seen.
Possible Causes of False-Positive Findings in 18F-FDG PET Studies in Chest
TUMOR EVALUATION
A qualitative comparison of tumor uptake may be sufficient to determine whether viable tumor is present after therapy. A quantitative analysis may be necessary during treatment to predict subsequent tumor response (125). Table 7 lists the factors involved in the tumor uptake of 18F-FDG. Multiple other factors, aside from tumor metabolism, affect 18F-FDG uptake (163,164). The partial-volume effect resulting from the limited spatial resolution of PET causes an underestimation of the true activity present. It has been shown that only 60% of maximal activity is measured in a lesion at 1.5 times the spatial resolution of the PET camera. Only at 4 times the spatial resolution does the difference between measured peak activity and true activity become less than 5% (165). The processing or “smoothing” of images with a gaussian filter also decreases image resolution and apparent 18F-FDG uptake.
Factors That Can Affect Measured 18F-FDG Uptake Within Tumors (125)
Tumoral uptake of 18F-FDG increases with increasing time between injection and scanning. Glucose levels cause changes in 18F-FDG uptake because of direct competition with glucose for accumulation. Finally, 18F-FDG is not identical to glucose. 18F-FDG and glucose differ in rates of phosphorylation, transport, and volume of distribution. To quantify the rate of metabolism of glucose, a conversion factor is used, but this constant also varies with the type of tissue examined. Table 8 summarizes the common sources of SUV measurement error.
Common Sources of Errors in Measurement of SUV (125)
FUTURE DIRECTIONS
As alluded to previously, there are multiple avenues of investigation that could be used to improve the ability of PET to diagnose and stage malignancies. One avenue that has received attention is improving the coregistration of lung tumors on PET/CT. In a study of 8 patients with 13 thoracic tumors, the researchers compared the SUVs of the tumors determined by attenuation correction with conventional helical CT (HCT) versus averaged CT with respiratory gating (ACT) (166). A difference of greater than 50% in the maximum SUV was demonstrated between the HCT and the ACT data for 4 of the 13 tumors. A significant reduction in diaphragmatic misregistration also was found with the ACT images. The researchers concluded that ACT provides a more accurate attenuation map for SUV quantitation. Further investigation is warranted, but it appears that respiratory gating provides potential improvements in quantitative and qualitative evaluations of thoracic malignancies.
A second avenue of investigation involves image processing and display formats for enhanced reader detectability. In a study of 15 patients with 21 intraluminal tumors, the researchers compared the detectability and localization of these lesions by conventional PET/CT and PET/CT virtual bronchoscopy and colonography (167). The data demonstrated 100% detection of lesions on virtual 3-dimensional images versus axial images and demonstrated subjective improvements. This initial work shows the potential improvement that can be obtained in detectability and localization by use of 3-dimensional display modes with fused PET/CT images.
A third avenue of investigation is the determination of the potential benefit of other PET radiotracers compared with the benefit of 18F-FDG. Other radiotracers, such as 18F-fluorothymidine (18F-FLT) and 18F-fluorocholine (18F-FCH), are being investigated for use in lung cancer. Buck et al. (168) compared the diagnosis and staging of lung cancer with 18F-FDG and 18F-FLT in 43 patients. They concluded that 18F-FLT had a higher specificity for malignant lung tumors; however, 18F-FLT was less accurate for N staging and M staging. Cobben et al. (169) compared 18F-FLT and 18F-FDG in 17 patients with NSCLC. 18F-FLT demonstrated a significantly lower maximum SUV in NSCLC than did 18F-FDG. They concluded that 18F-FLT was not useful in the staging or restaging of NSCLC. Similarly, 18F-FCH has been compared with 18F-FDG as a potentially useful tumor imaging agent. Tian et al. (170) compared 18F-FCH and 18F-FDG in 38 patients with various tumors, including 6 patients with lung cancer. They found similar radiotracer uptake in the known tumors, without clear improvement with 18F-FCH over 18F-FDG. Neither 18F-FLT nor 18F-FCH has shown clear improvement over 18F-FDG at this time; therefore, they have no role at present.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH MARCH 2007.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.
- 100.
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.
- 128.
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.
- 135.
- 136.
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.
- 145.
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- Received for publication November 1, 2005.
- Accepted for publication January 20, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- CONVENTIONAL IMAGING OF LUNG NODULES
- 18F-FDG PET FOR EVALUATION OF SOLITARY PULMONARY NODULES
- MULTIPLE PULMONARY NODULES
- STAGING OF LUNG CANCER
- CONVENTIONAL STAGING
- COMBINING CONVENTIONAL STAGING WITH METABOLIC IMAGING
- STAGING OF SMALL CELL LUNG CANCER (SCLC)
- COST-EFFECTIVENESS OF STAGING BY PET
- DETECTION OF DISTANT METASTASIS
- RESTAGING
- RADIATION THERAPY PLANNING
- PLEURAL DISEASE
- EVALUATING PET SCANS
- TUMOR EVALUATION
- FUTURE DIRECTIONS
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Quantitative Accuracy and Lesion Detectability of Low-Dose 18F-FDG PET for Lung Cancer Screening
- Serum Angiopoietin-2 as a Clinical Marker for Lung Cancer in Patients with Solitary Pulmonary Nodules
- The Effectiveness of 18F-FDG PET/CT Combined with STIR MRI for Diagnosing Nodal Involvement in the Thorax
- Evaluation of Dual-Time-Point 18F-FDG PET for Staging in Patients with Lung Cancer
- A Multicenter Clinical Trial on the Diagnostic Value of Dual-Tracer PET/CT in Pulmonary Lesions Using 3'-Deoxy-3'-18F-Fluorothymidine and 18F-FDG
- In Vivo Imaging of 64Cu-Labeled Polymer Nanoparticles Targeted to the Lung Endothelium
- Time Course of Early Response to Chemotherapy in Non-Small Cell Lung Cancer Patients with 18F-FDG PET/CT