


Abstract
Timing of diuretic administration is not universally standardized in renography. Over the past year, our practice has changed from F-15 administration of furosemide to an F+0 protocol. Therefore, we have retrospectively compared these 2 cohorts to assess if the shorter interval between diuretic administration and study completion in the F+0 study results in a greater frequency of patients able to complete the subsequent 30-min dynamic acquisition without disruption due to voiding. Methods: We identified 108 diuretic 99mTc-mercaptoacetyltriglycine renograms performed in the previous 18-mo period. Three patients were given furosemide at 30 min after the radiopharmaceutical and were excluded. Twenty studies in children under 3 y of age were excluded from consideration because voiding is neither restricted in this age group nor does voiding into a diaper cause disruption. Forty milligrams of furosemide were administered to adults, whereas 0.5 mg/kg was given to children. In the first cohort of 56 studies, radiopharmaceutical was administered 15 min after furosemide (F-15), whereas, in the second cohort of 29 patients, it was administered immediately thereafter (F+0). In all cases, patients were asked to void proximal to radiopharmaceutical injection. Dynamic images and renogram curves were inspected for evidence of interruption or voiding midstudy. Statistical significance was determined by a 1-tailed Fisher exact test for proportions, with P < 0.05. Results: The F-15 and F+0 groups of patients were comparable in terms of age, sex, and diuretic amount. In 17 of the F-15 patients, renography was interrupted because of voiding (30%), whereas this occurred in only 3 of the F+0 patients (10%). This difference was significant at the P = 0.033 level. The mean time of voiding was 18.3 min (range, 12–25 min) for F-15 patients and 16 min (range, 12–19 min) for the F+0 group. Conclusion: The F+0 renal diuretic protocol is associated with a significantly lower rate of disruption because of voiding than the F-15 protocol, likely due to the shorter period between diuretic administration and study termination, which results in less bladder distention and discomfort. On the basis of these data, the F+0 protocol appears to be a more tolerable procedure.
Diuretic renography is an established method for investigation of hydronephrosis. The distinction between mechanical obstruction and dilation not associated with obstruction is critical to patient management. When renography is performed without the use of a diuretic, both conditions may appear similar, with prolonged retention of radiotracer within the renal collecting system. The fundamental hypothesis underlying diuretic renography is that increased urine flow, as produced by the diuretic, will result in prompt washout of activity in a dilated nonobstructed system. In cases of obstruction, washout after diuretic remains slow and there will be prolonged retention of radiopharmaceutical proximal to the obstruction (1).
Currently, furosemide is the diuretic favored for this purpose (2). Onset of action is within the first several minutes, whereas, on average, maximal effect occurs between 15 and 18 min after intravenous administration (3). Several protocols for diuretic renography have been described based on variation in timing of diuretic administration relative to radiopharmaceutical. In the initially described method (4,5), diuretic was injected approximately 20 min after the radiopharmaceutical (F+20). Subsequent studies reported that this protocol produced equivocal results in at least 15% of cases (6–8). Alternative protocols have been proposed in which diuretic is given 15 min beforehand (F-15) (9,10) or concurrent with radiotracer (F+0) (11–13).
For the past several years, where diuretic renography was indicated in situations of suspected renal obstruction, we have performed the F-15 variation of diuretic renography. On the basis of a subsequently published report that the results of F+0 diuretic renography are similar to those of the F-15 protocol (14), we have more recently modified our practice to administer furosemide immediately after radiopharmaceutical injection (F+0), a technically more convenient procedure.
We have occasionally noted that some patients cannot tolerate the 30 min of imaging after injection of radiopharmaceutical without the need to void. In this article we retrospectively compare our 2 cohorts of diuretic renography patients to assess if the reduced interval between diuretic administration and completion of the study in the F+0 group has decreased the frequency of interrupted studies due to voiding.
MATERIALS AND METHODS
Institutional Review Board approval was obtained for this retrospective analysis. A total of 108 diuretic renography studies were performed in the previous 18-mo period. In 3 patients, furosemide was administered at 30 min after the radiopharmaceutical and these studies were excluded. An additional 20 studies in children <3 y of age were excluded from consideration because voiding in this group is not restricted nor does voiding into a diaper cause disruption. Of the 85 remaining cases, in the cohort of patients studied first, furosemide was administered 15 min before radiotracer in 56 patients (F-15). In the subsequent cohort of 29 patients studied since we modified our protocol, furosemide was administered immediately after radiotracer (F+0). To our knowledge, there was no change in the referral patterns or overall patient characteristics across the 2 study periods.
No restriction was placed on drinking before the scan. The amount of furosemide was standardized at 40 mg intravenously for adults and 0.5 mg/kg intravenously for children. Adults were administered 222 MBq (6 mCi) of 99mTc-mercaptoacetyltriglycine (MAG3) intravenously, whereas children received a reduced amount based on body weight. Patients were instructed to void before MAG3 injection. No bladder catheters were placed for purposes of the diagnostic examination.
Standard imaging techniques were used (15–17). Patients lay supine on the imaging pallet with the kidneys, ureters, and bladder included in the field of view of the posteriorly situated γ-camera. Flow images were acquired at 2 s per frame for the first minute followed by 1-min images acquired over 30 min. In the event that patients needed to void during the study, they either urinated into a bed pan with minimal movement or were temporarily removed from the gantry for this purpose. The γ-camera acquisition was allowed to continue uninterrupted and, whenever possible, patients were promptly repositioned after voiding, allowing completion of the acquisition curves. Renal curves were corrected for background using a perirenal area according to standard techniques (15,17).
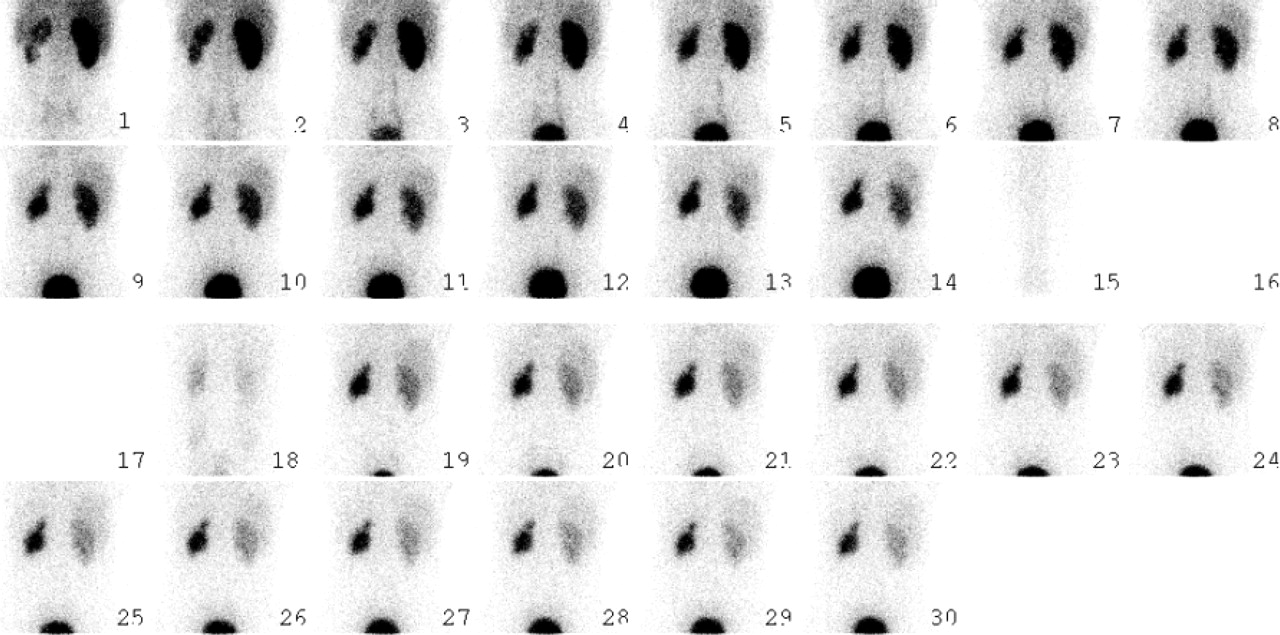
Dynamic images and renogram curves were inspected for evidence of voiding during the 30-min study period, apparent as transient disappearance of all patient activity from the field of view (when patients left the imaging table to void) or a decrease in bladder activity (when voiding occurred into a bedpan) (Figs. 1 and 2). The frequency of voiding in the study groups was determined. The statistical significance of the difference between the 2 cohorts was tested using a Fisher exact test for proportions and nonpaired t tests for continuous measurements, at a significance level of 0.05.

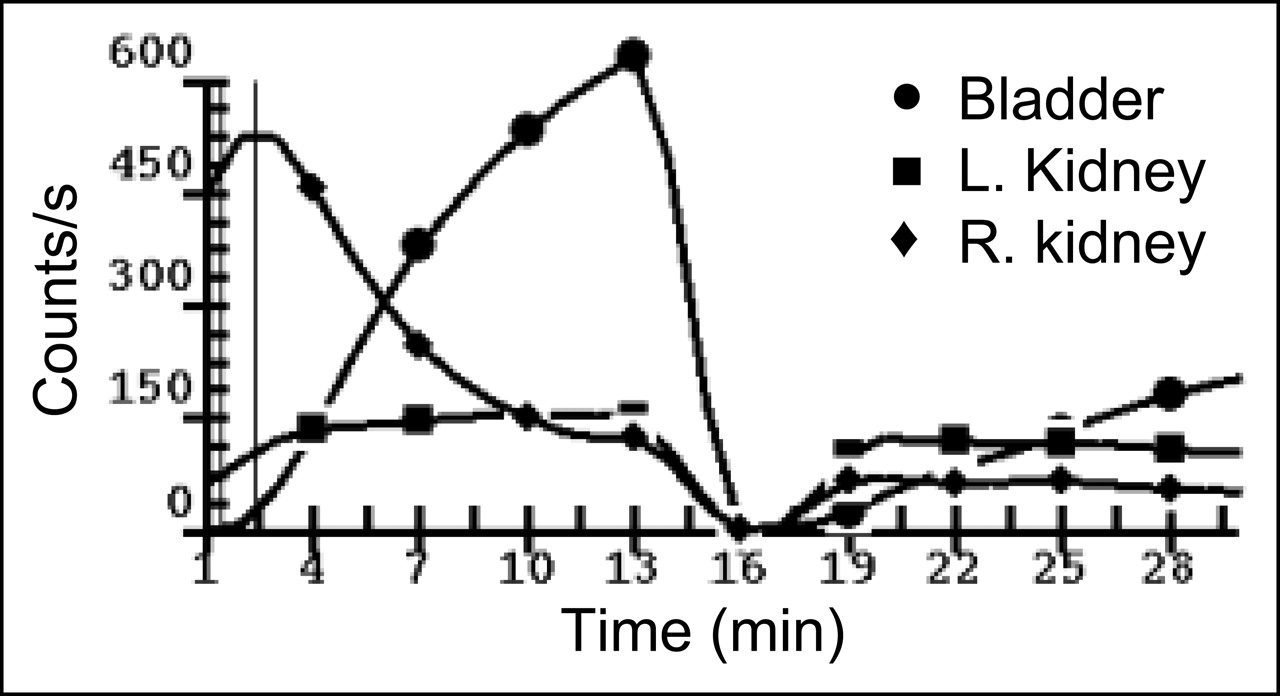
F-15 diuretic renography performed on 24-y-old man with left-sided hydronephrosis. Serial 1-min posterior images were obtained posteriorly over kidneys and bladder. Imaging was interrupted 14 min after MAG3 administration because of patient’s need to void. He was repositioned for completion of the 30 min of imaging.

Renogram findings in patient portrayed in Figure 1, typical of midstudy voiding.
RESULTS
Both cohorts of patients were comparable in term of age and sex (Table 1). An excess of females was noted in both groups. In the F-15 group, in 17 of 56 studies (30%) renography was interrupted because of voiding. In the F+0 cohort, voiding occurred in 3 of 29 (10%) patients. The frequency of voiding was significantly less for the F+0 cohort than the F-15 cohort in a 1-tailed comparison (P value = 0.033); in a 2-tailed test, the difference is of borderline significance (P value = 0.058).
Characteristics of Cohorts
The distributions of age and sex in the patients who voided were not different than those in the complete groups. Among 17 patients who voided in the F-15 group, there were 4 children (ages, 4, 5, 8, and 11 y) and 13 adults, whereas a 9-y-old child and 2 adults voided in the F+0 group. The mean time of voiding was 18.3 min in the F-15 group (range, 12–25 min) and 16.0 min in F+0 patients (range, 12–19 min). These differences were not statistically significant.
DISCUSSION
The timing of diuretic administration is not universally standardized in renography. The traditional F+20 technique allows observation of the rate of washout of radiopharmaceutical before diuresis; however, it requires careful supervision and a longer period of imaging on the γ-camera. The F-15 protocol has been designed such that the timing of radiopharmaceutical administration coincides with the maximal diuretic effect of furosemide (3). This modification has been shown to significantly reduce the equivocal response rate without significant effect on the assessment of split kidney function (18,19).
The F+0 protocol was first introduced for pediatric patients to shorten the acquisition time and avoid the need for an additional venous puncture (11,20). Although Donoso et al. (21) showed that early furosemide injection might result in an acceleration of renal transit and consequent underestimation of the renal function on the side with a short transit time, most groups have demonstrated good clinical results, comparable to F+20 and F-15 protocols (12). Turkolmez et al. (14) found that F+0 and F-15 protocols allow clarification in cases of equivocal F+20 studies, although the F+0 protocol was more practical and shorter.
In this study, we have analyzed whether the shorter interval between furosemide administration and study termination in the F+0 method results in a lower frequency of interrupted studies. For this reason, we have used the 1-tailed test for this comparison, resulting in a significant difference (P value = 0.033); using the more conservative 2-tailed test, the difference between groups is of borderline significance (P value = 0.058).
The present study analyzes a parameter that heretofore has not been discussed: the ability to tolerate 30 min of imaging of diuretic renography without need for voiding. Voiding in midstudy causes at least some degree of disruption and potential error in the renal time–activity curves and most certainly reflects underlying patient discomfort. Furthermore, overdistention of the bladder is associated with decreased renal drainage, and it is possible that the F-15 protocol results in greater fullness of the bladder and more significant obstructive effect on the upper renal tracts.
Our analysis therefore highlights an important difference between the F-15 and F+0 protocols. In our patients, F+0 renography was associated with a significantly lower rate of disruption of imaging because of voiding than the F-15 method. The lower frequency of voiding that we have noted in the F+0 studies compared with the F-15 studies is hypothesized to be due to the shorter period between diuretic administration and completion of imaging, which results in reduced bladder distention and discomfort. Although our patients were not randomized in this retrospective study, nor were parameters such as hydration status, baseline renal function, urine volume, and urine specific gravity tracked, there was no reason to believe that there was any change in the referral patterns or overall patient characteristics across the 2 contiguous study periods.
CONCLUSION
The F+0 renal diuretic protocol is associated with a significantly lower rate of disruption because of voiding than the F-15 protocol, likely due to the shorter period between diuretic administration and study termination, thereby resulting in less bladder distention and discomfort. Together with its more convenient intravenous regimen and shorter procedure time, we believe that the F+0 protocol is advantageous for routine clinical applications.
Footnotes
Received Dec. 22, 2004; revision accepted Apr. 19, 2005.
For correspondence contact: Lionel S. Zuckier, MD, Department of Radiology, Room H-125, New Jersey Medical School, 150 Bergen St., Newark, NJ 07101-1709.
E-mail: zuckier{at}umdnj.edu





{kind=link}
{kind=link}