


Abstract
Amisulpride appears to be an effective agent for treating positive or negative symptoms of schizophrenia, depending on dose. The aim of this study was to assess striatal dopamine D2 receptor availability by means of 123I-iodobenzamide (IBZM) SPECT in patients treated with high and low doses of this atypical antipsychotic drug. Methods: Twenty-nine patients (19 men and 10 women, age range, 19–68 y) with schizophrenia treated with high doses (15 patients; 400–1,200 mg/d; mean dose, 666.7 ± 219.3 mg/d) or low doses (14 patients; 50–300 mg/d; mean dose, 228.6 ± 93.5 mg/d) of amisulpride were examined. For assessment of plasma amisulpride concentration, blood samples were taken. Brain SPECT was performed 2 h after intravenous injection of 185 MBq of 123I-IBZM. For semiquantitative evaluation, transverse slices corrected for attenuation (Chang’s first-order method) were used to calculate specific binding in the striatum, with the frontal cortex used as background. Results: In all patients treated with amisulpride, specific binding of 123I-IBZM to D2 receptors was significantly lower (P < 0.001) than in healthy controls (0.95). Both groups treated with amisulpride differed significantly in specific binding of 123I-IBZM to dopamine D2 receptors (0.20 vs. 0.31, P < 0.05). D2 receptor blockade correlated well with the administered dose of amisulpride and with amisulpride plasma concentration. Conclusion: Our findings suggest that amisulpride treatment leads to a significant occupancy of postsynaptic dopamine D2 receptors. The blockade of D2 receptors tends to be significantly lower in patients receiving low-dose amisulpride therapy than in patients receiving high-dose therapy.
Schizophrenia is a chronic, severe, and disabling brain disorder. With a remarkably constant 1% worldwide lifetime incidence, schizophrenia is one of the most common mental illnesses (1) and results in enormous costs to society. Since the advent of conventional antipsychotic medications in the mid-1950s, the outlook has greatly improved for individual patients through reduction of the psychotic symptoms of schizophrenia and amelioration of the prognosis. These drugs, given at usual doses, may exert their therapeutic action on positive symptoms of schizophrenia by decreasing the dopaminergic activity mediated by the affinity for dopamine D2 receptors (2). Unfortunately, antipsychotic medications such as haloperidol are often associated with a wide range of undesired side effects (3), including parkinsonism, anticholinergic adverse effects, dystonia, and risk of tardive dyskinesia. Since the early 1990s, new neuroleptic medications, such as clozapine, olanzapine, and risperidone, have been introduced. Termed atypical, these agents represent a new generation of antipsychotics characterized by a significantly lower incidence of extrapyramidal side effects (EPS) and little or no effect on prolactin levels. The exact mechanisms that make these drugs atypical are not well understood (4). One important aspect of the pharmacologic profile of atypical neuroleptics, compared with conventional neuroleptics, is a higher affinity for 5-hydroxytryptamine type 2 (5-HT2) than for D2 receptors (5). Because of their superior therapeutic efficacy, tolerability, and safety profiles, compared with those of classic neuroleptics, atypical antipsychotic agents are considered to be the treatment of choice in first-episode patients (6).
Amisulpride is a substituted benzamide derivative highly predictive of potent antipsychotic activity with a low potential to cause EPS (7). It is considered to bind selectively and distinctly to the D2 and D3 dopaminergic receptors (8). Animal studies and clinical evidence suggest that the efficacy of amisulpride for treating negative or positive symptoms of schizophrenia may be dose dependent (2,9). At high doses (400–1,200 mg/d), amisulpride is used to treat acute symptomatology and positive symptoms in patients with schizophrenia. Furthermore, beneficial effects on negative symptoms in schizophrenic patients with a predominantly deficient syndrome have been demonstrated with lower doses of up to 300 mg/d (8).
As previously reported, dopamine D2 receptors can be adequately studied in vivo using SPECT, applying the benzamide derivate 123I-iodobenzamide (IBZM). This radiopharmaceutical crosses the blood–brain barrier and selectively binds to the postsynaptic dopamine D2 and D3 receptors (10). The aim of this study was to evaluate the degree of D2 receptor occupancy in schizophrenic patients treated with high and low antipsychotic dosages.
MATERIALS AND METHODS
Twenty-nine patients aged 19–68 y (mean age ± SD, 32 ± 12 y) with schizophrenia or schizoaffective disorder (DSM-IV) being treated with the atypical antipsychotic amisulpride were investigated. Fifteen patients (9 men and 6 women) received high doses of amisulpride (400–1,200 mg/d; mean dose, 666.7 ± 219.3 mg/d), and 14 other patients (10 men and 4 women) were treated with low, steady doses (50–300 mg/d; mean dose, 228.6 ± 93.5 mg/d) of amisulpride during 13.4 ± 2.4 d. On the day of the SPECT investigation, no amisulpride medication was given. The last dose of medication was administered in the hospital ward on the evening before the day of scintigraphy. Concomitant medication was restricted to biperiden and zopiclone. The literature shows no evidence that these concomitantly administered drugs affect the binding of IBZM to the dopamine D2 receptor (11). For patients pretreated with classic neuroleptics, 3 d were allowed for washout of prior neuroleptic treatment before monotherapy with amisulpride began. In 28 of 29 patients, plasma levels of amisulpride were assessed just before the SPECT investigation. Each subject received 185 MBq of 123I-IBZM intravenously 12–14 h after taking the last dose of amisulpride. Two hours after radiotracer administration, SPECT images were acquired during a period of 50 min. SPECT images were acquired using a Prism 3000 XP triple-head γ-camera (Picker) equipped with high-resolution fanbeam collimators. The acquisition parameters included a 20% energy window centered on 159 keV, a rotational radius of 13 cm or less, 120 projection angles over 360°, and a 128 × 128 matrix with a pixel width of 2.11 mm in the projection domain. The projection images were reconstructed by filtered backprojection and filtered by a low-pass filter. For uniform attenuation correction, Chang’s first-order method was used. Images were uniformly resliced using a line drawn to connect the most anterior aspect of the frontal pole to the most posterior aspect of the occipital pole, which approximates the line connecting the anterior and posterior commissures. The control group was 10 healthy age- and sex-matched subjects (6 men and 4 women; mean age, 32 y; range, 22–58 y).
To assess specific tracer uptake in the striatum, we used the region-of-interest technique. In each patient, data were evaluated for the 2 consecutive transverse slices showing the highest tracer accumulation in the basal ganglia; afterward, the arithmetic mean of these 2 slices was calculated. Mean specific binding in the basal ganglia regions was calculated by subtracting the mean counts per pixel in the frontal cortex as background (BKG) from the basal ganglia region (STR) and dividing the results by the mean counts per pixel in the background ([STR − BKG]/BKG). Templates were used for defining the striatal regions of interest. The size and shape of the templates were established and optimized using the data of the control group. The nonspecific background activity was estimated by drawing a region of interest around the frontal cortex. Mean specific binding (SB) values of a healthy control group were used to calculate the percentage occupancy of striatal dopamine D2 receptor ([SBcontrol –SBpatient]/SBcontrol). For statistical analyses, ANOVA, regression analyses (least-squares method), and the Student t test were used. All values were normally distributed. Data were compared with those of the control group. Differences were considered to be statistically significant when P was <0.05 and highly significant when P was <0.001.
RESULTS
The high-dose amisulpride group was significantly different from the low-dose group in administered dosage (8.8 ± 3.6 mg/kg of body weight vs. 3.2 ± 1.3 mg/kg of body weight, P < 0.001; total dose, 666.7 ± 219.3 mg/d vs. 228.6 ± 93.5 mg/d, P < 0.001). The measured amisulpride plasma concentrations were 257.7 ± 217.3 μg/L in the high-dose group and 134.2 ± 101.3 μg/L in the low-dose group. Specific binding of 123I-IBZM to the striatal dopamine D2 receptor was significantly lower (P < 0.001) in all patients undergoing low-dose therapy (0.31 ± 0.11) or high-dose therapy (0.20 ± 0.12) with amisulpride than in untreated healthy controls (0.95 ± 0.10). The estimation of dopamine D2 receptor occupancy by amisulpride indicated a mean of 73.3% ± 13.7% and a range of 41.9%–100% (P < 0.001). A significant difference was found between the high-dose group (mean D2 occupancy, 79.1% ± 12.9%; range, 51.3%–100%) and the low-dose group (mean D2 occupancy, 67.1% ± 12.1%; range, 41.9%–100%, P < 0.05). Individual indices for dopamine D2 receptor occupancy are presented in Table 1. Figure 1 shows the specific binding of 123I-IBZM to the dopamine D2 receptors in untreated healthy controls and treated schizophrenic patients. A good dose–response relationship between dopamine D2 receptor occupancy and daily dose of amisulpride (r = 0.72; P < 0.001) was observed, as shown in Figure 2. A similar correlation between amisulpride plasma concentration and binding of 123I-IBZM to striatal dopamine D2 receptors was observed (r = 0.65; P < 0.001), as shown in Figure 3. Figure 4 shows typical images of patients treated with different doses of amisulpride.
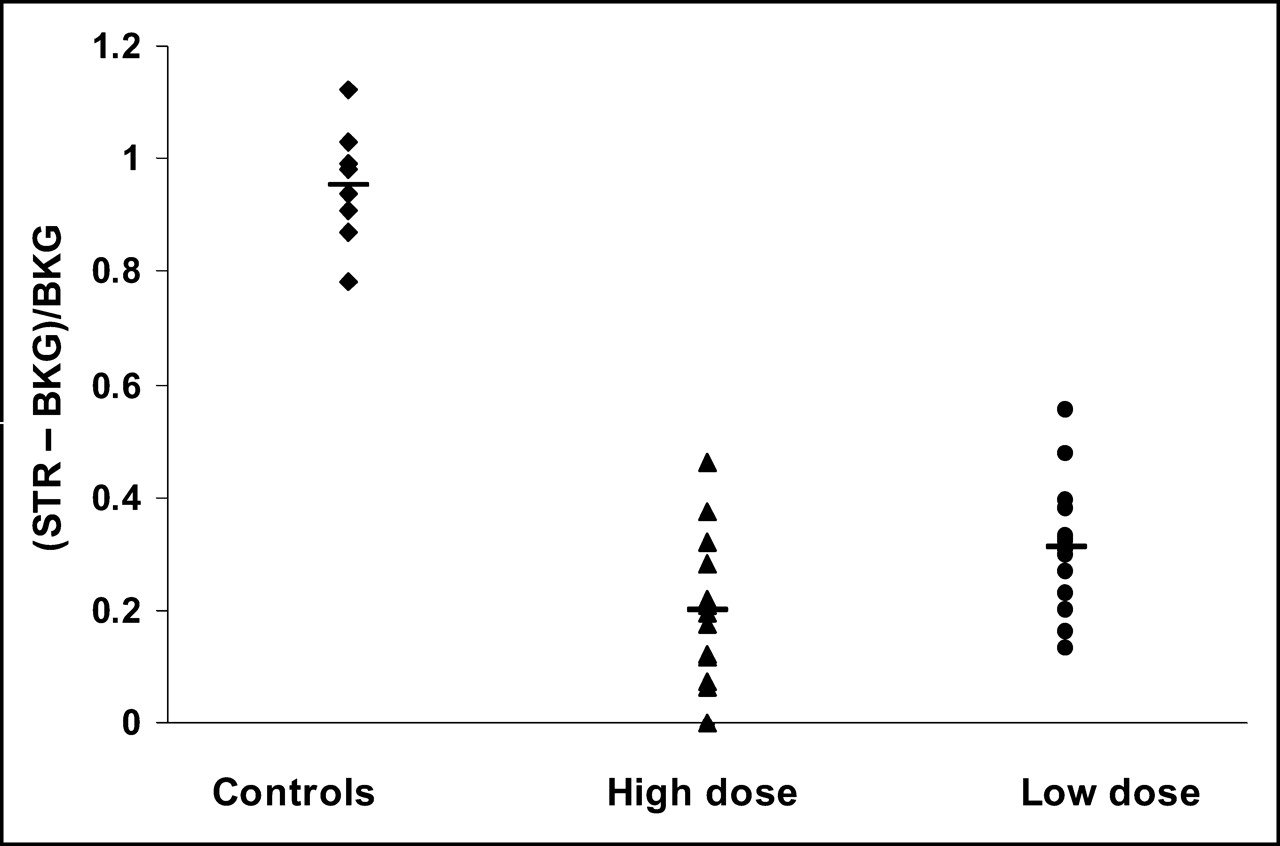
Specific binding ([STR − BKG]/BKG) of 123I-IBZM in healthy controls and in schizophrenic patients treated with high or low doses of amisulpride.

Dose–response relationship between striatal dopamine D2 receptor occupancy ([SBcontrol –SBpatient]/SBcontrol) and daily dose of amisulpride (mg/kg of body weight [b.w.]).
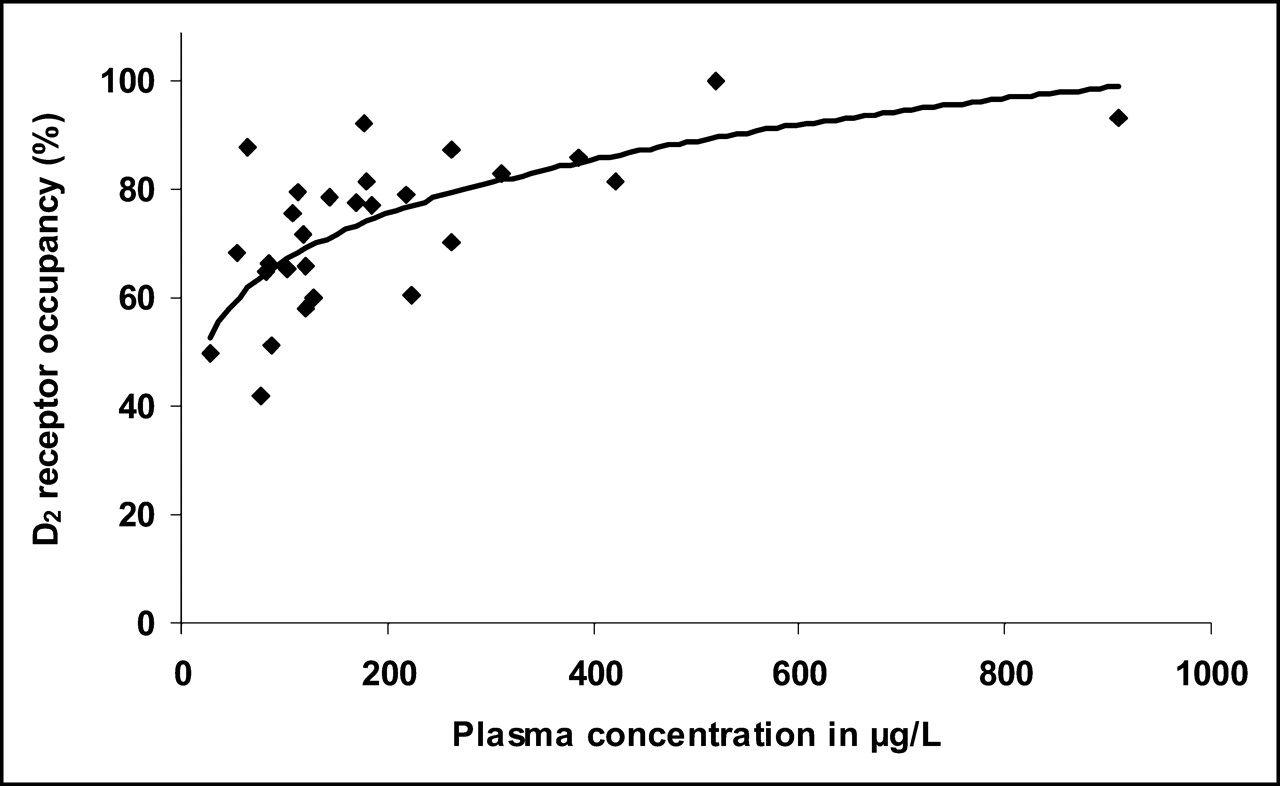
Dose–response relationship between striatal dopamine D2 occupancy ([SBcontrol –SBpatient]/SBcontrol) and amisulpride plasma concentration (μg/L).
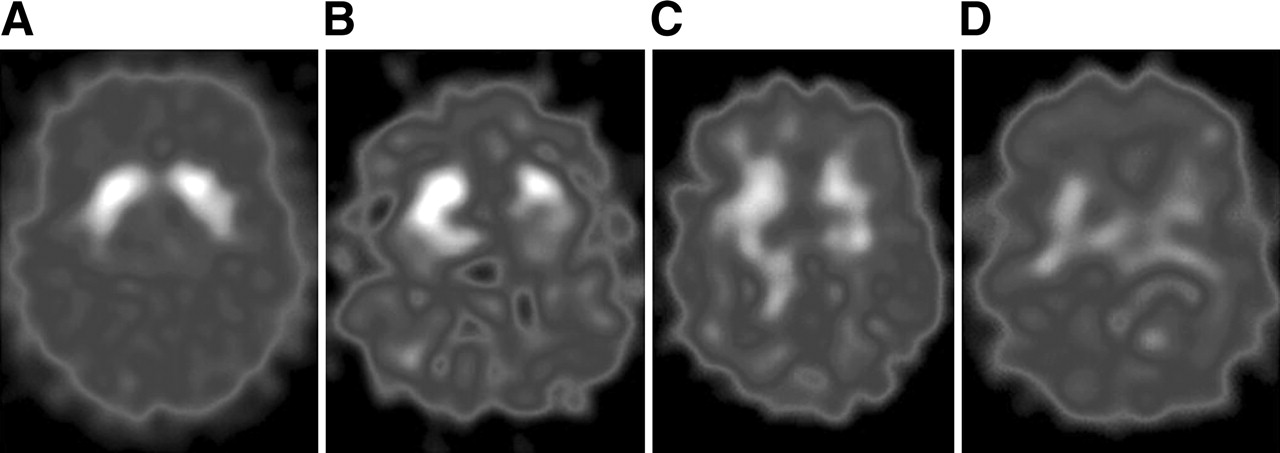
123I-IBZM SPECT images of dopamine D2 receptor binding at equilibrium: drug-naive schizophrenic patient (A) and schizophrenic patients being treated with 50 mg (B), 300 mg (C), or 800 mg (D) of amisulpride per day.
Mean Dosages of Amisulpride and Background-Corrected D2 Receptor Binding
DISCUSSION
The objective of the present study was to assess striatal dopamine D2 receptor occupancy in 29 patients with schizophrenia and schizoaffective disorder under high- or low-dose treatment with the atypical antipsychotic amisulpride, as measured by 123I-IBZM SPECT. The clinical utility of this method to measure brain dopamine receptor occupancy in healthy volunteers, in patients with diverse neuropsychiatric disorders, and in schizophrenic patients receiving different types of antipsychotic medication has previously been reported by several investigators (12–20), despite the fact that SPECT studies cannot quantify results as well as can PET studies.
It is thought that dopamine D2 receptor blockade mediates the antipsychotic action of typical neuroleptics such as haloperidol. This hypothesis has been confirmed in various studies with PET and SPECT (19,21). In defining the atypicality of antipsychotics, however, some experts include not only the criterion of no or lower risk of inducing EPS coupled with enhanced improvement in negative symptoms but also efficacy in schizophrenic patients refractory to treatment with classic neuroleptics, or lack of drug-induced hyperprolactinemia (22). Evidence presently suggests that atypical drugs differ from the typical in their mechanism of action but that not all share the same mechanism (23).
In contrast to other atypical antipsychotics, the substituted benzamide derivative amisulpride binds selectively and distinctly to the dopaminergic D2 and D3 receptors without substantial affinity to D1 or serotonergic 5-HT2 receptors (8). Several studies have demonstrated a biphasic effect of amisulpride on positive and negative symptoms, depending on the administered dose range (24–26), accompanied by a low incidence of EPS (9). The physiologic mechanism of amisulpride and its dose–response relationship has not, to date, been definitely explained. One hypothesis is that its clinical efficacy against negative symptoms may be explained by blockade of presynaptic dopaminergic D2 and D3 autoreceptors that control dopamine release at low doses, whereas at higher doses, amisulpride occupies postsynaptic dopamine D2 receptors (27,28). To date, 2 PET studies (2,29) have reported striatal binding indices in patients treated with amisulpride. Martinot et al. reported a low postsynaptic D2 occupancy in the striatum at low doses of amisulpride (50–100 mg/d). The authors also suggested that extrastriatal binding could mediate the effect on negative symptoms (2). At amisulpride doses resulting in low plasma levels, no apparent interaction of amisulpride with the striatum was detectable by Xiberas et al. (29). The authors hypothesized that low plasma concentrations are associated with low striatal binding and marked extrastriatal binding, in contrast to marked binding in both striatal and extrastriatal regions for higher plasma concentrations (29).
Our study found a clear correlation between the degree of striatal dopamine D2 receptor occupancy and the amisulpride plasma concentration and a quite similar correlation between the degree of striatal dopamine D2 receptor occupancy and the administered dose of amisulpride. Thus, our results are concordant with the findings of other studies that demonstrated positive correlations between the plasma rates of amisulpride and the binding indices in striatal regions (29,30).
At therapeutic doses, the dopamine D2 receptor occupancy of amisulpride was closer to that of atypical neuroleptics such as olanzapine and risperidone than to that of clozapine, the archetype of atypical neuroleptics, which presented by far the lowest occupancy seen in our studies. The high- and low-dose treatment groups differed significantly in dopamine D2 receptor occupancy, and binding of 123I-IBZM was significantly lower in both groups than in untreated healthy controls. With regard to differences from the findings of Xiberas et al. (29), their mean administered dosage in the low dose range was explicitly lower (105.6 mg/d) than our average administered low dose (228.6 mg/d). Consequently, we assume that, in our low-dose group, the administered mean daily dose of amisulpride was above the threshold described by Xiberas et al. under which no or only little striatal interaction appeared. Overall dopamine D2 receptor occupancy in the high-dose group was higher in our study than in other studies (2,20,29), as again may partly be explained by the higher average dose administered to our patients. However, we believe that in view of the described differences in estimation of D2 receptor occupancy, the use of different methods such as SPECT and PET, and the consequent use of different radioligands, the accuracy of predicting D2 occupancy from plasma levels is not assured.
Overall, our findings revealed that at doses considered to be low in our institution, amisulpride had already blocked postsynaptic striatal dopamine D2 receptors and successfully treated negative symptoms. The different actions of amisulpride dosage on positive and negative symptoms may be due to interactions with other areas of the dopaminergic neurotransmitter systems. A limitation of this study is that the radiopharmaceutical 123I-IBZM provides reliable information about dopaminergic D2 receptor status in only the striatum and does not allow adequate visualization of extrastriatal D2 receptors. However, it has been postulated that amisulpride also binds to dopamine receptors in limbic and hippocampal structures. This effect suggests that, compared with typical neuroleptics, 123I-IBZM has a low propensity to induce EPS (30).
Reports in the literature indicate an apparent relationship between the degree of striatal D2 receptor occupancy, the onset of EPS, and treatment with neuroleptics (19,21,31,32). Atypical neuroleptics such as clozapine are considered to cause fewer EPS than do typical neuroleptics (33), potentially related to their lower striatal dopamine D2 blockade in vivo (34) and, in part, to their affinity to 5-HT2 receptors (5). However, also under discussion is that a preferential action on serotonin 5-HT2 or D4 receptors or a more rapid dissociation from the dopamine D2 receptor may explain the atypicality (4,22).
When compared with the findings for olanzapine, clozapine, and risperidone in our previous studies, the findings for amisulpride in the present study revealed a higher dose–response relationship for the former neuroleptics. The low propensity for inducing EPS in patients treated with olanzapine, found in our previous study, (35) can be explained not only by relatively low striatal D2 receptor blocking but also by other receptor-binding profiles such as affinity to muscarinic receptors or particularly to the 5-HT2 system (36). However, amisulpride does not have any significant affinity to the 5-HT2 system or to other nondopaminergic transmitter systems. Therefore, the D2/5-HT2 receptor hypothesis cannot explain the atypicality of antipsychotics. Nevertheless, amisulpride clearly has the clinical profile of an atypical antipyschotic, characterized in particular by its lower propensity to induce EPS and its greater efficacy in treating negative symptoms (22). Thus, the decreased tendency of atypical neuroleptics to induce EPS at therapeutic doses can be considered to be due not only to limited occupancy of striatal dopamine D2 receptors or to affinity to the 5-HT2 system in vivo but also, at least partly, to other mechanisms.
Two possible mechanisms that could explain the atypicality of amisulpride in light of these findings were suggested by Schoemaker et al. and include action on limbic D2/D3 receptors and preferential blockade of presynaptic D2/D3 receptors (22,28). The hypothesis of limbic-selective occupancy of D2 receptors by amisulpride could be confirmed by the findings of Bressan et al. for 123I-epidepride (30). Otherwise, the “fast-off” theory of antipsychotic action, which postulates a rapid dissociation of atypical antipsychotics from the dopamine D2 receptors, is discussed in the literature (37). A limitation of this study is that, for ethical reasons, repeated SPECT investigations of schizophrenic patients in drug-naive periods or while receiving amisulpride medication could not be performed. Dopamine D2 receptor binding has been assessed by PET and SPECT in untreated schizophrenic patients in several studies, with inconsistent results (38–41). In view of the results of 2 published 123I-IBZM studies that found no significant differences in D2 receptor availability between patients with schizophrenia and a comparison group (38,42), and for better comparison with previously published studies, we expressed D2 receptor occupancy in relation to our standardized control population.
CONCLUSION
The findings of the present study indicated that low-dose therapy with the atypical antipsychotic agent amisulpride is associated with a significantly lower blockade of striatal dopamine D2 receptors than is seen during high-dose treatment. However, a significant striatal D2 blockade was demonstrated at therapeutically effective dose ranges. Furthermore, this study showed a good relationship between the degree of striatal dopamine D2 receptor occupancy and the amisulpride plasma concentration or the administered dose. The measured striatal D2 receptor occupancy was as high as that observed in our previous olanzapine and risperidone studies and even explicitly higher than the receptor occupancy observed with clozapine. Further studies with radiotracers of higher affinity than 123I-IBZM, such as 123I-epidepride and 18F-fallypride, are warranted to assess the role of D2 occupancy of amisulpride and other atypical antipsychotics in the limbic cortex.
Acknowledgments
We are grateful for the support and superb technical assistance of the technicians in the Department of Nuclear Medicine at the University of Munich.
Footnotes
Received Sep. 17, 2004; revision accepted Feb. 14, 2005.
For correspondence or reprints contact: Stefan Dresel, MD, Department of Nuclear Medicine, Ludwig-Maximilians-University of Munich, Ziemssenstrasse 1, 80336 Munich, Germany.
E-mail: stefan.dresel{at}med.uni-muenchen.de





{kind=link}
{kind=link}
{kind=link}
{kind=link}