


Abstract
Uptake of radiolabeled peptides in the kidneys may obscure abdominal tumors in radiopeptide scintigraphy. This problem is much more pronounced in peptide receptor radionuclide therapy (i.e., radiopeptide therapy), possibly leading to renal damage or even failure. Cationic peptide uptake in the kidneys can be reduced by the application of cationic amino acids, such as lysine or arginine. The aim of this study was to develop a suitable method to reduce anionic peptide uptake in the kidneys. 111In-Diethylenetriaminepentaacetic acid dGlu1-minigastrin (111In-DTPA-dGlu-Glu-Glu-Glu-Glu-Glu-Ala-Tyr-Gly-Trp-Met-Asp-Phe-NH2) was chosen as a model compound with a sequence of 6 negatively charged glutamic acids in a chain and an additional aspartic acid. Methods: TT (human medullary carcinoma cells)-bearing nu/nu mice of the Institute of Cancer Research genotype received intraperitoneal injections of different chain lengths and weights of glutamic acids, aspartic acids, and derivatives of glutamic acids. Uptake in tumors and organs was determined and compared with the values for untreated control mice. Results: Accretion of 111In-DTPA-dGlu1-minigastrin in the kidneys could be reduced by up to 90%. The uptake values for all other organs and the tumors were not affected. These results were obtained with a chain of 5 or more glutamic acids, whereas uptake in kidneys was affected not at all or only slightly with poly-d-glutamic or polyaspartic acids and with Glux (x = 1–4). Conclusion: These studies indicated a specific blocking of uptake by Glu5 sequences in the kidneys. Application of polyglutamic acids is a new, successful method of reducing uptake of negatively charged peptides in the kidneys during radiopeptide therapy.
Uptake of radiolabeled low-molecular-weight biomolecules such as peptides or monoclonal antibody fragments by the kidneys is a problem because of the anticipated nephrotoxicity. Because the kidney is radiosensitive, it is the dose-limiting organ in radioimmunotherapy with antibody fragments and peptide receptor radionuclide therapy (i.e., radiopeptide therapy) (1). Therefore, strategies are needed to protect the kidneys by lowering radionuclide uptake. Pimm et al. and Behr et al. discovered that uptake of activity bound to antigen-binding fragments in the kidney was due mainly to the positive charges of basic amino acids such as lysine and arginine (2–4). These investigators demonstrated the possibility of reducing this uptake by up to 80% with l- and d-lysine in animals. In patients, infusion of positively charged amino acids could reduce uptake in the kidneys by up to 40% without affecting uptake in other tissues (2). This knowledge was transferred to peptides, especially to radiolabeled octreotide analogs (which have a lysine in their structure) used for therapy. High toxicity to the kidneys during therapy with 90Y-DOTA-Tyr3-octreotide (DOTATOC) is a problem that can lead to chronic and acute renal failure caused by the long-range β-emitter (5). Renal accretion was reduced by more than 45% in rats by injection of lysine (6,7) and by approximately 40% in humans by infusion of basic amino acids (5,8,9).
We have developed 111In-DTPA-dGlu1-minigastrin for the diagnosis and staging of medullary thyroid cancer. Unfortunately, in mice the kidneys take up as much as 40% of the injected dose (%ID) per gram of body weight (10–12). The dGlu1-minigastrin possesses 7 acidic amino acids (6 glutamic acids and 1 aspartic acid). This fact led us to conclude that the high uptake in the kidneys could be due to the high number of acidic amino acids. In this study, we evaluated the possibility of reducing uptake of 111In-DTPA-dGlu1-minigastrin (DTPA-dGlu-Glu-Glu-Glu-Glu-Glu-Ala-Tyr-Gly-Trp-Met-Asp-Phe-NH2) in the kidneys with preinjection or coinjection of acidic amino acids.
MATERIALS AND METHODS
Chemicals
Unless stated otherwise, all chemicals were purchased from Fluka, Sigma-Aldrich, or Merck and were used without further purification. dGlu1-minigastrin was synthesized by Sigma Genosys. DTPA-dGlu1-minigastrin was synthesized and labeled with 111In as described elsewhere (11). Glu4 and Glu5 were synthesized by Sigma Genosys. Glu and Glu3 were obtained from Bachem. Poly-l-Glu, 2–15 kDa (Glu15—Glu116); poly-l-Glu, 15–30 kDa (Glu116—Glu232); poly-d-Glu, 2–15 kDa (dGlu15—dGlu116); poly-l-Gln, 2–15 kDa (Gln15—Gln117); and poly-l-Asp, 2–15 kDa (Asp17—Asp130) were purchased from Sigma-Aldrich.
Animal Models and Biodistribution Studies
All animal studies were performed according to German legislation and approved by the local animal welfare committee. Six-week-old female nu/nu mice (body weight, about 25 g) of the Institute of Cancer Research genotype received, in the scapular region, subcutaneous injections of 200 μL of a cell suspension with 106 cells of a human medullary thyroid cancer cell line (TT). After 3 wk, the tumors weighed about 300 mg. The mice received about 555 kBq of 111In-DTPA-dGlu1-minigastrin intravenously into the tail. Three mice per group were killed by cervical dislocation at 10 min, 1 h, 2 h, 4 h, and 24 h after injection of the radiolabeled peptide. Samples of blood and organs were removed and weighed, and their radioactivity was measured in an automatic NaI(Tl) γ-counter. The %ID/g was calculated for each organ and tissue. A Mann—Whitney test was performed using GraphPad (GraphPad Software, Inc.) to compare the biodistribution results with those of an untreated group and to determine the significance of differences.
Uptake Reduction
The uptake reduction studies were performed on 3 tumor-bearing animals per group. The biodistribution was evaluated 4 h after injection of 555 kBq of 111In-minigastrin as already described.
Two milligrams of monomers and oligomers of glutamic acid (Glu, Glu2, Glu4, Glu5, Glu7, Glu15–116, and Glu116–232) per gram of body weight were injected to evaluate the influence of the glutamic acid chain on uptake in the kidneys. The glutamic acids were injected intraperitoneally 10 min before intravenous injection of 555 kBq of 111In-DTPA-dGlu1-minigastrin.
The animals received intraperitoneal injections of 0.01–40 mg of Glu15—Glu116 per gram of body weight 10 min before injection of 111In-DTPA-dGlu1-minigastrin, to evaluate the mass of blocking agent needed to significantly reduce uptake in the kidneys.
The mice received a 2-mg injection of Glu15—116 per gram of body weight and were sacrificed after 4 h; their tissues and organs were measured for comparison with those of the untreated group.
Different oligo-amino acids, such as Glu15—Glu116, dGlu15—dGlu116, Gln15—Gln117, and Asp17—Asp130, were tested to evaluate the influence of charge on uptake in the kidneys.
The influence of the timing of the amino acid injection was evaluated separately. For this purpose, Glu15–117 was injected intraperitoneally at 60, 20, and 10 min before or 10 and 30 min after injection of the radiolabeled peptide.
RESULTS
The results of the normal biodistribution in tumor-bearing mice are shown in Table 1. Uptake in the kidneys was comparably high, reaching about 40 %ID/g after 4 h. Specific uptake was observed in the receptor-positive stomach (0.113% ± 0.025 %ID/g) and tumor (0.216% ± 0.012 %ID/g). The other organs showed fast clearance with a low background uptake.
Biodistribution of 111In-DTPA-dGlu1-Minigastrin
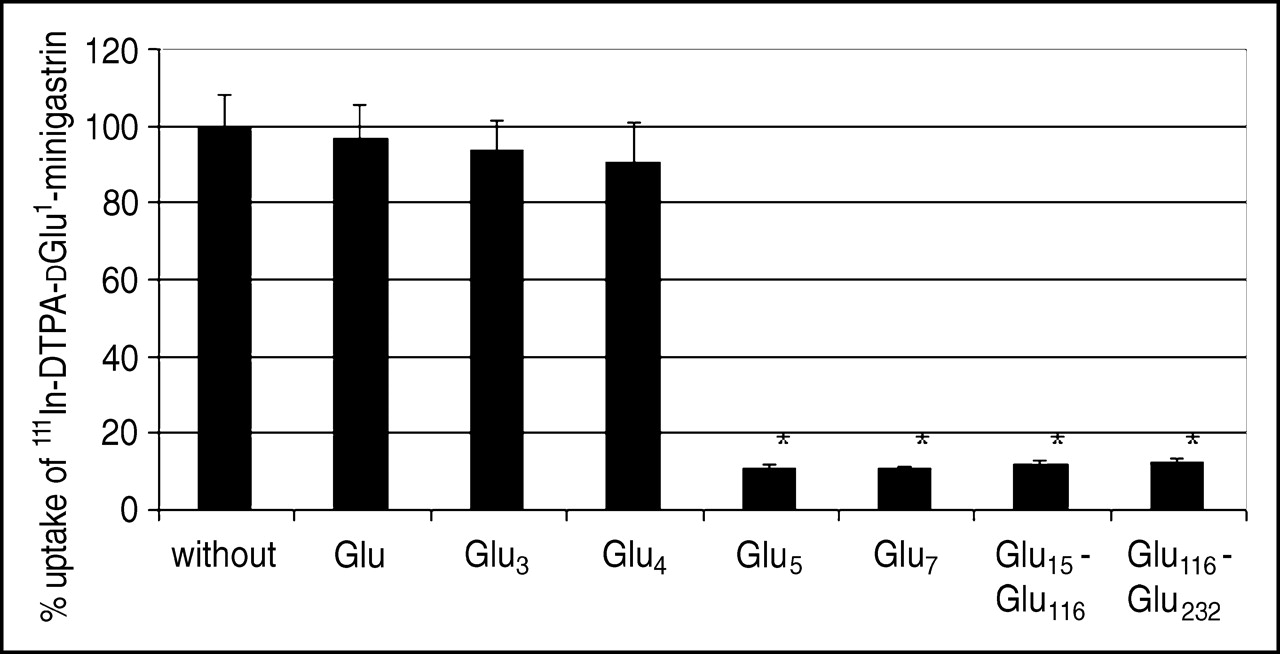
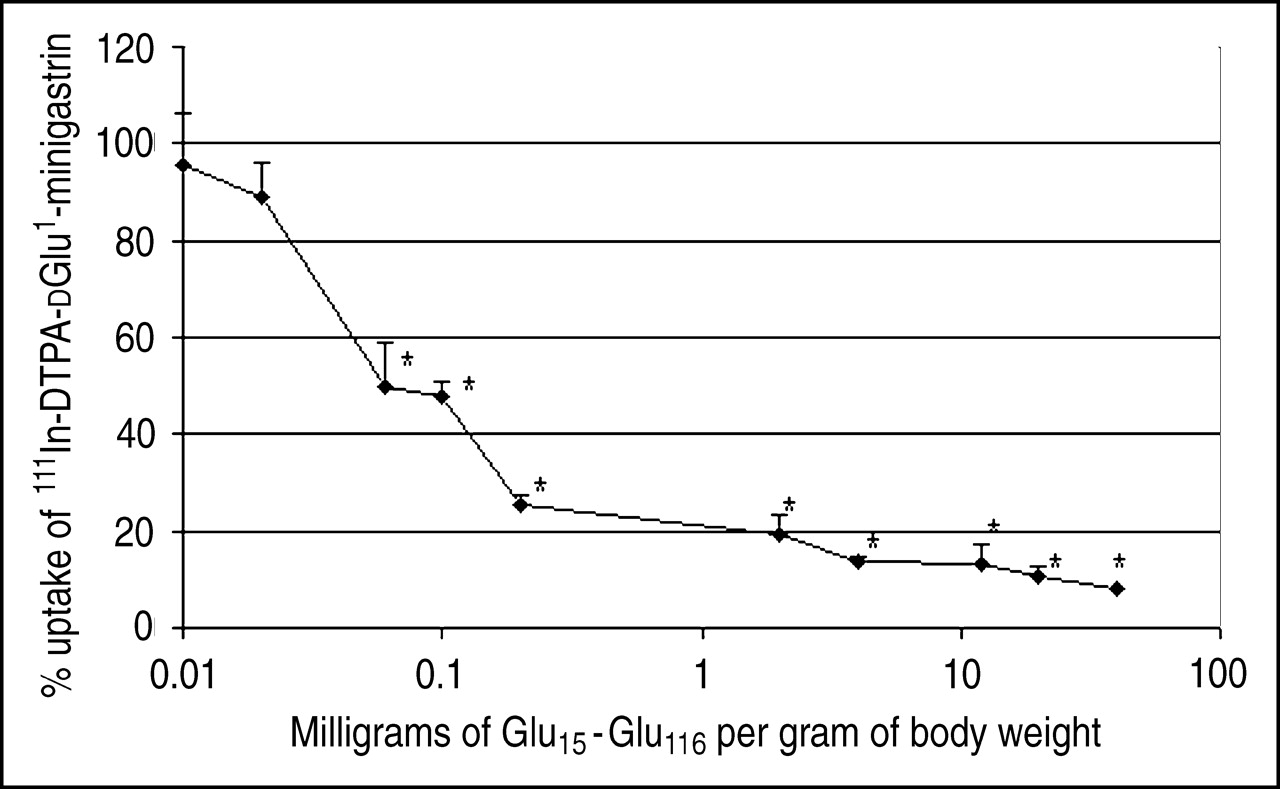
Uptake in the kidneys was dramatically reduced (by up to 90%, compared with the control group) in our mouse model after intraperitoneal injection of 2 mg (per gram of body weight) of oligo-glutamic acid chains with 5 or more amino acids (Fig. 1), whereas uptake with chains shorter than 5 amino acids remained unchanged, compared with the control group, at about 40 %ID/g. Uptake in other organs and tissues after 4 h was not significantly affected (Table 2). We were able to demonstrate the dependency of the molecular weight/chain length of the injected glutamic acids in further experiments with Glu15–116. Uptake in the kidneys was significantly reduced (by 50%) with 0.06 mg or more per gram of body weight. The maximal reduction in uptake—more than 80%—was found with 2 mg or more per gram of body weight (Fig. 2).

Comparison of 111In-DTPA-dGlu1-minigastrin uptake in kidneys after injection of 7 different glutamic acid chains. *P < 0.05, compared with biodistribution without injection of glutamic acids.

Reduction of 111In-DTPA-dGlu1-minigastrin uptake in kidneys after injection of Glu15—Glu116. Reduction is seen to depend on mass of Glu15—Glu116, in mg/g of body weight. *P < 0.05, compared with biodistribution without injection of Glu15—Glu116.
Biodistribution of 111In-DTPA-dGlu1-Minigastrin 4 Hours After Injection of 2 mg of Glu15—Glu116
Uptake in the kidneys with coinjection was compared with that without coinjection (Table 3). Uptake was reduced significantly with Glu15—Glu116 (down to 12% ± 3%, compared with the control group), less with dGlu15—dGlu116 (down to 65% ± 12%, compared with the control group), and not at all with the other substances.
Comparison of Uptake With and Without Injection of Amino Acids
The influence of the timing of the injection was tested with Glu15—Glu116. A reduction of 90%–95% could be achieved at all time points before intravenous injection of 111In-DTPA-dGlu1-minigastrin, whereas a reduction of about only 10% occurred if Glu15—Glu116 was administrated after the intravenous injection (Table 4).
Dependency of Uptake on Timing of Injection of Glu15—Glu116
DISCUSSION
The kidneys are known to be the dose-limiting organ in radiopeptide therapy with β-emitters such as 90Y or, to a lesser extent, 177Lu (5,13). These radiopeptides are cleared physiologically via the kidneys, which have a tubular reuptake mechanism to avoid the loss of substances otherwise valuable. Most peptides are cleaved to single amino acids or metabolites in the kidneys to restore these metabolites. Activity bound to metabolites is reabsorbed, resulting in a high and mainly residualizing uptake in the tubular cells (14,15). Damage to the kidneys induced by irradiation can cause nephropathy after therapeutic application of radiopeptides (16) and has been widely discussed in the literature (17–23). The strategies to reduce uptake in the kidneys are based mainly on blocking of the positively charged reuptake mechanism with basic amino acids such as lysine or arginine (5,9) but also with the drug colchicine, which prevents endocytosis in tubular cells (24). The dose to the kidney in patients was reduced by about 25% (5,9).
Initial therapeutic application of 90Y-labeled DTPA-dGlu1-minigastrin showed the same problems. An objective response in 2 of 8 patients was achieved at the levels of 148 and 185 GBq/m2. But in patients treated at these levels, 1 case of acute reversible renal failure developed; 1 of chronic renal failure after 12 mo, requiring hemodialysis; and 1 of myelodysplastic syndrome (12). The renal failures were caused by high retention of radioactivity in the kidneys. Uptake in the kidneys must be reduced if safe, therapeutic application to patients is to be possible.
Therefore, we examined the influence of an injection of negatively charged amino acids on uptake of radiolabeled minigastrin compounds in the kidneys. We found that reuptake occurred not only for positively charged amino acids but also for negatively charged amino acids. Blocking of uptake with negatively charged amino acids showed high specificity. A high reduction could be achieved only with penta-l-glutamic acids or longer chains (up to 90%). Oligo-d-glutamic acid (molecular weight, 2–15 kDa) caused a reduction of only 35%, whereas polyaspartic acid, which is shorter only by a CH2 in the side chain, caused no significant reduction compared with oligo-glutamic acid. The effect disappeared as expected with oligo-glutamine, in which the negative carbonic acid had been converted to a neutral amide.
These results show that, for radiolabeled peptides, different pathways play a role in the reuptake mechanism of the kidneys. Somatostatin derivatives are taken up via a mechanism driven by positive charges (lysine), whereas minigastrin reuptake is driven by negatively charged glutamic acid. Therefore, the use of glutamic acid to reduce uptake of somatostatin analogs is hard to envision, and lysine cannot be used to reduce uptake of negatively charged amino acids.
The finding that reuptake in the kidney can be reduced opens new horizons for the safe use of radiopeptide therapy with minigastrin derivatives and extends the application of radiopeptide therapy to tumors which can rarely be imaged or treated satisfactorily with somatostatin analogs, such as medullary thyroid tumors and small cell lung cancer, and to dedifferentiated neuroendocrine tumors or other cholecystokinin-2—positive malignant lesions.
CONCLUSION
The high uptake of 111In-DTPA-dGlu1-minigastrin in the kidneys of mice could be specifically blocked with a chain of more than 5 glutamic acids. This finding leads to the possibility of reducing uptake of negatively charged peptides in the kidneys and of improving the tumor-to-kidney ratio, allowing one to deliver more activity to the tumor without exceeding the renal dose limit and to administer safe radiopeptide therapy for cholecystokinin-2 receptor—positive tumors.
Acknowledgments
We thank Birgit Herbst, Ulla Cramer, and Christa Angerstein for technical assistance. We are grateful to the participants of the COST action B12 for fruitful discussions. This work was financially supported by grant 10-1600-Be2 from the Deutsche Krebshilfe.
Footnotes
Received Oct. 21, 2004; revision accepted Feb. 14, 2005.
For correspondence or reprints contact: Martin Béhé, PhD, Department of Nuclear Medicine, Philipps-University of Marburg, Baldingerstrasse, D-35043 Marburg, Germany.
E-mail: behe{at}staff.uni-marburg.de
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Radiohybrid Ligands: A Novel Tracer Concept Exemplified by 18F- or 68Ga-Labeled rhPSMA Inhibitors
- Cholecystokinin 2 Receptor Agonist 177Lu-PP-F11N for Radionuclide Therapy of Medullary Thyroid Carcinoma: Results of the Lumed Phase 0a Study
- Diabody Pretargeting with Click Chemistry In Vivo
- Evaluation of a Nonpeptidic Ligand for Imaging of Cholecystokinin 2 Receptor-Expressing Cancers
- Pharmacokinetic Properties of Peptidic Radiopharmaceuticals: Reduced Uptake of (EH)3-Conjugates in Important Organs
- Renal Toxicity of Radiolabeled Peptides and Antibody Fragments: Mechanisms, Impact on Radionuclide Therapy, and Strategies for Prevention
- Selection of Radiolabeled Gastrin Analogs for Peptide Receptor-Targeted Radionuclide Therapy
- Indication for Different Mechanisms of Kidney Uptake of Radiolabeled Peptides
- Added value of gastrin receptor scintigraphy in comparison to somatostatin receptor scintigraphy in patients with carcinoids and other neuroendocrine tumours
- Gelatin-Based Plasma Expander Effectively Reduces Renal Uptake of 111In-Octreotide in Mice and Rats
- CCK-2/Gastrin Receptor-Targeted Tumor Imaging with 99mTc-Labeled Minigastrin Analogs