


Abstract
The aim of this study was to assess the relationship between brachial artery flow–mediated dilation (FMD) and coronary flow reserve (CFR) in patients with peripheral artery disease (PAD). Methods: Thirty patients who had PAD, who showed no cardiac symptoms, and who had normal stress SPECT cardiac imaging results and 28 control subjects underwent brachial artery FMD assessment by ultrasound and dipyridamole 99mTc-sestamibi imaging. Myocardial blood flow (MBF) was estimated by measuring first-transit counts in the pulmonary artery and myocardial counts from SPECT images. Estimated CFR was expressed as the ratio of MBF at stress to MBF at rest. Results: Patients with PAD were separated into 2 groups according to the median value of overall FMD (6.85%): group 1 (n = 15) with FMD above the median (mean ± SD, 8.78% ± 1.3%) and group 2 (n = 15) with FMD below the median (mean ± SD, 5.14% ± 0.94%). FMD was significantly higher in control subjects (11.4% ± 3.4%) than in both groups of PAD patients (P < 0.001 for both). In control subjects, estimated CFR was 2.2 ± 0.4—significantly higher than CFR in both groups of PAD patients (P < 0.001 for both). In addition, in PAD patients of group 1, estimated CFR was 1.5 ± 0.4—higher than CFR in group 2 (1.0 ± 0.4) (P < 0.01). When all PAD patients were considered, a significant correlation between FMD and estimated CFR was observed (r = 0.56, P < 0.005). Conclusion: Estimated CFR is significantly lower in patients with PAD than in control subjects, and CFR impairment correlates with the degree of peripheral endothelial dysfunction.
Endothelial dysfunction, by impairing vasomotor tone and promoting arterial thrombosis, vascular cell migration, and proliferation, is a major determinant of atherosclerosis (1,2). Endothelial dysfunction precedes clinically manifested atherosclerosis, and its assessment through the use of high-resolution ultrasound to measure brachial artery diameter in response to reactive hyperemia has increased the clinical relevance of vascular function evaluation (3,4). High-resolution ultrasound provided evidence that reduced endothelium-mediated vasodilatation is associated with increased risk for cardiovascular events in a variety of conditions (5,6). In particular, patients with peripheral artery disease (PAD) have a marked reduction in flow-mediated dilation (FMD) that portends an adverse prognosis (7,8). Noteworthy, in patients with coronary artery disease (CAD), endothelium-mediated vasodilatation of the brachial artery correlates with the coronary vasodilator response (9,10). Interestingly, coronary flow reserve (CFR), which depends, at least in part, on endothelium-mediated vasoreactivity, also may be impaired in the absence of clinically manifested CAD, and the evaluation of CFR may allow early detection of coronary atherosclerosis (11,12). At this time, little is known about the relationship between peripheral endothelial function and CFR.
PET leads to the absolute quantitation of myocardial blood flow (MBF) and CFR (13,14). Recent studies also demonstrated that SPECT is a useful noninvasive and less expensive technique for estimating relative CFR (15–18). The aim of this study was to assess the relationship between brachial artery FMD and estimated CFR in patients with PAD but without evidence of CAD.
MATERIALS AND METHODS
Patients
We studied 30 consecutive patients (26 men; mean age ± SD, 65 ± 9 y) who had evidence of PAD at Doppler examination, who showed no cardiac symptoms, and who had normal stress SPECT cardiac imaging results. All of them were referred to the Department of Clinical Medicine for leg pain while walking and had an ankle–brachial pressure index of <0.90, which decreased by at least 15% after treadmill exercise. Two Doppler examinations measured the systolic pressure in the right and left posterior tibial arteries and in the right brachial artery, and the average of the 2 measurements was used to calculate the ankle–brachial pressure index (the lower ankle–brachial pressure index of the 2 legs was used for analysis). Twenty-eight subjects (25 men; mean age ± SD, 61 ± 10 y) who did not have PAD or CAD at coronary angiography and who were referred for functional evaluation of chest pain represented the control group. The decision to perform coronary angiography for these subjects was made by referring physicians. All PAD patients and control subjects underwent FMD evaluation followed by dipyridamole SPECT on the same day after withdrawal of all cardiac drugs for ≥18 h before the study. Angiotensin-converting enzyme inhibitors were used in 40% and 32% of PAD patients and control subjects, lipid-lowering agents were used in 66% and 36%, and calcium channel blockers were used in 53% and 28%, respectively. All abstained from smoking and intake of caffeine-containing food or beverages for at least 24 h before the study. The ethical committee of University Federico II approved the protocol, and each patient or control subject gave informed consent.
FMD Evaluation by Brachial Artery High-Resolution Ultrasound Imaging
Endothelial function evaluation was performed in the morning, after an overnight fast, in a quiet room at a constant temperature of 21°C ± 1°C, as previously reported (8). FMD was measured according to recent guidelines (19) with ultrasound unit electronic calipers (Image Point Hx; Hewlett Packard) and a 7.5-MHz linear-array transducer. Briefly, FMD was assessed by measuring the change in brachial artery diameter after 60 s of reactive hyperemia compared with a baseline measurement after deflation of a cuff that had been placed around the forearm and that had been inflated to 50 mm Hg above systolic blood pressure for 5 min. The diameter increase after sublingual nitroglycerin spray (0.4 mg) was used as a measure of endothelium-independent vasodilatation. The response of the vessel diameter to reactive hyperemia and to nitroglycerin was expressed as the percent change relative to the diameter immediately before cuff inflation and to the diameter immediately before drug administration, respectively. In the Department of Clinical Medicine, the intraobserver variability for repeated measurements of resting arterial diameter is 0.01 ± 0.02 mm (8). When reactive hyperemia studies are performed on 2 different days, the between-occasion, within-patient difference for measurements of FMD is 1.5% ± 0.7% (8).
Sestamibi Imaging
Dipyridamole was infused intravenously at a dose of 0.74 mg/kg of body weight over a period of 6 min with monitoring of symptoms and blood pressure and 12-lead electrocardiography. 99mTc-sestamibi at 555 MBq was injected intravenously as a bolus 1–2 min before completion of the stress. Dynamic planar images were acquired for 60 s (4 frames per second) in the anterior view to measure the first-transit counts in the pulmonary artery. SPECT was performed 60 min later. Data were acquired with a rotating single-head γ-camera (SP4HR; Elscint) connected to a dedicated computer system. No attenuation or scatter correction was applied. Rest imaging was performed on a separate day after the same acquisition protocol.
For first-pass analysis (16,17), serial images of the first-transit study were evaluated frame by frame, and on the summed image (3- to 5-s duration), a 3 × 2 pixel region of interest (ROI) at the main right pulmonary artery was assigned. After smoothing, the area under the time–activity curve was calculated to obtain the time integral of the first-pass tracer counts for the pulmonary artery (∫[C(t)dt]). Sestamibi activity was measured on 2 representative short-axis tomograms (at the medial–basal and medial–apical levels). For each short-axis tomogram, an epicardial global ROI was assigned, and tracer activity was expressed as absolute myocardial counts. Estimated MBF under stress and rest conditions was measured as myocardial counts divided by ∫[C(t)dt] (15–17). Estimated CFR was expressed as the ratio of MBF at stress to MBF at rest (16,17). The accuracy and reproducibility of this method were assessed previously in the Department of Biomorphological and Functional Sciences (17).
Statistical Analysis
Continuous data were expressed as mean ± SD, and categoric data were expressed as percentages. For continuous data, differences among groups were compared with 1-way ANOVA, checking for linear trends. If a significant F value was found by ANOVA, post hoc analysis with Bonferroni correction was performed. χ2 Analysis for categoric variables was used to assess differences among groups. The relationships among parameters were assessed by linear regression analysis. A P value of <0.05 was considered statistically significant.
RESULTS
All PAD patients and control subjects successfully completed the dipyridamole myocardial perfusion study without major side effects. Individual characteristics, FMD, and CFR for patients with PAD and for control subjects are reported in Tables 1 and 2, respectively. The prevalence of coronary risk factors was greater in PAD patients than in control subjects (degrees of freedom = 3, χ2 = 10.1, P < 0.02).
Individual Patient Data
Individual Control Subject Data
FMD in Control Subjects and in Patients
FMD was 11.4% ± 3.4% in control subjects and 6.9% ± 2.1% in patients with PAD (P < 0.0001). Conversely, no difference was observed for nitroglycerin-mediated vasodilatation between control subjects and PAD patients (11.2% ± 1.0% vs. 11.0% ± 1.2%; P was not significant). PAD patients were separated into 2 groups according to the median value of overall FMD (6.85%): group 1 (n = 15) with FMD above the median (mean ± SD, 8.78% ± 1.3%) and group 2 (n = 15) with FMD below the median (mean ± SD, 5.14% ± 0.94%). ANOVA showed a significant difference among groups (degrees of freedom = 57, F = 30.5, P < 0.0001), FMD being higher at post hoc analysis in control subjects than in both groups of PAD patients (P < 0.001 for both).
CFR in Control Subjects and in Patients
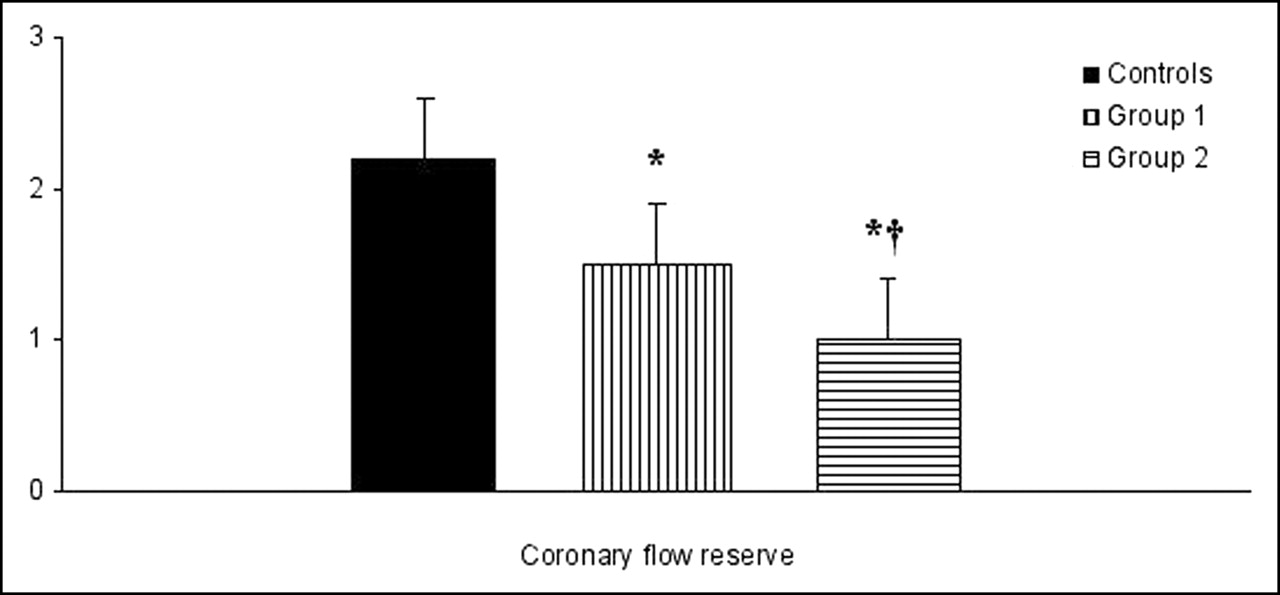
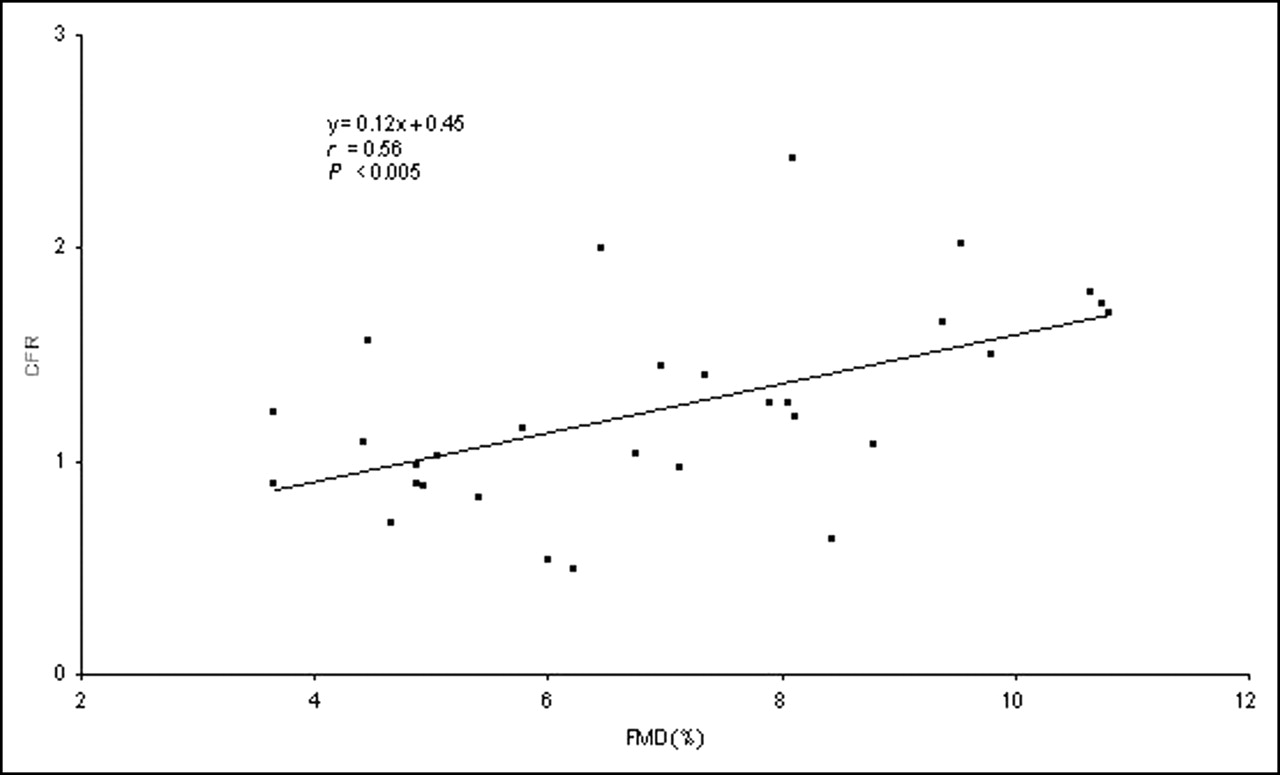
A significant difference in CFR among groups was found (degrees of freedom = 57, F = 30.5, P < 0.0001) (Fig. 1). In control subjects, estimated CFR was 2.2 ± 0.4—significantly higher than CFR in both groups of patients with PAD (P < 0.001 for both). Individual data analysis showed that 27 (90%) of PAD patients had CFR values below the 25th percentile (i.e., 2.0) of control subjects (Fig. 2). In addition, estimated CFR was significantly higher in PAD patients of group 1 than in PAD patients of group 2 (1.5 ± 0.4 vs. 1.0 ± 0.4) (P < 0.01). When all patients with PAD were considered, a significant correlation between FMD and estimated CFR was observed (r = 0.56, P < 0.005) (Fig. 3).
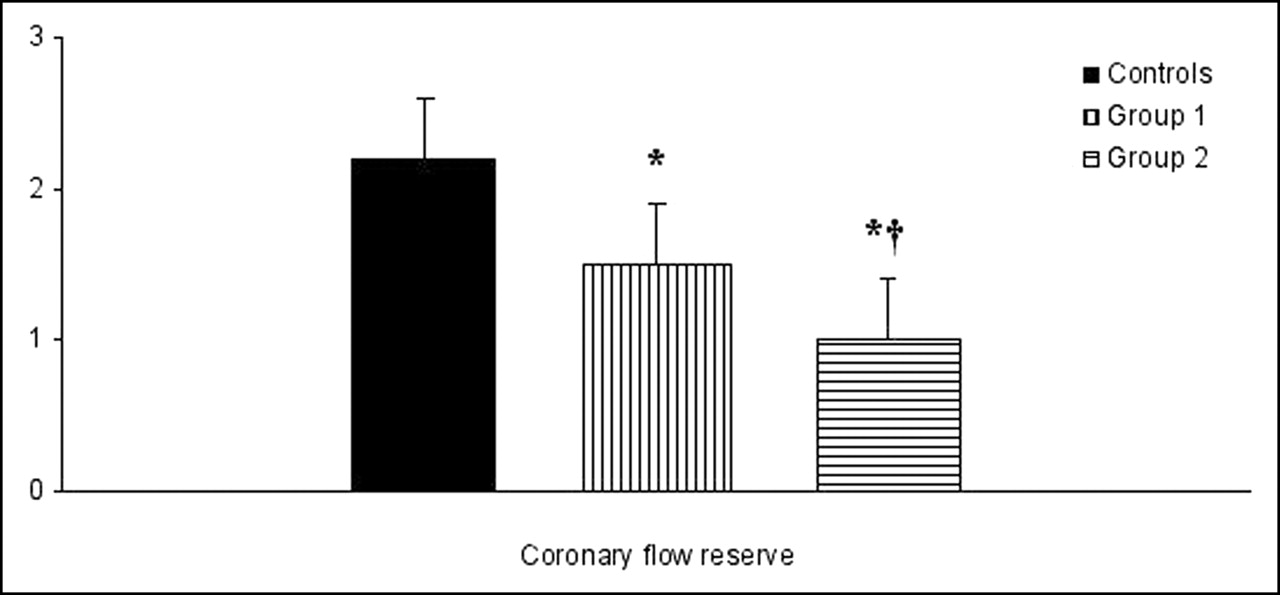
Mean ± SD CFR estimated by 99mTc-sestamibi imaging in control subjects (controls) and in patients with PAD and brachial artery FMD above (group 1) or below (group 2) median. *P < 0.001 vs. control subjects. †P < 0.001 vs. group 1.
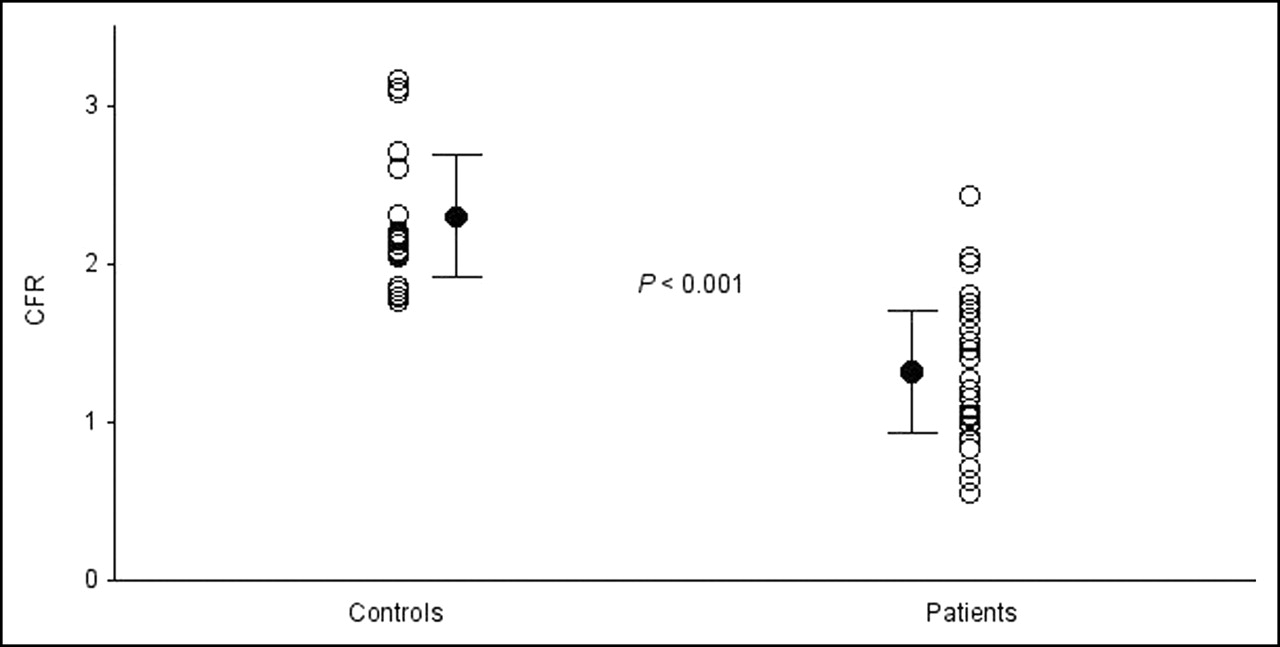
Individual values for CFR (○) estimated by 99mTc-sestamibi imaging in control subjects (controls) and in patients with PAD (patients). •, mean ± SD.
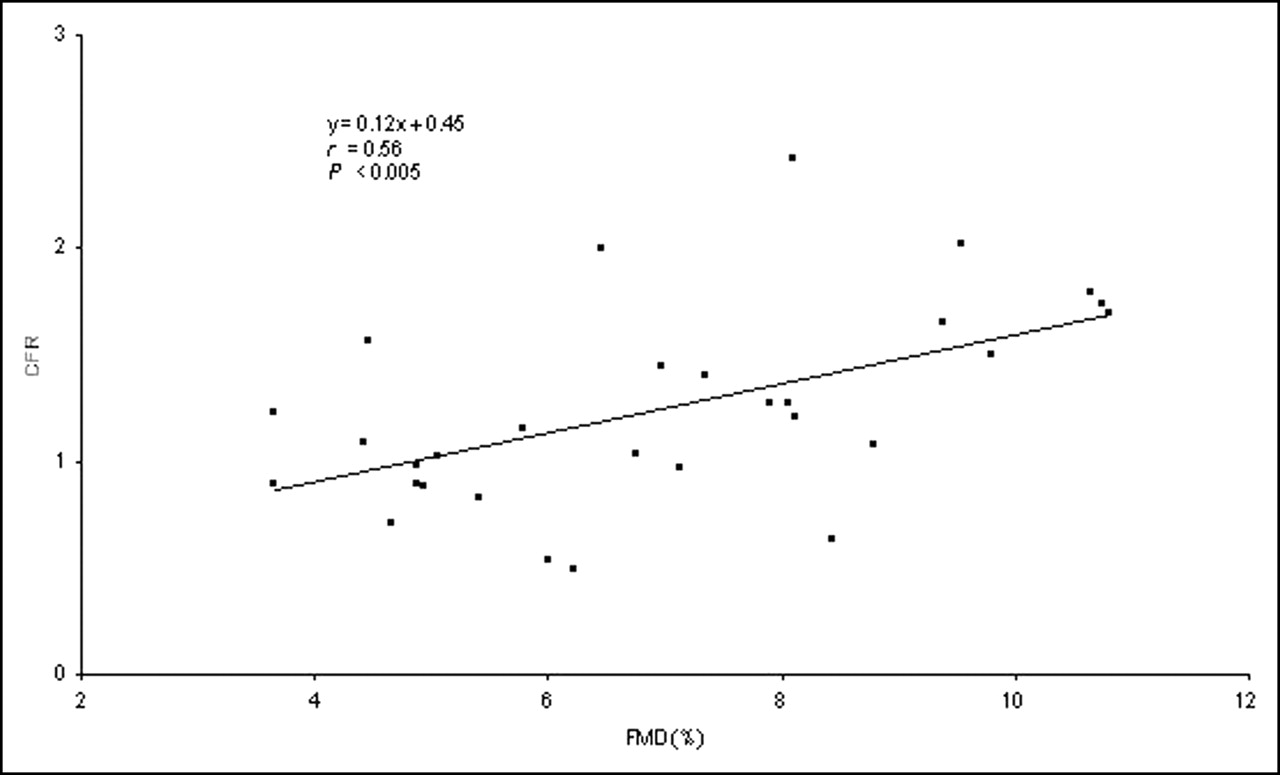
Relationship between brachial artery FMD and CFR estimated by 99mTc-sestamibi imaging in patients with PAD, with no cardiac symptoms, and without evidence of CAD at stress SPECT.
DISCUSSION
The results of this study demonstrate that estimated CFR is significantly lower in PAD patients without cardiac symptoms and with normal stress SPECT cardiac imaging results than in control subjects and that CFR impairment correlates with the severity of peripheral endothelial dysfunction.
Increased blood flow is an important cause of endothelium-mediated vasodilatation, which is reduced in pathophysiologic conditions (20). Loss of endothelium-dependent dilatation in systemic arteries occurs in the early preclinical stages of CAD, being associated with known coronary risk factors, such as advanced age, male sex, hypercholesterolemia, hypertension, smoking, and diabetes (21). Endothelial function can be evaluated in the coronary and peripheral circulation by monitoring the vasodilatation produced by the administration of endothelium-dependent agonists or by increased blood flow shear (8,22). At the myocardial level, CFR is an important indicator of the significance of coronary lesions as well as of other pathophysiologic conditions impairing coronary vasomotor function (23).
Recently, the results of attempts to estimate CFR with single-photon tracers achieved good agreement with the results obtained by invasive methods (15,17). For patients with multivessel CAD, Storto et al. (17) demonstrated that sestamibi imaging is an accurate and simple way to noninvasively estimate CFR with good inter- and intraobserver reproducibilities. This procedure is based on the microsphere method, which makes use of the fact that sestamibi is taken up by myocardium according to blood flow. Factors related to low resolution, such as scatter, attenuation, and partial-volume effects, hamper the absolute quantitation of both arterial and tissue counts, but they may be canceled out by computing the ratio of tissue and arterial counts. The accuracy of the arterial input function was improved by assigning an ROI at the pulmonary artery, avoiding spillover from bordering cardiac structures that can be observed with the ascending aorta (16). Estimation of CFR with single-photon tracers also has been validated by comparison with PET results (18), despite some underestimation at higher blood flow rates. Taki et al. (15) demonstrated that sestamibi retention increased as coronary flow velocity increased but reached a plateau at >2.5–3 times baseline flow velocity, confirming that the increase in the myocardial retention of 99mTc-labeled agents probably underestimates CFR at high flow rates because of tracer retention characteristics and kinetics. In particular, the reasons for this underestimation could be related, in large part, to the limited extraction of 99mTc-labeled tracers at high blood flow rates.
The brachial circulation and the myocardial circulation differ in terms of microvascular architecture and resistance, pattern of blood flow, metabolic regulation, and pathways that are activated to induce hyperemia (24). Nevertheless, the assumption that endothelial dysfunction detectable in brachial arteries is a manifestation of systemic dysfunction, including the coronary circulation, cannot be excluded because of the common underlying pathologic processes involved (25). In fact, a close correlation between peripheral endothelial function and coronary endothelial function was demonstrated previously in patients with CAD (9). Previous studies demonstrated that vasomotor dysfunction of epicardial coronary arteries is a predictor of cardiac events in patients without angiographic evidence of CAD (26,27). In addition, it was shown that many patients with chest pain and normal vessels at coronary angiography have early atherosclerosis, as documented by intravascular ultrasound, reduced CFR, and coronary endothelial dysfunction (28).
The results of the present study demonstrate that the impairment of endothelium-dependent vasodilatation in the coronary arteries can be demonstrated in patients who have PAD, who have no cardiac symptoms, and who have no evidence of CAD at stress SPECT. In addition, compromised CFR appears to be related to the degree of peripheral artery dysfunction. In our setting, the estimated CFR of PAD patients with moderate and severe impairment of arterial reactivity was 1.5 ± 0.4 and 1.0 ± 0.4, respectively. These observations were not dependent on the threshold value that was arbitrarily chosen to define the severity of impairment of arterial reactivity, as there was a significant correlation between FMD and CFR estimated by sestamibi imaging for the entire group of patients with PAD. In the present study, the prevalence of coronary risk factors was higher in patients with PAD than in control subjects. A higher prevalence of risk factors also may explain the lower FMD and CFR observed in PAD patients than in control subjects.
It has been extensively demonstrated that a negative stress myocardial perfusion study is predictive of a low rate of cardiovascular events in patients with suspected or known CAD (29,30). It also has been reported that in patients with PAD, a normal perfusion status is associated with a very low (3%) cardiac event rate (31). The results of the present study suggest that the assessment of CFR may be useful for risk stratification in patients with PAD and normal stress myocardial perfusion imaging results. More recently, Brevetti et al. (8) reported that FMD is also a powerful independent predictor of cardiovascular events in patients with PAD. Thus, it can be assumed that brachial artery FMD in patients with PAD correlates with the atherosclerotic coronary load, as reported by Kuvin et al. (10), who showed that in patients at high risk for cardiovascular events, preserved FMD was associated with a high prevalence of normal stress myocardial perfusion imaging results. In fact, in that study, an FMD of >10% was associated with a 95% likelihood of normal SPECT imaging results. The findings of the present study provide further support for this hypothesis, suggesting that estimated CFR may recognize a subset of PAD patients who have no evidence of functionally significant CAD but who are likely at high risk for cardiovascular events.
This study has some limitations that should be considered. We evaluated a relatively small number of patients, and coronary anatomy was not systemically evaluated in patients with PAD, because it would have been unethical to perform coronary angiography in asymptomatic subjects with normal stress SPECT cardiac imaging results. Thus, the possibility that coronary atherosclerosis was present in some PAD patients with normal SPECT cardiac imaging results cannot be excluded. However, it has been repeatedly reported that the functional assessment of myocardial perfusion is prognostically more relevant than coronary anatomy (29,30,32).
CONCLUSION
The results of the present study indicate that CFR estimated by sestamibi imaging is significantly lower in patients with PAD than in control subjects. In addition, CFR impairment correlates with the severity of peripheral endothelial dysfunction. Follow-up studies are warranted to verify whether reduced CFR identifies a subset of patients who have PAD and who are at increased risk for cardiovascular events.
Footnotes
Received Jun. 17, 2005; revision accepted Sep. 1, 2005.
For correspondence or reprints contact: Alberto Cuocolo, MD, Department of Biomorphological and Functional Sciences, University Federico II, Via S. Pansini, 5, I-80131 Napoli, Italy.
E-mail: cuocolo{at}unina.it
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Local Association Between Endothelial Dysfunction and Intimal Hyperplasia: Relevance in Peripheral Artery Disease
- Benefits of Statins in Elderly Subjects Without Established Cardiovascular Disease: A Meta-Analysis
- Endothelial Dysfunction in Diabetic Patients with Abnormal Myocardial Perfusion in the Absence of Epicardial Obstructive Coronary Artery Disease