


Abstract
The aim of this study was to determine the effect of perfusion defect and imaging sequence on the evaluation of myocardial stunning with gated perfusion SPECT. Methods: A dynamic mathematic cardiac torso phantom was used to create 100 gated SPECT simulations (50 stress-rest and 50 rest-stress sequences) with a wide range of perfusion defects. No segmental wall motion abnormalities were created. After generating projection images, 2 additional acquisitions were simulated by thresholding the projected data to 25% and 75% of the maximum. Finally, gated SPECT projections were grouped by 2s to generate 2 series of phantoms corresponding to stress-rest and rest-stress imaging sequences. For each sequence, the first dataset was the 25% thresholded gated SPECT. Both 75% thresholded and 100% signal intensity were used as a second dataset. Each simulated gated SPECT image differed from others in the extent of myocardial scar or ischemia, but all had the same end-diastolic volume (EDV) (125 mL), end-systolic volume (ESV) (48 mL), and ejection fraction (EF) (62%). Left ventricular perfusion and function were each assessed using validated software. Results: Mean stress EDV was decreased when compared with rest-simulated data (111 ± 4.7 and 112.4 ± 4.8 mL, respectively; P ≤ 0.05), and mean stress ESV was increased when compared with rest-simulated data (44 ± 4.2 and 42.7 ± 4 mL, respectively; P < 0.02). The resulting mean stress EF was decreased in the same comparison (60.3% ± 3.1% and 62% ± 2.7%, respectively; P = 0.0001). After multivariate analysis, the difference between stress and rest EF was significantly influenced by myocardial infarction (P = 0.0027), severe extent of myocardial ischemia (P = 0.0017), and imaging sequence (P < 0.0001). A ≥5% decrease in EF on stress SPECT (i.e., myocardial stunning) was significantly associated with the stress-rest sequence (χ2 = 26; P < 0.0001). Conclusion: Perfusion defects and imaging sequence had significant effects on the evaluation of myocardial stunning using gated perfusion SPECT.
Gated myocardial perfusion SPECT enables analysis of wall motion, wall thickening, and ejection fraction (EF) measurements with a combined assessment of myocardial perfusion and ventricular function by a single injection of a radiopharmaceutical agent. Although left ventricular (LV) volume determination requires endocardial edge detection based on myocardial perfusion, it has been demonstrated that gated SPECT provides reliable information on global LV function even in patients with large perfusion defects (1–4). Gating of both rest and poststress perfusion SPECT data is feasible, and a high correlation has been reported between the severity of reversible perfusion defects (i.e., ischemia) and a drop in poststress LVEF (i.e., myocardial stunning) (5–8). However, it remains unclear whether this stress-induced drop in EF is related only to myocardial stunning or may be influenced by variations in myocardial perfusion between poststress and rest gated SPECT in patients with coronary artery disease or myocardial ischemia.
When using a same-day protocol, different amounts of radioactivity injected at rest and at stress could potentially influence the evaluation of LV function. In the past, comparison of a rest-stress with a stress-rest 1-d technique showed that the rest-stress protocol had advantages in demonstrating ischemia in segments that were interpreted as being fixed on the stress-rest protocol (9). However, only limited data are available about the effect of imaging sequence (rest-stress or stress-rest) on the evaluation of LV function (10). When compared with studies in patients, phantom studies have the advantage of allowing control of parameters that may influence either image quality (count statistics or imaging sequence) or the occurrence of myocardial stunning, including the amount and severity of ischemia.
The aim of this study was to assess the respective effects of perfusion defect and image acquisition sequence on evaluation of global LV function using perfusion gated SPECT in a phantom with different degrees of disease, as a step to developing a large simulated patient database.
MATERIALS AND METHODS
The Dynamic Mathematic Cardiac Torso Phantom
All simulated data for this study were generated using the dynamic 3-dimensional (3D) mathematic cardiac torso phantom (dMCAT 2.01) developed at the University of North Carolina at Chapel Hill (11). All generated hearts had the same LVEF (62%), end-systolic volume (ESV; 48 mL), and end-diastolic volume (EDV; 125 mL). This phantom consists of geometric approximations of various organs inside the human upper torso, which can be used to compute radionuclide uptake distribution. According to previous results, 16 frames per cycle were used to represent the heart motion during a single cardiac cycle to minimize temporal undersampling bias (12). The distribution of 99mTc-labeled sestamibi was chosen for modeling the phantom. Compared with the heart, the relative radioactive intensities in soft tissue, blood, lung, liver, kidney, and spleen were 0.03, 0.03, 0.053, 1, 1, and 0.8, respectively. The source distribution was sampled at 64 × 64 pixels with a pixel size of 6.25 mm/pixel. Heart rotation and apical thinning were included in the phantom simulation, but respiratory motion was not included.
Perfusion defects were created separately as localized regions of myocardial uptake. These were scaled relative to the normal wall concentration and then subtracted from the normal heart to yield regions of reduced uptake. Two anterior defects were created: 1 “small” defect approximating half the anterior myocardial wall, and 1 “large” defect calculated as twice the latter defect and approximating the anterior myocardial wall supplied by the left anterior descending artery. As previously described, each defect was scaled to 50%, 75%, and 95% of the activity concentration of the heart and then subtracted from the normal heart (13). No segmental wall motion abnormalities were created, so that LVEF remained unchanged in all simulated datasets, regardless of the defect added. Thus, 7 phantoms were created: 1 normal, 3 with a small perfusion defect, and 3 with a large perfusion defect.
Simulation of Gated SPECT Imaging
Projections were generated using a 3D ray-driven projector. Further image manipulations were performed using ImageJ 1.29w software (ImageJ; National Institutes of Health). To simulate collimator blurring, a gaussian stationary 2D blur was added after generating projections. For each dataset, 2 additional acquisitions were simulated by thresholding the projected data to 25% and 75% of the maximum, leading to 21 sets of simulated gated SPECT projection data. Then, a uniform gaussian noise was added (SD = 10) to each dataset. Finally, gated SPECT projection datasets were grouped 2 by 2 to simulate patient data. The effect of scatter was not simulated.
Two series of simulated patients were generated corresponding to 2 different imaging sequences: stress-rest and rest-stress. For each sequence, the first dataset was the 25% thresholded gated SPECT. Both 75% thresholded and 100% signal intensity (SI) were used as a second dataset, corresponding respectively to a 3- and 4-fold increase over the amount of radiotracer usually injected in the clinical setting (14). The rearrangement of datasets with different defect sizes and intensities led to the generation of a wide range of simulated myocardial infarction and ischemia. These simulated patients corresponded to normal scans (n = 4), myocardial infarction without ischemia (n = 24), myocardial ischemia without infarction (n = 24), and myocardial infarction with residual ischemia (n = 48).
As a result, 100 simulated datasets were created, corresponding to 50 simulated patients examined twice using both stress-rest and rest-stress sequences. Simulated datasets differed in the amount of myocardial scar or ischemia, but all had the same EDV (125 mL), ESV (48 mL), and EF (62%), with no segmental wall motion abnormalities.
Image Reconstruction and Processing
All projection data were reconstructed and reoriented into 3 orthogonal views with an automated algorithm (MyoSPECT, Vision 5.0.2; GEMS) using filtered backprojection with a Butterworth filter (order, 5.0; cutoff frequency, 0.30 cycles/pixel). For each reconstruction, LV volumes were calculated using automated processing with QGS software (Cedars Sinai Medical Center) (15). Perfusion was evaluated on summed nongated images using QPS. This software analysis starts with LV segmentation and the extraction of the 3D endocardial and epicardial surfaces as described for gated and nongated SPECT (16). Perfusion at each myocardial sampling point is calculated as the average uptake along a count activity profile (from endocardium to epicardium) normal to the myocardium and passing through that point. In areas of apparent absence of perfusion, endocardial and epicardial surfaces are derived using rule-based criteria ensuring the continuity of surface myocardial count profile. As previously validated, relative segmental myocardial uptake is evaluated using a 20-segment model of the LV and automatically rated using a 5-point scale (from 0 = normal uptake to 4 = no uptake) analogous to that usually used for visual scoring (16,17). Summed stress score (SSS), summed rest score (SRS), and summed difference score (SDS) were automatically calculated for each simulated patient with reference to a normal male 99mTc-sestamibi SPECT database.
Statistical Analysis
Data were expressed as mean value ± 1 SD. Differences between volumes and EFs were calculated using an appropriate paired or unpaired t test. The impact of qualitative parameters on continuous data was evaluated by multiple ANOVA. The interaction between qualitative parameters was tested by the χ2 test. A P value ≤ 0.05 was considered statistically significant.
RESULTS
The mean values of EDV, ESV, and EF within the 21 originally simulated gated SPECT datasets (before rearrangement) are shown in Table 1. The accuracy of EDV, ESV, and EF measurements was high, ranging respectively from 86% to 95%, 84% to 97%, and 94% to 103% of the true phantom parameters values.
End-Diastolic and End-Systolic Values and Ejection Fractions for Defect Severities in Simulated Phantoms
As shown in Table 2, image SI did not significantly influence the measurement of EDV and ESV. However, LVEF was significantly reduced in 25% SI data compared with 100% SI data (60% ± 3% and 63% ± 1%, respectively; P = 0.01).
Effect of Signal Intensities on Assessment of Left Ventricular Volumes and Ejection Fraction
Impact of Image Sequence
Mean stress EDV was decreased when compared with rest-simulated data (111 ± 4.7 and 112.4 ± 4.8 mL, respectively; P ≤ 0.05), and mean stress ESV was increased when compared with rest-simulated data (44 ± 4.2 and 42.7 ± 4 mL, respectively; P < 0.02). The resulting mean stress EF was decreased in the same comparison (60.3% ± 3.1% and 62% ± 2.7%, respectively; P = 0.0001).
As illustrated in Figure 1, calculated stress EDV was decreased, stress ESV was increased, and stress EF was decreased on simulated stress-rest sequences compared with rest-stress data. In contrast, rest EDV was increased, rest ESV was decreased, and rest EF was increased on simulated stress-rest sequences compared with rest-stress sequences. Consequently, the difference (ΔEF) between stress and rest EF (stress EF − rest EF) was more significant when using the stress-rest sequence (−4.8% ± 3%) than the rest-stress sequence (1.3% ± 3.2%; P < 0.0001).

Values of LVEF, EDV, and ESV for stress (Ex)- and rest (Rest)-simulated acquisitions for each imaging sequence (stress-rest [black] and rest-stress [white]).
Mean SSS and SRS were similar in the stress-rest sequence (23.4 ± 5.6 and 12.8 ± 9, respectively) and the rest-stress sequence (21.9 ± 7.7, not significant; and 15.7 ± 8.9, not significant, respectively), but SDS was higher when calculated on the stress-rest sequence than with the rest-stress sequence (10.6 ± 8.4 and 6.2 ± 8.5, respectively; P = 0.01).
Impact of Perfusion Defect
In the generated phantoms, the mean SSS, SRS, and SDS were 22.7 ± 6.7 (range, 0–30; median, 26), 14.3 ± 9 (range, 0–30; median, 14.5), and 8.4 ± 8.7 (range, −9 to 27; median, 7.5), respectively. Summed perfusion scores were categorized according to their median values (SSS = 26; SRS = 14.5). In phantoms with large stress perfusion defects (SSS ≥ 26), stress EDV was lower (109.5 ± 4.1 mL), stress ESV was higher (44.8 ± 4.4 mL), and stress EF was decreased (59.1% ± 3%) compared with the same parameters in phantoms with smaller stress perfusion defects (113.1 ± 4.7 mL, P < 0.0001; 43.1 ± 3.9 mL, P < 0.05; and 62% ± 2.4%, P < 0.0001, respectively). Similarly, in phantoms with large rest perfusion defects (SRS ≥ 14.5), rest EDV (113.3 ± 5.5 mL) was not statistically different, rest ESV (44.6 ± 4.7 mL) was increased, and rest EF (60.8% ± 3%) was decreased compared with the same parameters in a phantom with smaller rest perfusion defects (111.6 ± 3.9 mL, not significant; 40.8 ± 2.1 mL, P < 0.0001; and 63.4% ± 1.3%, P < 0.0001, respectively).
In phantoms with simulated myocardial infarction (i.e., with a rest perfusion defect, whatever the size) rest EDV was not different from those without myocardial infarction (112.5 ± 5.1 mL and 112.1 ± 4 mL, respectively). In contrast, rest ESV was increased in phantoms with simulated myocardial infarction compared with those without (42.7 ± 4.1 mL and 40.1 ± 2.5 mL; P < 0.0001), and consequently, EF was significantly decreased (61.3 ± 2.8 vs. 64 ± 0.8; P < 0.0001).
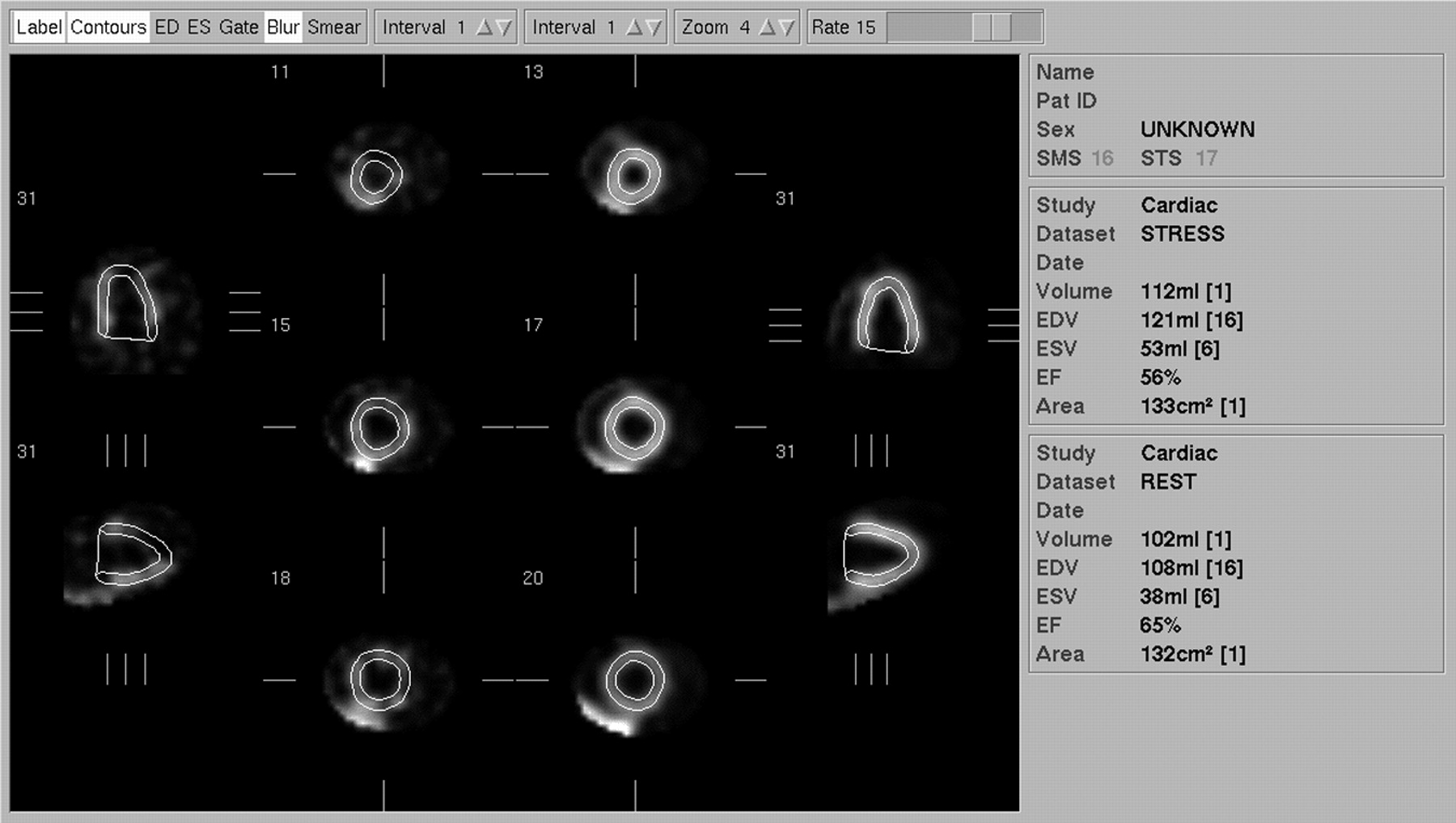
Finally, ΔEF was significant in phantoms with ischemia compared with the same value in phantoms without ischemia (−2.4% ± 4.2% and 0% ± 4.2%; P < 0.02). Moreover, linear regression demonstrated a significant correlation between ΔEF and the amount of ischemia evaluated by SDS (Fig. 2). Figure 3 is an example of a simulated stress-rest sequence, with significant ischemia and without infarction, showing a 9% drop in poststress EF.
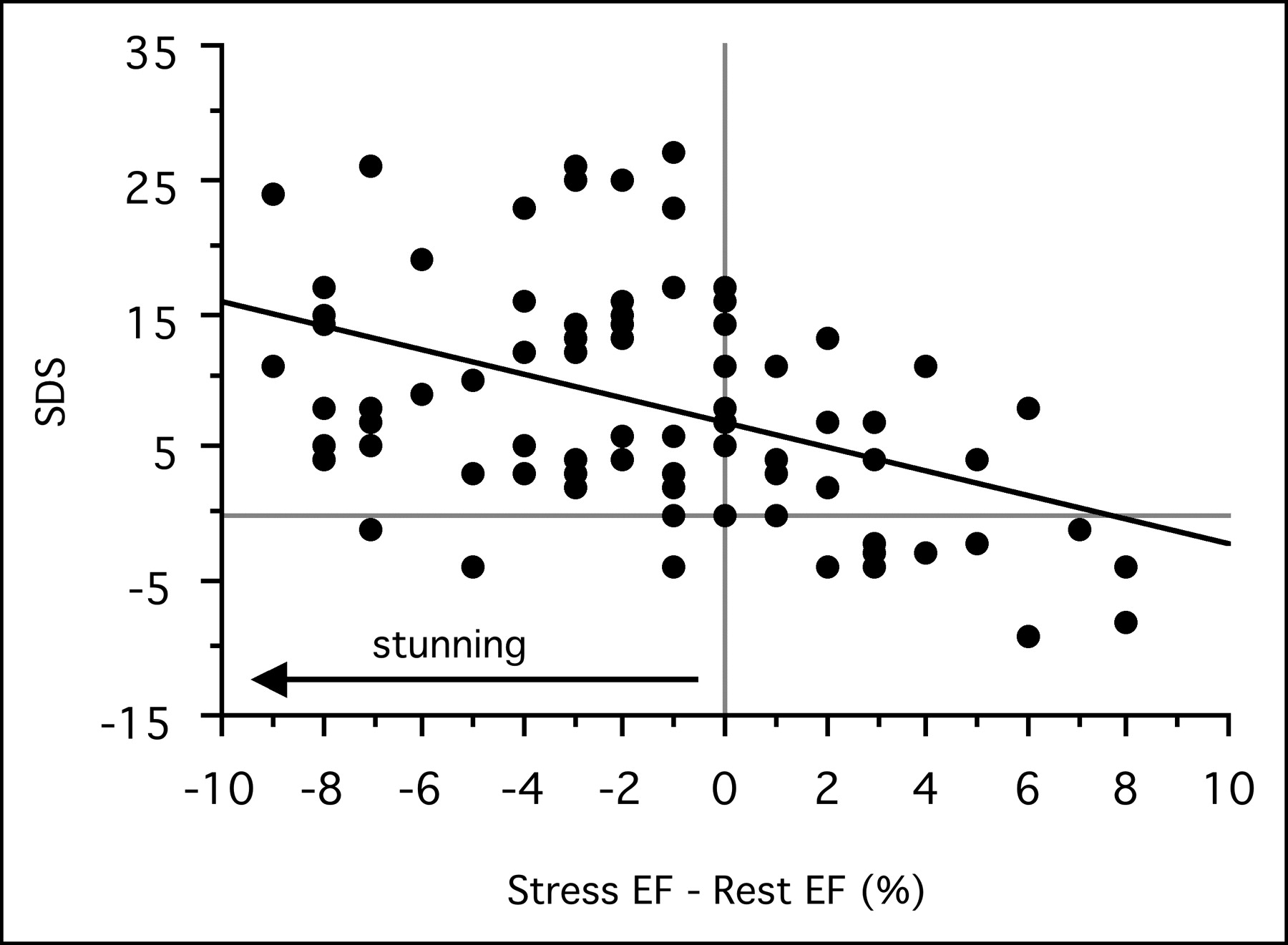
Correlation between ΔEF and amount of ischemia evaluated by SDS. y = 6.815–0.911 × x; r = 0.46; P < 0.0001.
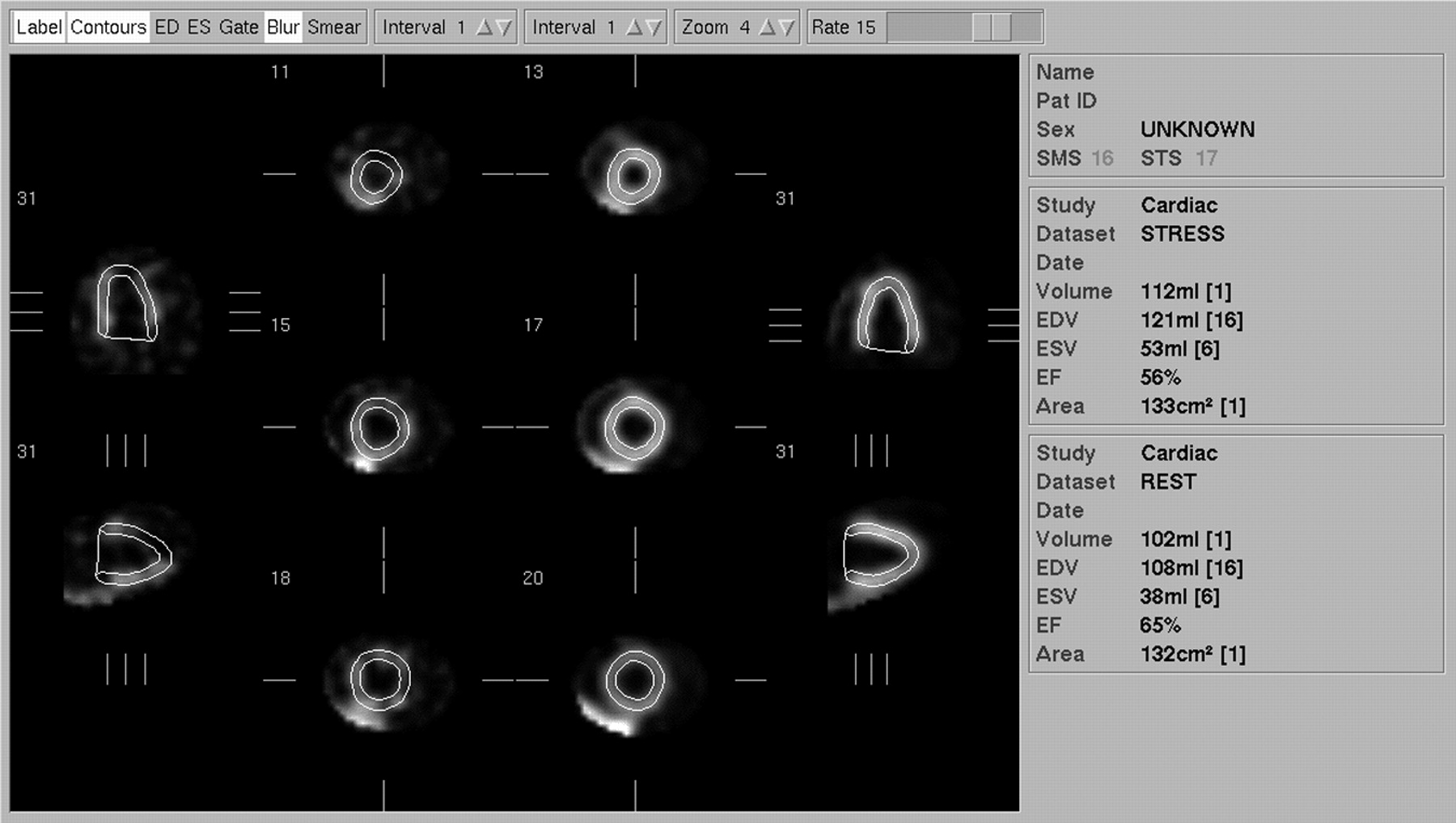
Simulated stress-rest sequence showing myocardial ischemia (SSS = 26; SRS = 2; SDS = 24) and a 9% EF decrease on poststress images (stress EF = 56%; rest EF = 65%).
Multivariate Analysis
The results of multivariate analysis are summarized in Table 3. The presence of myocardial infarction significantly influenced the results of measured rest EDV, rest EF, ΔESV, and ΔEF. The presence of large ischemia (SSS = 26) significantly influenced the results of measured stress EDV, stress EF, and ΔEF. Finally, the simulated acquisition sequence significantly influenced the results of measured stress ESV, stress EF, rest EDV, rest EF, ΔEDV, ΔESV, and ΔEF. The most important factor that influenced the difference between stress and rest EF was the acquisition sequence (F value = 58; P < 0.0001). Considering the variation of EF between stress and rest conditions, there was a significant interaction between the presence of myocardial infarction and the choice of acquisition sequence (F value = 14.5, P < 0.002). As illustrated in Figure 4, in phantoms with myocardial infarction, stress worsening of EF was observed only with the simulated stress-rest sequence.

Variation of EF between stress and rest (ΔEF) acquisitions (stress-rest [black] and rest-stress [white]). MI = myocardial infarction.
Multivariate Analysis
Finally, myocardial stunning was defined as a 5% decrease in EF on stress compared with rest SPECT. Although no stunning was present (EF = 62% in all simulations), 24 phantoms (24%) showed myocardial stunning. As shown in Table 4, 23 of those 24 cases (96%) were observed with the stress-rest imaging sequence, resulting in a high association between the stress-rest sequence and the occurrence of myocardial stunning (χ2 = 26; P < 0.0001).
Association Between Imaging Sequence and Observation of Myocardial Stunning*
DISCUSSION
This study examined the impact of perfusion pattern and imaging sequence on the accuracy of gated perfusion SPECT in determining LV volumes and EF. Absolute results were considered accurate for the evaluation of LV function, but there was a significant influence of low SI on the measurement of EF. When combining data from different SIs to simulate patient acquisitions, we found that both myocardial perfusion and imaging sequence had a significant influence on LV function assessment. Large perfusion defects resulted in an EF decrease as measured by quantitative gated SPECT. Similarly, the use of a stress-rest sequence and not a rest-stress sequence resulted in a reduced stress EF. Consequently, a myocardial stunning artifact was frequently observed when using the stress-rest acquisition sequence.
The accuracy of quantitative gated SPECT has been widely investigated and validated (2,15,18–20). In this study, we used a computer simulation with systolic and diastolic volume parameters within published normal ranges (21–23). As previously described, SI influenced the measurement of EF, with lower EF observed on the 25% than the 100% SI acquisition. Using a similar mathematic cardiac torso phantom simulation and the same quantitative gated SPECT software, Achtert et al. (13) found a comparable 3% underestimation of EF at the lower count levels.
The effect of perfusion defect on assessment of LV function has been suggested but not yet clearly demonstrated (2,4). Several studies have shown an underestimation of LVEF measured by means of gated SPECT compared with planar radionuclide angiography in patients with perfusion defects (2,20). However, those perfusion defects were observed in patients with large myocardial infarction and LV dysfunction. To our knowledge, the effect of large isolated perfusion defects without ischemic LV dysfunction has not been reported. In the present study, perfusion defect significantly influenced the assessment of LV function by affecting EDV or ESV measurement as well as the resulting EF. Poststress EDV and ESV increased and EF decreased in simulated phantoms with large stress perfusion defects. At rest, EF decrease was related to ESV increase without significant EDV increase. Moreover, multivariate analysis confirmed the independent impact of rest and stress perfusion defect on the evaluation of LVEF. This interaction between myocardial perfusion and EF had a major effect on the occurrence of pseudo myocardial stunning, as demonstrated by a 2.4% fall in poststress EF in phantoms with myocardial ischemia. Myocardial stunning (or postischemic dysfunction) is a mechanical dysfunction induced by a brief episode of severe ischemia, which, despite the absence of irreversible cellular damage, persists after the recovery of normal coronary blood flow (24). The total recovery of contractile function may require minutes to weeks, depending on the intensity and duration of the ischemic episode. This phenomenon has been demonstrated in clinical settings of transient ischemia and reperfusion, including myocardial infarction, unstable angina, and coronary artery bypass grafting (25). Several echocardiographic studies have demonstrated that stunning may occur after treadmill exercise (26,27). Poststress myocardial stunning also has been observed in patients with coronary artery disease when examined with gated perfusion SPECT, using both 201Tl- and technetium-labeled tracers (5,6,8,28–30). However, in those gated SPECT studies, it remains unclear whether a decreased poststress EF reflected only myocardial stunning or a combination of stunning and perfusion-related artifacts. Heiba et al. (6) found a >5% decrease in EF after stress in 20 (45%) of 44 patients with myocardial ischemia. Using 99mTc-sestamibi gated SPECT, Johnson et al. (8) found similar results in 22 (36%) of 61 patients with reversible perfusion defects, although gated SPECT acquisitions were performed 30 min after the completion of exercise. In a similar population evaluated using exercise and recovery radionuclide angiography, Ambrosio et al. (31) emphasized that global EF decreased during exercise in the presence of severe coronary artery disease and ischemia. In the latter study, EF returned to baseline within 10 min, although regional LV function in the ischemic area remained substantially impaired 60 min into recovery. However, delayed recovery of a stress-induced global LV dysfunction can be observed in patients with major myocardial ischemia and regional dysfunction during stress, as a result of severe coronary artery disease (32).
In our study, the most important factor influencing the difference between stress and rest EF was the acquisition sequence. When simulating a stress-rest imaging sequence, the underestimation of EF as a result of low SI after stress was incremental with the underestimation related to perfusion abnormalities. As the signal increased on the second simulated acquisition (i.e., rest) and perfusion improved in the ischemic pattern, the conditions for underestimating EF were no longer present at rest. The consequence of these transient conditions was the appearance of a “pseudo stunning” (defined as a 5% decrease in EF) in 23 of 50 (46%) simulated stress-rest acquisitions, although all original simulated phantoms had the same EF. On the other hand, this phenomenon was observed in only 1 rest-stress acquisition where the lower SI acquisitions were used at rest and did not interfere with the largest perfusion abnormalities observed at stress.
In a recent gated SPECT study, Hashimoto et al. (7) assessed cardiac function immediately and 20 min after a single peak exercise injection of 99mTc-sestamibi. In patients with no coronary artery stenosis or scintigraphic evidence of ischemia, there was an overshot of EF immediately after exercise that returned to normal 20 min later. In patients with mild-to-moderate ischemia, EF remained unchanged immediately after exercise and at 20 min thereafter. Finally, in 11 of 47 (23%) patients with severe myocardial ischemia, baseline EF was 53.6% ± 8% and significantly decreased on postexercise scans (45.6% ± 12.1%; P < 0.01). Twenty min after exercise, EF further increased to 49.7% ± 10.7% without reaching the baseline level. In this subgroup, the authors used a rest-stress protocol, and in the absence of significant redistribution of 99mTc-labeled tracers, myocardial perfusion uptake did not differ at 5 and 20 min after stress acquisition. The mean poststress EF decrease was 8%, which is much more significant than the 5% cutoff usually used for assessing myocardial stunning in gated SPECT studies.
Borges-Neto et al. (10) evaluated the difference between poststress and rest EF by using a same-day perfusion-function protocol in 126 patients. Patients with and without ischemia had significant differences in poststress versus rest EF (−4.0% and 1.0%, respectively; P < 0.01). In a subgroup analysis of those with and without ischemia, the authors concluded that stress-rest (−2.5% and 1.0%, respectively; P = < 0.05) and rest-stress (−4.0% and 1.0%; P = 0.006) protocols yielded similar results. Nevertheless, this latter study has several limitations. First, patients undergoing exercise (74%) and pharmacologic stress test were pooled. Second, 39 patients underwent a stress-rest protocol whereas many more patients (87) underwent a rest-stress protocol. Third, poststress images were obtained 30 min after the stress injection, a delay that probably underestimated the magnitude of EF changes (7). Finally, the absence of statistical analysis of the impact of imaging sequence on the difference between poststress and resting EF did not allow a final conclusion from this series.
Our study had some limitations. All defects were placed in the anterior wall. However, the reliability of quantitative programs may be more affected by an inferior defect, particularly in the presence of high liver activity. Based on a similar dynamic mathematic cardiac torso phantom simulation, Achtert et al. (13) demonstrated that with an increased hepatic uptake of 2 or more times the normal heart uptake, no meaningful EF could be obtained. Consequently, the introduction of a hot liver spot or a severe inferior defect could potentially affect the intrinsic capabilities of the QGS program itself. In this case, it would be impossible to statistically characterize the impact of perfusion defect size, because of the strong interaction between the defect location and QGS properties. For similar statistical considerations we decided to use image sets that were identical with regard to LV chamber sizes, and our results may not be extrapolated to either small or dilated hearts. The investigation of the impact of LV chamber size, as well as transient dilation, would require a specific study design.
The QGS program is a geometry-based algorithm and may be affected by count density, background changes, filtering, and heart size. Using a computer simulation and a patient database, Nakajima et al. (33) recently found high correlations between QGS and 3 available programs (4D-MSPECT [University of Michigan], ECT [Emory University], and pFAST [Sapporo Medical University School of Medicine]) for rest EDV and EF assessment, but they did not evaluate the impact of transient LV dysfunction or imaging sequence. In the current study, our goal was to investigate the impact of these latter factors but not to compare geometry versus count-based methods for EF measurement. It remains questionable whether similar results would be obtained with other available programs that are potentially less dependent on geometry for estimation of left ventricular boundaries.
CONCLUSION
Both imaging sequence and perfusion abnormalities influenced the measurement of LV volumes and EF with gated myocardial perfusion SPECT. To avoid these effects in assessing stress-induced LV dysfunction, the rest-stress protocol may be preferable to the stress-rest protocol. Moreover, when using the stress-rest imaging sequence, a poststress EF decrease potentially reflects changes in myocardial perfusion as well as true myocardial stunning.
Acknowledgments
The authors would like to thank Karen J. Lacroix and Benjamin M. Tsui for use of the dMCAT phantom developed at the University of North Carolina at Chapel Hill, and Richard Medeiros for his advice in editing the manuscript.
Footnotes
Received Mar. 18, 2004; revision accepted Sep. 13, 2004.
For correspondence or reprints contact: Alain Manrique, MD, Département de Médecine Nucléaire et Laboratoire Universitaire Quant.IF. Centre Henri Becquerel, 1 rue d’Amiens, 76000 Rouen, France.
E-mail: alain.manrique{at}rouen.fnclcc.fr





{kind=link}
{kind=link}
{kind=link}
{kind=link}