


Abstract
Although ventilation/perfusion (V/Q) lung scintigraphy is a well-accepted and frequently performed procedure in the diagnosis of pulmonary embolism, there is growing controversy about its relevance, particularly due to the increasing competition between scintigraphy and CT. Even though comparative studies between both modalities have already been performed, their results were highly inconsistent. Remarkably, in most of those studies, conventional planar perfusion scans were compared with tomographic images acquired using state-of-the-art CT scanners—a study design that cannot give impartial results. Hence, the aim of our study was a balanced comparison between V/Q lung scintigraphy and CT angiography using advanced imaging techniques for both modalities. Methods: A total of 83 patients with suspected pulmonary embolism were examined using V/Q lung scintigraphy in SPECT technique as well as 4-slice spiral CT. Ventilation scans were done using an ultrafine aerosol. Additionally, planar images in 8 views were extracted from the V/Q SPECT datasets. Two experienced referees assessed each of the 3 modalities. The final diagnosis was made at a consensus meeting while taking into account all of the imaging modalities, laboratory tests, clinical data, and evaluation of a follow-up period. Results: In the course of the consensus conference, pulmonary embolism was diagnosed in 37 of the 83 patients (44.6%). Compared with planar scintigraphy, SPECT raised the number of detectable defects at the segmental level by 12.8% (+11 defects; P = 0.401) and at the subsegmental level by 82.6% (+57 defects; P < 0.01). The sensitivity/specificity/accuracy of planar V/Q scintigraphy and V/Q SPECT was 0.76/0.85/0.81 and 0.97/0.91/0.94, respectively, compared with 0.86/0.98/0.93 for multislice CT. Conclusion: SPECT and ultrafine aerosols are technical advancements that can substantially improve lung scintigraphy. Using advanced imaging techniques, V/Q scintigraphy and multislice spiral CT both yield an excellent and, in all aspects, comparable diagnostic accuracy, with CT leading in specificity while SPECT shows a superior sensitivity. Even though planar lung scintigraphy yields satisfactory results for a nontomographic modality, it does not compare with tomographic imaging.
Since its introduction in 1964, ventilation/perfusion (V/Q) lung scintigraphy has developed into one of the major imaging procedures for diagnosing pulmonary embolism (1–3). Milestones were the prospective McMaster’s and PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) studies, which led to a significant method refinement (4–7). Currently, new challenges arise in the form of competing radiologic procedures such as CT and—to a lesser degree—MRI. Although MRI of patients with pulmonary embolism is still in an experimental stage and, therefore, inappropriate for diagnostic routine, CT has shown promising results (8–15). According to the literature, however, evidence was found that CT may have a relatively low sensitivity with regard to subsegmental embolisms. Single-slice CT seems to be particularly affected (14,16–18) while multidetector row scanners produce distinctly better results (19,20). Since the detection of subsegmental embolism is one of the strong points of V/Q scintigraphy, a comparison between both methodic approaches seems to be in order.
Several studies have compared V/Q scintigraphy with pulmonary CT angiography. However, their results are highly inconsistent and lead to contradicting recommendations and conclusions (12–15,17,21–23). Remarkably, in most of those studies, a modern tomographic modality is compared with planar perfusion scintigraphy acquired using a technique similar to that of the PIOPED study, which was designed in 1983 (24). Recent advances in acquisition technique, image reconstruction, or image analysis are rarely considered. Moreover, ventilation scans are sometimes neglected altogether or performed in an outdated technique. Hence, in most of those studies, a modern tomographic modality is compared with an older planar one—a study design that cannot give impartial results.
Therefore, the aim of the present study was a balanced comparison between V/Q lung scintigraphy and CT angiography using advanced imaging techniques for both modalities. To that end, CT was done using a state-of-the-art 4-slice scanner, whereas the V/Q lung scans were acquired by SPECT. SPECT acquisitions of the ventilation were performed using an ultrafine aerosol. To assess the effect of SPECT on the diagnostic accuracy of V/Q lung scans compared with conventional scintigraphy, planar images were extracted from the SPECT datasets and evaluated separately. Special care was taken to analyze the diagnostic ability of all 3 modalities with regard to subsegmental embolism. Finally, we determined whether the PIOPED criteria can be applied to tomographic V/Q scans without modification or if reassessment is in order.
MATERIALS AND METHODS
Subjects
A total of 83 patients (36 men, 47 women; mean age, 53.9 ± 19.5 y; age range, 18–88 y) were examined between January 2001 and April 2003. The subjects were chosen from a pool of 546 CT examinations and 542 V/Q lung scans performed during that period on patients with suspected pulmonary embolism. The retrospective study was designed according to the regulations of the local board for protection of data privacy and confidentiality. Only those patients who had V/Q lung scintigraphy in SPECT technique as well as multislice spiral CT within an interval of 3 d were included in the study. Although 41 patients (49.4%) had both examinations done on the same day, the mean time between CT and scintigraphy was 1.7 d. The maximum interval of 3 d was chosen because the endogenous lysis of even small pulmonary clots takes at least 2–3 d, whereas larger clots cannot be lysed endogenously in less than a week (25). The only way to significantly accelerate the lysis of thrombotic clots is fibrinolytic therapy and, even under such treatment, thrombolysis takes between 48 h and 13 d (26). No one included in the study received fibrinolytic therapy because it is indicated solely in hemodynamically unstable patients due to the overall incidence of major hemorrhage of about 12% (27). On the other hand, a medication with heparin was not considered to interfere with our study design because heparin does not accelerate lytic processes. Instead, its effectiveness is based exclusively on an impairment of clot growth and the prevention of recurrent thromboembolism (27).
V/Q Scintigraphy: SPECT
The V/Q lung scintigraphy was performed exclusively in SPECT technique using a double-head and a triple-head γ-camera equipped with low-energy, high-resolution, parallel-hole collimators (ECAM and MultiSPECT 3; Siemens). Ventilation scans were done after inhalation of 485 ± 72 MBq 99mTc-technegas over 3–5 respiratory cycles. Technegas is an ultrafine aerosol that is considered to behave truly like a gas due to a mean aerodynamic diameter of the particles between 30 and 90 nm. Because of the small particle size, the degree of efficiency reaches values of up to 20% (28–30). Here, the degree of efficiency is defined as the ratio between the amount of applied activity and its actual pulmonary deposition. By comparison, conventional aerosol devices produce particles with a mean aerodynamic diameter of about 450 nm and show a degree of efficiency between 1% and 3% (28,29). As a drawback, the application of 500 MBq 99mTc-technegas leads to a radiation exposure of up to 1.5 mSv, which is higher than that from ventilation agents such as 99mTc-diethylenetriaminepentaacetic acid, 133Xe, or 81mKr. For preparation of the ultrafine aerosol, a special furnace device is required (Technegas Generator; Vita Medical Ltd.). In this furnace device, 99mTc-O4 is vaporized in graphite crucibles at a temperature of 2,500°C in a pure argon atmosphere. Although technegas is currently not available in the United States, Vita Medical Ltd. announced that it will be registered for approval by the Food and Drug Administration in the near future. Perfusion scintigraphy was done immediately after the ventilation scan with a mean activity of 206 ± 22 MBq 99mTc-labeled macroaggregated albumin (99mTc-MAA) administered over 5 respiratory cycles (radiation exposure, ≈3.4 mSv). All patients remained in supine position throughout the examination. A 360° SPECT acquisition of the pulmonary ventilation and perfusion was performed using a 64 × 64 matrix. For the double-head camera, a 180° rotation per head was done in 32 steps of 30 s each. For the triple-head camera, the protocol could be shortened to a rotation of 120° per head in 20 steps of 30 s each. Accordingly, the total acquisition time per SPECT turn was 16 min for the double-head camera and 10 min for the triple-head camera. Reconstruction of coronal and transversal slices was done by filtered backprojection with a third-order Butterworth filter and a cutoff frequency at 0.65. A slice thickness of 1.2 cm was chosen for hard copies on film (Drystar 4500; Agfa).
V/Q Scintigraphy: Planar Images
Planar images in 8 views were extracted from the SPECT datasets of the ventilation and perfusion scans. To that end, 3 consecutive SPECT projections were assembled for each planar image as schematically shown in Figure 1. For example, the anterior image was extracted from the SPECT acquisition by adding the 3 projections centered around the 12 o’clock position.

Extraction of planar images from SPECT datasets: planar views were assembled by adding 3 consecutive SPECT projections each, with the corresponding projections indicated.
Multislice Spiral CT
Multislice spiral CT examinations of the chest were done using a 4-detector row scanner (SOMATOM Volume Zoom; Siemens) after intravenous application of 120 mL contrast medium at a flow rate of 3 mL/s (Ultravist 370; Schering). After a standardized delay of 27 s, the contrast medium was followed by a saline chaser bolus of 30 mL injected with a flow rate of 3 mL/s using a double-power injector (CT 9000 Digital Injection System; Liebel-Flarsheim). Scan parameters were 120 kV and 100 mA, using a thin collimation of 4 × 1 mm and a table speed of 7 mm per rotation. Tube rotation time was 0.5 s. Therefore, the entire chest could be examined in approximately 20 s. Three sets of images were reconstructed with an adapted field of view in correspondence with body height and weight. For printouts, axial slices were reconstructed and displayed in 5-mm-thick sections, using soft-tissue kernels (“smooth;” Siemens B30) and lung window kernels (“sharp;” Siemens B50) with an effective slice thickness of 5 mm. However, diagnoses were based on thin axial slices (effective slice thickness STeff = 1.25 mm) that were reconstructed with an overlap of 36% (reconstruction increment RI = 0.8 mm; B30). These images were assessed on a second console of the CT scanner (Wizard workstation; Siemens).
Assessment
The images from all 3 modalities—multislice spiral CT, V/Q SPECT, and V/Q planar—were each assessed by 2 experienced referees who were unaware of the results of other examinations and clinical data. A consensus between the 2 referees was reached by discussing each case. All cases were evaluated in random order with an interval of 1 wk between each modality. A segmental lung reference chart was used to assess the scintigraphy. With the help of this chart, the localization of each defect was recorded as well as its type (match or mismatch) and extent (segmental or subsegmental). A match was defined as a pulmonary region affected by a severe reduction or complete loss of perfusion while the ventilation in this region is likewise distinctly reduced. In contrast, a mismatch was characterized as a region with regular ventilation but severely reduced or no perfusion. The scintigraphic scans were evaluated twice: first, all mismatch defects were assessed as pulmonary embolisms regardless of their extent or localization; next, the PIOPED criteria in the modified version of Worsley and Alavi were applied (31). For this second analysis, planar chest radiograms acquired within 24 h from the V/Q scintigraphy were included in the evaluation. Regarding CT angiography, pulmonary embolism was diagnosed if one or more embolic clots were detected in the pulmonary arteries. The final diagnosis was made at a consensus meeting while taking into account all imaging modalities, clinical data, D-dimer levels, the opinions of the physicians responsible for treatment, and a clinical follow-up of at least 5 mo (maximum, 10 mo).
Statistical Analysis
Statistical analysis was done using SPSS for Windows, release 11.0. Results are expressed as mean values ± SDs. Significance was tested using the nonparametric χ2 test, with P < 0.05 being considered significant. Furthermore, the degree of conformity between the image modalities was determined by calculating κ-values (range, 0–1; 0 = no conformity, 1 = total conformity).
RESULTS
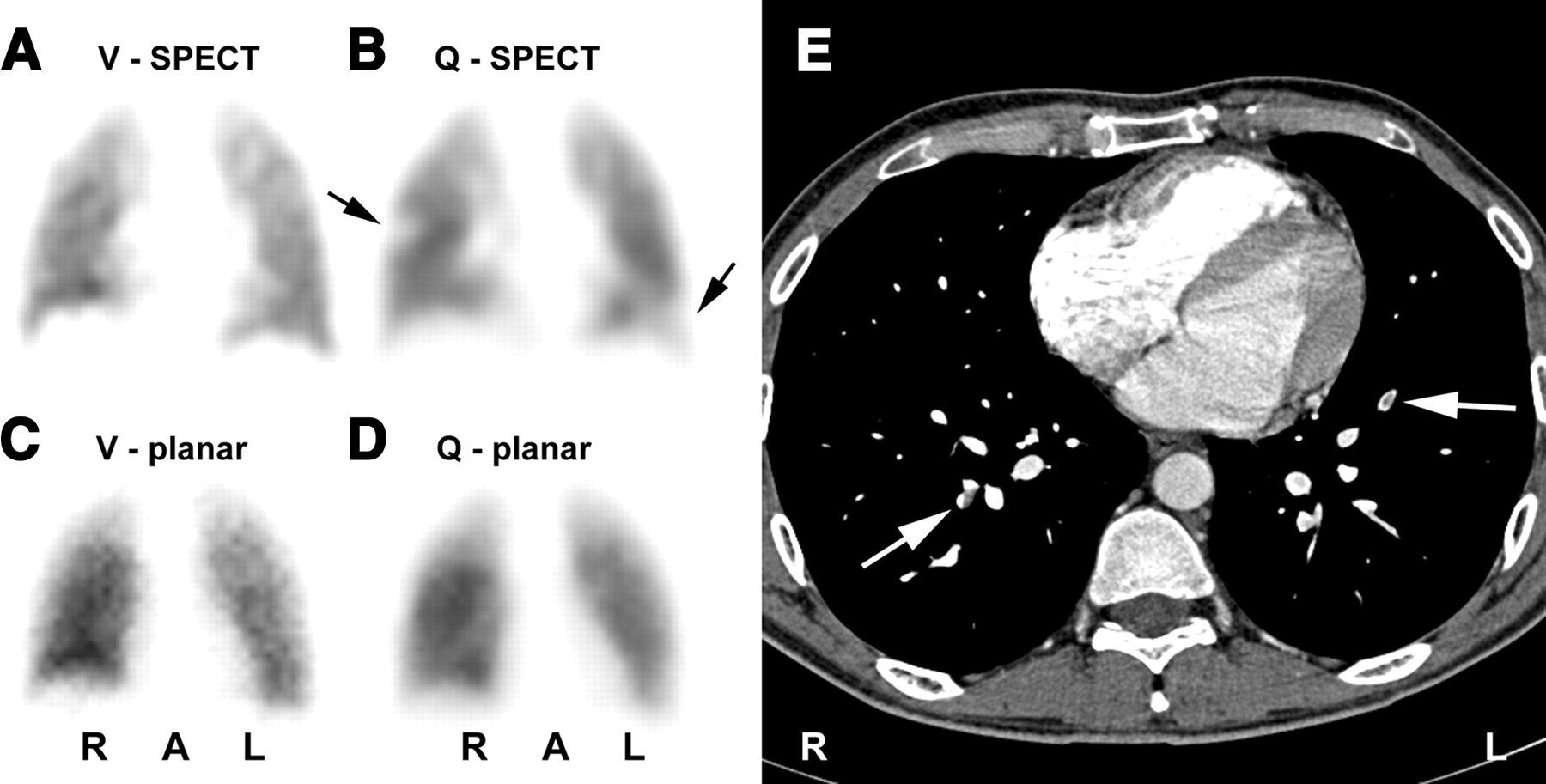
At the consensus meeting, pulmonary embolism was diagnosed in 37 of the 83 patients (44.6%). The correct diagnosis was made by multislice spiral CT in 77 of 83 patients (92.8%), by V/Q SPECT in 78 of 83 patients (94.0%), and by planar V/Q scintigraphy in 67 of 83 patients (80.7%). The results of the evaluation as well as the corresponding statistical data are given in Table 1. For purposes of analysis, all scintigraphic mismatch defects were classified as embolisms. Exemplary cases of patients with pulmonary embolism are shown in Figures 2 and 3. Whereas the segmental mismatch defect in Figure 2 is well visible on the planar and the SPECT scans, the subsegmental mismatch defects in Figures 2 and 3 could only be detected by SPECT. Figure 4 shows one of the 4 false-positive scintigraphic cases in which a mismatch defect in the right upper lobe was caused by large emphysematic bullae.

Patient with multiple embolisms in both lungs: segmental mismatch defect in left lung was detected by both SPECT (A and B) and planar scintigraphy (C and D). Defects are marked by arrows in B and D. However, subsegmental mismatch defects in right lung were only diagnosed by SPECT (B). CT angiography found thrombotic clots in branches of middle lobe artery and both lower lobe arteries (E, arrows). V = ventilation scan; Q = perfusion scan; R = right; A = anterior; L = left.
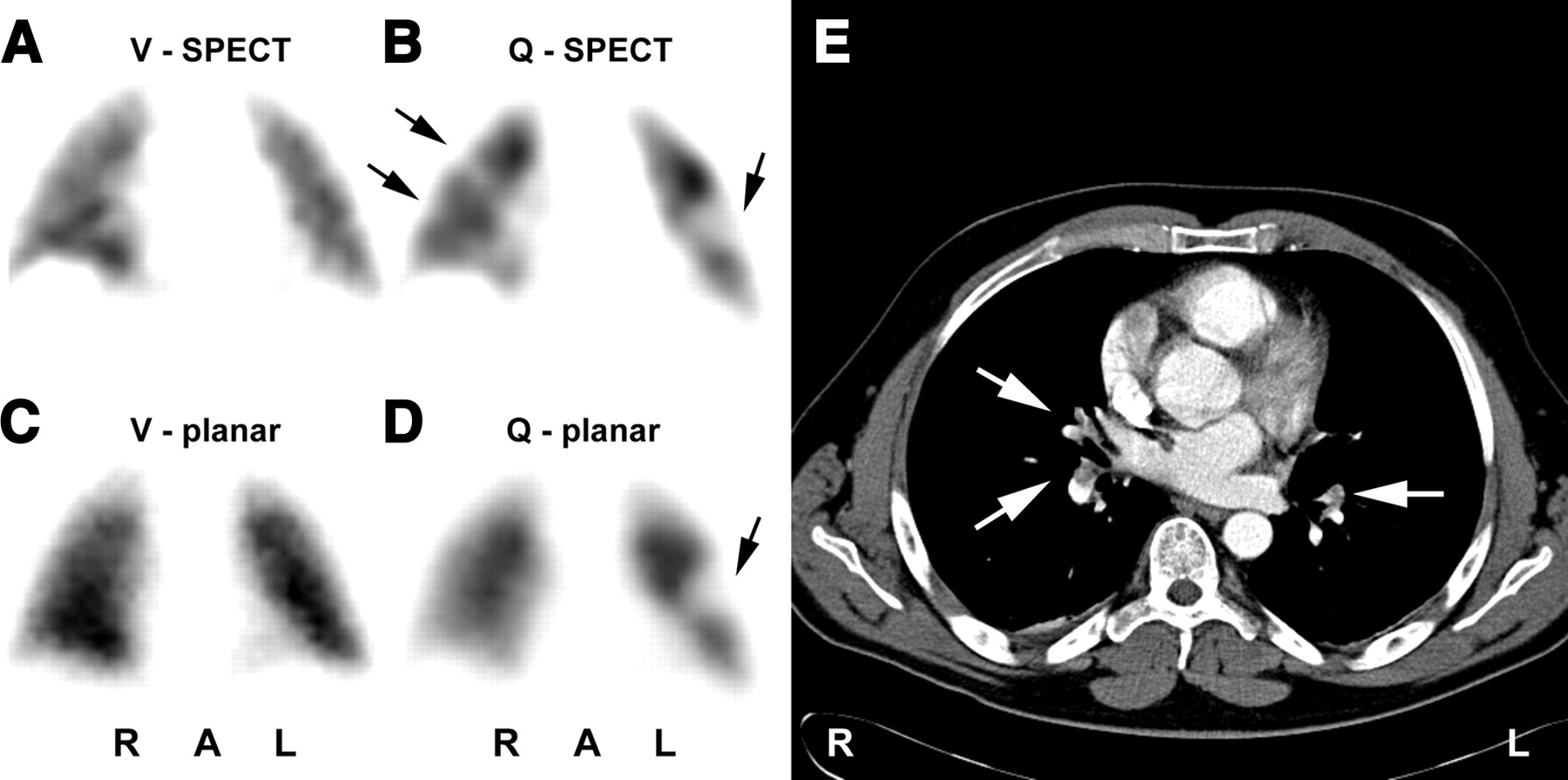
Patient with subsegmental embolisms in both lungs: mismatch defects were diagnosed by SPECT (A and B) but could not be seen on planar scans (C and D). Defects are marked by arrows in B. CT angiography found thrombotic clots in subsegmental branches of middle lobe artery (not shown) and in both lower lobe arteries (E, arrows). V = ventilation scan; Q = perfusion scan; R = right; A = anterior; L = left.

Patient with severe case of chronic obstructive pulmonary disease (COPD) and pulmonary emphysema. Large emphysematic bullae in right upper lobe (E) led to false-positive diagnosis in V/Q scintigraphy (B and D, mismatch defects marked by arrows). No pulmonary embolism was diagnosed in course of consensus meeting. CT was true-negative. Inhomogeneous distribution of ventilation agent is typical for patients with COPD (A and C). V = ventilation scan; Q = perfusion scan; R = right; A = anterior; L = left.
Diagnostic Ability of Multislice CT, V/Q SPECT, and Planar V/Q Scintigraphy to Detect Pulmonary Embolism (n = 83)
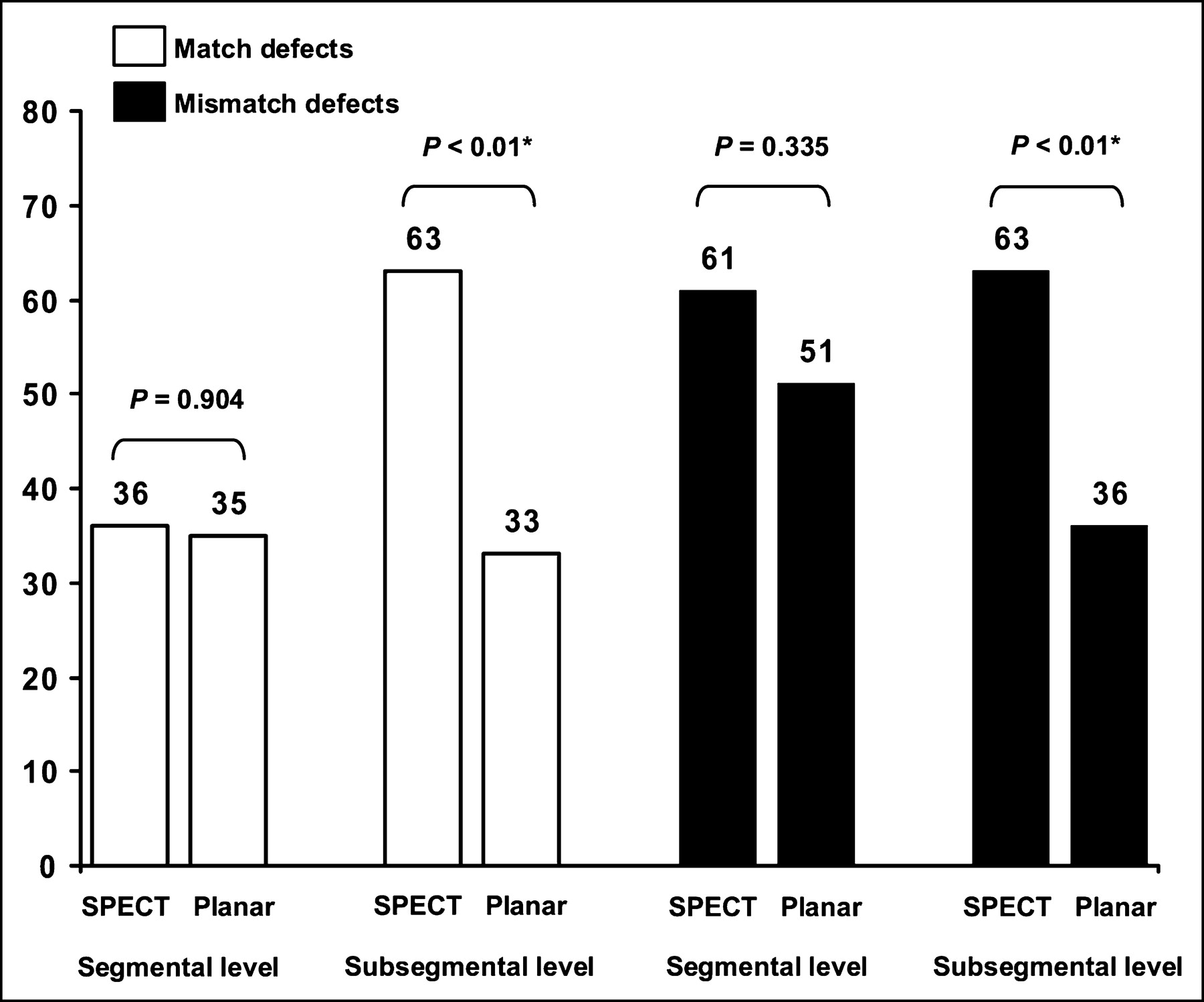
The results of a comparison between planar scintigraphy and SPECT with regard to the number of match and mismatch defects are shown in Figure 5. According to the analysis, SPECT increased the number of detectable defects on the segmental level by 12.8% (+11 defects), whereas the number of defects on the subsegmental level increased by 82.6% (+57 defects). The χ2 test showed the difference of defects detected at the subsegmental level to be highly significant (P < 0.01) compared with that at the segmental level (P = 0.401). The number of defects and their localization are given in Table 2. Unlike the middle or upper lobes, the lower lobes were more susceptible to ventilation and perfusion defects.
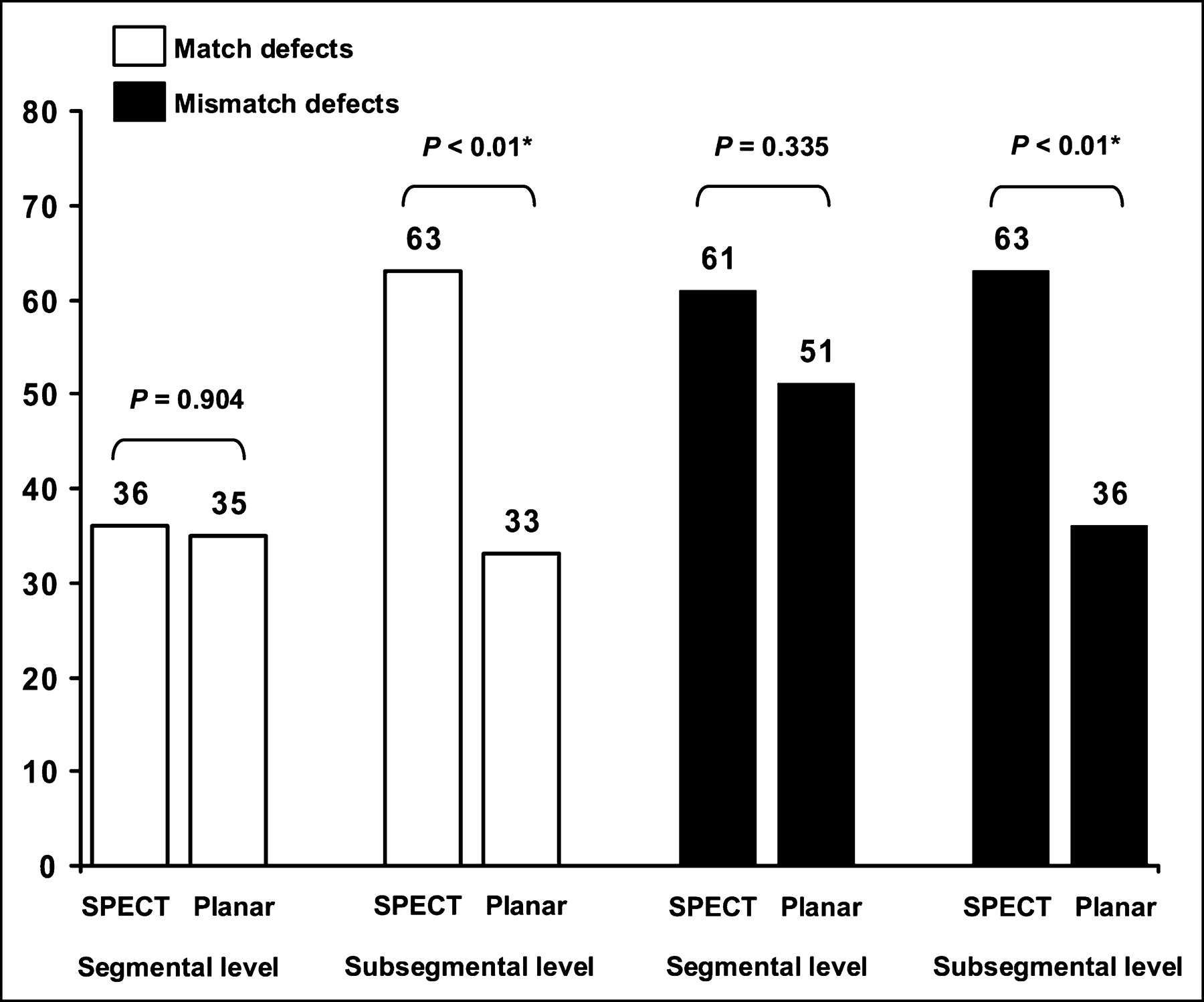
Comparison between planar V/Q scintigraphy and SPECT with regard to number of match and mismatch defects detected on segmental and subsegmental levels. Asterisks indicate significant differences (χ2 test).
Comparison Between V/Q SPECT and Planar V/Q Scintigraphy (n = 83): Number, Size, and Localization of Match and Mismatch Defects
Since the planar images in our study were not acquired conventionally but extracted from the SPECT datasets, the count statistics were analyzed to rate the image quality. The assessment showed that none of the planar ventilation images showed <100 kilocounts (kcts) and none of the planar perfusion images showed <500 kcts (mean values for anterior/posterior views: ventilation, 192 ± 73 kcts; perfusion, 803 ± 198 kcts).
The evaluation of the V/Q scintigraphy under consideration of the PIOPED criteria in the modified version of Worsley and Alavi (31) is shown in Table 3. The results are categorized by final diagnosis as made at the consensus meeting. A comparison between SPECT scans and planar images yielded a total of 24 differently categorized cases (28.9%). In 23 of those 24 cases (95.8%), SPECT led to a reclassification into a higher probability class, whereas tomographic imaging only assigned 1 patient (4.2%) to a lower class (−3 ranks). In 18 cases (75.0%), SPECT raised the probability class by 1 rank, in 1 case (4.2%) by 2 ranks, in 3 cases (12.5%) by 3 ranks, and in 1 case (4.2%) by 4 ranks.
Evaluation of V/Q Scintigraphy Under Consideration of PIOPED Criteria in Modified Version of Worsley and Alavi (31): Comparison Between SPECT and Planar Imaging (n = 83)
κ-values were calculated to evaluate the degree of conformity between the different imaging modalities (Table 4). On a scale between 0 and 1, a high κ-value indicates a high degree of conformity, whereas a low κ-value negates a close relationship.
Degree of Conformity Between Imaging Modalities and Results of Consensus Meeting Assessed by Calculating κ-Values
DISCUSSION
SPECT is a well-established imaging method that is widely used in modern nuclear medicine diagnostics. Particularly in the fields of cardiology and neurology, tomographic scans have almost completely replaced planar acquisitions. With regard to V/Q lung scintigraphy, several studies have assessed the effectiveness of SPECT in the diagnosis of pulmonary embolism (32–36) and, although the results were encouraging, only a few departments have implemented SPECT acquisitions in clinical routine so far. In view of increasing competition from CT angiography, a modernization of the conventional V/Q lung scan seems essential. The aim of our study was to assess the effectiveness of an advanced tomographic acquisition protocol for V/Q lung scintigraphy compared with planar scans and state-of-the-art CT. As a result, SPECT of pulmonary ventilation and perfusion led to a substantial improvement of the method. Especially at the subsegmental level, the number of detectable defects could be significantly increased by 82.6% compared with that of planar scintigraphy (P < 0.01). At the segmental level, the increase was still considerable (+12.8%) but statistically not significant (P = 0.401). This observation applies to match as well as mismatch defects, as shown in Table 2 and Figure 5. The superior detection rate of SPECT in comparison with planar scintigraphy is reflected by a distinctly improved sensitivity, specificity, and accuracy (Table 1). One limitation in our study is that the planar images did not correspond completely with conventional planar scans. The extraction of planar views from the SPECT datasets was necessary because an additional acquisition of conventional scans would have prolonged the examination time by 40 min each and, since pulmonary embolism is a potentially life-threatening condition, this was unacceptable. Compared with conventional planar scans, the planar images in our study include a small overlap and are acquired over 90 s instead of 240 s. The shorter acquisition time was compensated for by increasing the applied activity to 200-MBq 99mTc-MAA. Because of this increase in activity, the count statistics of the extracted planar images were comparable to those of conventional planar scans. Although it cannot be excluded that the extraction of planar images from the SPECT datasets may have negative and partly uncorrectable effects on other imaging parameters—for example, spatial resolution—the acceptable quality of our planar images is evident from the fact that the statistical parameters found in our study show good agreement with those reported by others for this method. With regard to sensitivity, specificity, and diagnostic accuracy, Blachere et al. (15) and Collart et al. (34) report values of 0.81/0.74/0.77 and 0.80/0.78/0.79, respectively, which correspond well with those of 0.76/0.85/0.81 found for our cohort. It is likely that the high specificity determined for our study group and the utilization of an ultrafine aerosol for the ventilation scans are related.
In contrast to planar lung scintigraphy, the literature contains no consistent data for sensitivity, specificity, and accuracy with regard to V/Q SPECT. Whereas Collart et al. (34) found no increase in sensitivity using tomographic imaging, Bajc et al. (33) and Corbus et al. (35) reported significant improvements up to a value of 1.0. However, with regard to specificity, all 3 groups found a substantial increase up to values between 0.87 and 0.96 for SPECT compared with planar scintigraphy (33–35). The results of our study confirm these observations.
An analysis of the data acquired by CT angiography shows that multidetector row scanners have virtually overcome the limitations of single-detector scanners for subsegmental embolisms. Although 4 of the 5 false-negative results still related to patients with pulmonary embolism at a subsegmental level, the overall accuracy was equivalent to that of V/Q SPECT. This high degree of conformity between CT and SPECT is reflected by a κ-value of 0.733 (Table 4). A direct comparison between the 2 methods shows that lung scintigraphy in SPECT technique has an excellent sensitivity with a somewhat lower but still very good specificity, whereas the exact opposite is true for CT. With regard to false diagnoses, CT shows a certain predisposition for false-negative results, whereas the scintigraphy with SPECT tends to produce false-positive results. Planar V/Q scans, on the other hand, led to a considerable number of false-positive and false-negative findings. Accordingly, the accuracy of planar lung scintigraphy was distinctly lower compared with that of the tomographic modalities.
Remarkably, SPECT does not increase the acquisition time for lung scans. Conventional planar V/Q scintigraphy with 8 views each and a scan time of 4 min per view takes 32 min, provided that a double-head camera is used. On the same camera system, SPECT takes exactly the same time. With a triple-head camera, the acquisition time can be reduced by 37.5% to 20 min for a complete V/Q scan.
Another focus of the study was an evaluation of whether the PIOPED criteria can be applied to tomographic V/Q scans without modifications or if there is a need for reassessment. A corresponding analysis yielded heterogeneous results. According to our data, SPECT led to a substantial improvement in discriminatory power for the probability classes “normal” and “very low probability,” as shown in Table 3. By definition, the risk for embolism should not exceed 10% for patients assigned to these classes. In our study, pulmonary embolism was confirmed in only 1 of the 30 patients (3.3%) assigned to these categories by SPECT, whereas an evaluation of the planar scans yielded a distinctly higher ratio, with 9 of 38 subjects (23.7%). In contrast to these findings, the discriminatory power of the categories “intermediate probability” and “high probability” was not improved by tomographic imaging. Comparable results were found for both modalities. Surprisingly, SPECT showed inferior results compared with planar scintigraphy with regard to the “low probability” class. Although pulmonary embolism should be present in <20% of all patients assigned to this category, embolism was confirmed in 7 of 11 patients (63.6%) allocated to this class by SPECT. In comparison, planar scintigraphy yielded a ratio of 3 of 7 patients (42.9%), which is slightly better than SPECT but, nonetheless, too high.
A closer look at the results of our study reveals severe shortcomings for the diagnostic system based on the PIOPED criteria, independent of the type of imaging technique used. Particularly the unsatisfactory intermediate probability class must be regarded as one of its major drawbacks. By definition, in patients assigned to this category, there is 20%–80% probability of pulmonary embolism. Such an inconclusive diagnosis definitely helps neither therapy nor the referring physician. The questionable value of intermediate probability findings is underlined by the fact that during the course of our study about half of the patients assigned to this class showed embolism whereas the other half did not. Given that these “intermediates” are relatively common—more than 25% of the patients in our cohort were assigned to this class—the situation appears even worse. In this context, SPECT only had a minor positive effect on the frequency of intermediate findings: their ratio was reduced from 28.9% (24/83) diagnosed by planar scintigraphy to 26.5% (22/83) assigned to this class by SPECT. Accordingly, additional examinations would have been required in more than a quarter of the patients referred to V/Q scintigraphy to exclude or confirm pulmonary embolism. In times of dwindling funds, such an outcome is not good enough. Compared with the probability classes of the PIOPED system, the clear-cut diagnoses given by CT angiography are far more attractive. Specific therapy can be applied immediately without further loss of time and money by supplementary examinations, whereas at the same time a certain degree of legal protection is afforded in cases in which malpractice is assumed.
In addition to the ambiguous intermediate probability class, several other arguments challenge the utilization of the PIOPED criteria in their present form. First, it must be considered that the PIOPED data were acquired between January 1985 and fall 1986 (6,7,24). The diagnostic methods used in the course of that study are now largely obsolete and can no longer be accepted as standards. Furthermore, the PIOPED study gives no physiologic explanation of why large mismatch defects should be a sign for pulmonary embolism while small ones are not. The growing dissatisfaction in the scientific community with the PIOPED criteria is reflected by the great number of modifications found in many studies (13,22,24,31,32,35,37).
Considering the shortcomings of the PIOPED study and the increasing competition between V/Q scintigraphy and CT angiography, a reformation of the V/Q scan interpretation criteria definitely seems in order. Especially the categorization into different probability classes appears to be detrimental compared with the clear-cut diagnoses made by CT. According to our data, highly accurate results with an excellent sensitivity and specificity can be achieved by the alternative diagnostic approach that assesses all mismatch defects as embolisms. Further methodic improvement may be achieved by the simultaneous interpretation of chest radiographs, preferably acquired within 24 h before or after scintigraphy. In the light of such additional morphologic information, the emphysematic bullae of the patient in Figure 4 would have been easily identified and the false-positive diagnosis averted.
SPECT and ultrafine aerosols aside, several other techniques could significantly refine V/Q lung scintigraphy. Iterative image reconstruction (33) and the use of artificial neural networks (38) are only some of the techniques that show considerable potential. Taking into account recent developments in the field of CT angiography—such as 16-slice scanners, electron-beam CT (39), or perfusion-weighted color maps (40)—the continuous methodic improvement of V/Q lung scintigraphy and its consequent implementation into clinical routine are mandatory. Planar imaging can no longer be considered state-of-the-art.
CONCLUSION
Using advanced imaging techniques, both tomographic modalities—V/Q lung scintigraphy and multislice spiral CT—are highly accurate and, in all aspects, comparable in detecting pulmonary embolism. According to our data, CT has the greater specificity while V/Q SPECT shows a superior sensitivity. With regard to CT angiography, our results suggest that the multidetector row technique has virtually overcome the limitations of single-detector row scanners for detecting subsegmental embolism. With regard to V/Q scintigraphy, SPECT and the utilization of ultrafine aerosols have proven their potential as powerful technical advances with the capability to substantially improve the method. Even though planar lung scintigraphy showed satisfactory results for a nontomographic modality, it does not compare with V/Q SPECT scans or multislice spiral CT, with tomographic imaging being superior, particularly at the subsegmental level. Analogous to developments in the fields of neurology and cardiology, it can be expected that SPECT will replace planar lung scintigraphy in the near future. Considering the limitations of the PIOPED study and the increasing competition from CT angiography, continued use of the PIOPED criteria in their present form seems questionable. According to our data, excellent results with high sensitivity, specificity, and accuracy can be achieved using the alternative diagnostic approach that assesses all mismatch defects as embolisms.
Acknowledgments
Thanks are due to Alejandro Rodón and Birgit Reinartz for general and language editing.
Footnotes
Received Oct. 23, 2003; revision accepted Mar. 12, 2004.
For correspondence or reprints contact: Patrick Reinartz, MD, Department of Nuclear Medicine, University Hospital Aache, Pauwelsstrasse 30, 52074 Aachen, Germany.
E-mail: preinartz{at}compuserve.com
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Observational cohort study to validate SEARCH, a novel hierarchical algorithm to define long-term outcomes after pulmonary embolism
- V/Q SPECT and SPECT/CT in Pulmonary Embolism
- Imaging of pulmonary hypertension in adults: a position paper from the Fleischner Society
- A Prospective, Comparative Study of Ventilation-Perfusion Planar Imaging and Ventilation-Perfusion SPECT for Chronic Thromboembolic Pulmonary Hypertension
- The optimal imaging test for diagnosis of acute pulmonary embolism: a second chance for lung scintigraphy?
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)
- Deep vein thrombosis and pulmonary embolism in the military patient
- Ventilation-Perfusion Lung Scanning: Stuck in a Rut?
- V/Q Scanning Using SPECT and SPECT/CT
- V/Q SPECT: the primary imaging test for suspected pulmonary embolism
- Potential of hybrid V/P SPECT-low-dose CT in lung diagnostics
- Assessment of correlation between CT angiographic clot load score, pulmonary perfusion defect score and global right ventricular function with dual-source CT for acute pulmonary embolism
- Successful and Safe Implementation of a Trinary Interpretation and Reporting Strategy for V/Q Lung Scintigraphy
- High Frequency of Silent Pulmonary Embolism in Patients With Cryptogenic Stroke and Patent Foramen Ovale
- Imaging in Acute Pulmonary Embolism With Special Clinical Scenarios
- Detection of Pulmonary Embolism: Comparison of Methods
- Ventilation-Perfusion SPECT with 99mTc-DTPA Versus Technegas: A Head-to-Head Study in Obstructive and Nonobstructive Disease
- Reply: Detection of Pulmonary Embolism: Comparison of Methods
- SPECT in Acute Pulmonary Embolism
- Detection of Pulmonary Embolism with Combined Ventilation-Perfusion SPECT and Low-Dose CT: Head-to-Head Comparison with Multidetector CT Angiography
- To PIOPED, or Not to PIOPED
- Merits of V/Q SPECT Scintigraphy Compared with CTPA in Imaging of Pulmonary Embolism
- Bayes pulmonary embolism assisted diagnosis: a new expert system for clinical use
- SPECT Imaging in the Diagnosis of Pulmonary Embolism: Automated Detection of Match and Mismatch Defects by Means of Image-Processing Techniques
- Tomographic Imaging in the Diagnosis of Pulmonary Embolism: Still, We Do Not Know