


Abstract
The high renal uptake of radiolabeled somatostatin analogs is dose limiting. Lowering this uptake permits higher radioactivity doses and, thus, tumor doses to be administered. We tested the effects of the microtubule drug colchicine on renal uptake of [111In-DTPA0]octreotide. Also, the effects of fructose were tested. Methods: Organ radioactivity 24 h after injection of [111In-DTPA0]octreotide was determined in rats. Results: Coinjection of 1 mg of colchicine per kilogram did not influence renal uptake of [111In-DTPA0]octreotide, whereas this dose administered 5 h before [111In-DTPA0]octreotide resulted in significant renal uptake reduction (63%). d-Lysine plus colchicine reduced the uptake by 76% (P < 0.01 vs. d-lysine alone). Liver and blood radioactivity levels were significantly elevated by colchicine. Fructose did not affect the biodistribution of [111In-DTPA0]octreotide. Conclusion: Renal uptake of [111In-DTPA0]octreotide is dependent on microtubule function in rats. The addition of colchicine to amino acid protocols may permit administration of higher doses, improving the therapeutic window of peptide receptor radionuclide therapy.
Radiolabeled somatostatin analogs have proven helpful in the diagnostic work-up for neuroendocrine tumors (1). In addition, coupling Auger electron or β-particle–emitting radionuclides to these octreotide derivatives made internal irradiation of these neuroendocrine tumors possible, and several peptide receptor radionuclide therapy (PRRT) studies have been conducted using [111In-DTPA0]octreotide (2), [90Y-DOTA0]octreotide (3), and [177Lu-DOTA0]octreotate (4).
The radioactivity dose to be administered in PRRT is limited by normal-organ toxicity, of which the kidneys are the principal dose-limiting organs. In the kidney, radiolabeled octreotide is efficiently reabsorbed by proximal tubule cells, causing high kidney radiation doses. Lowering kidney uptake of radioactivity may permit larger doses to be administered to tumors.
Hammond et al. (5) showed in a semiquantitative method that a mixture of amino acids inhibited kidney uptake of radiolabeled octreotide. Further studies on animals and patients have shown that this inhibition of renal uptake of [111In-DTPA0]octreotide is caused mainly by the positively charged amino acids lysine and arginine (6,7). The effects of these positively charged amino acids are explained by competition for negatively charged binding sites at the proximal tubule cell surface.
We previously found indications that reabsorption of [111In-DTPA0]octreotide requires energy. Injection of a 400 mg/kg dose of maleate, which inhibits the citric acid cycle, inhibited kidney uptake of [111In-DTPA0]octreotide by about 74% in rats (6).
However, the exact mechanism by which radiolabeled octreotide derivatives are taken up in the kidney is not fully understood. In general, peptide and protein reabsorption in the proximal tubule occur mostly via endocytosis of cell membrane after binding of the ligand. The complex is then transported to the lysosomal apparatus for proteolysis. Then, the scavenger receptor proteins are recycled to the cell surface and are again made available for endocytosis (8,9).
We investigated, using fructose administration, whether kidney uptake of radiolabeled octreotide is adenosine triphosphate (ATP) dependent. Fructose can be administered to humans and is known to significantly lower cellular ATP in proximal tubule cells (10). Also, we tested if microtubule-dependent endocytosis plays a role in kidney uptake of radiolabeled octreotide in rats, using colchicine administration. Colchicine prevents the return of the cell membrane parts to the cell surface by disruption of cellular microtubules (11–13). The subsequent result is lowered peptide and protein reabsorption in the proximal tubule. The results presented here suggest microtubule-dependent uptake of [111In-DTPA0]octreotide in the proximal tubule of the rat kidney.
MATERIALS AND METHODS
Radiolabeling
Commercially available kits of [DTPA0]octreotide and 111InCl3 were obtained from Tyco Health Care. The radiolabeling procedure was in accordance with standard procedures (14).
Tissue Distribution of [111In-DTPA0]Octreotide
Animal experiments were performed in compliance with the regulations of the institution and with generally accepted guidelines governing such work.
Male Wistar rats weighing 250–300 g were used. The rats received an intravenous injection of [111In-DTPA0]octreotide (3 MBq; 0.5 μg of octreotide) into the dorsal vein of the penis. Twenty-four hours later, organs were isolated. Radioactivity was measured in isolated organs and in a blood sample taken at 24 h after injection. The experimental groups are described in Table 1.
Description of Experimental Groups
The results represent 4 experiments with a total of 3–9 rats per experimental group. Data are expressed as mean ± SEM. Statistical evaluation was performed using 1-way ANOVA. A P value less than 0.05 was considered statistically significant.
RESULTS
The tissue distribution of [111In-DTPA0]octreotide 24 h after injection in control rats is shown in Table 2.
Tissue Distribution of [111In-DTPA0]Octreotide in Control Rats 24 Hours After Injection
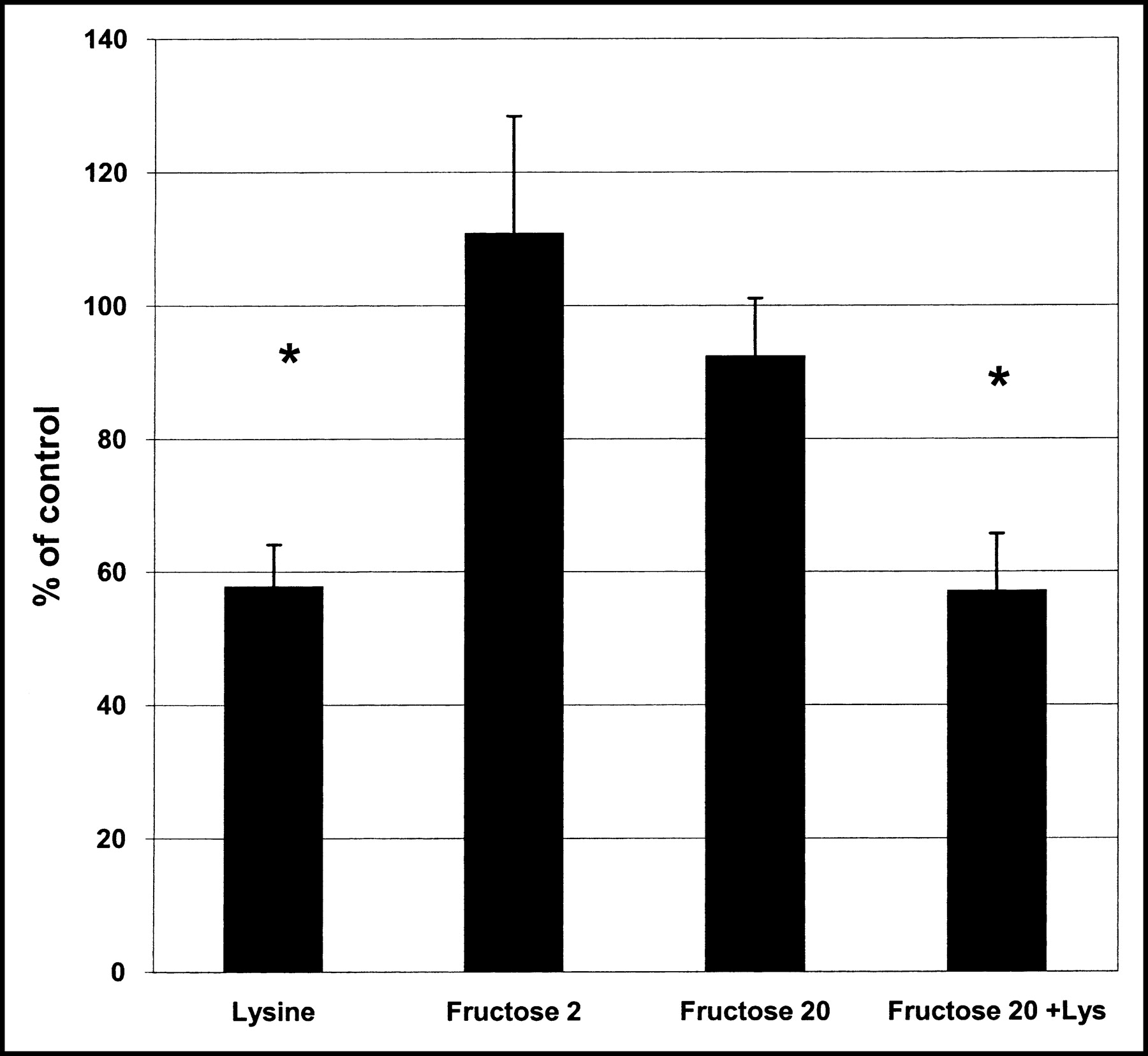
Figure 1 shows the kidney radioactivity 24 h after injection of [111In-DTPA0]octreotide and the effects of d-lysine (400 mg/kg), fructose (2 mmol/kg and 20 mmol/kg), and the combination of d-lysine with fructose on renal uptake of the radioligand. Administration of d-lysine clearly inhibited kidney radioactivity by about 40%. However, administration of both 2 and 20 mmol of fructose per kilogram had no effect. The inhibition of renal radioactivity by the combination of d-lysine and fructose was comparable to that by d-lysine alone. Fructose administration did not influence radioactivity in other organs tested.
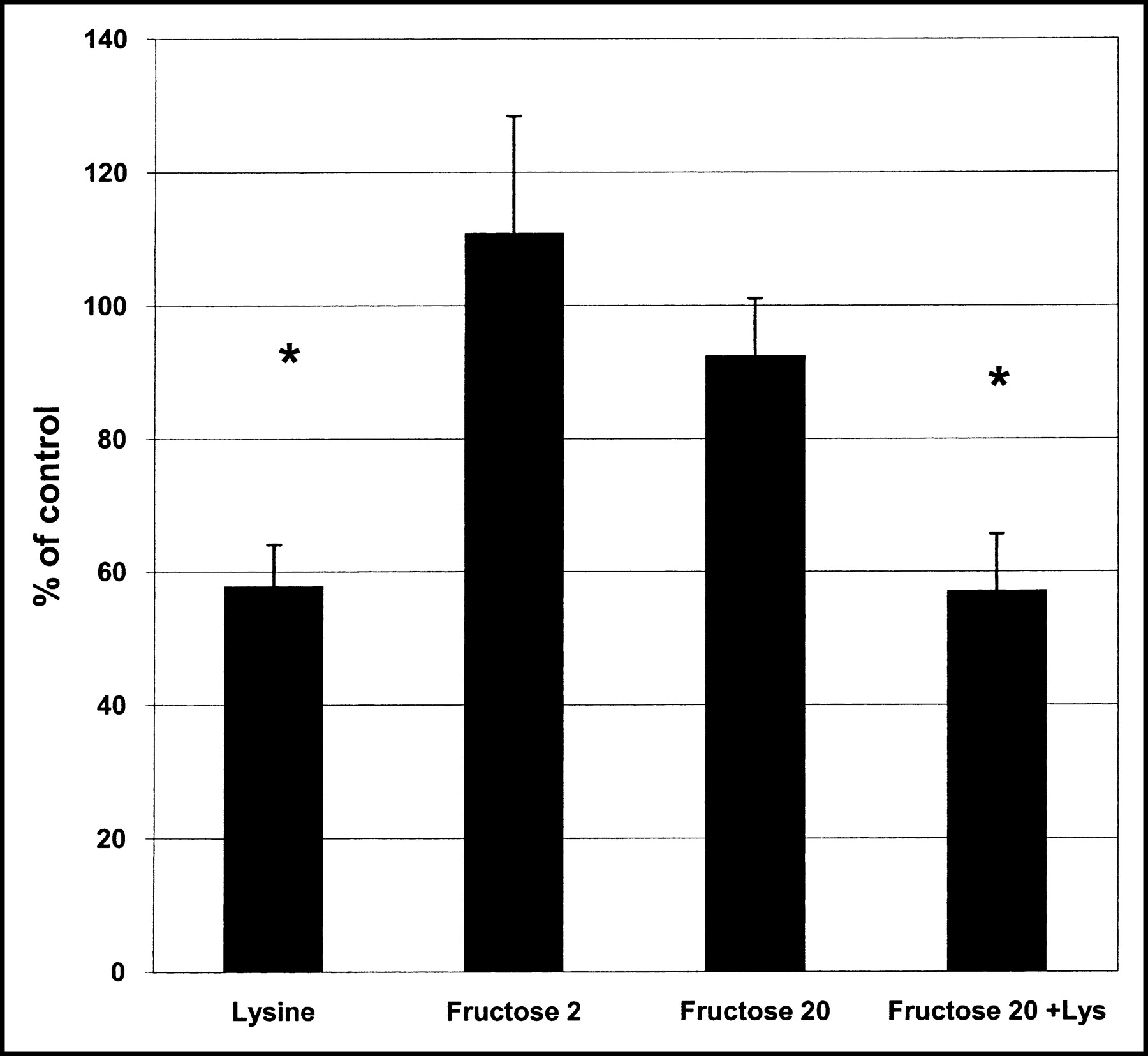
Effects of d-lysine (400 mg/kg), fructose (2 and 20 mmol/kg) and the combination of 400 mg of d-lysine per kilogram plus 20 mmol of fructose per kilogram on kidney radioactivity 24 h after injection of [111In-DTPA0]octreotide. Groups consist of 3 rats. *P < 0.01 versus control.
Figure 2 shows the effects of colchicine treatment onkidney uptake of [111In-DTPA0]octreotide. Coinjection of 1 mg of colchicine per kilogram with the radioligand did not inhibit kidney radioactivity. However, injecting 0.5, 1, or 2 mg of colchicine per kilogram 5 h before injection of [111In-DTPA0]octreotide significantly reduced kidney uptake (respective inhibitions of 28% ± 13%, P < 0.01 vs. control; 63% ± 6%, P < 0.001 vs. control; and 56% ± 6%, P < 0.001 vs. control).
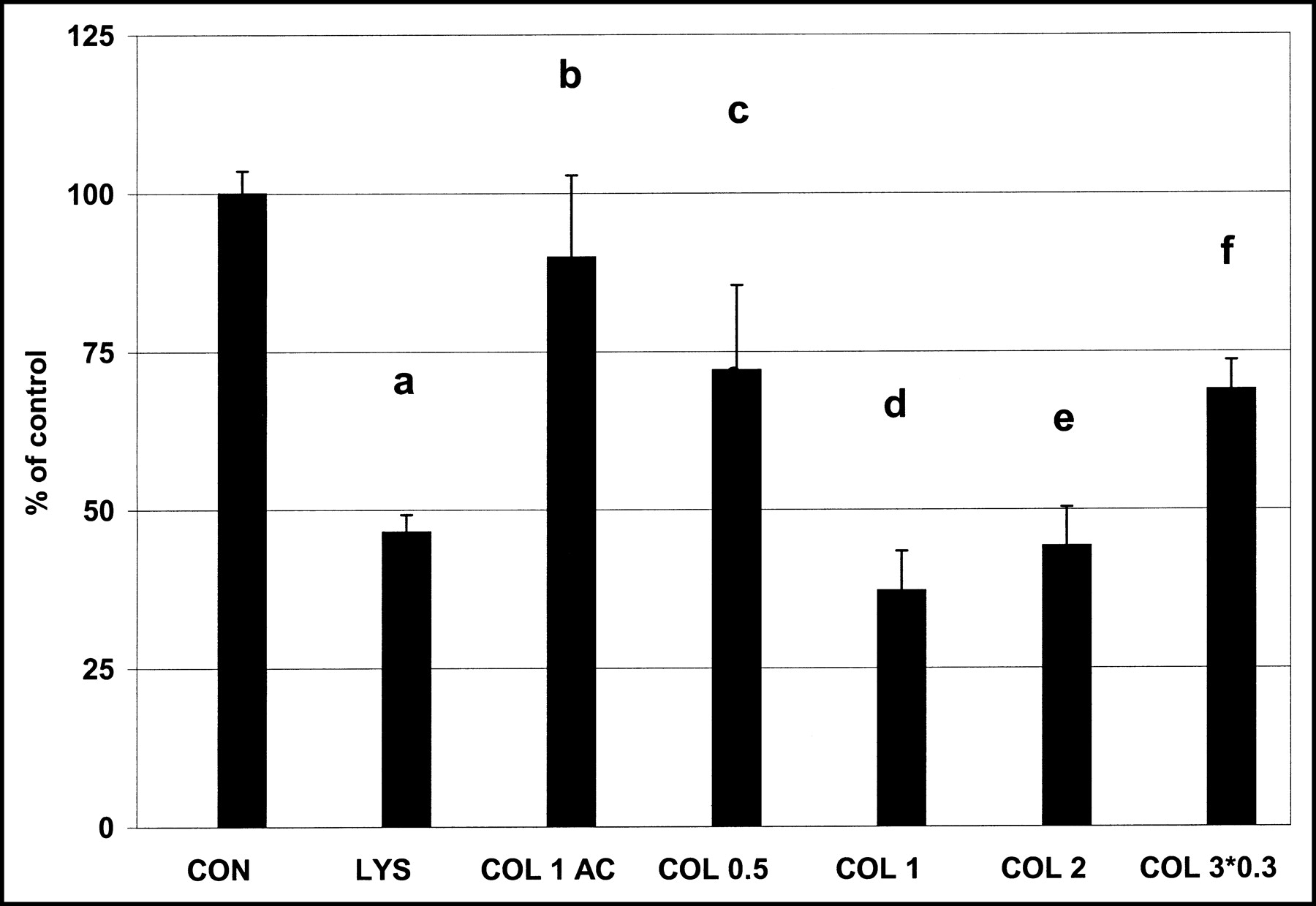
Effects of different treatment modalities with colchicine on kidney radioactivity 24 h after injection of [111In-DTPA0]octreotide. Groups consist of 6–9 rats. Table 1 describes the experimental groups and gives their abbreviations. Probability values are as follows: (a) P < 0.001 vs. control; (b) P = not statistically significant (NS) vs. control; (c) P < 0.01 vs. control, and P < 0.001 vs. 1 mg of colchicine per kilogram; (d) P < 0.001 vs. control, and P = NS vs. 400 mg of d-lysine per kilogram; (e) P < 0.001 versus control, and P = NS vs. 1 mg of colchicine per kilogram; (f) P < 0.001 vs. control, and P < 0.001 vs. 1 mg of colchicine per kilogram.
A dose–response relationship was found: The inhibition caused by 1 mg/kg was significantly better than that caused by 0.5 mg of colchicine per kilogram. However, treatment with 2 mg of colchicine per kilogram did not augment the inhibition caused by 1 mg/kg. Repeated administration of colchicine (0.3 mg/kg at 5, 29, and 53 h before radioligand injection) inhibited kidney radioactivity by about 31%, but this degree of inhibition was significantly lower than caused by the comparable dose of 1 mg/kg 5 h before radioligand injection (63%, P < 0.001).
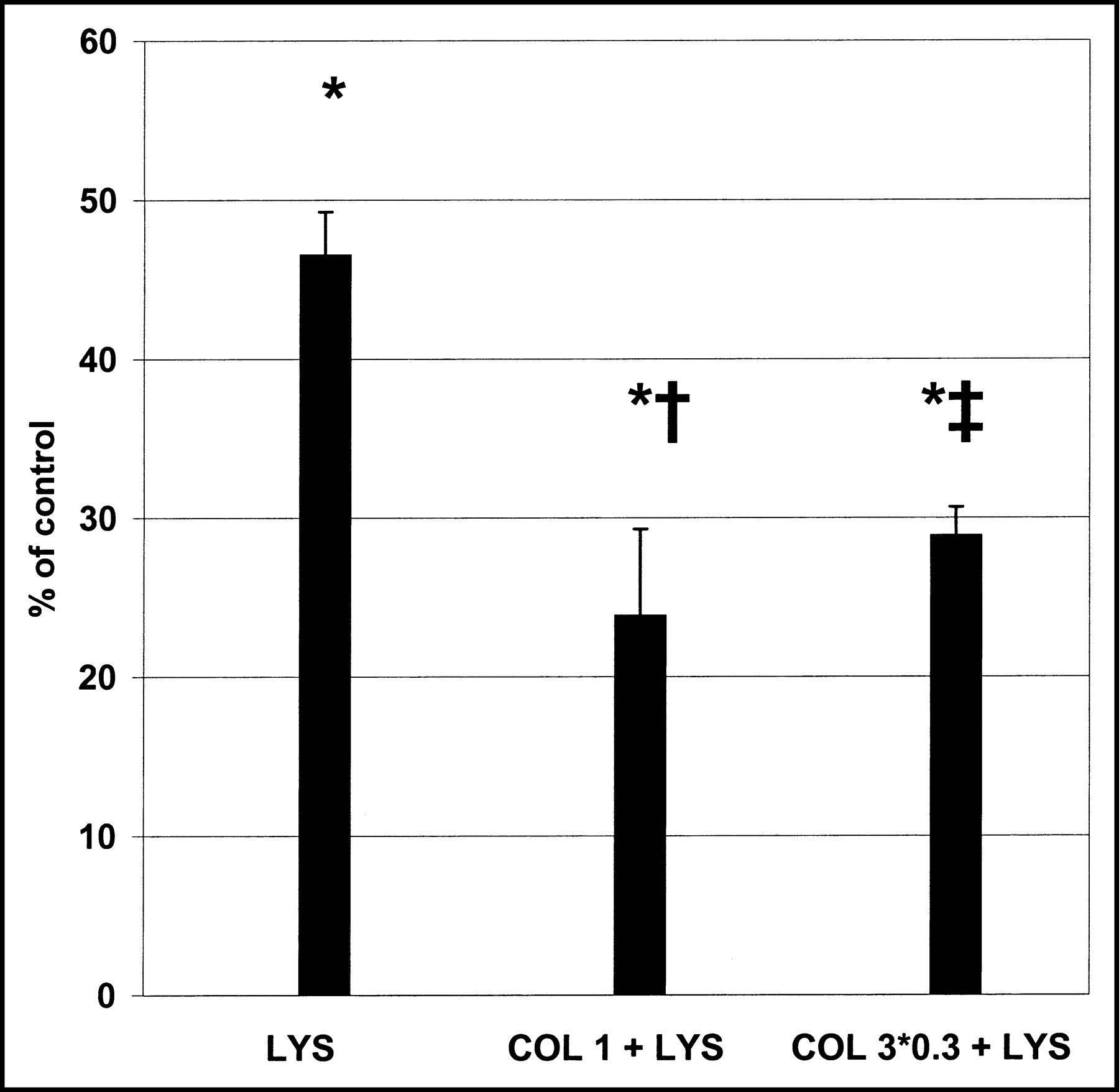
In Figure 3, the treatment combinations of colchicine and lysine versus lysine alone are compared with regard to their potential to inhibit kidney uptake of [111In-DTPA0]octreotide. Kidney-uptake reduction was more pronounced with 1 mg of colchicine per kilogram plus 400 mg of d-lysine per kilogram than with 400 mg of d-lysine alone per kilogram (76% ± 5% vs. 54% ± 3%, P < 0.01). There was a clear trend, although not statistically significant, for better inhibition of kidney radioactivity by the combination of 1 mg of colchicine per kilogram and 400 mg of d-lysine per kilogram than by colchicine alone (inhibitions of 76% ± 5% vs. 63% ± 6%, P = NS). Administration of 3 doses of 0.3 mg of colchicine per kilogram at 24-h intervals plus d-lysine treatment was not better than administration of d-lysine alone.

Effects of d-lysine (400 mg/kg) and 2 combinations of colchicine with d-lysine on kidney radioactivity 24 h after injection of [111In-DTPA0]octreotide. Groups consist of 6–9 rats. Table 1 describes the experimental groups and gives their abbreviations. *P < 0.001 vs. control; †P < 0.01 vs. 400 mg of d-lysine per kilogram; ‡P = NS vs. 400 mg of lysine per kilogram.
Table 3 shows the effects of the different colchicine doses on radioactivity in different organs. Except for the repeated-dose group, all colchicine treatment modalities elevated the radioactivity level in blood and liver. Radioactivity in the spleen was higher only in the rats treated with 2 mg of colchicine per kilogram. The tissue content of [111In-DTPA0]octreotide in stomach, muscle, pancreas, and adrenals, of which the last 2 are somatostatin receptor–positive organs, was not changed by colchicine treatment.
Effects of Colchicine Administration on Tissue Radioactivity After Injection of [111In-DTPA0]Octreotide
DISCUSSION
Radiolabeled somatostatin analogues are efficiently excreted by the kidneys, but a significant amount is reabsorbed by proximal tubule cells (15). This kidney uptake is the major dose-limiting factor in PRRT using these peptides (16), and lowering it will allow larger doses to be administered, thereby enlarging the therapeutic window of PRRT. However, the maximal safe radiation dose to the kidney is not known. At present, a maximal radiation dose of 23–27 Gy to the kidney is accepted in humans (16).
The positively charged amino acids lysine and arginine have been shown effective and safe in reducing kidney radiation dose during PRRT with radiolabeled octreotide (7). The presumed mechanism of action is competition between the radiopharmaceutical and the amino acids for negatively charged membrane molecules.
This study was performed to gain better insight into the uptake process in order to find new kidney protection methods to add to or substitute for the currently used amino acid solutions.
In general, low-molecular-weight proteins and peptides are easily filtered and subsequently reabsorbed in the proximal tubule. This reabsorption process is mediated mainly by endocytosis (8): After binding to a carrier molecule, an endosome is formed and transported through the cytoplasm to the lysosomal apparatus for hydrolysis. Then, the carrier molecule is transported back to the cell surface (9).
Several reports have suggested that proper functioning of endocytosis is dependent on ATP via the endosomal acidification machinery (17,18). We previously showed that reuptake of [111In-DTPA0]octreotide in the rat kidney was inhibited by maleate (6), which is used to mimic Fanconi’s syndrome in rats. Maleate causes a generalized tubule transport dysfunction, possibly by inhibiting the citric cell cycle (19), pointing to a possible ATP dependency of kidney uptake of radiolabeled somatostatin analogues. Maleate cannot be used in humans, whereas fructose can. In the present study we tested if the ATP-lowering substance fructose would inhibit kidney uptake of [111In-DTPA0]octreotide. Burch et al. (10) showed that administration of 20 mmol of fructose per kilogram resulted in a 41% decline of ATP in rat proximal tubule cells within 40 min. However, our results showed that fructose did not affect kidney uptake of [111In-DTPA0]octreotide. It cannot be excluded that higher doses, repeated doses, or an earlier dose of fructose may reduce kidney radioactivity.
Several reports have shown that the endocytosis process in the proximal tubule is also dependent on microtubule action (11,13). Colchicine is a drug that prevents polymerization of microtubules in the cytoplasm and the nucleus. Its efficacy has been proved in patients with gout, Behçet’s syndrome, familial Mediterranean fever, and cirrhosis (20). Treatment with colchicine results in scattering of multiple vesicles throughout the proximal tubule cell containing specific uptake molecules (11,13). Normally, these vesicles would fuse to form dense apical tubules that later would insert into the apical membrane again (9). However, transportation of these vesicles into dense apical tubules is inhibited because of microtubule disruption. In turn, this causes a defect in proximal tubule reabsorption of low-molecular-weight proteins and peptides (11,13).
Our data on colchicine treatment show that colchicine efficiently blocked tubule uptake of [111In-DTPA0]octreotide. A dose–response relationship was found, with a maximal effect at a dose of 1 mg/kg. The effects of 1 mg of colchicine per kilogram on kidney [111In-DTPA0]octreotide depend on the interval between colchicine administration and injection of [111In-DTPA0]octreotide. For instance, injection of colchicine 5 h before the radioligand inhibited kidney uptake by about 60%, whereas no effects were seen when colchicine was coinjected with the radioligand. This finding is in accordance with a previous study of Gutmann et al. (12), which found that the effects of colchicine on transport proteins did not appear before 4–8 h after colchicine treatment, depending on the dose used. The investigators suggested that this interval, rather than representing transcriptional factors, may represent the effects of colchicine on recycling membrane parts, as is supported by the fact that the effects of colchicine were reversed after 24 h (12). We found indications for reversibility of the effects of colchicine as well. Rats treated with 3 doses of 0.3 mg/kg at 24-h intervals had higher kidney [111In-DTPA0]octreotide content than did rats treated with 1 mg/kg injected 5 h before the radioligand was injected. Thus, tubule cells may have recovered (partially) before the next dose was administered.
Colchicine strongly elevated radioactivity uptake in both blood and liver in almost all treatment groups. The elevated blood levels may indicate a higher uptake of radioactivity by bone marrow and may constitute a dose-limiting factor in PRRT. However, whether colchicine will similarly affect blood radioactivity levels in humans is unclear, especially when the lower colchicine doses that are used in humans are considered. The higher radioactivity distributed to the liver may reflect cellular damage by metabolism of colchicine in the liver. Despite higher circulating radioactivity levels, radioactivity accumulation in other organs was not elevated.
We did not show any effect of colchicine on uptake in the somatostatin receptor–positive organs pancreas and adrenal, but it might be interesting to test the effects of colchicine on tumor radioactivity uptake in rats bearing tumors positive for somatostatin receptor type 2.
From our study, we conclude that 1 mg of colchicine per kilogram adds significantly to the renal-protecting effects of 400 mg of d-lysine per kilogram—a finding that is promising for clinical use. However, the colchicine doses used in our experimental study on rats are much higher than those applied clinically. Within the time frame of the study, we saw no toxic side effects on the rats treated with colchicine. It remains difficult, however, to extrapolate drug dosage schedules and toxicity data from one species to another, because of large differences in metabolic turnover of drugs and different susceptibilities for toxic effects of drugs.
In humans, colchicine is usually administered orally at an initial dose of 1 mg, followed by 0.5 mg every 2 h until gastrointestinal side effects occur or until a total dose of 6 mg has been given within several days. This procedure is usually safe, unless the patient has renal or liver disease or is elderly (21). It might be of interest to find out if this clinically applicable dosage of colchicine can further enhance kidney protection during PRRT with radiolabeled octreotide.
CONCLUSION
Injection of fructose, known to lower proximal-tubule ATP content, did not reduce kidney radioactivity after injection of [111In-DTPA0]octreotide in rats. The microtubule-disrupting drug colchicine significantly inhibited kidney uptake of [111In-DTPA0]octreotide. The combination of lysine and colchicine significantly enhanced the reduction of renal uptake.
Footnotes
Received Apr. 2, 2003; revision accepted Dec. 5, 2003.
For correspondence or reprints contact: Edgar J. Rolleman, MD, Department of Nuclear Medicine, Erasmus MC Rotterdam, Room V-220, Dr. Molewaterplein 50, 3015 GD Rotterdam, The Netherlands.
E-mail: e.rolleman{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Development of Improved Tumor-Residualizing, GRPR-Targeted Agents: Preclinical Comparison of an Endolysosomal Trapping Approach in Agonistic and Antagonistic Constructs
- Diabody Pretargeting with Click Chemistry In Vivo
- Renal Toxicity of Radiolabeled Peptides and Antibody Fragments: Mechanisms, Impact on Radionuclide Therapy, and Strategies for Prevention
- Synthetic Affibody Molecules: A Novel Class of Affinity Ligands for Molecular Imaging of HER2-Expressing Malignant Tumors
- Pretargeted Radioimmunotherapy with a Single-Chain Antibody/Streptavidin Construct and Radiolabeled DOTA-Biotin: Strategies for Reduction of the Renal Dose
- Use of Polyglutamic Acids to Reduce Uptake of Radiometal-Labeled Minigastrin in the Kidneys
- Long-Term Follow-Up of Renal Function After Peptide Receptor Radiation Therapy with 90Y-DOTA0,Tyr3-Octreotide and 177Lu-DOTA0, Tyr3-Octreotate