


Abstract
The imaging of dopamine transporter (DAT) with 99mTc-TRODAT-1 ([2-[[2-[[[3-(4-chlorophenyl)-8-methyl-8-azabicyclo[3,2,1]oct-2-yl]methyl](2-mercaptoethyl)amino]ethyl]amino]ethanethiolato(3-)-N2,N2′,S2,S2′]oxo-[1R-(exo-exo)]-99mTc-technetium) and SPECT has been recently proposed to be a valuable and feasible means of assessment of the integrity of dopamine neurons. The purpose of this study was to further investigate the clinical correlations and the age-specific sensitivity and specificity of this new approach in the diagnosis of patients with idiopathic Parkinson’s disease (PD) that manifests in patients >50 y of age. Methods: SPECT imaging with 99mTc-TRODAT-1 was conducted in 78 consecutive PD patients and in 40 age-matched healthy subjects. The images were obtained 4 h after the intravenous injection of the tracer. The ratios of specific striatal binding to nonspecific occipital binding were calculated. S/O represents the ratio for whole striatal binding, whereas P/O and C/O represent the putamen and caudate nucleus, respectively. Statistical analyses of the sensitivity and specificity of these ratios in different age-specific subgroups were performed. The correlations between these ratios and clinical assessments were also analyzed. The age-related declines in the striatal binding in both patients and controls were given particular focus. Results: The S/O, C/O, and P/O ratios decreased significantly both contralaterally and ipsilaterally to the dominant symptomatic side in the PD group (P < 0.0001). The mean reduction of binding was found in the order of putamen (contralateral side, −81%; ipsilateral side, −67%) and caudate nucleus (contralateral side, −46%; ipsilateral side, −40%). The sensitivity and specificity of both P/O and S/O ratios were 100% in discriminating PD patients from healthy subjects in the age-specific groups. The binding ratios correlated negatively with the Unified Parkinson’s Rating Scale and Hoehn and Yahr (H–Y) staging. Of particular interest, the binding of the striatum contralateral to the asymptomatic side in H–Y stage I patients also decreased significantly. The age-related decline of these ratios was significant in the control group. Conclusion: We have demonstrated that 99mTc-TRODAT-1 SPECT has a high sensitivity and specificity for measuring the decrement of DAT in PD patients. In addition to its wide availability, we suggest that this new approach may serve as a diagnostic marker for PD.
The current diagnosis of idiopathic Parkinson’s disease (PD) is substantially based on the clinical symptoms—including resting tremor, rigidity, bradykinesia, and postural instability—as well as a favorable response to levodopa therapy. An easily applicable marker for the diagnosis is still unavailable. Several proposed clinical criteria have been established (1,2), and the most recent one has classified PD as possible PD, probable PD, and definite PD (2). For definite PD, the presence of Lewy bodies in the pathologic findings is required. However, Lewy bodies are also present in many other diseases (3,4) and are probably absent in autosomal recessive juvenile parkinsonism (5). The clinicopathologic correlation is not totally satisfactory (6). For clinical diagnosis and further management, practical laboratory assistance is required.
Neuroimaging approaches using 18F-dopa PET have been the gold standard for the functional evaluation of nigral dopaminergic neurons in PD (7,8) and play a major role in research. Dopamine transporter (DAT) is a protein located on the membrane of the dopamine terminal in the striatum. The reduction of DAT correlates with the loss of dopaminergic neurons in the striatum (9,10). A compensatory downregulation of the DAT in the striatum in PD patients is further suggested by a PET study (11). This finding indicates that the functional imaging using the DAT ligand is more sensitive than 18F-dopa in detecting the degeneration of dopaminergic neurons even in the preclinical stage. Several ligands of DAT have been successfully used in PET and SPECT for the diagnosis of PD (12–16). However, these examinations require excessive time or cost and a cyclotron is necessary to produce these radioligands. This requirement seriously limits their clinical applications.
99mTc-TRODAT-1 ([2-[[2-[[[3-(4-chlorophenyl)-8-methyl-8-azabicyclo[3,2,1]oct-2-yl]methyl](2-mercaptoethyl)amino]ethyl]amino]ethanethiolato(3-)-N2,N2′,S2,S2′]oxo-[1R-(exo-exo)]-99mTc-technetium) is the first 99mTc-labeled tracer of DATs. In a series of recent reports, Kung and his colleagues have studied the availability of 99mTc-TRODAT-1 and suggested that it is an ideal ligand with a high affinity and specificity for DAT (17–19). Subsequent studies provided further evidence of the usefulness of 99mTc-TRODAT-1 SPECT for the evaluation of the presynaptic dopamine function in both animal and human experiments (20–23). Mozley et al. and Huang et al. (21,22) have reported studies of 99mTc-TRODAT-1 SPECT in the diagnosis of PD. However, the correlation between the clinical manifestations and the uptake of 99mTc-TRODAT-1 in the subregions of the basal ganglia was lacking. The number of studied patients was limited and the range of patient ages was wide. Also, the effect of the age-related decline of DAT (23,24) that would mimic the disease-related decline was not discussed.
Using a modified preparation of 99mTc-TRODAT-1 (25), by means of a kit produced by the Institute of Nuclear Energy Research of Taiwan (INER), we have studied the presynaptic DAT in PD, vascular parkinsonism, Machado–Joseph disease, and other parkinsonism disorders (26–31). For further evaluation of the diagnostic power among patients with PD, we extended our experience by conducting a 99mTc-TRODAT-1 SPECT study in a large series of PD patients whose clinical symptoms commenced after the age of 50 y. We calculated the age-specific sensitivity and specificity of 99mTc-TRODAT-1 SPECT in differentiating patients with PD from healthy subjects. The normal range of 99mTc-TRODAT-1 binding ratios and the threshold of disease diagnosis in age-specific subgroups are also provided.
MATERIALS AND METHODS
The clinical protocol was approved by the National Public Health Bureau and by the local ethics committee of Chang Gung Memorial Hospital. All subjects, including the PD patients and healthy volunteers, gave written informed permission before the SPECT scanning.
Subjects
Seventy-eight PD patients (38 women, 40 men; mean age, 68.6 ± 6.1 y; age range, 51–77 y), whose clinical symptoms commenced after the age of 50 y, were enrolled. None revealed a history of familial parkinsonism or had undergone any previous intracranial operations. Magnetic resonance (MR) images of the brain, in all patients, were normal, except for mild cortical atrophy. Sixty patients met the criterion for probable PD and 18 patients met the criterion for possible PD because the symptoms were present for <3 y (1,2).
The PD group then was divided into 3 subgroups, based on their age when undergoing the 99mTc-TRODAT-1 SPECT examination: 11 patients were in the 50- to 59-y-old age group, 44 in the 60- to 69-y-old age group, and 23 in the 70- to 79-y-old age group. A serial clinical assessment including the Unified Parkinson’s Rating Scale (UPDRS) and modified Hoehn and Yahr (H–Y) staging was undertaken in the “off” state by the same movement disorders specialist. Table 1 summarizes the basic clinical information and the assessments of the PD patients.
Clinical Data and Assessments of PD Patients in 3 Age-Specific Groups
The control group included 40 age-matched healthy volunteers (21 women, 19 men) from 49 to 79 y old (mean age, 63.2 ± 9.1 y). For comparison with the PD patients, 3 similar subgroups were formed: 15 were in the 50- to 59-y-old age group (mean age, 52.3 ± 3.8 y), 15 in the 60- to 69-y-old age group (mean age, 64.9 ± 2.3 y), and 10 in the 70- to 79-y-old age group (mean age, 73.2 ± 3.6 y).
Radiopharmaceutical Preparation
The 99mTc-TRODAT-1 was obtained in a 1-vial kit formulation from the INER (26). The final sterilized product was produced by autoclaving the mixture for 30 min. Radiochemical purity was 97% ± 2%, as measured with high-performance liquid chromatography.
Imaging Acquisition Protocol
All antiparkinsonian drugs and neuroleptic medications were discontinued at least 12 h before the test. After the clinical evaluation, patients were brought to the Nuclear Medicine Department. A dose of 925 MBq (25 mCi) 99mTc-TRODAT-1 was injected intravenously. SPECT images were acquired 4 h later using a Siemens MULTISPECT triple-head γ-camera, with fanbeam collimators and 120 equally spaced projections over 360°, taking 20 s per step and using a 128 × 128 matrix size. Individual images were reconstructed with backprojection using a ramp–Butterworth filter, with a cutoff of 0.3 cm−1 and an order of 10. The data were corrected for the effects of photon attenuation using Chang’s first-order method with an attenuation coefficient of 0.12 and with the attenuation ellipses defined on the summed images of the entire dataset and applied, without modification, to all images individually. No attempt was made to correct for partial-volume effects. The slice thickness and in-plane size was 2.9 mm. Three reconstructed transaxial slices were summed together and reoriented to be parallel to the orbitomeatal (OM) line with the highest signal in the region of the basal ganglia as the central slice (27–29). All images underwent a blind review by one nuclear physician, who had experience with this type of image.
MRI of Brain
Each subject also provided a single MR image for anatomic structure information for image coregistration. The MR images were acquired on a VISION VB33D 1.5-T instrument (Siemens Medical Systems). T1-weighted axial images (repetition time [TR], 500 ms; echo time [TE], 25 ms) and T2-weighted axial images (TR, 3,500 ms; TE, 120 ms) were obtained in the transaxial plane (6-mm thickness, 0.6- mm gap). The MR images were resized and resliced in planes parallel to the OM line.
Data Processing
The SPECT images were first coregistered automatically with each subject’s corresponding MR image and then fine adjusted manually with a visual inspection of the overlaid images, using MultiModality software (Nuclear Diagnostics). For an analysis of striatal 99mTc-TRODAT-1 binding, we selected the slice with the highest activity. Regions of interest (ROIs) were drawn on the MR image corresponding to the putamen, caudate nucleus, and occipital cortex, and the ROIs were applied directly to the coregistered SPECT images. The ratios of specific to nonspecific striatal 99mTc-TRODAT-1 binding were then calculated as: 99mTc-TRODAT-1 binding ratio = (ROI counts − occipital cortex counts)/occipital cortex counts.
We also calculated the (putamen − occipital cortex)/(caudate − occipital cortex) ratio (P/C ratio) to determine the specific pattern and the selective loss of DATs in the PD group.
In the PD group, we defined the contralateral striatum as the striatum located opposite the side with the dominant symptoms. In the control group, the contralateral striatum was defined as the right striatum and the ipsilateral striatum was defined as the left striatum.
For an expression of the asymmetry of the binding ratio in the PD group, we calculated the asymmetric index (ASI) as the following formula:
 .
.
Statistical Methods
The Mann–Whitney test was performed to compare the striatal binding ratios between the PD group and the control group since the binding ratios in the PD group were not normally distributed. The Wilcoxon signed rank test was used to compare the difference in the binding ratios between the contralateral and the ipsilateral striatum for the PD group. All tests were defined as significant when P < 0.05. The 2-by-2 table was used to determinate the cutoff levels and to examine the sensitivity and specificity of the binding ratios between the PD and control groups. Receiver-operating-characteristic (ROC) curves (SPSS 10.0 software; SPSS Inc.) were generated to compare the diagnostic accuracy of each binding ratio, based on to the areas under the ROC curves. Spearman correlation and multiple regression analyses were performed to evaluate the correlation between binding ratios and severity, duration, and age.
RESULTS
Figure 1 shows the 99mTc-TRODAT-1 SPECT images of 3 PD patients in different H–Y stages and 1 healthy subject. A marked decrease in 99mTc-TRODAT-1 uptake in the striatum was easily observed in the patients. The reduction of uptake was most pronounced in the putamen contralateral to the dominant symptomatic side. We could usually distinguish PD patients from healthy subjects by viewing the images.

99mTc-TRODAT-1 SPECT images of 4 subjects. (A) A 62-y-old female healthy volunteer. (B) A 63-y-old female patient (H–Y stage I) with left side tremor and bradykinesia. The binding of 99mTc-TRODAT-1 decreased significantly in the right striatum and was also slightly reduced in the left putamen. (C) A 62-y-old female patient (H–Y stage III) with bilateral bradykinesia, dominant in the left side. The uptake decreased significantly in the bilateral putamen and was also slightly reduced in the bilateral caudate nuclei. The reduction was more severe in the right striatum. (D) A 63-y-old male patient (H–Y stage V) with severe bilateral akinesia. The uptake decreased in all defined regions.
Table 2 summarizes the S/O, C/O, and P/O ratios of PD patients and controls in each age-specific group. The mean binding ratios of all defined regions in the PD group were significantly lower than those in the control group (P < 0.0001). The mean P/C ratios were also significantly lower in the PD group (contralateral side, 0.21 ± 0.11; ipsilateral side, 0.34 ± 0.13) than those in the control group (both sides, 0.63 ± 0.05; P < 0.0001). Loss of the DAT was most severe in the contralateral putamen compared with the controls, followed by the ipsilateral putamen, contralateral caudate nucleus, and ipsilateral caudate nucleus (Table 2). The selective loss of the DAT was the characteristic finding of the PD patients.
Mean 99mTc-TRODAT-1 Binding Ratios in Defined Regions of PD Patients in Each Age Group and Healthy Volunteers
In the control group, the 99mTc-TRODAT-1 binding ratios were symmetric (Fig. 2A). The 99mTc-TRODAT-1 binding ratios of the PD group were significantly asymmetric (Fig. 2B). The mean ASI of the PD group was 65.6 in the putamen, 30.7 in the whole striatum, and 11.2 in the caudate nucleus.

99mTc-TRODAT-1 binding ratios of the healthy subjects (A) and PD patients (B) in different age groups. The binding ratios of the healthy subjects were symmetric and decreased significantly with aging. The binding ratios of the PD patients were asymmetric. The significant decrease of binding ratios in the contralateral putamen is a specific finding in PD.
Table 3 summarizes the sensitivity and specificity of the 99mTc-TRODAT-1 binding ratios using ROC curve analysis. When analyzing all patients together, only the contralateral P/O and the contralateral P/C had 100% sensitivity and specificity in discriminating the PD patients from the healthy subjects. However, with further analysis in 3 different age-specific groups separately, all binding ratios, except the C/O ratios and ipsilateral P/C ratios, showed 100% sensitivity and specificity. Therefore, the decrease of 99mTc-TRODAT-1 binding in the striatum was extremely reliable in the diagnosis of PD. Using ROC analysis, we further demonstrated the statistical age-specific cutoff level for disease diagnosis in the different regions of the striatum (Table 3).
Sensitivity and Specificity of 99mTc-TRODAT-1 Binding Ratios and Cutoff Levels for Disease Diagnosis in 3 Age-Specific Groups
There was no sexual difference in the 99mTc-TRODAT-1 binding ratios in the PD and control groups. The binding ratios also declined with age in the control group (Fig. 3A). Using Spearman rank correlation analysis, the age-related decline in all defined regions was significant in the control group (P < 0.0001). In the PD group, the reduction of the S/O, C/O, and ipsilateral P/O ratios also correlated with age (Fig. 3B). The contralateral P/O did not decline significantly with age in the PD group. The P/C ratios did not correlate with age in either group.
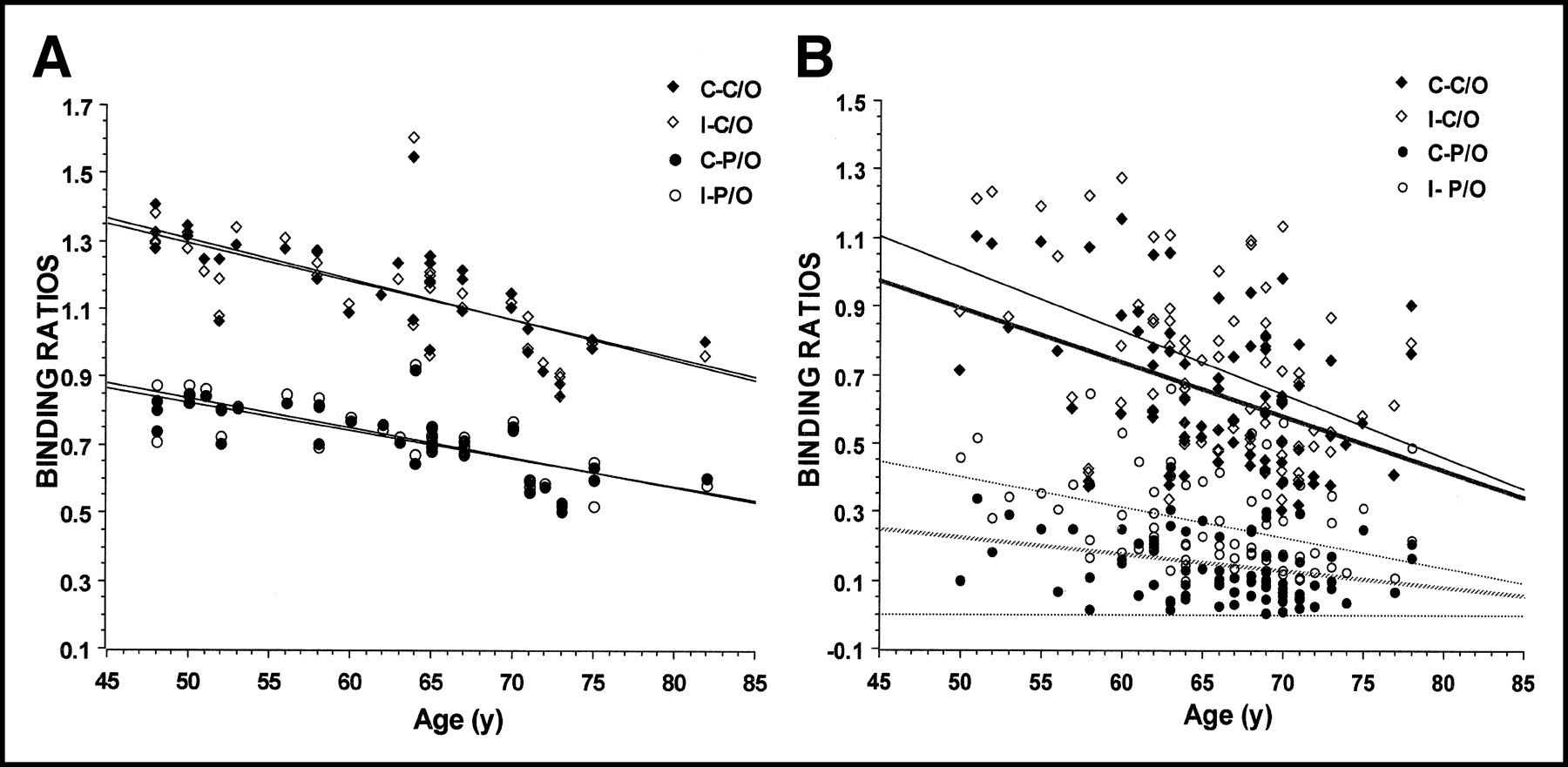
The correlation of age and the C/O and P/O ratios in the controls (A) and PD patients (B). In the control group, the reduction of the binding ratios with normal aging was symmetric and even loss. The binding ratios also decreased with aging, except the contralateral P/O ratios in the PD patients with a similar duration and severity of disease (C-C/O, P = 0.0004; I-C/O, P = 0.016; C-P/O, P = 0.211; I-P/O, P = 0.045). The pattern of the age-related decline of binding ratios was quite different between the PD patients and the normal controls., regression line for C-C/O;, regression line for I-C/O; ····, regression line for C-P/O; ·····, regression line for I-P/O.
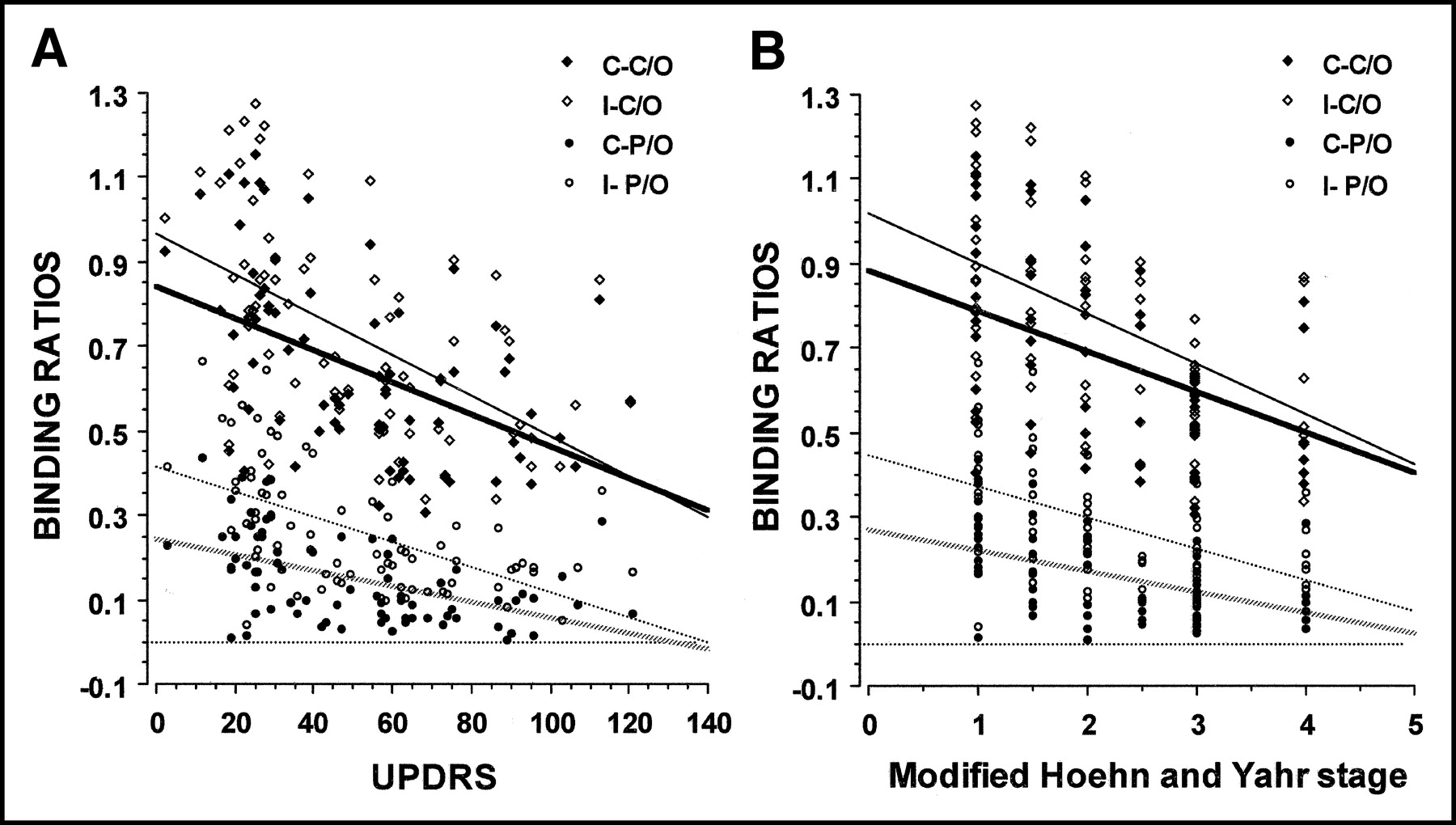
Using Spearmen correlation analysis, the reduction of the binding ratios significantly correlated with the UPDRS and H–Y staging (P < 0.0001) in the PD group (Fig. 4).
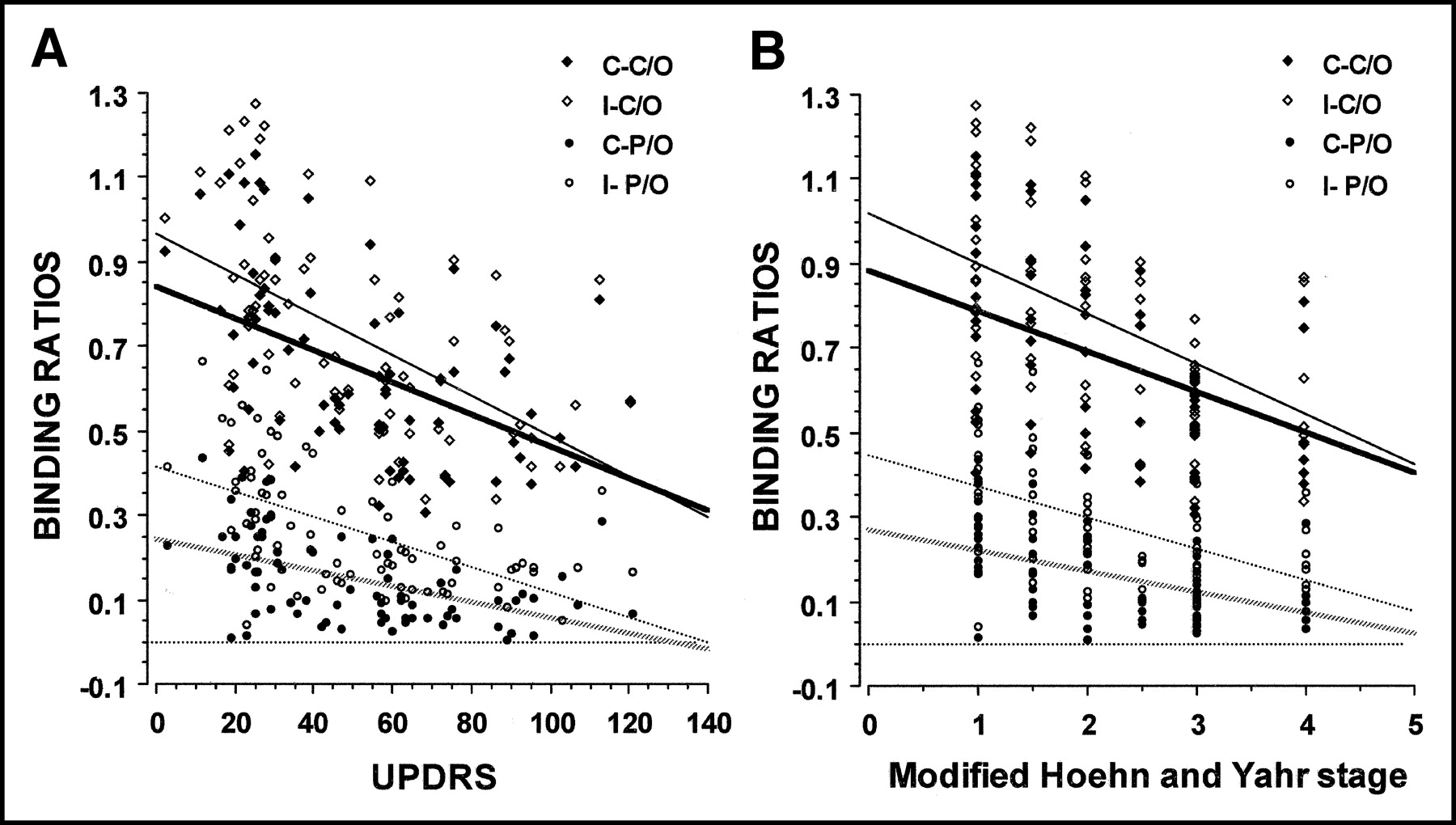
The binding ratios of 99mTc-TRODAT-1 in the PD patients significantly negatively correlated with the UPDRS (A) and H–Y staging (B)., regression line for C-C/O;, regression line for I-C/O; ····, regression line for C-P/O; ·····, regression line for I-P/O.
We paid particular attention to the early-stage PD patients with unilateral symptoms (H–Y stage I). Twenty-three PD patients with H–Y stage I (mean age, 61.6 ± 6.2 y; age range, 51–69 y; mean duration of disease, 3.2 ± 2.1 y) were compared separately with 26 age-matched healthy subjects (mean age, 59.2 ± 6.5 y; age range, 50–67 y). The S/O, C/O, and P/O ratios contralateral to the asymptomatic side in those patients were significantly lower than those of the healthy subjects (P < 0.0001) (Table 4). Table 4 summarizes the sensitivity and specificity of the 99mTc-TRODAT-1 binding ratios for the early stage. The S/O, P/O, and contralateral P/C ratio had 100% sensitivity and specificity in discriminating early-stage PD patients from the healthy subjects in 2 different age-specific groups.
Mean Binding Ratios and Sensitivity and Specificity of 99mTc-TRODAT-1 of 23 PD Patients with H–Y Stage I and 26 Age-Matched Healthy Volunteers
DISCUSSION
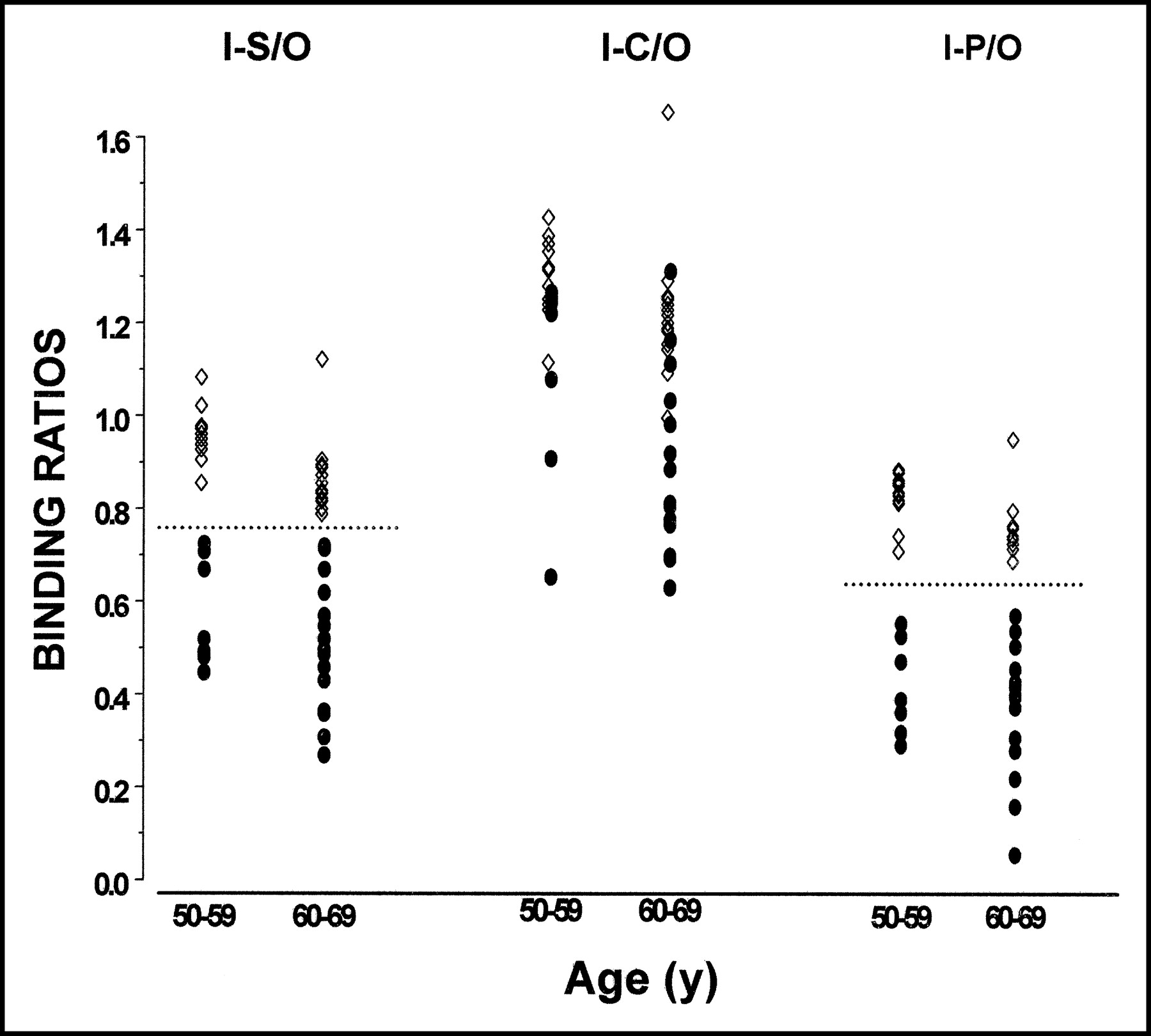
We have demonstrated that there was a significant decrease of striatal 99mTc-TRODAT-1 binding in PD patients with an onset age of ≥50 y compared with age-matched healthy controls. In the majority of patients, this distinction was obvious when viewing the images. However, the age-related decline of the DAT in healthy subjects was sometimes similar to the reduction of the DAT in patients with PD (Fig. 5) (21,23,24). A high sensitivity and specificity of 99mTc-TRODAT-1 uptake values in discriminating PD patients from healthy subjects has been reported by Mozley et al. (21). These researchers believed that most of the inaccuracy in their study could be accounted for by the hemi-PD patients and the elderly volunteers. The wide range of ages of the patients and controls, even with the mean ages matched between the 2 groups, could reduce the diagnostic accuracy (21). Our results showed a slightly higher sensitivity and specificity than those in Mozley’s report, when analyzing all patients together. However, the sensitivity and specificity greatly increased in all subregions when the subjects in different age-specific groups were analyzed. Therefore, establishing the normal range of the binding ratios in different age groups is very important. Setting up an age-specific cutoff level for disease is also useful in clinical diagnosis in the early stage of disease and in the screening of the high-risk population, such as the relatives of familial parkinsonian patients. We now have set up the age-specific normal range and the cutoff levels of the 99mTc-TRODAT-1 binding ratios in the Taiwanese population (Table 5).

The ipsilateral P/O ratios of the controls and the PD patients. The binding ratios of 99mTc-TRODAT-1 in the elderly controls were equal to or even lower than those in some younger PD patients. The dotted circle = ipsilateral P/O ratios of the controls; the dotted oval = ipsilateral P/O ratios of the PD patients.
Normal Range of 99mTc-TRODAT-1 Binding Ratios in 3 Different Age Groups
The dopamine neurons, which are located in the ventral tier of the substantia nigra, were most severely affected in PD patients (32). The characteristic loss of DAT binding in the posterior putamen has been well documented in other studies (14–16,21,22). However, there is a lack of an anatomic and gross demarcation between the anterior and posterior putamen using the MRI atlas. To draw the ROI of the posterior putamen is sometimes difficult. The intra- and interinvestigator’s variation, as well as the bias of diagnosis, may increase. In our study, we also confirmed that the contralateral P/O and P/C ratios were the best predictors for distinguishing all PD patients from the controls (100% sensitivity, 100% specificity). However, the sensitivity and specificity of the S/O ratios were 100% and equal to those of the P/O ratios in 3 different age-specific groups. The S/O and P/O ratios were also easier to apply in clinical use than the ratios of the posterior putamen. We conclude that, using age-specific comparisons, the S/O and P/O ratios can be used as diagnostic markers instead of the binding ratios of the posterior putamen.
Similar to 2β-carbomethoxy-3β-(4-iodophenyl)tropane (β-CIT), the binding capability of 99mTc-TRODAT-1 to the DAT is highly specific (18,19). However, 99mTc is far superior to 123I for routine nuclear medicine use. The striatal-to-background ratios at 240–280 min showed greater differences between the healthy subjects and PD patients (29). It is important that only a 4-h waiting period was required to perform 99mTc-TRODAT-1 SPECT, instead of the 20 h needed for β-CIT SPECT (29). The shorter time requirement allowed for a 1-d scan session and gave the 99mTc-TRODAT-1 SPECT improved applicability. Both the ease in preparation and the widespread availability of 99mTc-TRODAT-1 are certainly other advantages. Our results support previous findings that have suggested that 99mTc-TRODAT-1 SPECT is useful in detecting the decrease of striatal DAT concentration. We have further affirmed that 99mTc-TRODAT-1 SPECT is a superior tool for clinical applications.
We used the occipital cortex as a reference region because of its low density of DAT (15,19,22). To overcome the background activity and to reduce the interinvestigator variation, we fused the SPECT imaging with individual MR images to accurately draw the area of the caudate and putamen. However, we proved that the S/O ratio was a sensitive and specific diagnostic marker as well as the P/O ratio. According to our study, investigators can simply draw the striatum instead of the putamen. The individual MR scan is not necessary the routine clinical use.
The reduction of the binding ratios in all defined regions significantly correlated with the severity of disease. This indicates that 99mTc-TRODAT-1 SPECT is useful in monitoring the progression of disease as well as the effect of the neuroprotective therapy.
In the PD patients with unilateral symptoms, the ipsilateral P/O ratios and S/O ratios (contralateral to the asymptomatic side) were significantly reduced by about 50% and 40%, respectively. These results are compatible with pathologic findings (33) and other SPECT studies (15). In the study of Huang et al., the uptake ratios of the ipsilateral putamen and posterior putamen showed several overlaps between the stage I PD patients and the controls (22). However, in our study, the ipsilateral S/O and P/O ratios were significantly lower in the early-PD group, without any overlapping between the 2 groups (Fig. 6). The sensitivity and specificity of the ipsilateral S/O, P/O, and P/C ratios were 100% in the different age-specific group. This means that 99mTc-TRODAT-1 SPECT is a potentially useful tool for the preclinical diagnosis of an individual subject and for the screening of hereditary parkinsonism (30,31). The confined age range of the subjects, the higher dose of 99mTc-TRODAT-1, and the triple-head camera are the reasons why the results in our study were superior to those of Huang’s report.

The binding ratios in 28 age-matched controls and in 24 PD patients with unilateral symptoms: The ipsilateral S/O and P/O ratios, which represented the DAT concentration in the preclinical striatum, showed a more clear-cut reduction than the ratios in the healthy subjects. •, PD; ⋄, control.
Previously, the rate of misdiagnosis of idiopathic PD was as high as 24% (6). The PD patient group might contain patients with other parkinsonian disorders, such as multiple system atrophy, progressive supranuclear palsy, or vascular parkinsonism. However, we used more stringent criteria to select patients (2). Diagnostic accuracy could be up to 90%, which may be the highest using current diagnostic criteria (34). That the patients were more stringently selected in our study than in other studies may be another reason for the superior sensitivity and specificity in our study (21,22).
There were 2 major reasons why we selected sporadic PD patients with a disease onset after 50 y of age as the study subjects. One was that the vast majority of PD is sporadic, with a mean age of >60 y (35). The other reason was to exclude the possibility of a genetic etiology in those patients whose onset of disease was <50 y of age, as has been recently suggested by Tanner et al. in their study of twins (36).
The striatal DAT decreased significantly with age in the healthy subjects. The decrease in 99mTc-TRODAT-1 uptake was also symmetric, in correlation with the increase in age. Interestingly, the rate of decrement for P/O and C/O was similar, which indicates that the neuronal degeneration of the substantia nigra, reflected from DAT activity, was diffuse and symmetric in normal aging. These results correspond to the symmetric and even loss of nigral neurons in a postmortem study (37) and other functional imaging studies (23,24,38). Variable correlations between the striatal DAT binding and age in PD patients have been reported in the literature (with a wide-ranging age of onset). Some authors have reported a smaller age-related decline in the ipsilateral striatum (39), whereas other authors (40) have shown no age-related decline. In our PD patients with an age of onset of >50 y, the significant correlation between age and binding ratios could be detected in the caudate regions and ipsilateral putamen. The age-related decline of binding ratios was more significant in the earlier-stage and younger patients. Using an age-matched control group is very important when investigating the 99mTc-TRODAT-1 SPECT images. However, the rate of age-related decline in the PD patients was similar to that of the control group. We suggest that aging may not play a major role in the etiology of PD. Further studies using 99mTc-TRODAT-1 are necessary to evaluate the aging factor in PD and its progression.
CONCLUSION
99mTc-TRODAT-1 SPECT is accurate and widely available for the assessment of DAT activity, which might shed light on the integrity of the presynaptic nigrostriatal function. There are several ways to make this examination more sensitive and specific for the diagnosis of PD: careful clinical screening, using a higher dose of 99mTc-TRODAT-1 and a triple-head camera, fusing the SPECT images with individual MR images, and setting up the age-specific thresholds of disease. The high sensitivity and specificity of SPECT images can serve as a useful marker in the clinical diagnosis of PD and even in preclinical screening for asymptomatic individuals.
Acknowledgments
The study was supported by grants from the Chang-Gung Medical Research Council (CMRP957), the Institute of Nuclear Energy Research (90-NU-7-182A-003), and the National Science Council (NMRPG0073) of Taiwan.
Footnotes
Received May 19, 2003; revision accepted Oct. 9, 2003.
For correspondence or reprints contact: Chin-Song Lu, MD, Movement Disorders Unit, the First Department of Neurology, Chang Gung Memorial Hospital; 5 Fu-Shin St., Kweishan, Taoyuan, Taiwan.
E-mail: c81214{at}adm.cgmh.org.tw





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}