


Abstract
Therapeutic options in patients with advanced-stage gastroenteropancreatic (GEP) neuroendocrine tumors are limited. We compared the efficacy of radionuclide therapy with 111In-pentetreotide and 131I-metaiodobenzylguanidine (MIBG) in 20 patients (group A) with the outcome of similar patients who could not be treated for nonmedical reasons (group B, n = 12). The intent was to treat all patients because of uncontrolled tumor disease (n = 21), contraindication to chemotherapy or surgery (n = 7), or uncontrolled and badly tolerated clinical symptoms (n = 4). Methods: Group A patients received 3 monthly administrations of 3.7–7.4 GBq of 131I-MIBG (n = 5) or 7 GBq of 111In-pentetreotide (n = 15), according to the best tracer uptake. Clinical evaluation, biologic tests, and conventional imaging were performed at 3, 6, 12, 18, and 24 mo. Therapy was considered beneficial if clinical status improved, laboratory tests for secreting tumors improved by >20%, tumor progression was halted, the size of the most significant localization had decreased by >25%, and the dosage of analgesic and cold somatostatin therapy could be lowered. Pejorative events were defined as side effects due to therapy, relapse in clinical symptoms, tumor progression, tumor laboratory marker increase, and death. Results: The overall survival rate at 3 mo was significantly higher in group A (P = 0.05). Radionuclide therapy was beneficial in 14 patients (73% of group A), with only 1 significant side effect. The average time before relapse was 16.1 ± 7.8 mo. The overall Kaplan–Meier survival rate and cumulative progression-free and cumulative event-free survival rates during the first 15 mo were significantly higher in patients receiving radionuclide therapy (P = 0.019, P = 0.024, and P = 0.019, respectively). Conclusion: Radionuclide therapy is feasible and safe and significantly defers the occurrence of fatal and nonfatal events in patients clinically uncontrolled by conventional therapy.
Therapeutic options in patients with progressive and disseminated metastatic neuroendocrine gastroenteropancreatic (GEP) tumors are often limited, and prognosis is often poor (1,2). First-line choice of systemic chemotherapy has no obvious effect in half of the patients, and second-line rescue chemotherapy is effective in no more than a few patients. Interferon has no effect on tumor regression, even when used in combination with somatostatin analogs (3). Hepatic artery embolization is effective only in patients with large liver metastases but has no impact on extrahepatic disease (4). Consequently, radionuclide therapy may be proposed to patients with uncontrolled disease after conventional therapy (5,11).
Internal radiotherapy uses a specific agent that links to tumor cells, coupled to a radiotracer for electron-dose delivery. Two agents have been proposed for GEP tumor imaging: pentetreotide ([DTPA-d-Phe1]octreotide, where DTPA is diethylenetriaminepentaacetic acid) (6–8) and metaiodobenzylguanidine (MIBG) (9,10). MIBG can be labeled with 131I, which has a long half-time (8 d) and a maximal electron range of about 2.4 mm and is established in the treatment of tumors derived from the neural crest, such as GEP tumors (11). In France, 131I-MIBG can be used for radionuclide therapy. Octreotide labeling with 90Y has recently been proposed for radionuclide therapy (12–16) but, to date, it is not commercially available in France. Because 111In emits short-range electrons that can have significant biologic effects at a cellular level (17–19), radionuclide therapy with a high activity of 111In-pentetreotide has been used in a few patients with GEP tumors (5,20–30).
To our knowledge, there are no randomized controlled trials with radionuclide therapy in GEP tumors. We report the results of radionuclide therapy with either 111In-pentetreotide or 131I-MIBG in a population of patients with advanced-stage GEP tumors. Although the initial intent was that all patients would undergo treatment, a subset of patients was not treated for reasons pertaining to nonmedical considerations. Therefore, treated (n = 20) and untreated (n = 12) patients were compared with respect to fatal and nonfatal adverse events.
MATERIALS AND METHODS
Population
From January 1998 to October 2002, 33 consecutive patients were referred for radionuclide therapy as rescue therapy. All had documented advanced-stage GEP tumors and were in a clinical situation of therapeutic deadlock according to established criteria (2). With the exception of 1 patient who had a contraindication for chemotherapy, all patients had been treated with first-line chemotherapy using both 5-fluororuracil and streptozotocin. All patients had progressive tumor disease uncontrolled by previous and repeated conventional therapy (14 in group A, 7 in group B), presented a temporary or definitive contraindication to chemotherapy or surgery, needed a reduction of tumor volume before surgery (4 in group A, 3 in group B), or presented uncontrolled and badly tolerated clinical symptoms such as diarrhea, nausea, vomiting, flush, or abdominal pain (2 in group A, 2 in group B). One patient was excluded because of impaired renal function with a serum creatinine level of >200 μmol/L. No patient had hemogram anomalies such as hemoglobin concentration < 10 g/L, leukopenia < 3,000 white blood cell counts/mm3, or thrombocytopenia < 80,000 platelets/mm3. Finally, 32 patients entered the study. Patient characteristics are summarized in Table 1.
Patient Characteristics
Conditions for Delivering Internal Radiotherapy
In France, 131I-MIBG is the only agent that is officially allowed for the radionuclide therapy of GEP tumors, with treatment costs paid by the national health insurance system. Conversely, 111In-pentetreotide has no agreement, and the cost for 111In-pentetreotide therapy (around $4,700) is not supported by the national health insurance system. Because the direct payment for the cost of therapy by a patient is absolutely forbidden in France, a specific administrative procedure was established to obtain suitable financing. This implied that the institutions from which the patients were referred for staging and therapy had to be charged, which was not always possible due to the local agreement of each institution. Each included patient underwent both 111In-pentetreotide and 131I-MIBG imaging to compare tumor tracer uptake. If 131I-MIBG uptake was comparable to 111In-pentetreotide uptake, with a minimum uptake of grade 3 according to Krenning et al. (28) and Valkema et al. (29) (i.e., tumor uptake clearly higher than physiologic liver uptake) and a persistent 131I-MIBG uptake on the fourth day after injection, 131I-MIBG therapy was preferred over 111In-pentetreotide (n = 5). The intent was that other patients were to receive 111In-pentetreotide therapy (n = 27).
Unfortunately, 8 patients with insufficient 131I-MIBG uptake could not obtain financial agreement for 111In-pentetreotide therapy and did not receive radionuclide therapy. Four other patients refused to enter the study or to remain in a lead-shielded room for 5–7 consecutive days. At follow-up, 20 patients had received radionuclide therapy (group A) and were compared with the 12 untreated patients (group B).
Imaging
All imaging procedures were performed on a dual-head DST-XL γ-camera (SMV; General Electric Medical Systems).
111In-Pentetreotide Imaging.
Before radionuclide therapy, imaging was performed 4, 24, and, sometimes, 48 h after an intravenous administration of 140 MBq of 111In-pentetreotide (Mallinckrodt Nuclear Medicine). Imaging consisted of static 256 × 256 anterior and posterior views over the head and thorax excluding the liver (500 kilocounts or 900 s) and over the abdomen (500 kilocounts or 600 s) with 4 additional oblique and 2 profile views and abdominal tomography. The photopeak was centered on 171 and 245 keV, and cameras were equipped with medium-energy collimators.
During internal radiotherapy, anterior and posterior whole-body imaging (12 cm/min) and anterior and posterior static views over the abdomen and thorax (1,000 kilocounts or 300 s) were performed on days 5, 8, and 12.
131I-MIBG Imaging.
Before radionuclide therapy, imaging was performed 4 h, 24 h, 5 d, and 8 d after an intravenous injection of 37 MBq of 131I-MIBG (Cis-Bio International, Scherring S.A.) with a photopeak centered on 364 keV and high-energy collimators. The imaging procedure was similar to that of 111In-pentetreotide imaging.
During internal radiotherapy, anterior and posterior whole-body imaging (12 cm/min) and anterior and posterior static views over the abdomen and thorax (1,000 kilocounts or 300 s) were performed on days 5, 8, and 12.
Radionuclide Therapy
Patients were given 3 monthly therapeutic administrations of 7 GBq of 111In-pentetreotide or were given 3.7, 5.6, or 7.4 GBq of 131I-MIBG if the body weight was <50 kg, 50–70 kg, or >70 kg, respectively (Table 2). All patients were hydrated intravenously (with 1 L of 0.9% saline or 5% glucose) 1 h before and throughout tracer administration, followed by an additional liter of the same liquid solution for 18 h, with recommendations to drink water. No additional renal protective procedure was used. Patients were hospitalized in specific lead-shielded rooms for 5–7 d, until the external dose rate had decreased according to French regulation. Renal function and hematologic parameters were monitored with repeated blood samples throughout therapy and at follow-up.
Pretherapeutic Imaging and Radionuclide Therapy Characteristics
Follow-Up
A standardized clinical evaluation was performed at 3, 6, 12, 18, and 24 mo after the first cure. Two independent observers scored symptoms semiquantitatively (0 for absence of symptoms, 1 for mild clinical perturbations, 2 for major or invalidating symptoms). At the same times, laboratory tests and conventional imaging (CT or MRI) were performed. Tumor sites were numbered and diameters of significant localizations were measured. Radiologic measurements of tumor response were performed by therapy-blinded radiologists according to World Health Organization (WHO) criteria (minor response, decrease of tumor diameter from 25% to 50%; partial remission, decrease from 50% to 75%; complete remission, decrease from 75% to 100%). Since progression of neuroendocrine tumors is usually slow—particularly when compared with the poor expected spontaneous prognosis of our patients—we deliberately defined progression as an increase in tumor diameter of >25% (instead of >50% for WHO criteria). Occurrence of adverse events and time to symptom relapse were recorded.
Radionuclide therapy was considered beneficial if the patient had experienced no adverse event and fulfilled at least one of the following criteria: (a) clinical status and clinical score improved; (b) patient returned to a normal ambulatory way of life; (c) laboratory tests for secreting tumors improved by ≥20%; (d) tumor progression was halted, as evidenced by repeated conventional imaging and somatostatin receptor scintigraphy; (e) the number of tumor sites or the size of the most significant localization had decreased by ≥25%; and (f) the dosage of analgesic and cold somatostatin therapy could be lowered.
Radionuclide therapy was considered not beneficial if the patient met 1 pejorative event: relapse in clinical symptoms for which the patient was initially referred for radionuclide therapy, tumor progression or tumor laboratory marker increase, renal or hematologic side effects due to radionuclide therapy (even temporary), and death.
Data Management
Results are expressed as mean ± SD. Comparison between groups was performed using the χ2 test (with Yates’ adjustment when appropriate) for qualitative data and the unpaired t test for quantitative data. Overall Kaplan–Meier survival curves, progression-free Kaplan–Meier survival curves, and pejorative event-free Kaplan–Meier survival curves were generated for each group and compared with a log-rank test.
RESULTS
There was no significant difference between patients of group A and group B with respect to age, sex, and duration of disease before radionuclide therapy (Table 1). Patients in group A had a significantly longer follow-up than patients in group B: 26.6 ± 16.5 mo versus 9.9 ± 4.6 mo, respectively (P = 0.001). Gastrinomas were more frequently observed in group B (n = 6) than in group A (n = 1). Tumor uptake grades, as evidenced by pretherapeutic 111In-pentetreotide and 131I-MIBG imaging, are reported in Table 2, whereas the occurrence of fatal and nonfatal events (radiologic response, biologic response, and clinical status) are reported in Table 3.
Results: Fatal and Nonfatal Events
Fatal Events
One patient in group A (patient 20) was in a critical state when he was included in the study. He rapidly died of septicemia during the second tracer infusion. He was the only patient to have liver and peritoneal metastases. The medical staff agreed that the patient’s death did not relate to radionuclide therapy but, rather, to his end-stage disease. Because this patient did not receive the entire treatment, he was secondarily excluded from data analysis.
At the end of the follow-up period, 5 of the remaining 19 patients (26.9%) in group A and 5 of 12 patients (41.7%) in group B had died (P = not significant). The overall survival rate at 3 mo was significantly higher in group A than in group B (4 vs. 0 deaths; P = 0.05). The overall Kaplan–Meier survival curves in Figure 1 demonstrate a higher cumulative overall survival rate during the first 15 mo in patients receiving radionuclide therapy (P = 0.019).

Overall Kaplan–Meier survival curves of patients in group A (treated) and group B (nontreated) (P = 0.019).
Nonfatal Adverse Events
These events are displayed in Table 3. One patient (patient 13), treated with 131I-MIBG for a very fast and extensive tumor progression, developed pancytopenia during the second radionuclide administration. Therapy was discontinued, and this was reported as an adverse event in the event-free survival analysis. Nevertheless, it should be emphasized that a radiologic stabilization was then observed during the following 12 mo (and was reported in the progression-free survival analysis). Finally, because of this adverse event and despite this tumor stabilization, therapy was reported in Table 3 as not beneficial, according to the follow-up section.
Efficacy of Radionuclide Therapy
Radionuclide therapy was considered globally beneficial on radiologic, biologic, and clinical previously defined criteria in 14 of 19 patients of group A (73% of group A), with no side effects. Nine of these 14 patients (47% of group A) improved clinically. Two patients could work again, and 4 patients had their analgesic or cold somatostatin therapy significantly reduced. In 4 patients (21%) with carcinoids, there was a major marker response evidenced by a decrease of urinary 5-hydroxyindoleacetic acid (5-HIAA) by 65% ± 21% in 3 patients and a decrease of neuron-specific enolase (NSE) by 37% in the remaining patient (NSE being the sole abnormal marker in his case). It is worth noting that radionuclide therapy normalized urinary 5-HIAA in one of these patients (patient 18). Conventional imaging showed stabilization of tumors in 14 patients (73%, including patient 13) at 3 and 6 mo. Significant tumor regression (–75%) of a 20 × 20 mm liver metastasis occurred in patient 18 (who had a normalized marker), whereas in the same patient, a minor response was observed for 3 other tumor sites. 123I-MIBG uptake of these tumor sites was considerably reduced at 15 mo after radionuclide therapy (Fig. 2).
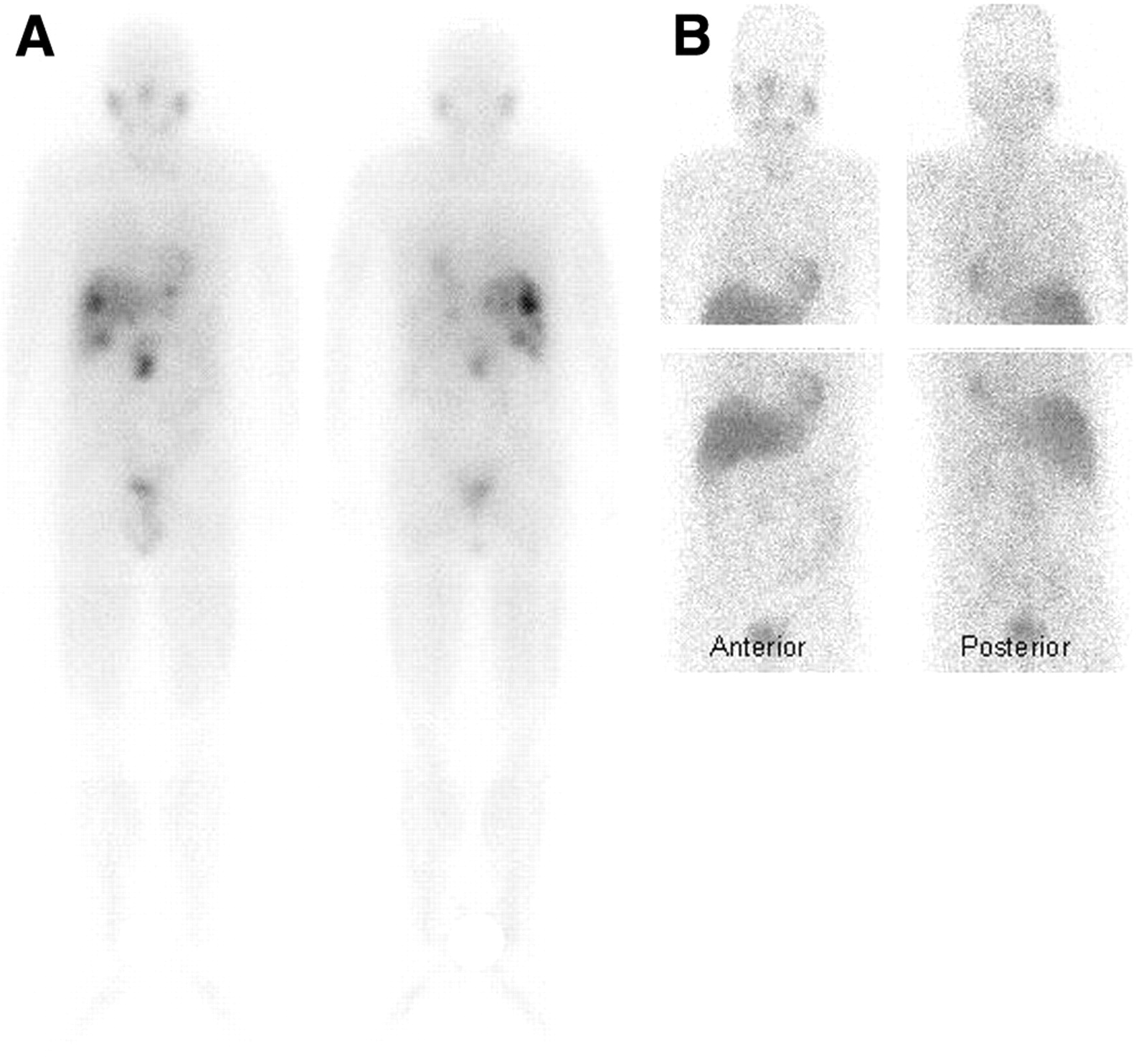
(A) 131I-MIBG imaging of patient 18 during radionuclide therapy shows high uptake in multiple liver metastases and primary site. (B) Fifteen months later, 123I-MIBG imaging shows partial remission, with only faint uptake in primary site.
For the 14 responder patients, the average time between the onset of cure and relapse was 16.1 ± 7.8 mo. At 6 mo after therapy, these 14 patients remained asymptomatic. At 12 mo, 7 of 14 patients were again symptomatic.
With regard to the radiotracer, 4 of 5 patients receiving 131I-MIBG improved, whereas 10 of 14 improved with 111In-pentetreotide (P = not significant). The time to relapse was not significantly different between 131I-MIBG (13.2 ± 5.6 mo) and 111In-pentetreotide (16.6 ± 9.1 mo). Three patients who received 111In-pentetreotide, and relapsed at 11, 12, and 26 mo, received a second treatment of radionuclide therapy. Two of these patients improved and had an event-free survival of 16.3 ± 8.4 mo.
Comparison with Untreated Patients
In group B, 9 of 12 patients (75% of group B) had significant tumor progression within 3 mo, according to conventional criteria. This rate was significantly higher than the rate in group A at 3 mo (P < 0.01). At 12 mo, only 2 patients in group B had no significant tumor progression according to conventional criteria. Consequently, 6 patients with tumor progression required chemotherapy alone (n = 2) or combined with external radiotherapy (n = 1), radiotherapy alone (n = 2), or chemoembolization (n = 1) as rescue therapy.
Figure 3 displays the progression-free Kaplan–Meier survival curves of both groups. The cumulative progression-free survival rate during the first 15 mo was significantly higher in patients receiving radionuclide therapy (P = 0.024).
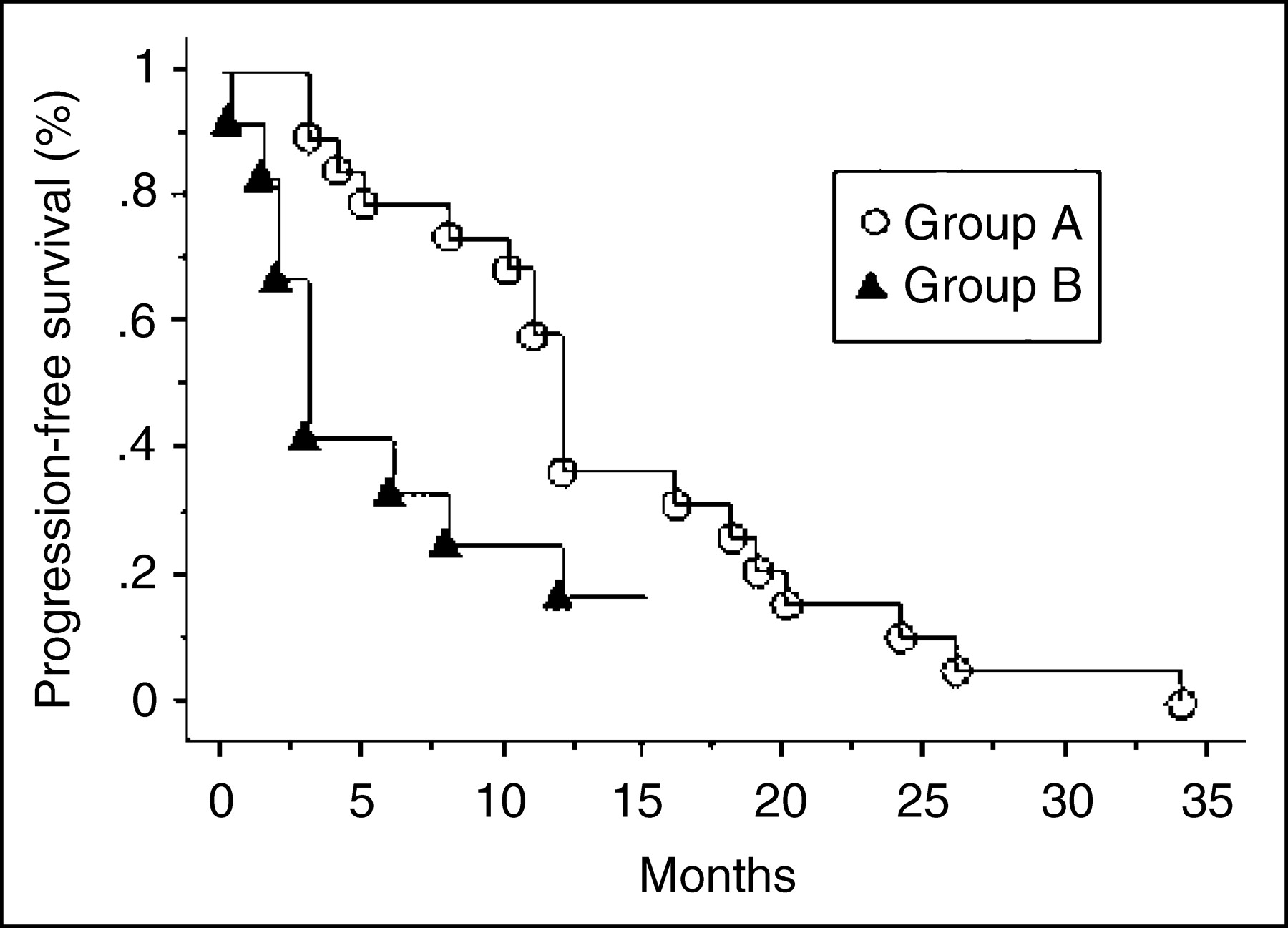
Progression-free Kaplan–Meier survival curves of patients in group A (treated) and group B (nontreated) (P = 0.024).
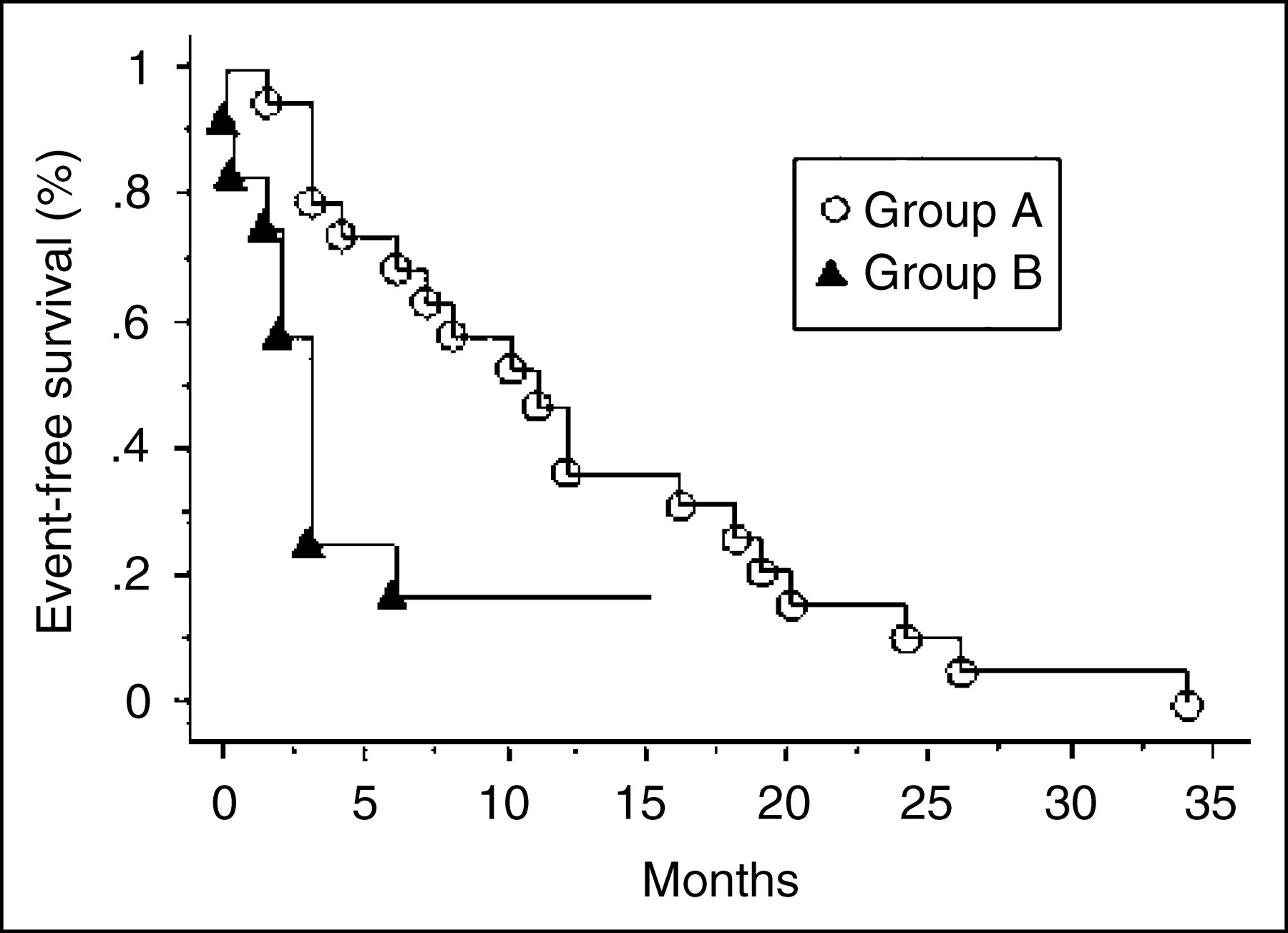
Figure 4 displays the event-free survival curves—as previously defined in the follow-up section—of both groups. The cumulative event-free survival rate during the first 15 mo was significantly higher in patients receiving radionuclide therapy (P = 0.019). In a multivariate analysis, no predictive factor of event-free survival was found among the following parameters: age, duration of disease > 5 y, type of primary lesion, and amount of administered radioactivity. Patients with extranodal and extrahepatic metastases may have had a shorter survival (P = 0.09).
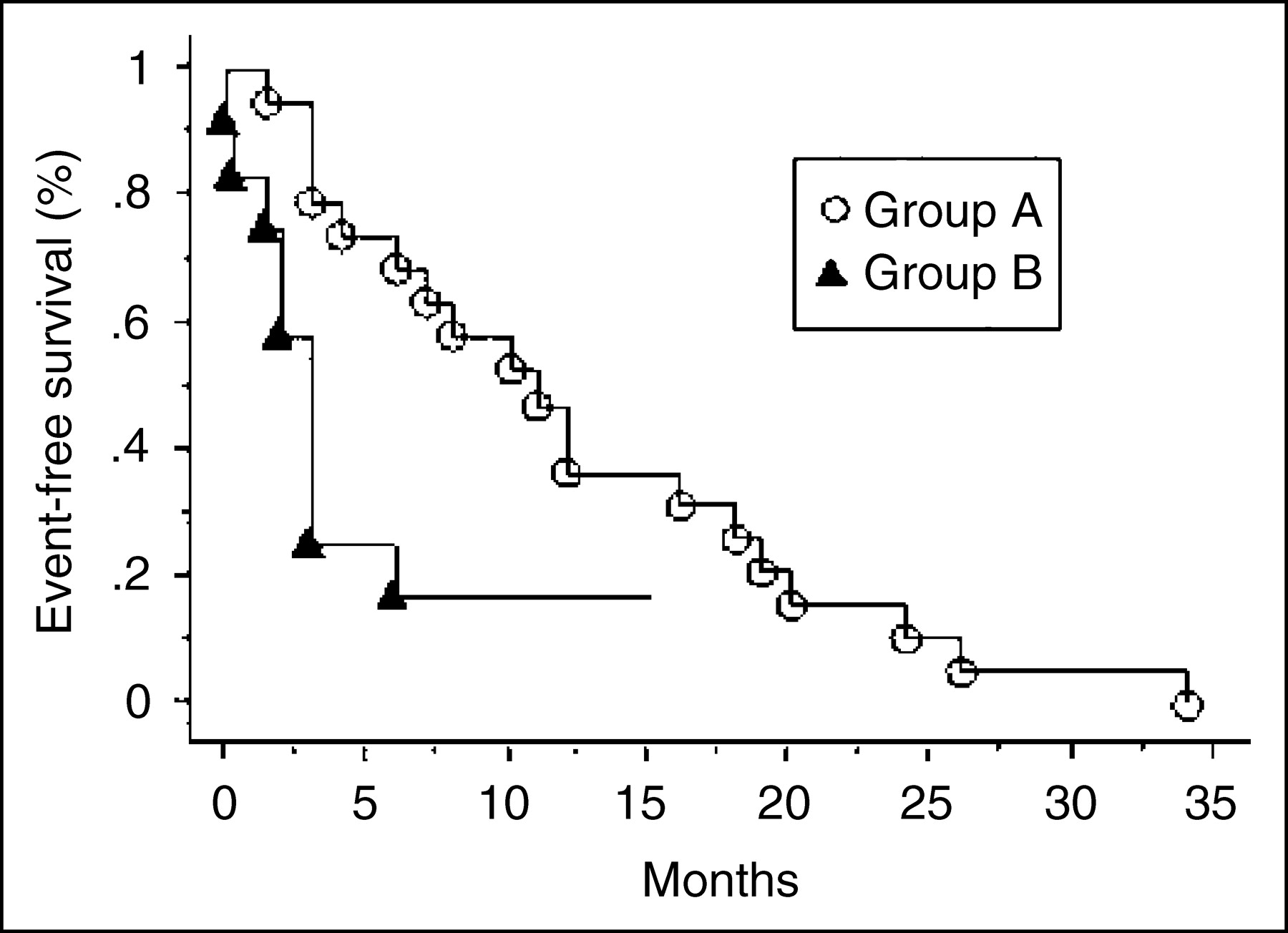
Event-free Kaplan–Meier survival curves of patients in group A (treated) and group B (nontreated) (P = 0.019).
DISCUSSION
To our knowledge, this is the first prospective study to compare the efficacy of radionuclide therapy with 111In-pentetreotide and 131I-MIBG in patients with advanced-stage GEP tumors in a situation of therapeutic deadlock with the outcome of untreated patients. Although the overall death rate at 24 mo was not significantly different between the groups, our results show that fatal and nonfatal events occur significantly earlier in untreated patients. There was a clinical response in 47% of treated patients, a marker response in 21%, tumor stabilization in 73%, and tumor regression in 5%. Tolerance of radionuclide therapy was excellent for both tracers: only 1 patient had a significant side effect with 131I-MIBG. Furthermore, during the follow-up, no major renal complication was detected by repeated laboratory tests, even though no protective procedure other than hydration was used (31) and delayed side effects cannot be excluded.
The use of 131I-MIBG for therapy was first reported by Hoefnagel et al. (11) in advanced-stage neuroendocrine tumors (including 19 carcinoids), with a single administration of 3.7–7.4 GBq. Despite the absence of objective tumoral response in the 19 carcinoid patients, 12 patients improved their clinical status. Further results have been reported by others. With 131I-MIBG therapy (32,33) in a series of 36 carcinoids, there were tumor responses in 22% and clinical improvement in 70% with 1–6 administrations of 1.8–60.5 GBq. More recently, Bongers et al. (34) reported a series of 12 patients (including 9 carcinoids) with clinical response in 65% and tumor size reduction in 15%. The time before relapse ranged from 3 to 24 mo. These results are similar to ours, allowing for the intermediate activity we administered (3 administrations of 3.7–7.4 GBq). According to data in the literature (35), the expected tumors’ absorbed dose ranged from 0.4 to 16.9 mGy/MBq.
Several authors reported the use of 111In-pentetreotide in digestive neuroendocrine tumors (5,24–26,29,30). The total activity that was administered varied from study to study: a maximum of 10 times 3–5 GBq for Buscombe et al. (5), 2 single administrations of 6.7 GBq for Anthony et al. (30), a maximum of 10 times 6–7 GBq for Valkema et al. (29), and 4 administrations of 5.9–11.1 GBq for Cornelius et al. (25). These various procedures resulted in various effects. Valkema et al. (29) did not report significant tumor size regression in 50 treated patients (with a follow-up of 10 mo), but the disease was stabilized in 14 patients and there was a “minor response” in 6 cases (25%–50% reduction of tumor size). Bone marrow toxicity occurred in 3 of 6 patients who received >100 GBq of 111In-pentetreotide. In the study by Anthony et al. (30), 2 of 26 patients showed partial tumor response 1 mo after therapy, 16 of 26 had a clinical response, and 21 of 26 had markers decreased by about 80%. One of these 26 patients suffered kidney toxicity. In this series, the intensity of initial tracer uptake was predictive of therapeutic response (29). In our series, all patients had a high tracer uptake according to this author’s criteria. Absorbed tumor dose when using 111In-pentetreotide ranged from 0.96 to 7.76 mGy/MBq according to Förster et al. (36). Other trials have reported the use of a somatostatin analog labeled with 90Y. A cumulative maximal activity of 8.5 GBq of 90Y-DOTA-lanreotide (DOTA is dodecanetetraacetic acid) was administered in patients with GEP tumors (16). Tumor appeared stabilized in 63 of 154 patients, and regressed in 22, with no significant side effect. De Jong et al. (14) reported the use of 90Y-DOTA-octreotide and 177Lu-DOTA-octreotate in patients with GEP tumors. Among 92 patients who received a maximal cumulative dose of 26 GBq of 90Y-DOTA-octreotide, 20% had a partial tumor response, and several patients experienced total resolution of symptoms. Preliminary results with 177Lu-DOTA-octreotate are also very promising (14,37). Although 90Y or 177Lu appears more suitable for radionuclide therapy in terms of the decay period and characteristics of electron emission, they were not available for medical use either in our country or elsewhere at the time of the study. To date, none of these molecules is commercially available.
In the present study, radionuclide therapy was used as a rescue therapy, which may lead to underestimation of its beneficial effects. Indeed, most untreated patients died in the first 3 mo, the minimal period during which the 3 monthly administrations were delivered. In 3 patients, a second course of radionuclide therapy could be delivered and these patients had the best survival rate. This suggests that prolonged remission may occur in patients with less-advanced stages of the disease. Further studies are needed to investigate this hypothesis. Larger series are also required to better define prognostic factors and patient outcome.
The efficacy of radionuclide therapy and the dose delivered to tumors depend on several physical and physiopathologic factors. First, the tumor affinity of the radiopharmaceutical (and the stability of the linkage) may vary from one patient to another and, for a given patient, from one localization to another. Pentetreotide was previously reported as highly specific for GEP tumors (6,38–40), whereas this affinity appeared to be lower for MIBG (9,10). Indeed, in our series, only 5 of 20 patients fulfilled the criteria for radionuclide therapy with 131I-MIBG. Second, the physical properties of the radionuclide linked to the tracer are also of major importance. Considering the average electron range and the local energy deposit at a cellular level, the efficacy of an 131I-labeled tracer should be better for large-sized tumors, and 111In should be better for smaller, millimeter-scale tumors. To illustrate this, the only patient whose liver metastases decreased in size and whose urinary 5-HIAA was normalized (patient 18) had been given 131I-MIBG. However, we cannot draw conclusions from our study about efficacy with respect to tumor size because, for financial reasons, 131I-MIBG was systematically used in patients whose uptake of both tracers was similar.
Our results may have several limitations. The number of treated patients is limited and patients were not randomized. Additionally, the absence of agreement by the national health insurance and, subsequently, the absence of treatment for financial constraints in several patients is ethically questionable: About one third of the patients could not be given the treatment. When the budget of our department was exceeded, we asked each center to assume the cost of therapy for its referred patient. Because this had not been previously anticipated, some centers could not support the cost in the 6 mo after the indication. This was not related to the socioeconomic condition or ethnic characteristics of patients, and no specific center was particularly involved. This reveals a deep limitation in our medical practice, which should be improved in the coming months. Nonetheless, our study, thus limited, reports a pragmatic use of the only available radiotracers in a clinically uncontrolled stage of the disease, in which untreated patients could be compared with treated patients. Since the intent was to treat all patients, the comparison between groups remains valid and our study highlights the relevance of internal radiotherapy at an advanced stage of the disease. Another limitation of our study concerns the criteria of therapeutic benefit. In patients with endocrine tumors with multiple locations and slow tumor growth, clinical improvement is a pragmatic goal for the patient’s comfort. Although regression in tumor size is seldom observed, in our study as well as in others, obtaining a significant clinical benefit raises the problem of criteria for therapeutic benefit in GEP tumors. Indeed, the objective estimation of tumor volume appears as artificial or unrealistic in patients with multiple tumor sites of various shape and size, and we deliberately chose the simplistic evaluation of tumor size, by measuring the diameters of significant localizations. The only significant and dramatic tumor regression (–75%), which was observed in patient 18, could not been explained by methodologic considerations. Although tumor regression was evaluated according to the WHO criteria, we deliberately chose a threshold of >25% in diameter increase (instead of >50%) for tumor progression. This threshold seemed more suitable for neuroendocrine tumors, with respect to the poor spontaneous prognosis of our patients. Furthermore, this cannot have impaired our conclusions, since the choice of a more “severe” threshold, rather, leads to a decrease in the efficacy of radionuclide therapy.
Finally, there are no objective data on cost–benefit ratios of second-line chemotherapy, including new promising drugs such as CTP11 (irinotecan) or oxaliplatine, compared with internal radiotherapy. Further studies are needed to assess the efficacy of radionuclide therapy in patients with less-advanced tumors.
CONCLUSION
Radionuclide therapy of GEP tumors with either 111In-pentetreotide or 131I-MIBG is feasible and safe. In patients who are clinically uncontrolled by conventional therapy, radionuclide therapy seems to significantly defer the occurrence of fatal and nonfatal events and may be repeated to prolong the initial benefit. Therapeutic effects may be observed as early as 3 mo, if the treatment is not administered at end-stage disease. Further studies are required to determine the optimal radiotracer and the activity to administer and to better define patient selection criteria.
Footnotes
Received Dec. 1, 2003; revision accepted Apr. 12, 2004.
For correspondence or reprints contact: Charles Nguyen, MD, Service de Médecine Nucléaire, Centre Hospitalier et Universitaire de Saint-Antoine, 184 rue du Faubourg Saint-Antoine, 75571 Paris, France.
E-mail: charles.nguyen{at}sat.ap-hop-paris.fr
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Anti-SSTR2 Antibody-Drug Conjugate for Neuroendocrine Cancer Therapy
- A population-based study of outcomes in patients with gastrointestinal neuroendocrine tumours
- Targeted Radionuclide Therapy: Proceedings of a Joint Workshop Hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging